
Impact of Resilience on Patient Reported Outcome of First Metatarsophalangeal Arthrodesis


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical Outcomes
3.2. Bivariate Analysis
3.3. Multivariate Linear Regression
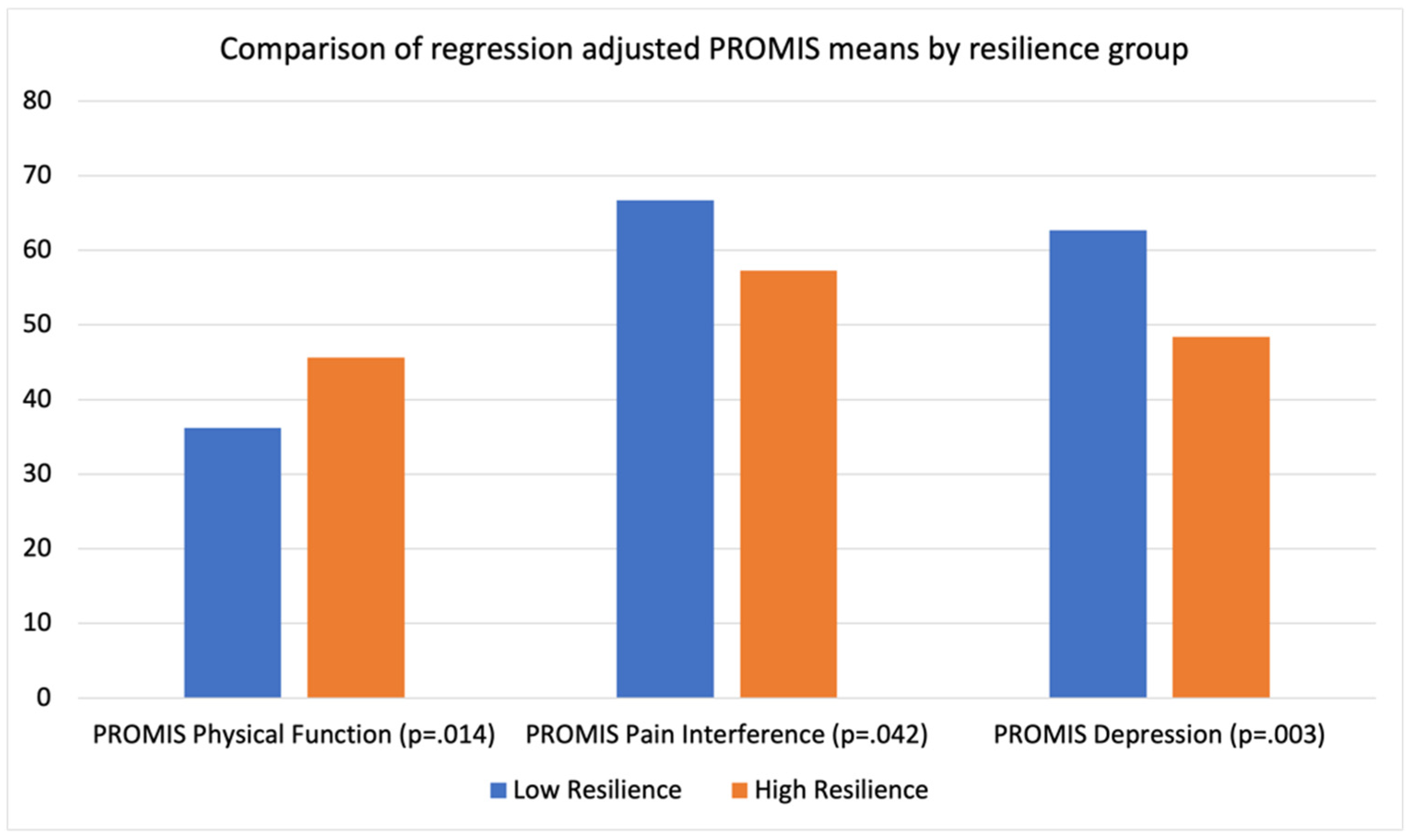
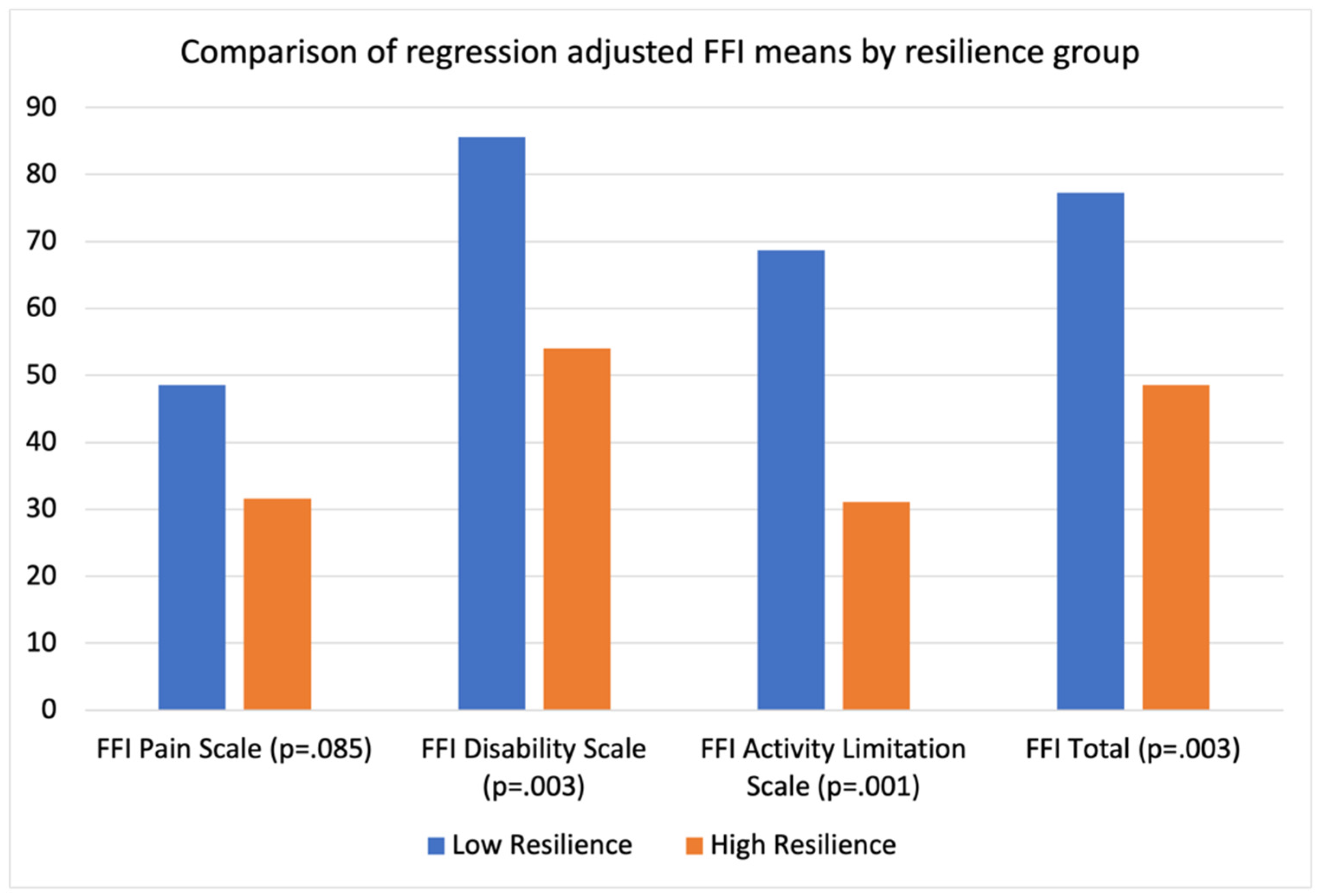
3.4. Comparison of Low and High Resilience Groups Using Regression Model Adjusted Means
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, B.W.; Epstein, E.M.; Ortiz, J.A.; Christopher, P.J.; Tooley, E.M. The Foundations of Resilience: What Are the Critical Resources for Bouncing Back from Stress? In Resilience in Children, Adolescents, and Adults: Translating Research into Practice; NPrince-Embury, S., Saklofske, D.H., Eds.; Springer: New York, NY, USA, 2013; pp. 167–187. [Google Scholar] [CrossRef]
- Vranceanu, A.M.; Beks, R.B.; Guitton, T.G.; Janssen, S.J.; Ring, D. How do orthopedic surgeons address psychological aspects of illness? Arch. Bone Jt. Surg. 2017, 5, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Ezeamama, A.E.; Elkins, J.; Simpson, C.; Smith, S.L.; Allegra, J.C.; Miles, T.P. Indicators of resilience and healthcare outcomes: Findings from the 2010 health and retirement survey. Qual. Life Res. 2015, 25, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Tokish, J.M.; Kissenberth, M.J.; Tolan, S.J.; Salim, T.I.; Tadlock, J.; Kellam, T.; Long, C.D.; Crawford, A.; Lonergan, K.T.; Hawkins, R.J.; et al. Resilience correlates with outcomes after total shoulder arthroplasty. J. Shoulder Elbow Surg. 2017, 26, 752–756. [Google Scholar] [CrossRef] [PubMed]
- Magaldi, R.J.; Staff, I.; Stovall, A.E.; Stohler, S.A.; Lewis, C.G. Impact of Resilience on Outcomes of Total Knee Arthroplasty. J. Arthroplasty 2019, 34, 2620–2623.e1. [Google Scholar] [CrossRef]
- Coronado, R.A.; Robinette, P.E.; Henry, A.L.; Pennings, J.S.; Haug, C.M.; Skolasky, R.L.; Riley, L.H., III; Neuman, B.J.; Cheng, J.S.; Aaronson, O.S.; et al. Bouncing Back after Lumbar Spine Surgery: Early Postoperative Resilience is Associated with 12-Month Physical Function, Pain Interference, Social Participation, and Disability. Spine J. 2020, 21, 55–63. [Google Scholar] [CrossRef]
- Giesinger, J.M.; Kuster, M.S.; Behrend, H.; Giesinger, K. Association of psychological status and patient-reported physical outcome measures in joint arthroplasty: A lack of divergent validity. Health Qual. Life Outcomes 2013, 11, 64. [Google Scholar] [CrossRef] [Green Version]
