
Does Testosterone Salvage PDE5i Non-Responders? A Scoping Review
Abstract
:1. Introduction
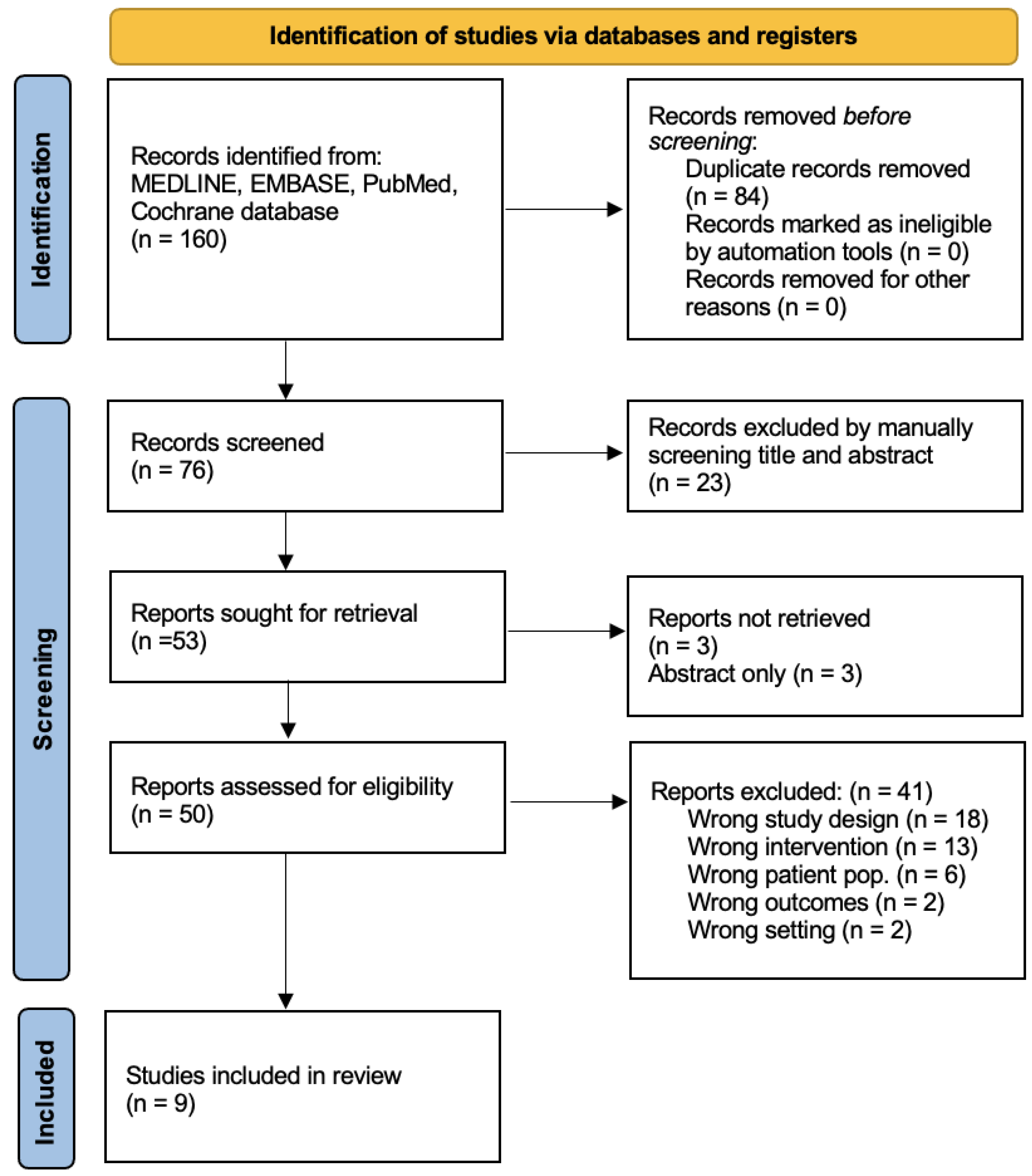
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burnett, A.L.; Nehra, A.; Breau, R.H.; Culkin, D.J.; Faraday, M.M.; Hakim, L.S.; Heidelbaugh, J.; Khera, M.; McVary, K.T.; Miner, M.M.; et al. AUA Guideline ED. AUA Clin. Guidel. 2018, 1–36. [Google Scholar] [CrossRef]
- Feldman, H.A.; Goldstein, I.; Hatzichristou, D.G.; Krane, R.J.; McKinlay, J.B. Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. J. Urol. 1994, 151, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Selvin, E.; Burnett, A.L.; Platz, E.A. Prevalence and Risk Factors for Erectile Dysfunction in the US. Am. J. Med. 2007, 120, 151–157. [Google Scholar] [CrossRef]
- Ayta, I.A.; McKinlay, J.B.; Krane, R.J. The likely worldwide increase in erectile dysfunction between 1995 and 2025: EBSCOhost. BJU Int. 1999, 84, 50–56. [Google Scholar] [CrossRef]
- Domes, T.; Najafabadi, B.T.; Roberts, M.; Campbell, J.; Flannigan, R.; Bach, P.; Patel, P.; Langille, G.; Krakowsky, Y.; Violette, P.D. CUA GUIDELINE Canadian Urological Association guideline: Erectile dysfunction. Can. Urol. Assoc. J. 2021, 15, 310. [Google Scholar] [CrossRef]
- Prieto, D. Physiological regulation of penile arteries and veins. Int. J. Impot. Res. 2008, 20, 17–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, A.M.B.; Meehan, J.P.; Zakhary, R.; Buckley, P.A.; Rogers, F.A. New observations on microarchitecture of corpora cavernosa in man and possible relationship to mechanism of erection. Urology 1982, 20, 259–266. [Google Scholar] [CrossRef]
- Andersson, K.E. Mechanisms of penile erection and basis for pharmacological treatment of erectile dysfunction. Pharmacol. Rev. 2011, 63, 811–859. [Google Scholar] [CrossRef]
- Williams-Ashman, H.G. Enigmatic Features of Penile Development and Functions. Perspect. Biol. Med. 1990, 33, 335–374. [Google Scholar] [CrossRef]
- Burnett, A.L. Nitric Oxide in the Penis: Physiology and Pathology. J. Urol. 1997, 157, 320–324. [Google Scholar] [CrossRef]
- Burnett, A.; Musicki, B. The Nitric Oxide Signaling Pathway in the Penis. Curr. Pharm. Des. 2005, 11, 3987–3994. [Google Scholar] [CrossRef] [PubMed]
- Christ, G.; Richards, S.; Winkler, A. Integrative erectile biology: The role of signal transduction and cell-to-cell communication in coordinating corporal smooth muscle tone and penile erection. Int. J. Impot. Res. 1997, 9, 69–84. [Google Scholar] [CrossRef] [Green Version]
- Wingard, C.J.; Lewis, R.; Mills, T.M. Erection and NO override the vasoconstrictive effect of α-adrenergic stimulation in the rat penile vasculature. Int. J. Impot. Res. 2001, 13, 212–220. [Google Scholar] [CrossRef] [Green Version]
