
The Prevalence and Indications of Intravenous Rehydration Therapy in Hospital Settings: A Systematic Review


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
- What is the prevalence of IV rehydration therapy in hospital settings?
- Is there a certain age group of people that is more likely to receive IV rehydration therapy in hospital settings?
2.1. Search Strategy
2.2. Study Inclusion and Exclusion
2.3. Data Extraction
2.4. Quality Assessment
3. Results
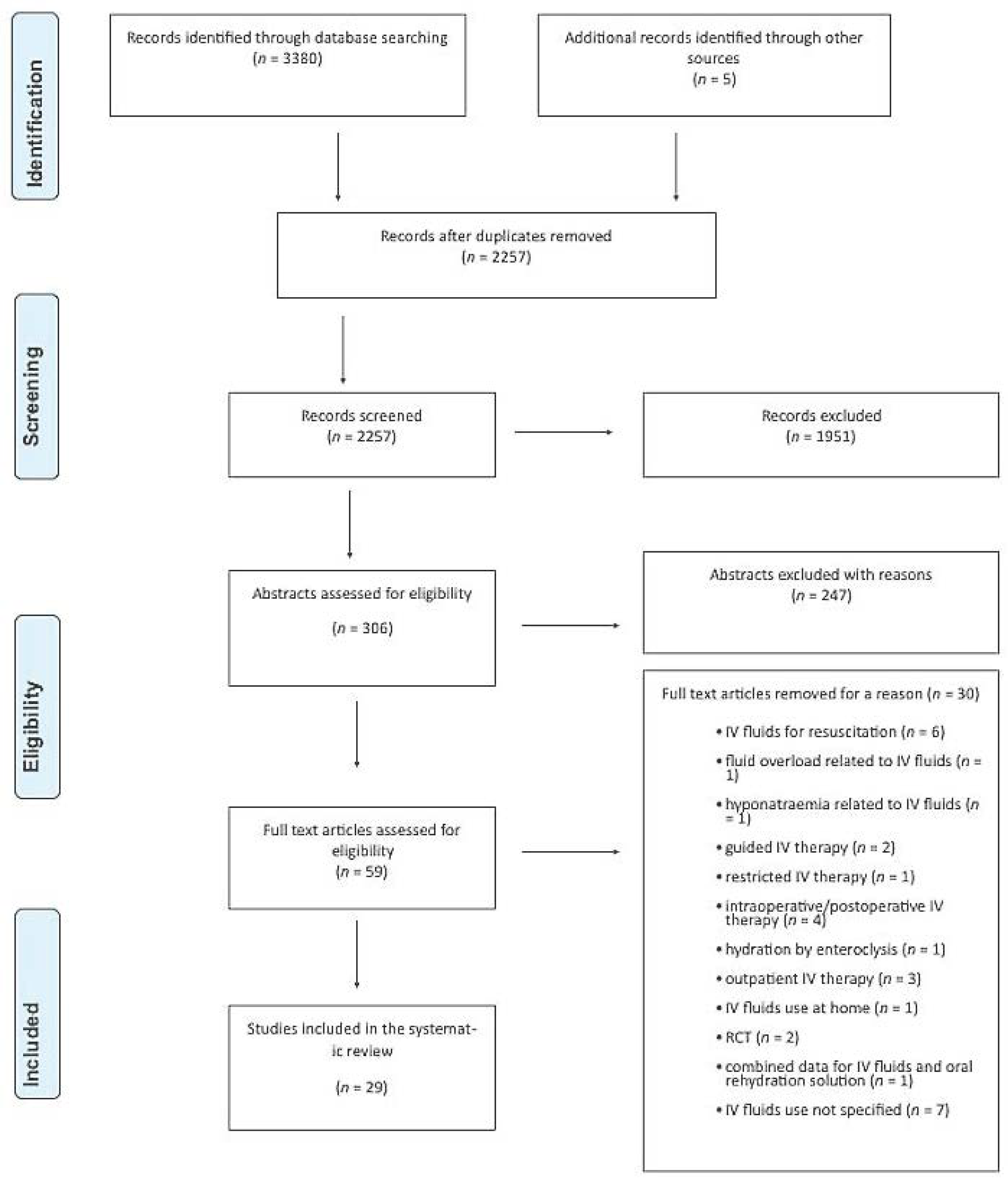
3.1. Search Results
3.2. Studies’ Characteristics

{kind=link}
| Author, Year | Country or Region | Study Duration | Study Design | Sample Size | Age Range | Age Mean (SD) | Age Median (IQR) | Sex % Male | Population | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Abdul-Mumin, Ervin and Halvorson, 2019 [18] | Ghana | January 2013–December 2014 | Retrospective chart review | 473 | NR | NR | 12 (9–24) months | 56 | Paediatric patients hospitalised with acute gastroenteritis | Good |
| Akech et al., 2018 [13] | Kenya | October 2013–December 2016 | Prospective chart review | 8025 | NR | NR | 12 (8–18) months | 0 | Paediatric patients hospitalised with diarrhoea and dehydration | Good |
| Ben- Shalom, Toker and Schwartz, 2016 [29] | Israel | 2001–2010 | Retrospective chart review | 58 | 0–24 months | 6.8 (5.27) months | NR | 59.7 | Paediatric patients hospitalised with hypernatremic dehydration | Good |
| Blacklock et al., 2015 [38] | Sierra Leone | 26 July 2012–22 September 2012 | Retrospective chart review | 798 | <5–≥60 years | NR | NR | 45 | Paediatric and adult patients hospitalised with cholera during the epidemic | Fair |
| Chow et al., 2009 [14] | China | 1 April 2021 to 31 March 2003 | Retrospective chart review | 7391 | NR | NR | 13 (6–26) months | 59 | Paediatric patients admitted to the hospital with diagnosis of diarrhoea. | Fair |
| Dbaibo et al., 2013 [19] | Lebanon | April 2007–August 2008 | Hospital-based surveillance design | 491 | NR | NR | 12 (0–59) months | NR | Paediatric patients hospitalised with a diagnosis of acute gastroenteritis | Fair |
| Fikrie, Alemayehu and Gebremedhin, 2019 [32] | Ethiopia | July 2015–June 2017 | Retrospective cohort | 381 | 6–59 months | 22.4 (15.8) | NR | 49.6 | Paediatric patients hospitalised with Severe Acute Malnutrition | Good |
| Freedman et al., 2014 [20] | USA | 1 January 2002–31 December 2011 | Retrospective cohort study | 804,000 | NR | 3.1 (3.9) years | NR | 53.1 | Paediatric patients who were diagnosed as having gastroenteritis in an emergency department | Good |
| Heyman et al., 1990 [15] | Malawi | July 1981–July 1986 | Retrospective chart review | 3495 | ≤12–≥24 months | NR | NR | 77 | Paediatric patients hospitalised with diarrhoea or gastroenteritis | Fair |
| Janet el al., 2015 [30] | Spain | 15 July 2012–15 December 2012 | Prospective cohort study | 83 | NR | NR | 4 (1.7–7) years | 56.6 | Paediatric patients with mild-to moderate isonatremic dehydration | Fair |
