
Clinical Features of Transient Growth Hormone Deficiency

Abstract
:1. Introduction
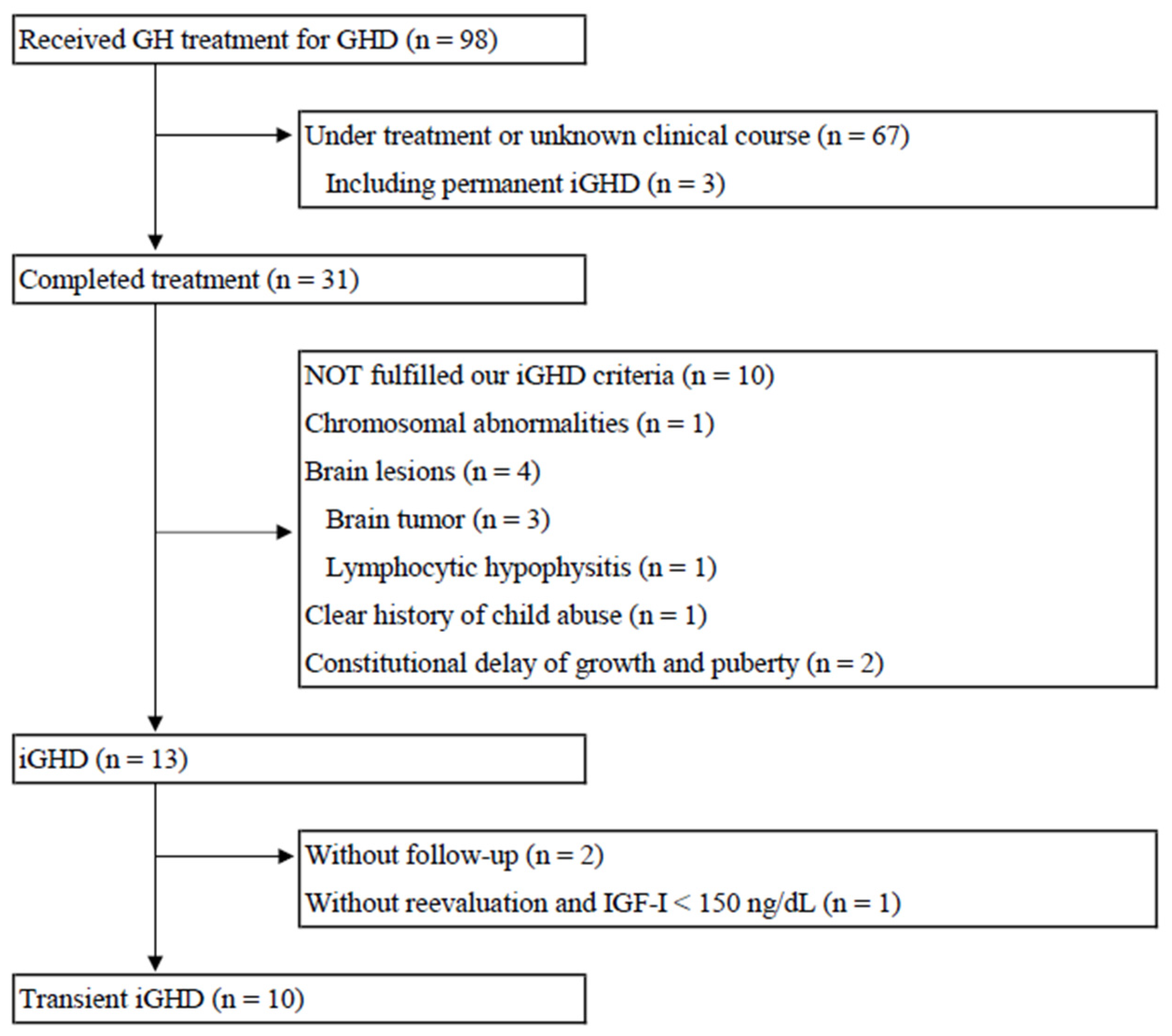
2. Materials and Methods
- pre-treatment height < −2.0 SD
- pre-treatment height velocity < 0 SD
- pre-treatment IGF-I value < −2.0 SD
- at least two GHSTs with a peak value < 6.0 ng/mL
- improvement in height velocity (>1.0 SD) after GH treatment
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jorge, A.A.L.; Grimberg, A.; Dattani, M.T.; Baron, J. Disorders of Childhood Growth. In Sperling Pediatric Endocrinology, 5th ed.; Sperling, M.A., Ed.; Elsevier: Philadelphia, PA, USA, 2020; pp. 299–356. [Google Scholar]
- Bonert, V.S.; Melmed, S. Growth Hormone. In The Pituitary, 4th ed.; Melmed, S., Ed.; Academic Press: London, UK, 2017; pp. 85–127. [Google Scholar]
- Cacciari, E.; Tassoni, P.; Parisi, G.; Pirazzoli, P.; Zucchini, S.; Mandini, M.; Cicognani, A.; Balsamo, A. Pitfalls in diagnosing impaired growth hormone (GH) secretion: Retesting after replacement therapy of 63 patients defined as GH deficient. J. Clin. Endocrinol. Metab. 1992, 74, 1284–1289. [Google Scholar] [PubMed]
- Maghnie, M.; Strigazzi, C.; Tinelli, C.; Autelli, M.; Cisternino, M.; Loche, S.; Severi, F. Growth hormone (GH) deficiency (GHD) of childhood onset: Reassessment of GH status and evaluation of the predictive criteria for permanent GHD in young adults. J. Clin. Endocrinol. Metab. 1999, 84, 1324–1328. [Google Scholar] [CrossRef]
- Lee, N.Y.; Kim, S.E.; Kim, S.; Ahn, M.B.; Kim, S.H.; Cho, W.K.; Cho, K.S.; Jung, M.H.; Suh, B.-K. Effect of body mass index on peak growth hormone level after growth hormone stimulation test in children with short stature. Ann. Pediatr. Endocrinol. Metab. 2021, 26, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Abawi, O.; Augustijn, D.; Hoeks, S.E.; de Rijke, Y.B.; Akker, E.L.T.V.D. Impact of body mass index on growth hormone stimulation tests in children and adolescents: A systematic review and meta-analysis. Crit. Rev. Clin. Lab. Sci. 2021, 58, 576–595. [Google Scholar] [CrossRef]
- Yang, A.; Cho, S.Y.; Kwak, M.J.; Kim, S.J.; Park, S.W.; Jin, D.-K.; Lee, J.-E. Impact of BMI on peak growth hormone responses to provocative tests and therapeutic outcome in children with growth hormone deficiency. Sci. Rep. 2019, 9, 16181. [Google Scholar] [CrossRef]
- Beas, F.; Contreras, I.; Maccioni, A.; Arenas, S. Growth hormone in infant malnutrition: The arginine test in marasmus and kwashiorkor. Br. J. Nutr. 1971, 26, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Rogol, A.D. Emotional Deprivation in Children: Growth Faltering and Reversible Hypopituitarism. Front. Endocrinol. 2020, 11, 596144. [Google Scholar] [CrossRef] [PubMed]
- Winter, W.E. Laboratory evaluation of short stature in children. In Handbook of Diagnostic Endocrinology, 3rd ed.; Winter, W.E., Ed.; Academic Press: London, UK, 2021; pp. 497–541. [Google Scholar]
