Role of Biomarkers in Detecting Acute Rejection in Kidney Transplantation

Department of Renal Transplantation, Careggi University Hospital, Viale Pieraccini 18, 50139 Florence, Italy
Transplantology 2023, 4(1), 18-21; https://doi.org/10.3390/transplantology4010004
Submission received: 6 December 2022
/
Accepted: 1 February 2023
/
Published: 10 February 2023
{kind=link}
1. Definition and Modality of Finding Biomarkers
Medicine has evolved from the so-called experience-based medicine to evidence-based medicine, which is now evolving into precision-based medicine. Biomarkers, among other findings, have allowed this change. In this editorial, how improved diagnosis and the treatment of acute rejection have benefited from the use of biomarkers will be documented.
Biomarkers are characteristics that evaluate biological processes and pathological processes and are the answer to therapeutic interventions [1].
In particular, in the case of kidney transplantation and in the prediction or diagnosis of acute rejection, biomarkers allow one to understand the recipient’s risk of developing acute rejection and allow the physician to make a non-invasive diagnosis at an early stage when the renal biopsy is apparently normal.
The principal characteristics of biomarkers applied to kidney transplantation are the following:
- - High sensitivity and specificity, predicting elevated receiver operating curves;
- - Biomarker validations are essential due to interindividual variations and interlaboratory variability.
Examples of non-invasive candidate biomarkers are mRNA transcripts, some chemokines, and donor-specific antibodies.
The main and innovative technologies applied to the identification of biomarkers are proteomics, that is, the analysis to understand the protein’s identity. Proteomics are applied to the serum and/or urine; genomics are the study of the genome to understand the risk of a patient with regard to the development of a disease; transcriptomics are the study of expression patterns of all gene transcripts; and metabolomics are the study of the metabolites involved in a biological process [2].
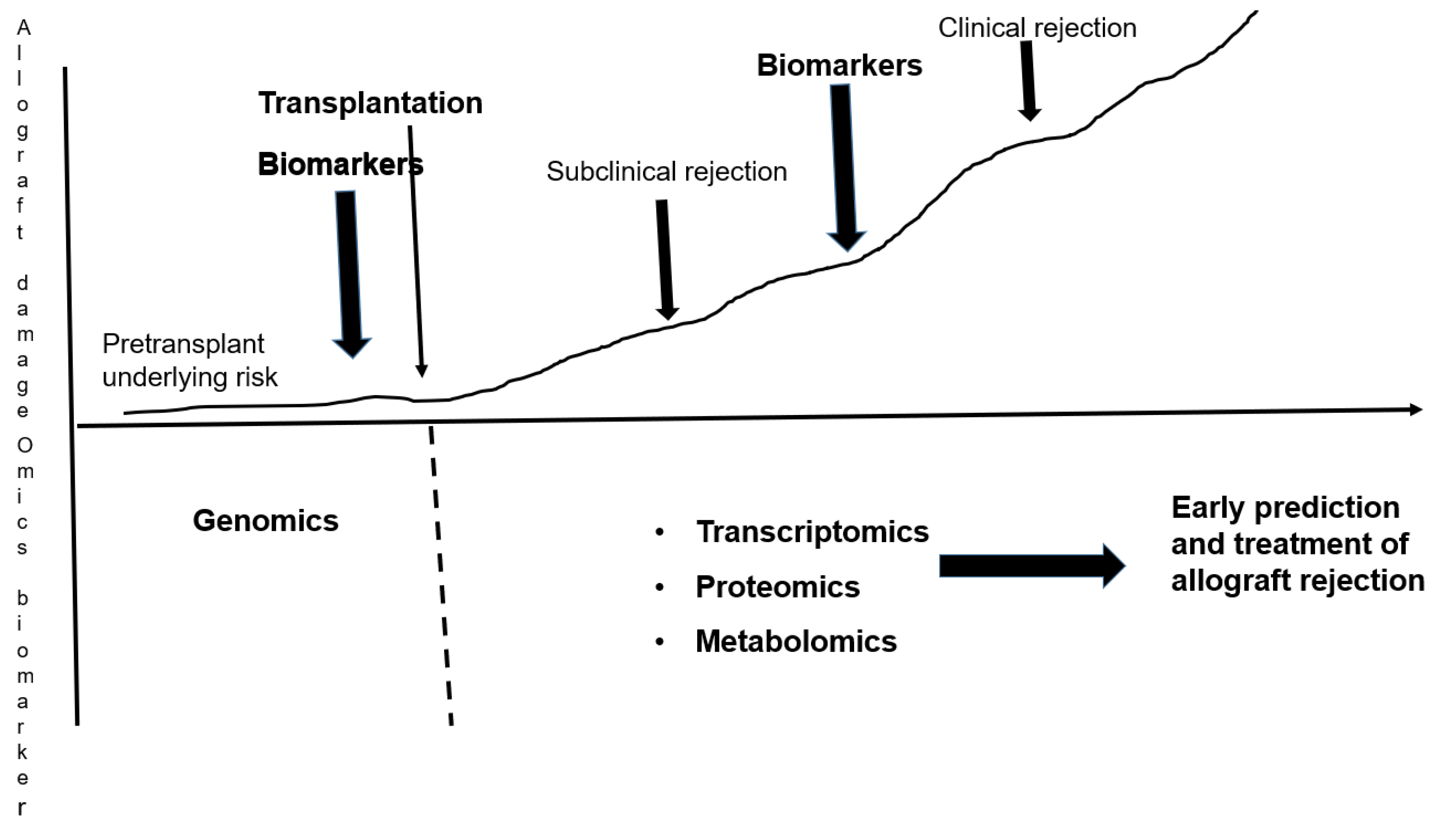