| Kao et al., 2019 [31] | Taiwan | January 2005–January 2015 | Retrospective chart review | 44 | NR | 9.9 (5.6) years | 11.1 (10.6) | 68.2 | Paediatric patients with chronic neuromuscular disorder who visited the emergency room | Good |
| Lopez-Medina et al., 2012 [33] | USA | 27 April 2009–23 March 2010 | Retrospective cohort study | 73 | 3–179 days | NR | 48 days | 48 | Paediatric patients hospitalised with laboratory-confirmed influenza | Fair |
| Machado et al., 2015 [41] | USA | 1 October 2010–30 September 2013 | Retrospective chart review | 72 | 54–87 years | 70.4 (NR) years | NR | 40 | Patients hospitalised with hypercalcemia | Good |
| Marra et al., 2011 [36] | Brazil | 8 April 2008–9 May 2008 | Retrospective chart review | 3393 | NR | NR | NR | NR | Paediatric and adult patients treated in the hydration tent during dengue fever epidemic | Fair |
| Moineau and Newman, 1990 [21] | Canada | December 1988–April 1989 | Prospective pilot study | 17 | NR | 2.6 (1.7) years | NR | 47 | Paediatric patients admitted to the emergency department with mild to moderate dehydration caused by viral gastroenteritis | Fair |
| Myat et al., 2021 [22] | Myanmar | May 2018–January 2020 | Hospital-based surveillance design | 3226 | 5 days to 59 months | NR | NR | 59.5 | Paediatric patients hospitalised for acute gastroenteritis | Fair |
| Nazurdinov et al., 2018 [23] | Tajikistan | January 2013–December 2014 | Hospital-based surveillance design | 2863 | 0–59 months | NR | NR | 61 | Paediatric patients hospitalised with acute gastroenteritis and rotavirus | Fair |
| Oakley et al., 2016 [34] | Australia | 1 April to 31 October 2011 to 2013 | Retrospective cohort study | 491 | NR | 5.1 (1.9) weeks | NR | 56 | Paediatric patients hospitalised with bronchiolitis | Fair |
| Patwari et al., 1991 [16] | India | January 1989–December 1989 | Retrospective chart review | 5996 | 0–5 years | NR | NR | 64.9 | Paediatric patients who attended hospital with diarrhoea | Fair |
| Perl et al., 2011 [24] | Israel | 1 April 2004–31 March 2006 | Retrospective chart review | 533 | NR | 21.7 (31) months | 13 months | 56.5 | Paediatric patients hospitalised with acute gastroenteritis, rotavirus gastroenteritis, and diarrhoea and vomiting | Good |
| Redondo-Gonzalez et al., 2016 [25] | Spain | 1 January 2003–31 December 2009 | Retrospective cohort study | 17,415 | 7 months–≥14 years | NR | NR | 53.4 | Paediatric patients hospitalised with acute gastroenteritis | Fair |
| Spiller et al., 2009 [39] | USA | 2000–2007 | Retrospective chart review | 137 | 1–82 years | 22 (NR) years | NR | 38 | Adult patients who had single substance ingestion of modafanil | Fair |
| Hasan et al., 2021 [40] | Bangladesh | 2 April 2018–12 May 2018 | Retrospective chart review | 1531 | 0–≥ 30 years | NR | NR | 58.4 | Paediatric and adult patients hospitalised with diarrhoea during epidemic | Good |