- Card, G.L.; England, B.P.; Suzuki, Y.; Fong, D.; Powell, B.; Lee, B.; Luu, C.; Tabrizizad, M.; Gillette, S.; Ibrahim, P.N.; et al. Structural Basis for the Activity of Drugs that Inhibit Phosphodiesterases. Structure 2004, 12, 2233–2247. [Google Scholar] [CrossRef] [Green Version]
- Corbin, J.D. Mechanisms of action of PDE5 inhibition in erectile dysfunction. Int. J. Impot. Res. 2004, 16 (Suppl. 1), S4–S7. [Google Scholar] [CrossRef] [Green Version]
- Giuliano, F.; Jackson, G.; Montorsi, F.; Martin-Morales, A.; Raillard, P. Safety of sildenafil citrate: Review of 67 double-blind placebo-controlled trials and the postmarketing safety database. Int. J. Clin. Pr. 2010, 64, 240–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, I.; Lue, T.F.; Padma-Nathan, H.; Rosen, R.C.; Steers, W.D.; Wicker, P.A. Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group. N. Engl. J. Med. 1998, 338, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Hellstrom, W.J.G.; Gittelman, M.; Karlin, G.; Segerson, T.; Thibonnier, M.; Taylor, T.; Padma-Nathan, H. Vardenafil for treatment of men with erectile dysfunction: Efficacy and safety in a randomized, double-blind, placebo-controlled trial. J. Androl. 2002, 23, 763–771. [Google Scholar]
- Jung, J.; Choi, S.; Cho, S.H.; Ghim, J.L.; Hwang, A.; Kim, U.; Kim, B.S.; Koguchi, A.; Miyoshi, S.; Okabe, H.; et al. Tolerability and pharmacokinetics of avanafil, a phosphodiesterase type 5 inhibitor: A single- and multiple-dose, double-blind, randomized, placebo-controlled, dose-escalation study in healthy Korean male volunteers. Clin. Ther. 2010, 32, 1178–1187. [Google Scholar] [CrossRef]
- Madeira, C.R.; Tonin, F.S.; Fachi, M.M.; Borba, H.H.; Ferreira, V.L.; Leonart, L.P.; Bonetti, A.F.; Moritz, R.P.; Trindade, A.C.L.B.; Gonçalves, A.G.; et al. Efficacy and safety of oral phosphodiesterase 5 inhibitors for erectile dysfunction: A network meta-analysis and multicriteria decision analysis. World J. Urol. 2021, 39, 953–962. [Google Scholar] [CrossRef]
- Corona, G.; Rastrelli, G.; Burri, A.; Serra, E.; Gianfrilli, D.; Mannucci, E.; Jannini, E.A.; Maggi, M. First-generation phosphodiesterase type 5 inhibitors dropout: A comprehensive review and meta-analysis. Andrology 2016, 4, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Alemany, M. The Roles of Androgens in Humans: Biology, Metabolic Regulation and Health. Int. J. Mol. Sci. 2022, 23, 11952. [Google Scholar] [CrossRef] [PubMed]
