
SARS-CoV-2 Infection of Unvaccinated Liver- and Kidney-Transplant Recipients: A Single-Center Experience of 103 Consecutive Cases

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Inclusion
2.2. Database Creation
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, X.; Zhou, Q.; He, Y.; Liu, L.; Ma, X.; Wei, X.; Jiang, N.; Liang, L.; Zheng, Y.; Ma, L.; et al. Nosocomial outbreak of COVID-19 pneumonia in Wuhan, China. Eur. Respir. J. 2020, 55, 2000544. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov (accessed on 31 July 2021).
- Centers for Disease Control and Prevention COVID Data Tracker. 2021. Available online: https://covid.cdc.gov/covid-data-tracker/#datatracker-home (accessed on 11 April 2022).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 30 December 2020).
- Avery, R.K.; Chiang, T.P.; Marr, K.A.; Brennan, D.C.; Sait, A.S.; Garibaldi, B.T.; Shah, P.; Ostrander, D.; Steinke, S.M.; Permpalung, N.; et al. Inpatient COVID-19 outcomes in solid organ transplant recipients compared to non-solid organ transplant patients: A retrospective cohort. Am. J. Transplant. 2020, 21, 2498–2508. [Google Scholar] [CrossRef]
- Cravedi, P.; Mothi, S.S.; Azzi, Y.; Haverly, M.; Farouk, S.S.; Pérez-Sáez, M.J.; Redondo-Pachón, M.D.; Murphy, B.; Florman, S.; Cyrino, L.G.; et al. COVID-19 and kidney transplantation: Results from the TANGO International Transplant Consortium. Am. J. Transplant. 2020, 20, 3140–3148. [Google Scholar] [CrossRef]
- Fernández-Ruiz, M.; Andrés, A.; Loinaz, C.; Delgado, J.F.; López-Medrano, F.; Juan, R.S.; González, E.; Polanco, N.; Folgueira, M.D.; Lalueza, A.; et al. COVID-19 in solid organ transplant recipients: A single-center case series from Spain. Am. J. Transplant. 2020, 20, 1849–1858. [Google Scholar] [CrossRef]
- Giorgakis, E.; Zehtaban, S.P.; Stevens, A.E.; Bhusal, S.; Burdine, L. COVID-19 in solid organ transplant recipients. Transpl. Infect. Dis. 2020, 23, e13419. [Google Scholar] [CrossRef]
- Kates, O.S.; Haydel, B.M.; Florman, S.S.; Rana, M.M.; Chaudhry, Z.S.; Ramesh, M.S.; Safa, K.; Kotton, C.N.; Blumberg, E.A.; Besharatian, B.D.; et al. Coronavirus Disease 2019 in Solid Organ Transplant: A Multicenter Cohort Study. Clin. Infect. Dis. 2020, 73, e4090–e4099. [Google Scholar] [CrossRef]
- Nair, V.; Jandovitz, N.; Hirsch, J.S.; Nair, G.; Abate, M.; Bhaskaran, M.; Grodstein, E.; Berlinrut, I.; Hirschwerk, D.; Cohen, S.L.; et al. COVID-19 in kidney transplant recipients. Am. J. Transplant. 2020, 20, 1819–1825. [Google Scholar] [CrossRef]
- Pereira, M.R.; Mohan, S.; Cohen, D.J.; Husain, S.A.; Dube, G.K.; Ratner, L.E.; Arcasoy, S.; Aversa, M.M.; Benvenuto, L.J.; Dadhania, D.M.; et al. COVID-19 in solid organ transplant recipients: Initial report from the US epicenter. Am. J. Transplant. 2020, 20, 1800–1808. [Google Scholar] [CrossRef]
- Raja, M.A.; Mendoza, M.A.; Villavicencio, A.; Anjan, S.; Reynolds, J.M.; Kittipibul, V.; Fernandez, A.; Guerra, G.; Camargo, J.F.; Simkins, J.; et al. COVID-19 in solid organ transplant recipients: A systematic review and meta-analysis of current literature. Transplant. Rev. 2020, 35, 100588. [Google Scholar] [CrossRef]