| Tewari et al., 2018 [37] | New Delhi | May 2013–September 2013 | Prospective cohort study | 500 | 6 months to 77 years | NR | NR | 53.9 | Paediatric and adult patients hospitalised with fever and other signs of dengue | Fair |
| Thronaes et al., 2021 [35] | Norway | 15 January 2019–15 January 2020 | Prospective longitudinal study | 451 | NR | 68.9 (13.1) years | NR | 60.3 | Adult patients with incurable cancer | Fair |
| Tseng et al., 2018 [42] | USA | January 2010–January 2017 | Retrospective cohort study | 332 | NR | 29.3 (9.5) years | NR | 10 | Adult patients’ postural tachycardia syndrome | Fair |
| Waisbourd-Zinman et al., 2008 [26] | Israel | 1 January 2003–31 December 2006 | Prospective cohort study | 356 | NR | 14.6 (24.7) months | 9 months | 54.5 | Paediatric patients hospitalised with nosocomial rotavirus gastroenteritis | Fair |
| Wathen, MacKenzie and Bothner, 2004 [28] | USA | January–October, 2004 | Prospective cohort study | 182 | 2.7 months to 8.5 years | 1.4 years | 51 | Paediatric patients presenting at the hospital with gastroenteritis and dehydration | Fair | |
| Wildi-Runge et al., 2009 [27] | Switzerland | July 2002–March 2006 | Retrospective chart review | 539 | NR | 1.4 (NR) years | NR | 55.6 | Paediatric patients hospitalised with rotavirus gastroenteritis | Fair |
3.3. Frequency of Intravenous Rehydration in Paediatric Patients
3.4. Frequency of Intravenous Rehydration in Adult Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoorn, E.J. Intravenous fluids: Balancing solutions. J. Nephrol. 2016, 30, 485–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brossier, D.W.; Tume, L.N.; Briant, A.R.; Chaparro, C.J.; Moullet, C.; Rooze, S.; Verbruggen, S.C.A.T.; Marino, L.V.; Alsohime, F.; Beldjilali, S.; et al. ESPNIC clinical practice guidelines: Intravenous maintenance fluid therapy in acute and critically ill children—A systematic review and meta-analysis. Intensiv. Care Med. 2022, 48, 1691–1708. [Google Scholar] [CrossRef] [PubMed]
- Rudnick, M.R.; Fay, K.; Wahba, I.M. Fluid administration strategies for the prevention of contrast-associated acute kidney injury. Curr. Opin. Nephrol. Hypertens. 2022, 31, 414–424. [Google Scholar] [CrossRef] [PubMed]
- Hwa, Y.L.; Kull, M.R. The why and how of maintaining hydration during cancer therapy. Curr. Opin. Support. Palliat. Care 2020, 14, 324–332. [Google Scholar] [CrossRef]
- Wood, C. Fluid management: An update for perioperative practitioners. J. Perioper. Pr. 2021, 31, 71–79. [Google Scholar] [CrossRef]
- Frost, P. Intravenous fluid therapy in adult inpatients. BMJ 2014, 350, g7620. [Google Scholar] [CrossRef] [Green Version]
- Crosignani, A.; Spina, S.; Marrazzo, F.; Cimbanassi, S.; Malbrain, M.L.N.G.; Van Regenemortel, N.; Fumagalli, R.; Langer, T. Intravenous fluid therapy in patients with severe acute pancreatitis admitted to the intensive care unit: A narrative review. Ann. Intensiv. Care 2022, 12, 1–15. [Google Scholar] [CrossRef]
- Bruno, C.; Collier, A.; Holyday, M.; Lambert, K. Interventions to Improve Hydration in Older Adults: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3640. [Google Scholar] [CrossRef]