- Agel, J.; Beskin, J.L.; Brage, M.; Guyton, G.P.; Kadel, N.J.; Saltzman, C.L.; Sands, A.K.; Sangeorzan, B.J.; SooHoo, N.F.; Stroud, C.C.; et al. Reliability of the Foot Function Index: A Report of the AOFAS Outcomes Committee. Foot Ankle Int. 2005, 26, 962–967. [Google Scholar] [CrossRef]
- Budiman-Mak, E.; Conrad, K.; Stuck, R.; Matters, M. Theoretical model and rasch analysis to develop a revised foot function index. Foot Ankle Int. 2006, 27, 519–527. [Google Scholar] [CrossRef]
- Hung, M.; Stuart, A.R.; Higgins, T.F.; Saltzman, C.L.; Kubiak, E.N. Computerized adaptive testing using the PROMIS physical function item bank reduces test burden with less ceiling effects compared with the short musculoskeletal function assessment in orthopaedic trauma patients. J. Orthop. Trauma 2014, 28, 439–443. [Google Scholar] [CrossRef]
- Hung, M.; Franklin, J.D.; Hon, S.D.; Cheng, C.; Conrad, J.; Saltzman, C.L. Time for a Paradigm Shift with Computerized Adaptive Testing of General Physical Function Outcomes Measurements. Foot Ankle Int. 2013, 35, 1–7. [Google Scholar] [CrossRef]
- Hung, M.; Clegg, D.O.; Greene, T.; Saltzman, C.L. Evaluation of the PROMIS physical function item bank in orthopaedic patients. J. Orthop. Res. 2011, 29, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.R.; Baumhauer, J.F.; DiGiovanni, B.F.; Flemister, S.; Ketz, J.P.; Oh, I.; Houck, J.R. Determining Success or Failure After Foot and Ankle Surgery Using Patient Acceptable Symptom State (PASS) and Patient Reported Outcome Information System (PROMIS). Foot Ankle Int. 2018, 39, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Hung, M.; Baumhauer, J.F.; Latt, D.L.; Saltzman, C.L.; SooHoo, N.F.; Hunt, K.J. Validation of PROMIS ® Physical Function computerized adaptive tests for orthopaedic foot and ankle outcome research. Clin. Orthop. 2013, 471, 3466–3474. [Google Scholar] [CrossRef] [Green Version]
- Hung, M.; Baumhauer, J.F.; Licari, F.W.; Voss, M.W.; Bounsanga, J.; Saltzman, C.L. PROMIS and FAAM Minimal Clinically Important Differences in Foot and Ankle Orthopedics. Foot Ankle Int. 2019, 40, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Hunt, K.J.; Alexander, I.; Baumhauer, J.; Brodsky, J.; Chiodo, C.; Daniels, T.; Davis, W.H.; Deland, J.; Ellis, S.; Hung, M.; et al. The Orthopaedic Foot and Ankle Outcomes Research (OFAR) Network: Feasibility of a Multicenter Network for Patient Outcomes Assessment in Foot and Ankle. Foot Ankle Int. 2014, 35, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Lakey, E.; Hunt, K.J. Patient-Reported Outcomes in Foot and Ankle Orthopedics. Foot Ankle Orthop. 2019, 4, 247301141985293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nixon, D.C.; McCormick, J.J.; Johnson, J.E.; Klein, S.E. PROMIS Pain Interference and Physical Function Scores Correlate With the Foot and Ankle Ability Measure (FAAM) in Patients With Hallux Valgus. Clin. Orthop. 2017, 475, 2775–2780. [Google Scholar] [CrossRef] [Green Version]