- Marin, G.; Domené, H.M.; Barnes, K.M.; Blackwell, B.J.; Cassorla, F.G.; Cutler, G.B. The effects of estrogen priming and puberty on the growth hormone response to standardized treadmill exercise and arginine-insulin in normal girls and boys. J. Clin. Endocrinol. Metab. 1994, 79, 537–541. [Google Scholar]
- Gourmelen, M.; Pham-Huu-Trung, M.T.; Girard, F. Transient partial hGH deficiency in prepubertal children with delay of growth. Pediatr. Res. 1979, 13, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Kashimada, K.; Onishi, T.; Ono, M.; Miyai, K.; Ohta, M.; Mizutani, S. A boy with “transient” growth hormone deficiency in prepubertal stage despite normal growth hormone secretion in childhood and after puberty. Endocr. J. 2007, 54, 1015–1019. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Hasegawa, T.; Kotoh, S.; Tsuchiya, Y. Ratio of False Positive Results of Growth Hormone Stimulation Tests (Arginine and Insulin). Clin. Pediatr. Endocrinol. 1993, 2, 65–67. [Google Scholar] [CrossRef] [Green Version]
- Van den Broeck, J.; Hering, P.; VandeLely, A.J.; Hokken-Koelega, A. Interpretative difficulties with growth hormone provocative retesting in childhood-onset growth hormone deficiency. Horm Res. 1999, 51, 1–9. [Google Scholar]
- Isojima, T.; Shimatsu, A.; Yokoya, S.; Chihara, K.; Tanaka, T.; Hizuka, N.; Teramoto, A.; Tatsumi, K.-I.; Tachibana, K.; Katsumata, N.; et al. Standardized centile curves and reference intervals of serum insulin-like growth factor-I (IGF-I) levels in a normal Japanese population using the LMS method. Endocr. J. 2012, 59, 771–780. [Google Scholar] [CrossRef]
- Matsuo, N. Skeletal and sexual maturation in Japanese children. Clin. Pediatr. Endocrinol. 1993, 2, 1–4. [Google Scholar] [CrossRef]
- Becker, P.J.; Nieman Carney, L.; Corkins, M.R.; Monczka, J.; Smith, E.; Smith, S.E.; Spear, B.A.; White, J.V. Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: Indicators recommended for the identification and documentation of pediatric malnutrition (undernutrition). J. Acad. Nutr. Diet. 2014, 114, 1988–2000. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software ‘EZR’ for Medical Statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Isojima, T.; Kato, N.; Ito, Y.; Kanzaki, S.; Murata, M. Growth standard charts for Japanese children with mean and standard deviation (SD) values based on the year 2000 national survey. Clinic Pediatr. Endocrinol. 2016, 25, 71–76. [Google Scholar] [CrossRef]
- Tauber, M.; Moulin, P.; Pienkowski, C.; Jouret, B.; Rochiccioli, P. Growth hormone (GH) retesting and auxological data in 131 GH-deficient patients after completion of treatment. J Clin Endocrinol. Metab. 1997, 82, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Loche, S.; Bizzarri, C.; Maghnie, M.; Faedda, A.; Tzialla, C.; Autelli, M.; Casini, M.R.; Cappa, M. Results of early reevaluation of growth hormone secretion in short children with apparent growth hormone deficiency. J Pediatr. 2002, 140, 445–449. [Google Scholar] [CrossRef]