- Xiao, H.; Barber, J.; Campbell, E.S. Economic burden of dehydration among hospitalized elderly patients. Am. J. Health Pharm. 2004, 61, 2534–2540. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ Br. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP Checklists. 2022. Available online: https://casp-uk.net/ (accessed on 15 September 2022).
- Critical Appraisal Skills Programme. CASP Cohort Study Checklist. 2022. Available online: https://casp-uk.net/images/checklist/documents/CASP-Cohort-Study-Checklist/CASP-Cohort-Study-Checklist_2018.pdf (accessed on 15 September 2022).
- Akech, S.; Ayieko, P.; Gathara, D.; Agweyu, A.; Irimu, G.; Stepniewska, K.; English, M.; Ngarngar, S.; Aduro, N.; Mutai, L.; et al. Risk factors for mortality and effect of correct fluid prescription in children with diarrhoea and dehydration without severe acute malnutrition admitted to Kenyan hospitals: An observational, association study. Lancet Child Adolesc. Health 2018, 2, 516–524. [Google Scholar] [CrossRef]
- Chow, C.; Choi, K.; Nelson, E.A.S.; Chan, P.; Mast, T.C.; Distefano, D.; Tam, J.S.; Bresee, J.S. Use of intravenous fluids in Hong Kong children hospitalised for diarrhoea and relationship to severity and aetiology. Vaccine 2009, 27, F55–F60. [Google Scholar] [CrossRef] [PubMed]
- Heymann, D.L.; Mbvundula, M.; Macheso, A.; McFarland, D.A.; Hawkins, R.V. Oral rehydration therapy in Ma-lawi: Impact on the severity of disease and on hospital admissions, treatment practices, and recurrent costs. Bull. World Health Organ. 1990, 68, 193–197. [Google Scholar]
- Patwari, A.K.; Kumar, H.; Anand, V.K.; Aneja, S.; Sharma, D. Diarrhea training and treatment unit: Experience from a teaching hospital. Indian J. Pediatr. 1991, 58, 775–781. [Google Scholar] [CrossRef]
- Abdul-Mumin, A.; Ervin, S.; Halvorson, E.E. Clinical characteristics associated with increased resource utilization of hospitalized children under 5 years with acute gastroenteritis at a tertiary hospital in the northern region of Ghana: A retrospective study. Pan Afr. Med. J. 2019, 33, 186. [Google Scholar] [CrossRef] [PubMed]
- Dbaibo, G.; Rajab, M.; Inati, A.; Mikhael, R.; Choueiry, E.; Al-Tannir, M.; Salam, O.; Ramakrishnan, G.; DeAntonio, R. Hospital-based surveillance study of rotavirus gastroenteritis in children under 5 years of age in Lebanon. Trials Vaccinol. 2013, 2, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Freedman, S.B.; Hall, M.; Shah, S.S.; Kharbanda, A.B.; Aronson, P.L.; Florin, T.A.; Mistry, R.D.; Macias, C.G.; Neuman, M.I. Impact of Increasing Ondansetron Use on Clinical Outcomes in Children With Gastroenteritis. JAMA Pediatr. 2014, 168, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Moineau, G.; Newman, J. Rapid intravenous rehydration in the pediatric emergency department. Pediatr. Emerg. Care 1990, 6, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Myat, T.W.; Thu, H.M.; Tate, J.E.; Burnett, E.; Cates, J.E.; Parashar, U.D.; Kyaw, Y.M.; Khaing, T.E.E.; Moh, K.M.; Win, N.N.; et al. Rotavirus infection among children under five years of age hospitalized with acute gastroenteritis in Myanmar during 2018–2020—Multicentre surveillance before rotavirus vaccine introduction. Vaccine 2021, 39, 6907–6912. [Google Scholar] [CrossRef]