Figure 1 represents when and which biomarkers, and by which technology, are useful for the prediction and diagnosis of acute rejection in the evolution of kidney transplantation. Before kidney transplantation, genomics may identify the pre-transplant underlying risk. This technique is difficult to be applied, mostly because it needs a wide number of patients to be representative of a real risk. The genomic wide application study (GWAS) should be applied, but may rarely be used because it needs a very large number of patients. In the post-transplantation period, transcriptomics, proteomics, and metabolomics are the technologies used to identify an early prediction of and treatment for allograft rejection. Approximately 10 years ago, in the clinical trial steroid-free vs. steroid-based immunosuppression in pediatric renal transplantation (SNSO1), it was documented that renal biopsy (the golden standard for identifying kidney rejection) did not identify “hidden injuries” in clinically stable patients [3,4]. In a following study, Naessens et al. [5] performed protocol biopsies, and documented that tissue examination at the molecular level was able to identify tissue abnormalities long before the appearance of acute rejection in the standard biopsy examination.
2. Genomics Studies for Acute Rejection
As aforementioned, genomic studies are mostly applied to identify risk factors in the pre-transplant period.
A recent study [6] became the most important study on this topic. According to this [7], the polymorphism of several genes such as CYP3A5, CCR5, FOXP3, and other genes such as TGF β and VEGF, frequently involved in inflammation, is a predictor of AR. The limitation of the study is the very small dataset that accounts for only 24 specimens.
A different recent study [8] reported on the recent genomic studies on this issue that applied the GWAS technique, such as by Ghisdal [9], Oetting [10], and Steers [11]. In particular, Ghisdal et al. found that the gene Protein Tyrosine Phosphatase Receptor Type O (PTPRO) and the gene CCDC667 could have two SNPs associated with T-cell-mediated acute rejection.
The study of Oetting et al. documented that the SNP rs2910164 is related to T-cell-mediated rejection and antibody-mediated acute rejection.
Finally, the study by Steers et al. documented that the LIMS1 gene (rs893403) is related to both T cell and antibody-mediated acute rejection.
