

Evaluation of Adult Height in Patients with Non-Permanent Idiopathic GH Deficiency
 , ,
, ,
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Subjects
2.2. Methods
2.3. Assays
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ibba, A.; Loche, S. Diagnosis of GH deficiency without GH stimulation tests. Front. Endocrinol. 2022, 13, 853290. [Google Scholar] [CrossRef] [PubMed]
- Guzzetti, C.; Ibba, A.; Pilia, S.; Beltrami, N.; Iorgi, N.D.; Rollo, A.; Fratangeli, N.; Radetti, G.; Zucchini, S.; Maghnie, M.; et al. Cut-off limits of the peak GH response to stimulation tests for the diagnosis of GH deficiency in children and adolescents: Study in patients with organic GHD. Eur. J. Endocrinol. 2016, 175, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenbloom, A.L.; Ketan, P.; Inusha, P.; Navdeep, D.; Sabyasachi, S.; Preeti, K. Sex hormone priming for growth hormone stimulation testing in pre- and early adolescent children is evidence based. Horm. Res. Paediatr. 2011, 75, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Galazzi, E.; Improda, N.; Cerbone, M.; Soranna, D.; Moro, M.; Fatti, L.M.; Zambon, A.; Bonomi, M.; Salerno, M.; Dattani, M. Clinical benefits of sex steroids given as a priming prior to GH provocative test or as a growth-promoting therapy in peripubertal growth delays: Results of a retrospective study among ENDO-ERN centres. Clin. Endocrinol. 2021, 94, 219–228. [Google Scholar] [CrossRef]
- Krukowska-Andrzejczyk, B.; Kalina, M.; Kalina-Faska, B.; Małecka-Tendera, E. Growth hormone therapy in children with partial growth hormone deficiency. Are we treating the right patients? Pediatr. Endocrinol. Diabetes Metab. 2020, 26, 65–72. [Google Scholar] [CrossRef]
- Singh, A.; Ketan, P.; Inusha, P.; Navdeep, D.; Sabyasachi, S.; Preeti, K. Components of IGF-axis in growth disorders: A systematic review and patent landscape report. Endocrine 2022, 76, 509–525. [Google Scholar] [CrossRef]
- Grimberg, A.; DiVall, S.A.; Constantin, P.; Allen, D.B.; Cohen, L.E.; Quintos, J.B.; Rossi, W.C.; Feudtner, C.; Murad, M.H.; Drug and Therapeutics Committee and Ethics Committee of the Pediatric Endocrine Society. Guidelines for growth hormone and insulin-like growth factor-I treatment in children and adolescents: Growth hormone deficiency, idiopathic short stature, and primary insulin-like growth factor-I deficiency. Horm. Res. Paediatr. 2016, 86, 361–397. [Google Scholar] [CrossRef] [Green Version]