- Nazurdinov, A.B.; Azizov, Z.A.; Tishkova, F.; Turkov, S.M.; Daniels, D.S.; Leshem, E. Rotavirus hospitalizations among children <5 years of age-Tajikistan, 2013–2014. Vaccine 2018, 36, 7794–7797. [Google Scholar]
- Perl, S.; Goldman, M.; Berkovitch, M.; Kozer, E. Characteristics of rotavirus gastroenteritis in hospitalized children in Israel. Isr. Med. Assoc. J. IMAJ 2011, 13, 274–277. [Google Scholar] [PubMed]
- Redondo-González, O.; Tenías-Burillo, J.M. A multifactorial regression analysis of the features of community-acquired rotavirus requiring hospitalization in Spain as represented in the Minimum Basic Data Set. Epidemiol. Infect. 2016, 144, 2509–2516. [Google Scholar] [CrossRef] [PubMed]
- Waisbourd-Zinman, O.; Ben-Ziony, S.; Solter, E.; Scherf, E.; Samra, Z.; Ashkenazi, S. Hospitalizations for nosocomial rotavirus gastroenteritis in a tertiary pediatric center: A 4-year prospective study. Am. J. Infect. Control 2009, 37, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Wildi-Runge, S.; Allemann, S.; Schaad, U.B.; Heininger, U. A 4-year study on clinical characteristics of children hospitalized with rotavirus gastroenteritis. Eur. J. Pediatr. 2009, 168, 1343–1348. [Google Scholar] [CrossRef]
- Wathen, J.E.; MacKenzie, T.; Bothner, J.P. Usefulness of the Serum Electrolyte Panel in the Management of Pediatric Dehydration Treated With Intravenously Administered Fluids. Pediatrics 2004, 114, 1227–1234. [Google Scholar] [CrossRef]
- Ben-Shalom, E.; Toker, O. and Schwartz, S. Hypernatremic Dehydration in Young Children: Is There a Solution? Isr. Med. Assoc. J. IMAJ 2016, 18, 95–99. [Google Scholar]
- Janet, S.; Molina, J.C.; Marañon, R.; García-Ros, M. Effects of Rapid Intravenous Rehydration in Children With Mild-to-Moderate Dehydration. Pediatr. Emerg. Care 2015, 31, 564–567. [Google Scholar] [CrossRef]
- Kao, W.-T.; Tseng, Y.-H.; Jong, Y.-J.; Chen, T.-H. Emergency room visits and admission rates of children with neuromuscular disorders: A 10-year experience in a medical center in Taiwan. Pediatr. Neonatol. 2019, 60, 405–410. [Google Scholar] [CrossRef] [Green Version]
- Fikrie, A.; Alemayehu, A.; Gebremedhin, S. Treatment outcomes and factors affecting time-to-recovery from severe acute malnutrition in 6–59 months old children admitted to a stabilization center in Southern Ethiopia: A retrospective cohort study. Ital. J. Pediatr. 2019, 45, 46. [Google Scholar] [CrossRef]
- Lopez-Medina, E.; Ardura, M.I.; Siegel, J.D.; Brock, E.; Sánchez, P.J. 2009 Influenza A in Infants Hospitalized at Younger than 6 Months. J. Pediatr. 2012, 160, 626–631.e1. [Google Scholar] [CrossRef]