- Lugg, J.A.; Rajfer, J.; González-Cadavid, N.F. Dihydrotestosterone is the active androgen in the maintenance of nitric oxide-mediated penile erection in the rat. Endocrinology 1995, 136, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, S.; Brito, J.P.; Cunningham, G.R.; Hayes, F.J.; Hodis, H.N.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Wu, F.C.; Yialamas, M.A. Testosterone Therapy in Men with Hypogonadism: An Endocrine Society* Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2018, 103, 1715–1744. [Google Scholar] [CrossRef] [Green Version]
- Kandeel, F.R.; Koussa, V.K.T.; Swerdloff, R.S. Male Sexual Function and Its Disorders: Physiology, Pathophysiology, Clinical Investigation, and Treatment. Endocr. Rev. 2001, 22, 342–388. [Google Scholar] [CrossRef] [PubMed]
- Snyder, P.J.; Ellenberg, S.S.; Cunningham, G.R.; Alvin, M.; Farrar, J.T.; Cella, D.; Rosen, R.C.; Susan, M. The Testosterone Trials: The Design of Seven. Clin. Trials 2015, 11, 362–375. [Google Scholar] [CrossRef] [Green Version]
- Barone, B.; Napolitano, L.; Abate, M.; Cirillo, L.; Reccia, P.; Passaro, F.; Turco, C.; Morra, S.; Mastrangelo, F.; Scarpato, A.; et al. The Role of Testosterone in the Elderly: What Do We Know? Int. J. Mol. Sci. 2022, 23, 3535. [Google Scholar] [CrossRef]
- Mulhall, J.P.; Trost, L.W.; Brannigan, R.E.; Kurtz, E.G.; Redmon, J.B.; Chiles, K.A.; Lightner, D.J.; Miner, M.M.; Murad, M.H.; Nelson, C.J.; et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J. Urol. 2018, 200, 423–432. [Google Scholar] [CrossRef] [Green Version]
- Jayasena, C.N.; Anderson, R.A.; Llahana, S.; Barth, J.H.; MacKenzie, F.; Wilkes, S.; Smith, N.; Sooriakumaran, P.; Minhas, S.; Wu, F.C.W.; et al. Society for Endocrinology guidelines for testosterone replacement therapy in male hypogonadism. Clin. Endocrinol. 2022, 96, 200–219. [Google Scholar] [CrossRef]
- Corona, G.; Goulis, D.G.; Huhtaniemi, I.; Zitzmann, M.; Toppari, J.; Forti, G.; Vanderschueren, D.; Wu, F.C.; Behre, H.; Punab, M.; et al. European Academy of Andrology (EAA) guidelines on investigation, treatment and monitoring of functional hypogonadism in males: Endorsing organization: European Society of Endocrinology. Andrology 2020, 8, 970–987. [Google Scholar] [CrossRef] [Green Version]
- Grober, E.D.; Krakowsky, Y.; Khera, M.; Holmes, D.T.; Lee, J.C.; Grantmyre, J.E.; Patel, P.; Bebb, R.A.; Fitzpatrick, R.; Campbell, J.D.; et al. Original Guideline Canadian Urological Association Guideline on Testosterone Deficiency in Men: Evidence-Based Q & A. Can. Urol. Assoc. J. 2021, 15, E234–E243. [Google Scholar] [CrossRef] [PubMed]