- Losa, M.; Castellino, L.; Pagnano, A.; Rossini, A.; Mortini, P.; Lanzi, R. Growth Hormone Therapy Does Not Increase the Risk of Craniopharyngioma and Nonfunctioning Pituitary Adenoma Recurrence. J. Clin. Endocrinol. Metab. 2020, 105, dgaa089. [Google Scholar] [CrossRef]
- Collett-Solberg, P.F.; Ambler, G.; Backeljauw, P.F.; Bidlingmaier, M.; Biller, B.M.K.; Boguszewski, M.C.S.; Cheung, P.T.; Choong, C.S.Y.; Cohen, L.E.; Cohen, P. Diagnosis, Genetics, and Therapy of Short Stature in Children: A Growth Hormone Research Society International Perspective. Horm. Res. Paediatr. 2019, 92, 1–14. [Google Scholar] [CrossRef]
- Kim, J.H.; Chae, H.K.; Chin, S.O.; Ku, C.R.; Park, K.H.; Lim, D.J.; Kim, K.J.; Lim, J.S.; Kim, S.; Choi, Y.M. Diagnosis and treatment of growth hormone deficiency: A position statement from Korean endocrine society and Korean society of pediatric endocrinology. Endocrinol. Metab. Seoul Korea 2020, 35, 272–287. [Google Scholar] [CrossRef]
- Binder, G.; Reinehr, T.; Ibáñez, L.; Thiele, S.; Linglart, A.; Woelfle, J.; Saenger, P.; Bettendorf, M.; Zachurzok, A.; Gohlke, S. GHD Diagnostics in Europe and the US: An Audit of National Guidelines and Practice. Horm. Res. Paediatr. 2019, 92, 150–156. [Google Scholar] [CrossRef]
- Growth Hormone Research Society. Consensus guidelines for the diagnosis and treatment of growth hormone (GH) deficiency in childhood and adolescence: Summary statement of the GH Research Society. GH Research Society. J. Clin. Endocrinol. Metab. 2000, 85, 3990–3993. [Google Scholar]
- Belen, A.; Jimenez, A.; Leiva, G.; Ollero, M.A.; Joes, M.; Siguero, L. Isolated Growth Hormone Deficiency and Idiopathic Short Stature: Comparative Efficiency after Growth Hormone Treatment up to Adult Height. J. Clin. Med. 2021, 10, 4988. [Google Scholar]
- Chaplin, J.E.; Berit, K.; Björn, J.; Maria, H.S.; Aronson, A.S.; Jovanna, D.; Kerstin, A.W. When do short children realize they are short? Prepubertal short children’s perception of height during 24 months of catch-up growth hormone treatment. Horm. Res. Paediatr. 2012, 77, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Vottero, A.; Guzzetti, C.; Loche, S. New aspects of the physiology of the GH-IGF-1 axis. Endocr. Dev. 2013, 24, 96–105. [Google Scholar] [PubMed]