- Oakley, E.; Bata, S.; Rengasamy, S.; Krieser, D.; Cheek, J.; Jachno, K.; Babl, F.E. Nasogastric Hydration in Infants with Bronchiolitis Less Than 2 Months of Age. J. Pediatr. 2016, 178, 241–245.e1. [Google Scholar] [CrossRef] [PubMed]
- Thronæs, M.; Løhre, E.T.; Kvikstad, A.; Brenne, E.; Norvaag, R.; Aalberg, K.O.; Moen, M.K.; Jakobsen, G.; Klepstad, P.; Solberg, A.; et al. Interventions and symptom relief in hospital palliative cancer care: Results from a prospective longitudinal study. Support. Care Cancer 2021, 29, 6595–6603. [Google Scholar] [CrossRef] [PubMed]
- Marra, A.R.; De Matos, G.F.J.; Janeri, R.D.; Machado, P.S.; Schvartsman, C.; Dos Santos, O.F.P. Managing patients with dengue fever during an epidemic: The importance of a hydration tent and of a multidisciplinary approach. BMC Res. Notes 2011, 4, 335. [Google Scholar] [CrossRef] [PubMed]
- Tewari, V.V.; Tewari, K.; Mehta, R. Clinical and hematological profile of patients with dengue fever at a tertiary care hospital—An observational study. Mediterr. J. Hematol. Infect. Dis. 2017, 10, e2018021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blacklock, A.; Sesay, A.; Kamara, A.; Kamara, M.; Blacklock, C. Characteristics and clinical management of patients admitted to cholera wards in a regional referral hospital during the 2012 epidemic in Sierra Leone. Glob. Health Action 2015, 8, 25266. [Google Scholar] [CrossRef] [Green Version]
- Spiller, H.A.; Borys, D.; Griffith, J.R.; Klein-Schwartz, W.; Aleguas, A.; Sollee, D.; Anderson, D.A.; Sawyer, T.S. Toxicity from modafinil ingestion. Clin. Toxicol. 2009, 47, 153–156. [Google Scholar] [CrossRef]
- Hasan, S.M.T.; Das, S.; Faruque, A.S.G.; Khan, A.I.; Clemens, J.D.; Ahmed, T. Taking care of a diarrhea epidemic in an urban hospital in Bangladesh: Appraisal of putative causes, presentation, management, and deaths averted. PLOS Neglected Trop. Dis. 2021, 15, e0009953. [Google Scholar] [CrossRef]
- Machado, M.C.; Bruce-Mensah, A.; Whitmire, M.; Rizvi, A.A. Hypercalcemia Associated with Calcium Supplement Use: Prevalence and Characteristics in Hospitalized Patients. J. Clin. Med. 2015, 4, 414–424. [Google Scholar] [CrossRef] [Green Version]
- Tseng, A.S.; Traub, N.A.; Harris, L.A.; Crowell, M.D.; Dnp, C.R.H.; Goodman, B.P.; DiBaise, J.K. Factors Associated With Use of Nonoral Nutrition and Hydration Support in Adult Patients With Postural Tachycardia Syndrome. J. Parenter. Enter. Nutr. 2018, 43, 734–741. [Google Scholar] [CrossRef]
- Cardenas, D. Ethical issues and dilemmas in artificial nutrition and hydration. Clin. Nutr. ESPEN 2020, 41, 23–29. [Google Scholar] [CrossRef]
- Alsolamy, S. Islamic Views on Artificial Nutrition and Hydration in Terminally Ill Patients. Bioethics 2012, 28, 96–99. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Treatment of Diarrhoea: A Manual for Physicians and Other Senior Health Workers, 4th Revision. 2005. Available online: https://www.who.int/publications/i/item/9241593180 (accessed on 15 September 2022).