3. Other Biomarkers for Acute Rejection Identified by other Omic Technologies (Proteomics, Metabolomics, Transcriptomics)
Several biomarkers have been identified by these technologies. Rogulska et al. [12] reported the most recent and relevant of these in a structured review. These biomarkers are as follows:
Neutrophil gelatinase-associated lipocalin (NGAL)
uNGAL is able to make a differential diagnosis between kidney acute rejection and other causes of acute kidney injury (AKI). In particular, serum NGAL is diagnostic for renal rejection when detected early post-transplantation, and high values of serum NGAL may be diagnostic of acute rejection instead of different causes of allograft dysfunction.
Kidney Injury Molecule-1 (KIM-1)
High urinary KIM-1 excretion in addition to being a relevant marker of kidney transplant rejection is a predictor of graft loss.
C-X-C Motif Chemokine 10 (CXCL-10)
CXCCL-10 levels are relevant markers of T-cell-mediated rejection, more so than of antibody-mediated rejection. In addition, CXCL-10 is an indicator of a response to antirejection treatment, even more so than serum creatinine levels.
Osteopontin (OPN)
Osteopontin, also called bone sialoprotein 1 (BSP-1), acts on the homeostasis of the immune system, acting as a cytokine. Plasma OPN levels correlate with the severity of acute cellular rejection, as documented via renal biopsy. Alchi et al. [13], comparing renal biopsies from patients with acute rejection with protocol biopsies and from patients without acute rejection, found higher levels of OPN in patients with acute rejection.
4. Conclusions
Biomarkers represent important findings in the evolution of medicine and have allowed the evolution from evidence-based medicine to the “so called” precision-based medicine.
They are essential in the diagnosis and the correct treatment of a disease and, in particular, in the diagnosis of acute kidney rejection after transplantation, allowing for a correct diagnosis even before the golden standard of renal biopsy. In addition, the evolution of biomarkers during treatment allows the efficacy of the treatment itself to be checked.
Recent molecular studies on the allograft and advanced urine bioassays suggest that the allograft biopsy may be the “copper standard” for an apparently stable allograft, where a graft rejection may be “hidden”.
The evolution of multiomic assays in serum and urine may personalize the immunosuppressive therapy by the increased frequency of non-invasive biomarker monitoring for the allograft status both in those with a healthy condition and with injury.
To date, the major drawback of such studies is the small number of patients involved.
Data that are more reliable will be provided by the use of the GWAS technique, in particular in finding genomic biomarkers. The technique, however, requires the cooperation of many transplant centers.
Funding
This study did not received any external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data may be found in the references.
Conflicts of Interest
The author declares no conflict of interest.
References
- Biomarkers Definition Working Group. Biomarkers and surrogate endpoints: Preferred definition and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Bontha, S.V.; Maluf, D.G.; Mueller, T.F.; Mas, V.R. Systems Biology in Kidney Transplantation: The Application of Multi-Omics to a Complex Model. Am. J. Transplant. 2017, 17, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Naesens, M.; Salvatierra, O.; Benfield, M.; Ettenger, R.B.; Dharnidharka, V.; Harmon, W.; Mathias, R.; Sarwal, M.M. Subclinical inflammation and chronic renal allograft injury in a randomized trial on steroid avoidance in pediatric kidney transplantation. Am. J. Transplant. 2012, 12, 2730–2743. [Google Scholar] [CrossRef] [PubMed]