- Tanner, J.M.; Whitehouse, R.H. Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch. Dis. Child. 1976, 51, 170–179. [Google Scholar] [CrossRef] [Green Version]
- Cacciari, E.; Milani, S.; Balsamo, A.; Spada, E.; Bona, G.; Cavallo, L.; Cerutti, F.; Gargantini, L.; Greggio, N.; Tonini, G. Italian cross-sectional growth charts for height, weight and BMI (2 to 20 yr). J. Endocrinol. Invest. 2006, 29, 581–593. [Google Scholar] [CrossRef]
- Bull, R.K.; Edwards, P.D.; Kemp, P.M.; Fry, S.; Hughes, I.A. Bone age assessment: A large scale comparison of the Greulich and Pyle, and Tanner and Whitehouse (TW2) methods. Arch. Dis. Child. 1999, 81, 172–173. [Google Scholar] [CrossRef] [Green Version]
- Elmlinger, M.W.; Kühnel, W.; Weber, M.M.; Ranke, M.B. Reference ranges for two automated chemiluminescent assays for serum insulin-like growth factor I (IGF-I) and IGF-binding protein 3 (IGFBP-3). Clin. Chem. Lab. Med. 2004, 42, 654–664. [Google Scholar] [CrossRef]
- Ibba, A.; Corrias, F.; Guzzetti, C.; Casula, L.; Salerno, M.; Iorgi, N.; Tornese, G.; Patti, G.; Radetti, G.; Maghnie, M. IGF1 for the diagnosis of growth hormone deficiency in children and adolescents: A reappraisal. Endocr. Connect. 2020, 9, 1095–1102. [Google Scholar] [CrossRef]
- Makimura, H.; Stanley, T.; Mun, D.; You, S.M.; Grinspoon, S. The Effects of Central Adiposity on Growth Hormone (GH) Response to GH-Releasing Hormone-Arginine Stimulation Testing in Men. J. Clin. Endocrinol. Metab. 2008, 93, 4254–4260. [Google Scholar] [CrossRef] [PubMed]
- Pozzobon, G.; Partenope, C.; Mora, M.; Garbetta, G.; Weber, G.; Barera, G. Growth hormone therapy in children: Predictive factors and short-term and long-term response criteria. Endocrine 2019, 66, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Reiter, E.O.; Price, D.A.; Wilton, P.; Albertsson-Wikland, K.; Ranke, M.B. Effect of growth hormone (GH) treatment on the near-final height of 1258 patients with idiopathic GH deficiency: Analysis of a large international database. J. Clin. Endocrinol. Metab. 