- Ozuah, P.O.; Avner, J.R.; Stein, R.E.K. Oral Rehydration, Emergency Physicians, and Practice Parameters: A National Survey. Pediatrics 2002, 109, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Conners, G.P.; Barker, W.H.; Mushlin, A.I.; Goepp, J.G.K. Oral versus intravenous: Rehydration preferences of pediatric emergency medicine fellowship directors. Pediatr. Emerg. Care 2000, 16, 335–338. [Google Scholar] [CrossRef] [PubMed]

| Author, Year | Sample Size | Exposure Group n (%) | Comparator Group n (%) | Overall n (%) | Effect Size | Population |
|---|---|---|---|---|---|---|
| Chow et al., 2009 [14] | 7391 | 3548 (48%) | - | - | - | Paediatric patients admitted to the hospital with diagnosis of diarrhoea |
| Patwari et al., 1991 [16] | 5996 | 366 (6.1%) | - | - | - | Paediatric patients who came to the hospital with diarrhoea |
| Akech et al., 2018 [13] | 8025 | 3569 (45%) | - | - | - | Paediatric patients hospitalised with diarrhoea and dehydration |
| Heyman et al., 1990 [15] | 3495 | 1310 (37.5%) | - | - | - | Paediatric patients hospitalised with diarrhoea or gastroenteritis |
| Abdul-Mumin, Ervin and Halvorson, 2019 [17] | 473 | 365 (77%) | - | - | - | Paediatric patients hospitalised with acute gastroenteritis |
| Freedman et al., 2014 [19] | 804,000 | 148,780 (18.5%) | - | - | - | Paediatric patients who were diagnosed as having gastroenteritis in an emergency department |
| Moineau and Newman, 1990 [20] | 17 | 17 (100%) | - | - | - | Paediatric patients admitted to the emergency department with mild to moderate dehydration caused by viral gastroenteritis |
| Wathen, MacKenzie and Bothner, 2004 [27] | 182 | 182 (100%) | - | - | - | Paediatric patients presenting at the hospital with gastroenteritis and dehydration |
| Waisbourd-Zinman et al., 2008 [25] | 356 | 239 (67%) | - | - | - | Paediatric patients hospitalised with nosocomial rotavirus gastroenteritis |
| Perl et al., 2011 [23] | 533 | Rotavirus positive (n = 202) 187 (92%) | Rotavirus negative (n = 331) 249 (75%) | 436 (82%) | 4.06 (2.28–7.21) | Paediatric patients hospitalised with acute gastroenteritis, rotavirus gastroenteritis, and diarrhoea, and vomiting |
| Dbaibo et al., 2013 [18] | 491 | Rotavirus positive (n = 136) 136 (100%) | Rotavirus negative (n = 351) 351 (96.3%) | 491 (97.4%) | p = 0.0234 | Paediatric patients hospitalised with a diagnosis of acute gastroenteritis |
| Nazurdinov et al., 2018 [22] | 2863 | Rotavirus positive (n = 1207) 1097 (91%) | Rotavirus negative (n = 1656) 1433 (87%) | 2530 (88.5%) | NR | Paediatric patients hospitalised with acute gastroenteritis and rotavirus. |
| Myat et al., 2021 [21] | 2977 | Rotavirus positive (n = 1320) 770 (58.3%) | Rotavirus negative (n = 1657) 880 (53.1%) | 1650 (55.5%) | <0.01 | Paediatric patients hospitalised for acute gastroenteritis |
| Redondo-Gonzalez et al., 2016 [24] | 17,415 | Rotavirus positive (n = 1657) 75 (4.5%) | Rotavirus negative (n = 15,758) 230 (1.6%) | NR | 3.2 (2.46–4.18) | Paediatric patients hospitalised with acute gastroenteritis |