- Shazadeh Safavi, P.; Janney, C.; Jupiter, D.; Kunzler, D.; Bui, R.; Panchbhavi, V.K. A Systematic Review of the Outcome Evaluation Tools for the Foot and Ankle. Foot Ankle Spéc. 2018, 12, 461–470. [Google Scholar] [CrossRef]
- Stephan, A.; Mainzer, J.; Kümmel, D.; Impellizzeri, F.M. Measurement properties of PROMIS short forms for pain and function in orthopedic foot and ankle surgery patients. Qual. Life Res. 2019, 28, 2821–2829. [Google Scholar] [CrossRef]
- Kitaoka, H.B.; Meeker, J.E.; Phisitkul, P.; Adams, S.B.; Kaplan, J.R.; Wagner, E. AOFAS Position Statement Regarding Patient-Reported Outcome Measures. Foot Ankle Int. 2018, 39, 1389–1393. [Google Scholar] [CrossRef]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Korim, M.T.; Mahadevan, D.; Ghosh, A.; Mangwani, J. Effect of joint pathology, surface preparation and fixation methods on union frequency after first metatarsophalangeal joint arthrodesis: A systematic review of the English literature. Foot Ankle Surg. 2017, 23, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Brewster, M. Does total joint replacement or arthrodesis of the first metatarsophalangeal joint yield better functional results? A systematic review of the literature. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2010, 49, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Pinsker, E.; Daniels, T.R. AOFAS Position Statement Regarding the Future of the AOFAS Clinical Rating Systems. Foot Ankle Int. 2011, 32, 841–842. [Google Scholar] [CrossRef]
- Challagundla, S.R.; Thomas, R.; Ferdinand, R.; Crane, E. First Metatarsophalangeal Joint Arthrodesis Using Memory Staples: Clinical and Functional Results. Foot Ankle Spéc. 2020, 14, 410–414. [Google Scholar] [CrossRef]
- DeSandis, B.; Pino, A.; Levine, D.S.; Roberts, M.; Deland, J.; O’Malley, M.; Elliott, A. Functional Outcomes Following First Metatarsophalangeal Arthrodesis. Foot Ankle Int. 2016, 37, 715–721. [Google Scholar] [CrossRef]
- Lunati, M.P.; Manz, W.J.; Maidman, S.D.; Kukowski, N.R.; Mignemi, D.; Bariteau, J.T. Effect of Age on Complication Rates and Outcomes Following First Metatarsophalangeal Arthrodesis for Hallux Rigidus. Foot Ankle Int. 2020, 41, 1347–1354. [Google Scholar] [CrossRef]