- Zucchini, S.; Pirazzoli, P.; Baronio, F.; Gennari, M.; Bal, M.O.; Balsamo, A.; Gualandi, S.; Cicognani, A. Effect on adult height of pubertal growth hormone retesting and withdrawal of therapy in patients with previously diagnosed growth hormone deficiency. J. Clin. Endocrinol. Metab. 2006, 91, 4271–4276. [Google Scholar] [CrossRef]
- Smyczyńska, J.; Stawerska, R.; Lewiński, A.; Hilczer, M. Incidence and predictors of persistent growth hormone deficiency (GHD) in patients with isolated, childhood-onset GHD. Endokrynol. Pol. 2014, 65, 334–341. [Google Scholar] [CrossRef]
- Vuralli, D.; Gonc, E.N.; Ozon, Z.A.; Alikasifoglu, A.; Kandemir, N. Clinical and laboratory parameters predicting a requirement for the reevaluation of growth hormone status during growth hormone treatment: Retesting early in the course of GH treatment. Growth Horm. IGF Res. 2017, 34, 31–37. [Google Scholar] [CrossRef]
- Penta, L.; Cofini, M.; Lucchetti, L.; Zenzeri, L.; Leonardi, A.; Lanciotti, L.; Galeazzi, D.; Verrotti, A.; Esposito, S. Growth Hormone (GH) Therapy During the Transition Period: Should We Think About Early Retesting in Patients with Idiopathic and Isolated GH Deficiency? Int J Environ. Res. Public Health 2019, 16, 307. [Google Scholar] [CrossRef] [PubMed]
- Cooke, D.W.; DiVall, S.A.; Radovick, S. Normal and Aberrant Growth in Children. In Williams Textbook of Endocrinology, 14th ed.; Melmed, S., Ed.; Elsevier: Philadelphia, PA, USA, 2020; pp. 937–1022. [Google Scholar]
- Sari, Y.O.; Aminuddin, A.; Hamid, F.; Prihantono, P.; Bahar, B.; Hadju, V. Malnutrition in children associated with low growth hormone (Gh) Levels. Gac. Sanit. 2021, 35, S327–S329. [Google Scholar] [CrossRef] [PubMed]
- Ali, O. Short Stature. In Nelson Pediatric Symptom-Based Diagnosis; Kliegman, R.M., Ed.; Elsevier: Philadelphia, PA, USA, 2018; pp. 791–810. [Google Scholar]
- Fliers, E.; Boelen, A. An update on non-thyroidal illness syndrome. J. Endocrinol. Invest. 2021, 44, 1597–1607. [Google Scholar] [CrossRef] [PubMed]
- Tamai, H.; Mori, K.; Matsubayashi, S.; Kiyohara, K.; Nakagawa, T.; Okimura, M.C.; Walter, J.R.M.; Kumagai, L.F.; Nagataki, S. Hypothalamic-pituitary-thyroidal dysfunctions in anorexia nervosa. Psychother. Psychosom. 1986, 46, 127–131. [Google Scholar] [CrossRef]
- Krassas, G.E. Endocrine abnormalities in Anorexia Nervosa. Pediatr. Endocrinol. Rev. 2003, 1, 46–54. [Google Scholar]
- Gwirtsman, H.E.; Kaye, W.H.; George, D.T.; Jimerson, D.C.; Ebert, M.H.; Gold, P.W. Central and peripheral ACTH and cortisol levels in anorexia nervosa and bulimia. Arch. Gen. Psychiatry 1989, 46, 61–69. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients with Transient iGHD (n = 10) | |
|---|---|
| Pre-treatment | |
| Age at the start of treatment | 6.1 (5.3~8.5) |
| Height velocity SD score | −4.1 (−4.9~−3.4) |
| Height SD score | −3.0 (−3.9~−2.8) |
| BMI SD score | −1.0 (−2.6~−0.3) |
| IGF-I SD score | −3.1 (−3.3~−2.3) |
| One year after the start of treatment | |
| Height velocity (cm/year) | 9.2 (8.0~10.2) |
| ⊿SD Height | 0.7 (0.6~1.1) |
| ⊿SD BMI | 0.1 (−0.1~0.4) |
| Post-treatment | |
| Age at the completion of treatment | 16.8 (14.7~17.4) |