2006, 91, 2047–2054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutfield, W.; Lindberg, A.; Wikland, K.A.; Chatelain, P.; Ranke, M.B.; Wilton, P. Final height in idiopathic growth hormone deficiency: The KIGS experience. Acta Paediatr. 1999, 88, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Bang, P.; Bjerknes, R.; Dahlgren, J.; Dunkel, L.; Gustafsson, J.; Juul, A.; Kriström, B.; Tapanainen, P.; Aberg, V. A comparison of different definitions of growth response in short prepubertal children treated with growth hormone. Horm. Res. Paediatr. 2011, 75, 335–345. [Google Scholar] [CrossRef]
- Chaler, E.A.; Ballerini, G.; Lazzati, J.M.; Maceiras, M.; Frusti, M.; Bergada, I.; Rivarola, M.A.; Belgorosky, A.; Ropelato, G. Cut-off values of serum growth hormone (GH) in pharmacological stimulation tests (PhT) evaluated in short-statured children using a chemiluminescent immunometric assay (ICMA) calibrated with the International Recombinant Human GH Standard 98/574. Clin. Chem. Lab. Med. 2013, 51, e95–e97. [Google Scholar] [CrossRef]
- Rosenfeld, R.G.; Wikland, K.A.; Cassorla, F.; Frasier, S.F.; Hasegawa, Y.; Hintz, R.L.; Lafranchi, S.; Lippe, B.; Loriaux, L.; Melmed, S. Diagnostic controversy: The diagnosis of childhood growth hormone deficiency revisited. J. Clin. Endocrinol. Metab. 1995, 80, 1532–1540. [Google Scholar]
- Graber, E.; Rapaport, R. Growth and growth disorders in children and adolescents. Pediatr. Ann. 2012, 41, e1–e9. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.; Kim, E.Y.; Kim, E.Y.; So, C.H.; Kim, C.J. Investigating whether serum IGF-1 and IGFBP-3 levels reflect the height outcome in prepubertal children upon rhGH therapy: LG growth study database. PLoS ONE 2021, 16, e0259287. [Google Scholar] [CrossRef]
- Yau, M.; Rapaport, R. Growth Hormone Stimulation Testing: To Test or Not to Test? That Is One of the Questions. Front. Endocrinol. 2022, 13, 902364. [Google Scholar] [CrossRef]
- Laurer, E.; Sirovina, A.; Blaschitz, A.; Tischlinger, K.; Montero-Lopez, R.; Hörtenhuber, T.; Wimleitner, M.; Högler, W. The landscape of retesting in childhood-onset idiopathic growth hormone deficiency and its reversibility: A systematic review and meta-analysis. Eur. J. Endocrinol. 2022, 187, 265–278. [Google Scholar] [CrossRef] [PubMed]