- Van Doeselaar, D.J.; Heesterbeek, P.J.C.; Louwerens, J.W.K.; Swierstra, B.A. Foot function after fusion of the first metatarsophalangeal joint. Foot Ankle Int. 2010, 31, 670–675. [Google Scholar] [CrossRef]
- Quach, C.W.; Langer, M.M.; Chen, R.C.; Thissen, D.; Usinger, D.S.; Emerson, M.A.; Reeve, B.B. Reliability and validity of PROMIS measures administered by telephone interview in a longitudinal localized prostate cancer study. Qual. Life Res. 2016, 25, 2811–2823. [Google Scholar] [CrossRef]
- Cella, D.; Yount, S.; Rothrock, N.; Gershon, R.; Cook, K.; Reeve, B.; Ader, D.; Fries, J.F.; Bruce, B.; Rose, M. The Patient-Reported Outcomes Measurement Information System (PROMIS): Progress of an NIH Roadmap cooperative group during its first two years. Med. Care 2007, 45, S3–S11. [Google Scholar] [CrossRef] [Green Version]
- Kendall, R.; Wagner, B.; Brodke, D.; Bounsanga, J.; Voss, M.; Gu, Y.; Spiker, R.; Lawrence, B.; Hung, M. The Relationship of PROMIS Pain Interference and Physical Function Scales. Pain Med. Malden Mass 2018, 19, 1720–1724. [Google Scholar] [CrossRef] [PubMed]
- Budiman-Mak, E.; Conrad, K.J.; Roach, K.E. The Foot Function Index: A measure of foot pain and disability. J. Clin. Epidemiol. 1991, 44, 561–570. [Google Scholar] [CrossRef]
- Markovitz, S.E.; Schrooten, W.; Arntz, A.; Peters, M.L. Resilience as a predictor for emotional response to the diagnosis and surgery in breast cancer patients. Psychooncology 2015, 24, 1639–1645. [Google Scholar] [CrossRef] [PubMed]
- Colpe, L.J.; Naifeh, J.A.; Aliaga, P.A.; Sampson, N.A.; Heeringa, S.G.; Stein, M.B.; Ursano, R.J.; Fullerton, C.S.; Nock, M.K.; Schoenbaum, M.L.; et al. Mental Health Treatment Among Soldiers With Current Mental Disorders in the Army Study to Assess Risk and Resilience in Service Members (Army STARRS). Mil. Med. 2015, 180, 1041–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merritt, V.C.; Lange, R.T.; French, L.M. Resilience and symptom reporting following mild traumatic brain injury in military service members. Brain Inj. 2015, 29, 1325–1336. [Google Scholar] [CrossRef] [PubMed]
- Sturgeon, J.A.; Zautra, A.J. Resilience: A New Paradigm for Adaptation to Chronic Pain. Curr. Pain Headache Rep. 2010, 14, 105–112. [Google Scholar] [CrossRef]
- Trinh, J.Q.; Carender, C.N.; An, Q.; Noiseux, N.O.; Otero, J.E.; Brown, T.S. Resilience and Depression Influence Clinical Outcomes Following Primary Total Joint Arthroplasty. J. Arthroplasty 2020, 36, 1520–1526. [Google Scholar] [CrossRef]