- Armagan, A.; Kim, N.N.; Goldstein, I.; Traish, A.M. Dose-Response Relationship Between Testosterone and Erectile Function: Evidence for the Existence of a Critical Threshold. J. Androl. 2006, 27, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, M.; Faber, S.; Nieschlag, E. Association of specific symptoms and metabolic risks with serum testosterone in older men. J. Clin. Endocrinol. Metab. 2006, 91, 4335–4343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.; Ku, J.H.; Kim, S.W.; Paick, J.-S. Risk factors in predicting a poor response to sildenafil citrate in elderly men with erectile dysfunction. BJU Int. 2005, 95, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Mulhall, J.P.; Brock, G.B.; Glina, S.; Baygani, S.; Donatucci, C.; Maggi, M. Impact of Baseline Total Testosterone Level on Successful Treatment of Sexual Dysfunction in Men Taking Once-Daily Tadalafil 5 mg for LUTS/BPH: An Integrated Analysis of Three Randomized Trials. J. Sex. Med. 2016, 13, 843–851. [Google Scholar] [CrossRef] [Green Version]
- Kalinchenko, S.Y.; Kozlov, G.I.; Gontcharov, N.P.; Katsiya, G.V. Oral testosterone undecanoate reverses erectile dysfunction associated with diabetes mellitus in patients failing on sildenafil citrate therapy alone. Aging Male 2003, 6, 94–99. [Google Scholar] [CrossRef]
- Aversa, A.; Isidori, A.M.; Spera, G.; Lenzi, A.; Fabbri, A. Androgens improve cavernous vasodilation and response to sildenafil in patients with erectile dysfunction. Clin. Endocrinol. 2003, 58, 632–638. [Google Scholar] [CrossRef]
- Shabsigh, R.; Kaufman, J.M.; Steidle, C.; Padma-Nathan, H. Randomized study of testosterone gel as adjunctive therapy to sildenafil in hypogonadal men with erectile dysfunction who do not respond to sildenafil alone. J. Urol. 2004, 172, 658–663. [Google Scholar] [CrossRef]
- Shamloul, R.; Ghanem, H.; Fahmy, I.; El-Meleigy, A.; Ashoor, S.; Elnashaar, A.; Kamel, I. Testosterone Therapy Can Enhance Erectile Function Response to Sildenafil in Patients with PADAM: A Pilot Study. J. Sex. Med. 2005, 2, 559–564. [Google Scholar] [CrossRef]
- Hwang, T.-S.; Chen, H.-E.; Tsai, T.-F.; Lin, Y.C. Combined use of androgen and sildenafil for hypogonadal patients unresponsive to sildenafil alone. Int. J. Impot. Res. 2006, 18, 400–404. [Google Scholar] [CrossRef] [Green Version]
- Buvat, J.; Montorsi, F.; Maggi, M.; Porst, H.; Kaipia, A.; Colson, M.H.; Cuzin, B.; Moncada, I.; Martin-Morales, A.; Yassin, A.; et al. Hypogonadal Men Nonresponders to the PDE5 Inhibitor Tadalafil Benefit from Normalization of Testosterone Levels with a 1% Hydroalcoholic Testosterone Gel in the Treatment of Erectile Dysfunction (TADTEST Study). J. Sex. Med. 2011, 8, 284–293. [Google Scholar] [CrossRef]