| Wildi-Runge, 2009 [26] | 539 | 378 (70.1%) | - | - | - | Paediatric patients hospitalised with rotavirus gastroenteritis |
| Ben- Shalom et al., 2016 [28] | 58 | 58 (100%) | - | - | - | Paediatric patients hospitalised with hypernatremic dehydration |
| Janet et al., 2015 [29] | 83 | 83 (100%) | - | - | - | Paediatric patients with mild-to moderate isonatremic dehydration |
| Lopez-Medina et al., 2012 [32] | 73 | 39 (53%) | - | - | - | Paediatric patients hospitalised with laboratory-confirmed influenza |
| Kao et al., 2019 [30] | 44 | 69 (34%) | - | - | - | Paediatric patients with chronic neuromuscular disorder who visited the emergency room |
| Fikrie, Alemayehu and Gebremedhin, 2019 [31] | 381 | 87 (22.8%) | - | - | - | Paediatric patients hospitalised with Severe Acute Malnutrition |
| Oakley et al., 2016 [33] | 491 | 65 (31%) | - | - | - | Paediatric patients hospitalised with bronchiolitis |
| Hasan et al., 2021 [39] | 1531 | Patients during 2018 epidemic (n = 562) 333 (59.3%) | Patients during the seasonally matched periods (n = 969) 450 (46.4%) | 783 (51%) | OR 95%CI 1.7 (1.4–2.1) | Paediatric and adult patients hospitalised with diarrhoea during epidemic |
| Marra et al., 2011 [35] | 3393 | 824 (24.3%) | - | - | - | Paediatric and adult patients treated in the hydration tent during dengue fever epidemic |
| Tewari et al., 2018 [36] | 500 | 45 (9.2%) | - | - | - | Paediatric and adult patients hospitalised with fever and other signs of dengue |
| Thronaes et al., 2021 [34] | 451 | 203 (45%) | - | - | - | Adult patients with incurable cancer |
| Spiller et al., 2009 [38] | 137 | 2 (1.5%) | - | - | - | Adult patients who had single substance ingestion of modafanil |
| Blacklock et al., 2015 [37] | 798 | 767 (96.1%) | - | - | - | Paediatric and adult patients hospitalised with cholera during the epidemic |
| Machado et al., 2015 [40] | 72 | Calcium supplement syndrome positive (n = 15) 15 (100%) | Calcium supplement syndrome negative (n = 57) 0 (0%) | 15 (22%) | NR | Patients hospitalised with hypercalcemia |
| Tseng et al., 2018 [41] | 332 | 21 (6.3%) | - | - | - | Adult patients with postural tachycardia syndrome |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gawronska, J.; Koyanagi, A.; López Sánchez, G.F.; Veronese, N.; Ilie, P.C.; Carrie, A.; Smith, L.; Soysal, P. The Prevalence and Indications of Intravenous Rehydration Therapy in Hospital Settings: A Systematic Review. Epidemiologia 2023, 4, 18-32. https://doi.org/10.3390/epidemiologia4010002
Gawronska J, Koyanagi A, López Sánchez GF, Veronese N, Ilie PC, Carrie A, Smith L, Soysal P. The Prevalence and Indications of Intravenous Rehydration Therapy in Hospital Settings: A Systematic Review. Epidemiologia. 2023; 4(1):18-32. https://doi.org/10.3390/epidemiologia4010002
Chicago/Turabian StyleGawronska, Julia, Ai Koyanagi, Guillermo F. López Sánchez, Nicola Veronese, Petre Cristian Ilie, Anne Carrie, Lee Smith, and Pinar Soysal. 2023. "The Prevalence and Indications of Intravenous Rehydration Therapy in Hospital Settings: A Systematic Review" Epidemiologia 4, no. 1: 18-32. https://doi.org/10.3390/epidemiologia4010002