- Werner, B.C.; Wong, A.C.; Chang, B.; Craig, E.V.; Dines, D.M.; Warren, R.F.; Gulotta, L.V. Depression and Patient-Reported Outcomes Following Total Shoulder Arthroplasty. J. Bone Jt. Surg 2017, 99, 688–695. [Google Scholar] [CrossRef]
- Lim, K.K.; Matchar, D.B.; Tan, C.S.; Yeo, W.; Østbye, T.; Howe, T.S.; Koh, J.S. The Association Between Psychological Resilience and Physical Function Among Older Adults With Hip Fracture Surgery. J. Am. Med. Dir. Assoc. 2020, 21, 260–266.e2. [Google Scholar] [CrossRef]
- Shakked, R.; McDonald, E.; Sutton, R.; Lynch, M.K.; Nicholson, K.; Raikin, S.M. Influence of Depressive Symptoms on Hallux Valgus Surgical Outcomes. Foot Ankle Int. 2018, 39, 795–800. [Google Scholar] [CrossRef]
- Kim, T.Y.; Lee, H.W.; Jeong, B.O. Influence of Depressive Symptoms on the Clinical Outcomes of Total Ankle Arthroplasty. J. Foot Ankle Surg. 2020, 59, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Schultz, B.J.; Tanner, N.; Shapiro, L.M.; Segovia, N.A.; Kamal, R.N.; Bishop, J.A.; Gardner, M.J. Patient-Reported Outcome Measures (PROMs): Influence of Motor Tasks and Psychosocial Factors on FAAM Scores in Foot and Ankle Trauma Patients. J. Foot Ankle Surg. 2020, 59, 758–762. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.M.; Lim, J.Y.; Kim, E.J.; Park, S.-M. Resilience of patients with chronic diseases: A systematic review. Health Soc. Care Community 2019, 27, 797–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joyce, S.; Shand, F.; Tighe, J.; Laurent, S.J.; Bryant, R.A.; Harvey, S.B. Road to resilience: A systematic review and meta-analysis of resilience training programmes and interventions. BMJ Open 2018, 8, e017858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lester, P.; Stein, J.A.; Saltzman, W.; Woodward, K.; MacDermid, S.W.; Milburn, N.; Mogil, C.; Beardslee, W. Psychological Health of Military Children: Longitudinal Evaluation of a Family-Centered Prevention Program to Enhance Family Resilience. Mil. Med. 2013, 178, 838–845. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patient Factor | N (%) Unless Otherwise Noted | Patient Factor | N (%) Unless Otherwise Noted | Patient Factor | N (%) Unless Otherwise Noted |
|---|---|---|---|---|---|
| Age (Mean ± SD) | 58.4 ± 11.4 | ASA Class | Complications: | ||
| BMI (Mean ± SD) | 30.7 ± 6.3 | 1 | 2 (2%) | Wound Complication | 6 (6%) |
| Sex | 2 | 40 (41%) | Revision Surgery | ||
| Female | 73 (74%) | 3 | 54 (55%) | Infection | 3 (3%) |
| Male | 25 (26%) | 4 | 2 (2%) | Painful Hardware | 5 (5%) |
| Isolated MTP Arthrodesis | 56 (57%) | Tobacco Users | 15 (15%) | Hardware Failure | 1 (1%) |