- Sarwal, M.M.; Ettenger, R.B.; Dharnidharka, V.; Benfield, M.; Mathias, R.; Portale, A.; McDonald, R.; Harmon, W.; Kershaw, D.; Vehaskari, V.M.; et al. Complete steroid avoidance is effective and safe in children with renal transplants: A multicenter randomized trial with three-year follow-up. Am. J. Transplant. 2012, 12, 2719–2729. [Google Scholar] [CrossRef] [PubMed]
- Naesens, M.; Khatri, P.; Li, L.; Sigdel, T.K.; Vitalone, M.J.; Chen, R.; Butte, A.J.; Salvatierra, O.; Sarwal, M.M. Progressive histological damage in renal allografts is associated with expression of innate and adaptive immunity genes. Kidney Int. 2011, 80, 1364–1376. [Google Scholar] [CrossRef] [PubMed]
- Lepoittevin, M.; Kerforne, T.; Pellerin, L.; Hauet, T.; Thuillier, R. Molecular Markers of Kidney Transplantation Outcome: Current Omics Tools and Future Developments. J. Mol. Sci. 2022, 23, 6318. [Google Scholar] [CrossRef] [PubMed]
- Sarwal, M.M.; Chua, M.-S.; Kambham, N.; Hsieh, S.-C.; Satterwhite, T.; Masek, M.; Salvatierra, O., Jr. Molecular heterogeneity in acute renal allograft rejection identified by DNA microarray profiling. N. Engl. J. Med. 2003, 349, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.-H.; Chung, B.H.; Lee, S.-H.; Jung, H.-Y.; Choi, J.-Y.; Cho, J.-H.; Park, S.-H.; Kim, Y.-L.; Kim, C.-D. Omics-based biomarkers for diagnosis and prediction of kidney allograft rejection. Korean J. Intern. Med. 2022, 37, 520–533. [Google Scholar] [CrossRef] [PubMed]
- Ghisdal, L.; Baron, C.; Lebranchu, Y.; Viklický, O.; Konarikova, A.; Naesens, M.; Kuypers, D.; Dinic, M.; Alamartine, E.; Touchard, G.; et al. Genome-Wide Association Study of Acute Renal Graft Rejection. Am. J. Transplant. 2017, 17, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Oetting, W.S.; Schladt, D.P.; Dorr, C.R.; Wu, B.; Guan, W.; Remmel, R.P.; Iklé, D.; Mannon, R.B.; Matas, A.J.; Israni, A.K.; et al. Analysis of 75 Candidate SNPs Associated With Acute Rejection in Kidney Transplant Recipients: Validation of rs2910164 in MicroRNA MIR146A. Transplantation 2019, 103, 1591–1602. [Google Scholar] [CrossRef] [PubMed]
- Steers, N.J.; Li, Y.; Drace, Z.; D’Addario, J.A.; Fischman, C.; Liu, L.; Xu, K.; Na, Y.-J.; Neugut, Y.D.; Zhang, J.Y.; et al. Genomic Mismatch at LIMS1 Locus and Kidney Allograft Rejection. N. Engl. J. Med. 2019, 380, 1918–1928. [Google Scholar] [CrossRef] [PubMed]
- Rogulska, K.; Wojciechowska-Koszko, I.; Dołęgowska, B.; Kwiatkowska, E.; Roszkowska, P.; Kapczuk, P.; Kosik-Bogacka, D. The Most Promising Biomarkers of Allogeneic Kidney Transplant Rejection. J. Immunol. Res. 2022, 2022, 6572338. [Google Scholar] [CrossRef] [PubMed]
- Alchi, B.; Nishi, S.; Kondo, D.; Kaneko, Y.; Matsuki, A.; Imai, N.; Ueno, M.; Iguchi, S.; Sakatsume, M.; Narita, I.; et al. Osteopontin expression in acute renal allograft rejection. Kidney Int. 2005, 67, 886–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Evolution of a kidney allograft; role of biomarkers and technologies used.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Salvadori, M. Role of Biomarkers in Detecting Acute Rejection in Kidney Transplantation. Transplantology 2023, 4, 18-21. https://doi.org/10.3390/transplantology4010004
AMA Style
Salvadori M. Role of Biomarkers in Detecting Acute Rejection in Kidney Transplantation. Transplantology. 2023; 4(1):18-21. https://doi.org/10.3390/transplantology4010004
Chicago/Turabian StyleSalvadori, Maurizio. 2023. "Role of Biomarkers in Detecting Acute Rejection in Kidney Transplantation" Transplantology 4, no. 1: 18-21. https://doi.org/10.3390/transplantology4010004