- Partenope, C.; Galazzi, E.; Albanese, A.; Bellone, S.; Rabbone, I.; Persani, L. Sex steroid priming in short stature children unresponsive to GH stimulation tests: Why, who, when and how. Front. Endocrinol. 2022, 13, 1072271. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.G.; Clark, J.W.; Connor, T.B. Growth hormone secretion enhanced by androgens. J. Clin. Endocrinol. Metab. 1968, 28, 425–428. [Google Scholar] [CrossRef]
- Guzzetti, C.; Gallo, M.; Loche, S. Quando e come effettuare il priming per la valutazione dell’increzione del GH nell’età evolutiva. L’Endocrinologo 2021, 22, 36–37. [Google Scholar] [CrossRef]
- Ibba, A.; Guzzetti, C.; Casula, L.; Salerno, M.; Iorgi, N.D.; Allegri, A.M.G.; Cappa, M.; Maghnie, M.; Loche, S. Reliability of clonidine testing for the diagnosis of growth hormone deficiency in children and adolescents. Clin. Endocrinol. 2018, 89, 765–770. [Google Scholar] [CrossRef]
- Cavallo, L.; Acquafredda, A.; Liuzzi, S.; Russo, R.; Zecchino, C.; Leuzzi, R.; Giobbe, T.; Piacente, T. Growth hormone release during insulin tolerance, clonidine, arginine and growth hormone releasing hormone tests in short normal children and adolescents. J. Endocrinol. Invest 1992, 15, 131–135. [Google Scholar] [CrossRef]
- Cohen, P.; Germak, J.; Rogol, A.D.; Weng, W.; Kappelgaard, A.M.; Rosenfeld, R.G. Variable degree of growth hormone (GH) and insulin-like growth factor (IGF) sensitivity in children with idiopathic short stature compared with GH-deficient patients: Evidence from an IGF-based dosing study of short children. J. Clin. Endocrinol. Metab. 2010, 95, 2089–2098. [Google Scholar] [CrossRef] [Green Version]
- Kriström, B.; Lundberg, E.; Jonsson, B.; Albertsson-Wikland, K. study group. IGF-1 and growth response to adult height in a randomized GH treatment trial in short non-GH-deficient children. J. Clin. Endocrinol. Metab. 2014, 99, 2917–2924. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| CASES (n = 24) | CONTROLS (n = 28) | p | |
|---|---|---|---|
| SEX M/F | 13 (54.2%)/11 (45.8%) | 23 (82.2%)/5 (17.8%) | 0.1 |
| AGE (years) | 12.08 (3.75; 16.16) | 12.46 (5.00; 15.90) | 0.61 |
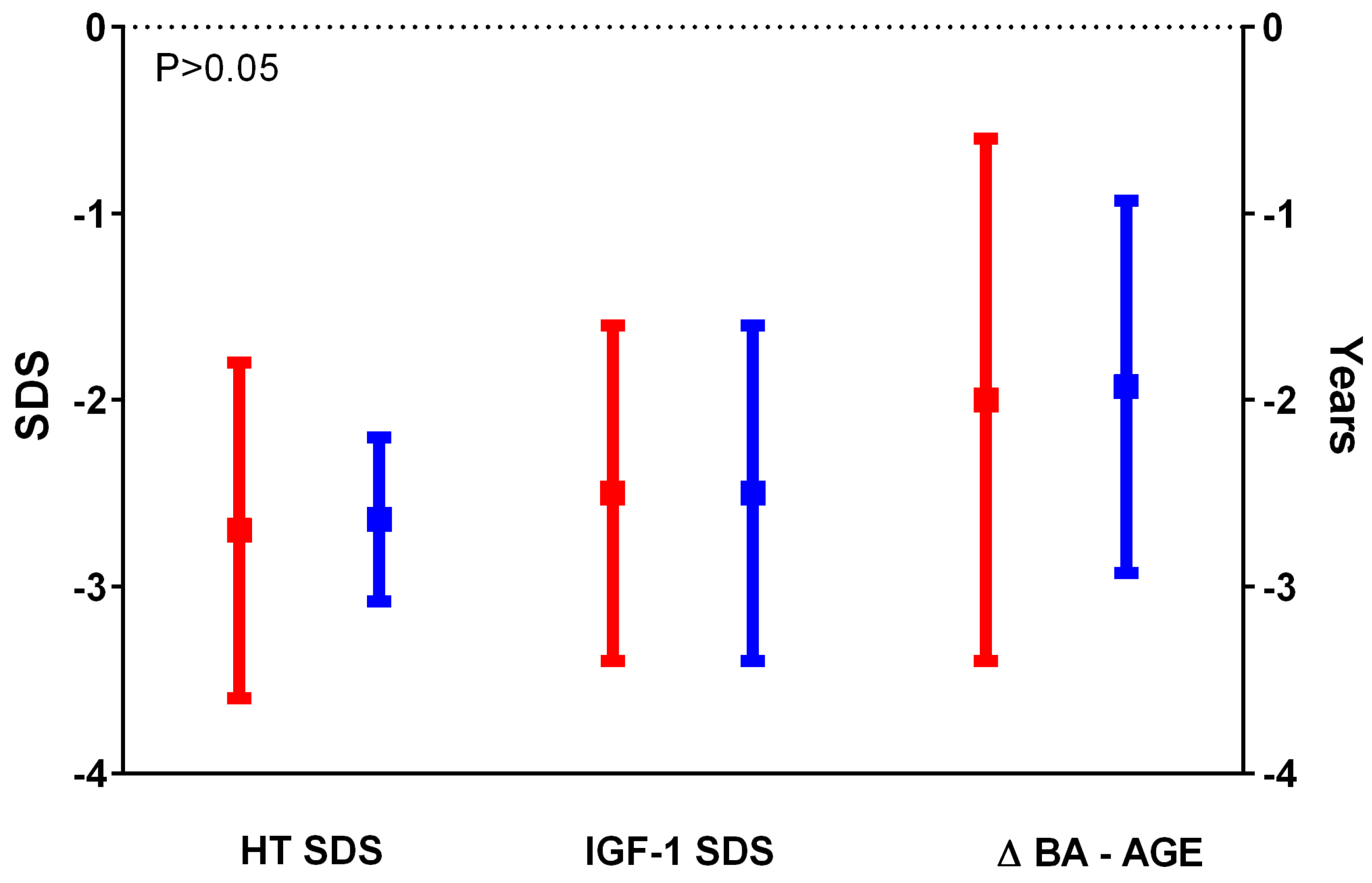
| HT SDS | −2.65 (−4.50; −0.01) | −2.60 (−3.58; −1.78) | 0.58 |