| Concomitant Procedures | Hypertension | 59 (60%) | Radiographic Union: | ||
| Weil Osteotomy | 23 (24%) | Diabetes Mellitus | 15 (15%) | Union | 91 (93%) |
| Hammer Toe Correction | 14 (14%) | Hypothyroidism | 11 (11%) | Nonunion | 7 (7%) |
| PIP Arthroplasty | 4 (4%) | Rheumatoid Arthritis | 12 (12%) | Time from surgery to survey in years (Mean ± SD) | 3.42 ± 0.65 |
| Midfoot Arthrodesis | 4 (4%) | COPD | 5 (5%) | PROMIS Domain Scores (Median ± IQR) | |
| Gatrocnemius Recession | 3 (3%) | CAD | 6 (6%) | Physical Function | 43.2 ± 14.7 |
| EHL Augmentation | 4 (4%) | Osteoporosis/Osteopenia | 8 (8%) | Pain Interference | 54.1 ± 14.4 |
| Neuroma Excision | 2 (2%) | Psychiatric Condition | 21 (21%) | Depression | 43.5 ± 17.6 |
| Metatarsal Head Resection | 7 (7%) | Immunosuppression | 15 (15%) | FFI Scores (Median ± IQR) | |
| Interfragmentary Screw | 74 (75%) | Pain | 27.5 ± 41.7 | ||
| Disability | 34.4 ± 45.0 | ||||
| Activity Limitation | 10.0 ± 25.0 | ||||
| Total | 32.1 ± 43.1 |
| Continuous Variables | PROMIS Physical Function R Value (p Value) | PROMIS Pain Interference R Value (p Value) | PROMIS Depression R Value (p Value) | FFI Pain R Value (p Value) | FFI Disability R Value (p Value) | FFI Activity Limitation R Value (p Value) | FFI Total R Value (p Value) |
|---|---|---|---|---|---|---|---|
| Age | −0.048 (p = 0.636) | −0.016 (p = 0.879) | −0.134 (p = 0.190) | −0.135 (p = 0.185) | −0.073 (p = 0.476) | 0.037 (p = 0.720) | −0.070 (p = 0.491) |
| BMI | −0.038 (p = 0.710) | 0.101 (p = 0.325) | 0.025 (p = 0.808) | 0.088 (p = 0.387) | 0.101 (p = 0.387) | 0.158 (p = 0.120) | 0.120 (p = 0.238) |
| Preop HVA | −0.120 (p = 0.240) | 0.040 (p = 0.695) | −0.045 (p = 0.662) | 0.055 (p = 0.593) | 0.109 (p = 0.287) | 0.059 (p = 0.561) | 0.076 (p = 0.455) |
| Postop HVA | −0.279 (p = 0.005) * | 0.142 (p = 0.163) | 0.105 (p = 0.303) | 0.101 (p = 0.323) | 0.141 (p = 0.166) | 0.158 (p = 0.120) | 0.129 (p = 0.204) |
| Preop IMA | −0.096 (p = 0.327) | −0.037 (p = 0.720) | 0.079 (p = 0.440) | −0.078 (p = 0.445) | 0.017 (p = 0.865) | 0.002 (p = 0.985) | −0.014 (p = 0.894) |
| Postop IMA | −0.138 (p = 0.175) | 0.027 (p = 0.788) | 0.110 (p = 0.281) | −0.026 (p = 0.799) | −0.022 (p = 0.831) | 0.044 (p = 0.668) | −0.010 (p = 0.925) |
| Postop dorsiflexion angle | 0.103 (p = 0.313) | 0.024 (p = 0.818) | −0.182 (p = 0.073) | −0.109 (p = 0.284) | −0.115 (p = 0.260) | −0.074 (p = 0.467) | −0.124 (p = 0.224) |