- Garcia, J.A.; Sanchez, P.E.; Fraile, C.; Escovar, P. Testosterone undecanoate improves erectile dysfunction in hypogonadal men with the metabolic syndrome refractory to treatment with phosphodiesterase type 5 inhibitors alone. Andrologia 2011, 43, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, M.; Basaria, S.; Travison, T.G.; Davda, M.N.; Paley, A.; Cohen, B.; Mazer, N.A.; Knapp, P.E.; Hanka, S.; Lakshman, K.M.; et al. Effect of Testosterone Replacement on Response to Sildenafil Citrate in Men with Erectile Dysfunction. Ann. Intern. Med. 2012, 157, 681–691. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.W.; Oh, M.M.; Park, M.G.; Park, J.Y.; Bae, J.H.; Kim, J.J.; Moon, D.G. Combination therapy of testosterone enanthate and tadalafil on PDE5 inhibitor non-reponders with severe and intermediate testosterone deficiency. Int. J. Impot. Res. 2013, 25, 29–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baba, K.; Yajima, M.; Carrier, S.; Morgan, D.M.; Nunes, L.; Lue, T.F.; Iwamoto, T. Delayed testosterone replacement restores nitric oxide synthase-containing nerve fibres and the erectile response in rat penis. BJU Int. 2000, 85, 953–958. [Google Scholar] [CrossRef]
- Baba, K.; Yajima, M.; Carrier, S.; Akkus, E.; Reman, J.; Nunes, L.; Lue, T.F.; Iwamoto, T. Effect of testosterone on the number of NADPH diaphorase-stained nerve fibers in the rat corpus cavernosum and dorsal nerve. Urology 2000, 56, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Shabsigh, R. The effects of testosterone on the cavernous tissue and erectile function. World J. Urol. 1997, 15, 21–26. [Google Scholar] [CrossRef]
- Traish, A.M.; Goldstein, I.; Kim, N.N. Testosterone and Erectile Function: From Basic Research to a New Clinical Paradigm for Managing Men. Eur. Urol. 2008, 52, 54–70. [Google Scholar] [CrossRef] [Green Version]
- Morelli, A.; Filippi, S.; Mancina, R.; Luconi, M.; Vignozzi, L.; Marini, M.; Orlando, C.; Vannelli, G.B.; Aversa, A.; Natali, A.; et al. Androgens Regulate Phosphodiesterase Type 5 Expression and Functional Activity in Corpora Cavernosa. Endocrinology 2004, 145, 2253–2263. [Google Scholar] [CrossRef] [Green Version]
- Traish, A.M.; Park, K.; Dhir, V.; Kim, N.N.; Moreland, R.B.; Goldstein, I. Effects of Castration and Androgen Replacement on Erectile Function in a Rabbit Model. Endocrinology 1999, 140, 1861–1868. [Google Scholar] [CrossRef]
- Zhang, X.-H.; Morelli, A.; Luconi, M.; Vignozzi, L.; Filippi, S.; Marini, M.; Vannelli, G.B.; Mancina, R.; Forti, G.; Maggi, M. Testosterone Regulates PDE5 Expression and in vivo Responsiveness to Tadalafil in Rat Corpus Cavernosum. Eur. Urol. 2005, 47, 409–416. [Google Scholar] [CrossRef]
- Lee, D.S.; Sohn, D.W. The Role of Testosterone in Amplifying the Effect of a Phosphodiesterase Type 5 Inhibitor After Pelvic Irradiation. J. Sex. Med. 2020, 17, 1268–1279. [Google Scholar] [CrossRef]
- Manning, B.D.; Cantley, L.C. AKT/PKB Signaling: Navigating Downstream. Cell 2007, 129, 1261–1274. [Google Scholar] [CrossRef] [Green Version]