| Treatment period | 10.6 (7.3~12.3) |
| IGF-I SD score | −1.3 (−1.6~−0.8) |
| Low BMI (n = 5) | Non-Low BMI (n = 5) | |
|---|---|---|
| Pre-treatment | ||
| Age at the start of treatment | 8.9 (1.8~11.3) | 5.5 (5.3~6.7) |
| Height velocity SD score | −4.8 (−5.2~−3.6) | −4.1 (−4.1~−3.4) |
| Height SD score | −3.1 (−4.1~−2.8) | −2.9 (−3.4~−2.8) |
| BMI SD score * | −2.8 (−2.9~−2.2) | 0.3 (−0.4~0.4) |
| IGF-I SD score | −3.1(−3.1~−2.2) | −3.3 (−3.6~−2.3) |
| Average peak value of GHSTs | 3.4 (2.7~4.3) | 3.6 (3.5~3.9) |
| Two GHSTs with a peak value < 3 ng/mL | n = 1 | n = 1 |
| One year after the start of treatment | ||
| Height velocity (cm/year) | 9.3 (7.9~10.3) | 9.1 (8.1~10.0) |
| ⊿SD Height | 0.6 (0.4~1.1) | 0.8 (0.6~1.0) |
| ⊿SD BMI | 0.5 (0.4~1.6) | 0.1 (−1.0~0.1) |
| Post-treatment | ||
| IGF-I SD score | −1.2 (−1.7~−1.2) | −1.4 (−1.6~−0.7) |
| Other hormone replacement | n = 3 | n = 0 |
| tGHD (%) | Reevaluation | Subject | Distinctive Criteria * | |
|---|---|---|---|---|
| M Tauber et al., 1997 [21] | 81/121 (67) | During the first year after completion of treatment | Idiopathic GHD Auxological criteria was not described | Excluding malnutrition |
| Loche S et al., 2000 [22] | 28/33 (84) | One to six months after diagnosis None of the children received treatment | Isolated and idiopathic GHD Height ≤ −2 SD Decreased HV (<25th %tile) SS relative to mid-parental height | Exclusion criteria was not described |
| Zucchini S et al., 2006 [23] | 25/69 (36.2) | Four to six weeks after interruption of treatment Testicular volume 6–12 mL (males) Breast development 2–3 (females) | Isolated and idiopathic GHD Height < 3rd %tile Height < 10th %tile with TH > 50th %tile Decreased HV < 25th %tile No signs of puberty | Excluding MPHD and age at diagnosis < 6 year |
| Smyczyńska J et al., 2014 [24] | 132/150 (88) | At least one month after completion of treatment | Isolated and idiopathic GHD Height < 3rd %tile | Excluding MPHD |
| Vuralli et al., 2017 [25] | 69/170 (40.6) | At the end of the first year of treatment | Isolated GHD Height < −2 SD Decreased HV (<25th %tile) Delayed BA (2 SD below the CA) | Including 21 patients with brain tumor |
| L Penta et al., 2019 [26] | 26/31 (83.9) | At least three months after completion of treatment | Isolated and idiopathic GHD Auxological criteria was not described | Excluding MPHD |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakai, Y.; Ikegawa, K.; Shimura, K.; Hasegawa, Y. Clinical Features of Transient Growth Hormone Deficiency. Endocrines 2023, 4, 102-109. https://doi.org/10.3390/endocrines4010009
Sakai Y, Ikegawa K, Shimura K, Hasegawa Y. Clinical Features of Transient Growth Hormone Deficiency. Endocrines. 2023; 4(1):102-109. https://doi.org/10.3390/endocrines4010009
Chicago/Turabian StyleSakai, Yuki, Kento Ikegawa, Kazuhiro Shimura, and Yukihiro Hasegawa. 2023. "Clinical Features of Transient Growth Hormone Deficiency" Endocrines 4, no. 1: 102-109. https://doi.org/10.3390/endocrines4010009