| TH SDS | −1.00 (−2.55; 0.30) | −1.60 (−2.45; 0.00) | 0.017 |
| BMI SDS | −0.02 (−2.87; 2.05) | −1.31 (−2.91; 0.38) | 0.0003 |
| Prepubertal/pubertal | 19 (79.2%)/5 (20.8%) | 15 (53.5%)/13 (46.4%) | 0.08 |
| Puberty onset (years) | 12.8 (9.11; 15.3) | 12.9 (11.9; 14.11) | 0.87 |
| BA (years) | 10.40 (3.90; 13.90) | 10.35 (3.00; 15.00) | 0.54 |
| BA—Age (years) | −2.20 (−4.20; −0.10) | −1.87 (−3.70; 0.30) | 0.91 |
| HV SDS pre-test | −1.11 (−3.79; 1.11) | −2.77 (−6.91; −0.46) | 0.05 |
| HV SDS post-test | 2.47 (−3; 11.64) | −1.01 (−5.7; 6.9) | 0.04 |
| IGF-1 SDS | −2.13 (−5.48; −1.56) | −2.19 (−4.9; −1.55) | 0.87 |
| IGFBP-3 SDS | −0.65 (−3.08; 0.37) | −0.61 (−1.87; 0.77) | 0.43 |
| Peak GH Arg (µg/L) | 6.78 (3.00; 7.90) (n = 11) | 13.25 (6.42; 21.20) (n = 4) | 0.0021 |
| Peak GH ITT (µg/L) | 5.70 (3.60; 7.91) (n = 5) | 8.56 (8.56; 8.56) (n = 1) | n.a. |
| Peak GH Clo (µg/L) | 5.48 (0.07; 9.80) (n = 22) | 13.20 (4.42; 28.40) (n = 16) | <0.0001 |
| Peak GH (µg/L) | 7.00 (3.00; 9.80) (n = 24) | 13.95 (8.56; 28.40) (n = 20) | <0.0001 |
| Peak GHRH+Arg (µg/L) | 6.89 (6.18; 8.60) (n = 3) | 26.60 (14.60; 40.00) (n = 10) | 0.007 |
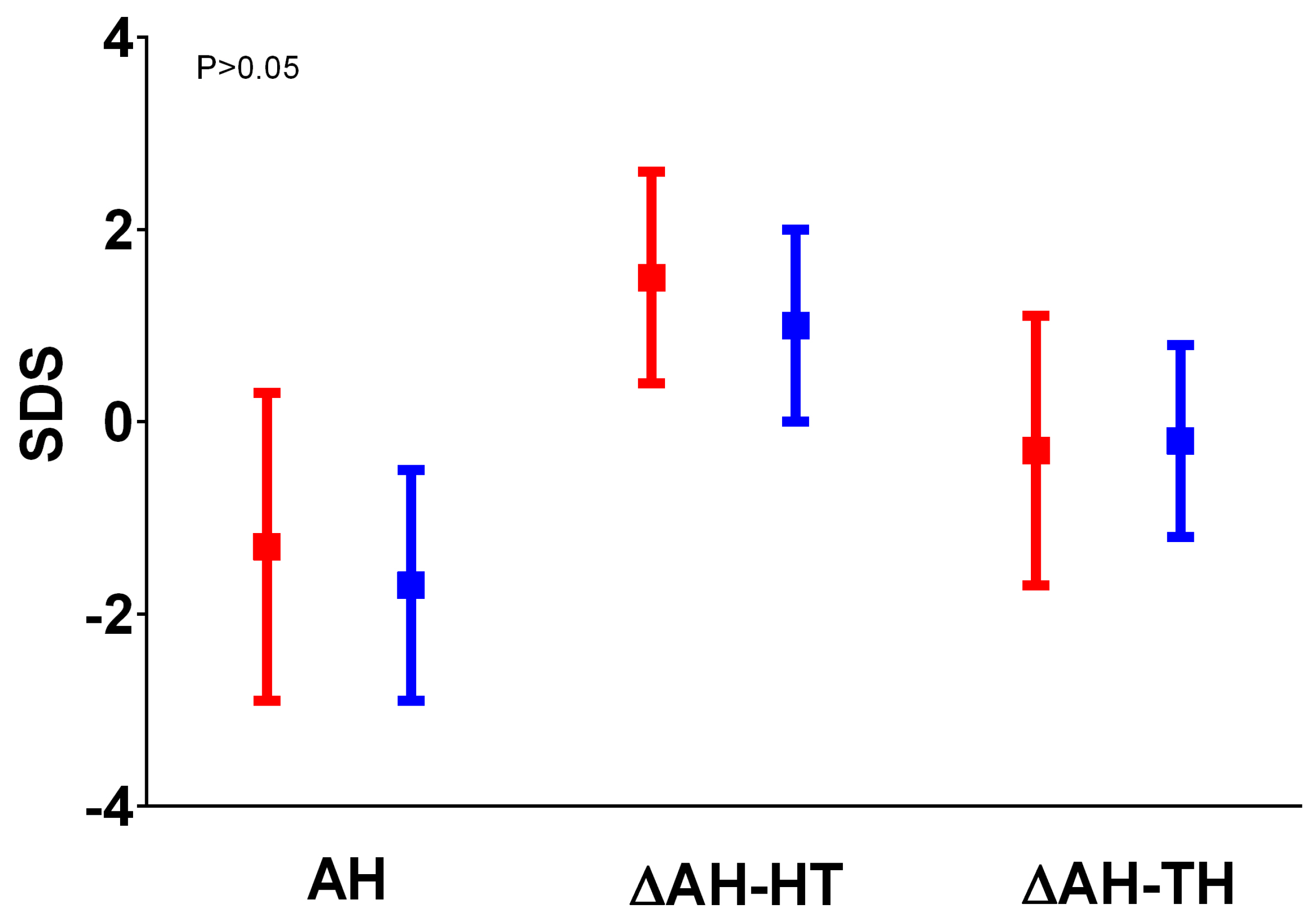
| AH SDS | −1.56 (−3.80; 1.76) | −1.76 (−3.44; 1.00) | 0.3 |
| Δ AH SDS- HT SDS | 1.29 (0.07; 3.78) | 0.95 (−1.27; 3.20) | 0.08 |
| Δ AH SDS- TH SDS | −0.31 (−3.40; 2.76) | −0.16 (−1.97; 2.00) | 0.69 |
| Controls (n = 28) | Partial GHD (n = 16) | p (Partial GHD vs. Controls) | Severe GHD (n = 8) | p (Severe GHD vs. Controls) | |
|---|---|---|---|---|---|
| SEX M/F | 23 (82.2%)/5 (17.8%) | 9 (56.25%)/7 (43.75%) | 0.05 | 4 (50%)/4 (50%) | 0.08 |
| AGE (years) | 12.46 (5.00; 15.90) | 11.50 (3.75; 15.66) | 0.31 | 12.63 (7.08; 16.16) | 0.59 |
| HT SDS | −2.60 (−3.58; −1.78) | −2.80 (−4.50; −2.00) | 0.12 | −2.45 (−3.87; −0.01) | 0.38 |
| TH SDS | −1.60 (−2.45; 0.00) | −1.00 (−2.41;0.20) | 0.03 | −0.89 (−2.55; 0.3) | 0.07 |
| BMI SDS | −1.31 (−2.91; 0.38) | −0.11 (−2.87;1.41) | 0.04 | 0.06 (−1.35; 2.05) | 0.0006 |
| Prepubertal/ pubertal | 15 (53.5%)/13(46.4%) | 12 (75%)/4 (25%) | 0.2 | 7 (87.5%)/1 (12.5%) | 0.11 |
| Puberty onset (years) | 12.9 (11.9; 14.11) | 12.40 (9.11;15.30) | 0.64 | 13.85 (12.8; 14.9) | 0.19 |