| Time from surgery to patient reported outcome collection | 0.078 (p = 0.447) | −0.061 (p = 0.549) | −0.045 (p = 0.663) | −0.115 (p = 0.261) | −0.115 (p = 0.259) | −0.069 (p = 0.501) | −0.101 (p = 0.325) |
| Resilience | 0.345 (p = 0.001) * | −0.244 (p = 0.015) * | −0.523 (p < 0.001) * | −0.204 (p = 0.044) * | −0.413 (p < 0.001) * | −0.391 (p < 0.001) * | −0.380 (p < 0.001) * |
| Covariates for PROMIS Physical Function | PROMIS Physical Function β | 95% Confidence Interval | p Value |
| Weil Osteotomy | −3.7 | −7.4 to 0.02 | 0.051 |
| ASA Classification | −2.5 | −5.3 to 0.312 | 0.081 |
| Postop Hallux Valgus Angle | −0.27 * | −0.43 to −0.12 | 0.001 * |
| Hypertension | −3.7 * | −7.0 to 0.02 | 0.021 * |
| Time from surgery to patient reported outcome collection | −0.11 | −0.73 to 0.52 | 0.737 |
| Resilience | 5.1 * | 2.6 to 7.6 | <0.001 * |
| Covariates for PROMIS Pain Interference | PROMIS Pain Interference β | 95% Confidence Interval | p Value |
| ASA Classification | 2.9 | −0.53 to 6.3 | 0.097 |
| Tobacco | 5.3 | −0.12 to 10.7 | 0.055 |
| CAD | 8.0 | −0.25 to 16.2 | 0.057 |
| Wound Complication | 4.3 | −3.9 to 12.5 | 0.300 |
| Time from surgery to patient reported outcome collection | −0.16 | −0.92 to 0.59 | 0.665 |
| Resilience | −4.7 * | −7.8 to −1.6 * | 0.004 * |
| Covariates for PROMIS Depression | PROMIS Depression β | 95% Confidence Interval | p Value |
| Weil Osteotomy | 6.0 * | 1.1 to 10.8 * | 0.016 * |
| COPD | 1.7 | −8.3 to 11.7 | 0.743 |
| Psychiatric Condition | 2.4 | −2.8 to 7.6 | 0.355 |
| Time from surgery to patient reported outcome collection | 0.34 | −0.46 to 1.1 | 0.401 |
| Resilience | −9.7 | −13.1 to −6.3 * | <0.001 * |
| Covariates for FFI Pain | FFI Pain β | 95% Confidence Interval | p Value |
| EHL Augmentation | −16.9 | −39.8 to 6.0 | 0.147 |
| ASA Classification | 4.5 | −3.0 to 12.1 | 0.234 |
| Tobacco Use | 15.4 * | 3.7 to 27.2 * | 0.011 * |
| CAD | 22.3 * | 4.6 to 39.9 * | 0.014 * |
| Psychiatric Condition | 7 | −3.4 to 17.4 | 0.187 |
| Time from surgery to patient reported outcome collection | −0.36 | −2.1 to 1.4 | 0.683 |
| Resilience | −6.3 | −13.0 to 0.45 | 0.067 |
| Covariates for FFI Disability | FFI Disability β | 95% Confidence Interval | p Value |
| Weil Osteotomy | 6.7 | −3.4 to 16.8 | 0.191 |
| ASA Classification | 4.8 | −3.0 to 12.6 | 0.225 |
| Tobacco Use | 11.2 | −1.1 to 23.5 | 0.074 |
| Diabetes Mellitus | 6.0 | −6.2 to 18.3 | 0.330 |
| COPD | 3.6 | −17.5 to 24.8 | 0.734 |
| CAD | 21.7 * | 3.4 to 39.9 * | 0.021 * |
| Wound Complication | 20.6 | −1.8 to 43.0 | 0.071 |
| Nonunion | 13.3 | −7.0 to 33.6 | 0.195 |