- Efesoy, O.; Çayan, S.; Akbay, E. The Effect of Testosterone Replacement Therapy on Penile Hemodynamics in Hypogonadal Men With Erectile Dysfunction, Having Veno-Occlusive Dysfunction. Am. J. Men’s Health 2018, 12, 634–638. [Google Scholar] [CrossRef] [Green Version]
- Yassin, A.A.; Saad, F.; Traish, A. Testosterone Undecanoate Restores Erectile Function in a Subset of Patients with Venous Leakage: A Series of Case Reports. J. Sex. Med. 2006, 3, 727–735. [Google Scholar] [CrossRef]
- Bella, A.J.; Lee, J.C.; Carrier, S.; Bénard, F.; Brock, G.B. 2015 CUA Practice guidelines for erectile dysfunction. Can. Urol. Assoc. J. 2015, 9, 23–29. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Study, Year | n | Study Type, Country | Testosterone Formulation | PDE5i | Control | Duration of Treatment (Weeks) | Outcome Measure |
|---|---|---|---|---|---|---|---|
| * Kalinchenko 2003 [36] | 120 | Cohort, Russia | Oral testosterone undecanoate (120 mg/day) | Sildenafil (100 mg PRN) | 8 | IIEF | |
| * Aversa 2003 [37] | 20 | RCT, Italy | Transdermal patch (5 mg/day) | Sildenafil (100 mg PRN) | Placebo | 10 | IIEF |
| Shabsigh 2004 [38] | 75 | RCT, USA | 1% testosterone gel | Sildenafil (100 mg PRN) | Placebo | 14 | IIEF |
| Shamloul 2005 [39] | 40 | Prospective cohort, Egypt | Oral undecanoate (120 mg/day) | Sildenafil (50–100 mg PRN) | 12 | PADAM, IIEF | |
| Hwang 2006 [40] | 32 | Cohort, Taiwan | Oral undecanoate (160–240 mg/day) | Sildenafil (100 mg PRN) | 4 | IIEF | |
| Buvat 2011 [41] | 173 | Multi-centered RCT, European | 1% hydroalcoholic T gel (up to 10 mg) | Tadalafil (10 mg/day) | Placebo | 8 | IIEF |
| Garcia 2011 [42] | 29 | Cohort, Venezuela | Parenteral testosterone undecanoate (2 injections q6 weeks, followed by 12-weekly injections) | Unspecified | 102 | IIEF | |
| † Spitzer 2012 [43] | 140 | RCT, USA | 1% transdermal testosterone gel (10 g/day) | Sildenafil (25–100 mg PRN) | Placebo | 12 | IIEF |
| Kim 2013 [44] | 46 | Cohort, Korea | Parental testosterone enanthate q4 weeks | Tadalafil (5 mg/day) | 36 | IIEF |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pignanelli, M.; Stern, N.; Brock, G. Does Testosterone Salvage PDE5i Non-Responders? A Scoping Review. Endocrines 2023, 4, 117-127. https://doi.org/10.3390/endocrines4010011
Pignanelli M, Stern N, Brock G. Does Testosterone Salvage PDE5i Non-Responders? A Scoping Review. Endocrines. 2023; 4(1):117-127. https://doi.org/10.3390/endocrines4010011
Chicago/Turabian StylePignanelli, Mike, Noah Stern, and Gerald Brock. 2023. "Does Testosterone Salvage PDE5i Non-Responders? A Scoping Review" Endocrines 4, no. 1: 117-127. https://doi.org/10.3390/endocrines4010011