| BA (years) | 10.35 (3.00; 15.00) | 10.40 (3.90;13.90) | 0.57 | 10.5 (9.7; 11.3) | 0.79 |
| BA—Age (years) | −1.87 (−3.70; 0.30) | −1.40 (−4.20; −0.10) | 0.99 | −2.25 (−2.3; −2.2) | 0.65 |
| HV SDS pre-test | −2.77 (−6.91; −0.46) | −1.03 (−3.79; −0.29) | 0.17 | −1.2 (−1.84; 1.11) | 0.07 |
| HV SDS post-test | −1.01 (−5.7; 6.9) | 2.47 (−3.00;10.23) | 0.01 | 4.78 (0.17; 11.64) | 0.003 |
| IGF-1 SDS | −2.19 (−4.9; −1.55) | −2.08 (−5.48; −1.56) | 0.94 | −2.61 (−3.61; −1.70) | 0.52 |
| IGFBP-3 SDS | −0.61 (−1.87; 0.77) | −0.57 (−3.08;0.37) | 0.42 | −1.89 (−2.69; −1.1) | 0.12 |
| Peak GH Arg (µg/L) | 13.25 (6.42; 21.20) (n = 4) | 6.84 (4.80;7.90) (n = 10) | 0.054 | 3 (n = 3) | n.a. |
| Peak GH ITT (µg/L) | 8.56 (8.56; 8.56) (n = 1) | 5.75 (4.27;7.91) (n = 4) | n.a. | 3.6 (n = 1) | n.a. |
| Peak GH Clo (µg/L) | 13.20 (4.42; 28.40) (n = 16) | 6.60 (3.70;9.80) (n = 14) | <0.0001 | 2.25 (0.07; 3.93) (n = 8) | <0.0001 |
| Peak GH (µg/L) | 13.95 (8.56; 28.40) (n = 20) | 7.15 (5.80;9.80) (n = 14) | <0.0001 | 2.70 (−0.07; 3.93) | <0.0001 |
| Peak GHRH+Arg (µg/L) | 26.60 (14.60; 40.00) (n = 10) | 6.53 (6.18;6.89) (n = 2) | 0.03 | 8.6 (n = 1) | n.a. |
| AH SDS | −1.76 (−3.44; 1.00) | −1.70 (−3.34;1.76) | 0.78 | −0.28 (−3.8; 1.1) | 0.07 |
| Δ AH SDS− HT SDS | 0.95 (−1.27; 3.20) | 1.16 (0.10;3.78) | 0.49 | 1.85 (0.07; 2.73) | 0.07 |
| Δ AH SDS− TH SDS | −0.16 (−1.97; 2.00) | −0.77 (−3.40; 2.76) | 0.18 | 0.39 (−1.8; 1.99) | 0.44 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murianni, A.; Lussu, A.; Guzzetti, C.; Ibba, A.; Casula, L.; Salerno, M.; Cappa, M.; Loche, S. Evaluation of Adult Height in Patients with Non-Permanent Idiopathic GH Deficiency. Endocrines 2023, 4, 169-178. https://doi.org/10.3390/endocrines4010015
Murianni A, Lussu A, Guzzetti C, Ibba A, Casula L, Salerno M, Cappa M, Loche S. Evaluation of Adult Height in Patients with Non-Permanent Idiopathic GH Deficiency. Endocrines. 2023; 4(1):169-178. https://doi.org/10.3390/endocrines4010015
Chicago/Turabian StyleMurianni, Agnese, Anna Lussu, Chiara Guzzetti, Anastasia Ibba, Letizia Casula, Mariacarolina Salerno, Marco Cappa, and Sandro Loche. 2023. "Evaluation of Adult Height in Patients with Non-Permanent Idiopathic GH Deficiency" Endocrines 4, no. 1: 169-178. https://doi.org/10.3390/endocrines4010015