| Time from surgery to patient reported outcome collection | −1.1 | −2.8 to 0.58 | 0.195 |
| Resilience | −12.2 * | −12.1 to −6.3 * | 0.001 * |
| Covariates for FFI Activity Limitation | FFI Activity Limitation β | 95% Confidence Interval | p Value |
| ASA Classification | 5.4 | −2.8 to 13.5 | 0.193 |
| Tobacco Use | 5.2 | −7.7 to 18.0 | 0.426 |
| CAD | 39.6 * | 20.1 to 59.2 * | <0.001 * |
| Wound Complication | 1.2 | −0.20.9 to 23.4 | 0.914 |
| Revision Surgery | 25.1 * | 6.3 to 44.0 * | 0.010 * |
| Time from surgery to patient reported outcome collection | −1.3 | −3.2 to 0.57 | 0.171 |
| Resilience | −14.7 * | −7.4 to −22.1 | <0.001 * |
| Covariates for FFI Total | FFI Total β | 95% Confidence Interval | p Value |
| Weil Osteotomy | 2.8 | −6.3 to 12.0 | 0.543 |
| ASA Classification | 6.2 | −0.74 to 13.1 | 0.079 |
| Tobacco Use | 13.0 * | 1.9 to 24.1 * | 0.022 * |
| COPD | 3.2 | −15.9 to 22.3 | 0.739 |
| CAD | 26.9 * | 10.3 to 43.4 | 0.002 * |
| Wound Complication | 14.2 | −5.6 to 34.1 | 0.157 |
| Nonunion | 14.1 | −4.3 to 32.5 | 0.131 |
| Time from surgery to patient reported outcome collection | −1.1 | −2.7 to 0.39 | 0.142 |
| Resilience | −10.6 * | −4.1 to −17.1 * | 0.002 * |
| Outcome Metric | Low Resilience (BRS < 3) Adjusted Means | High Resilience (BRS > 4.3) Adjusted Means | p-Value |
|---|---|---|---|
| PROMIS Physical Function | 36.2 | 45.6 | 0.014 * |
| PROMIS Pain Interference | 66.7 | 57.3 | 0.042 * |
| PROMIS Depression | 62.7 | 48.4 | 0.003 * |
| FFI Pain Scale | 48.6 | 31.6 | 0.085 |
| FFI Disability Scale | 85.6 | 54.0 | 0.003 * |
| FFI Activity Limitation Scale | 68.7 | 31.1 | 0.001 * |
| FFI Total | 77.3 | 48.6 | 0.003 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrews, N.; Tran, S.; Young, S.; Halstrom, J.; Ray, J.; Littlefield, Z.; McGwin, G.; Agarwal, A.; Shah, A. Impact of Resilience on Patient Reported Outcome of First Metatarsophalangeal Arthrodesis. Osteology 2022, 2, 87-98. https://doi.org/10.3390/osteology2020010
Andrews N, Tran S, Young S, Halstrom J, Ray J, Littlefield Z, McGwin G, Agarwal A, Shah A. Impact of Resilience on Patient Reported Outcome of First Metatarsophalangeal Arthrodesis. Osteology. 2022; 2(2):87-98. https://doi.org/10.3390/osteology2020010
Chicago/Turabian StyleAndrews, Nicholas, Sterling Tran, Sean Young, Jared Halstrom, Jessyca Ray, Zach Littlefield, Gerald McGwin, Abhinav Agarwal, and Ashish Shah. 2022. "Impact of Resilience on Patient Reported Outcome of First Metatarsophalangeal Arthrodesis" Osteology 2, no. 2: 87-98. https://doi.org/10.3390/osteology2020010