- Salto-Alejandre, S.; Jiménez-Jorge, S.; Sabé, N.; Ramos-Martínez, A.; Linares, L.; Valerio, M.; Martín-Dávila, P.; Fernández-Ruiz, M.; Fariñas, M.C.; Blanes-Juliá, M.; et al. Risk factors for unfavorable outcome and impact of early post-transplant infection in solid organ recipients with COVID-19: A prospective multicenter cohort study. PLoS ONE 2021, 16, e0250796. [Google Scholar] [CrossRef]
- Webb, G.J.; Marjot, T.; Cook, J.A.; Aloman, C.; Armstrong, M.J.; Brenner, E.J.; Catana, M.-A.; Cargill, T.; Dhanasekaran, R.; García-Juárez, I.; et al. Outcomes following SARS-CoV-2 infection in liver transplant recipients: An international registry study. Lancet Gastroenterol. Hepatol. 2020, 5, 1008–1016. [Google Scholar] [CrossRef]
- Caillard, S.; Anglicheau, D.; Matignon, M.; Durrbach, A.; Greze, C.; Frimat, L.; Thaunat, O.; Legris, T.; Moal, V.; Westeel, P.F.; et al. An initial report from the French SOT COVID Registry suggests high mortality due to COVID-19 in recipients of kidney transplants. Kidney Int. 2020, 98, 1549–1558. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. People with Certain Medical Conditions. 12 May 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 12 July 2021).
- Hadi, Y.B.; Naqvi, S.F.; Kupec, J.T.; Sofka, S.; Sarwari, A. Outcomes of COVID-19 in Solid Organ Transplant Recipients: A Propensity-matched Analysis of a Large Research Network. Transplantation 2021, 105, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Hardgrave, H.; Bhusal, S.; Rude, M.K.; Sharma, A.; Gonzalez, M.; Khan, N.; Deneke, M.; Thandassery, R.; Patel, R.; Dare, R.; et al. The Impact of Transplant Type, Age, and Immunosuppresion on Post COVID-19 Infection Survival: A Single Center United States Prospective Cohort Study. Transpl. Int. 2021, 34, 349. [Google Scholar]
- Verma, A.; Khorsandi, S.E.; Dolcet, A.; Prachalias, A.; Suddle, A.; Heaton, N.; Jassem, W. Low prevalence and disease severity of COVID-19 in post-liver transplant recipients—A single centre experience. Liver Int. 2020, 40, 1972–1976. [Google Scholar] [CrossRef]
- Colmenero, J.; Rodríguez-Perálvarez, M.; Salcedo, M.; Arias-Milla, A.; Muñoz-Serrano, A.; Graus, J.; Nuño, J.; Gastaca, M.; Bustamante-Schneider, J.; Cachero, A.; et al. Epidemiological pattern, incidence, and outcomes of COVID-19 in liver transplant patients. J. Hepatol. 2020, 74, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.B.; Izzy, S.; Tahir, Z.; Al Jarrah, A.; Fishman, J.A.; El Khoury, J. COVID-19 in solid organ transplant recipients: Dynamics of disease progression and inflammatory markers in ICU and non-ICU admitted patients. Transpl. Infect. Dis. 2020, 22, e13407. [Google Scholar] [CrossRef]
- Andersen, K.M.; Mehta, H.B.; Palamuttam, N.; Ford, D.; Garibaldi, B.T.; Auwaerter, P.G.; Segal, J.; Alexander, G.C. Association Between Chronic Use of Immunosuppresive Drugs and Clinical Outcomes from Coronavirus Disease 2019 (COVID-19) Hospitalization: A Retrospective Cohort Study in a Large US Health System. Clin. Infect. Dis. 2021, 73, e4124–e4130. [Google Scholar] [CrossRef]
- Angelico, R.; Blasi, F.; Manzia, T.; Toti, L.; Tisone, G.; Cacciola, R. The Management of Immunosuppression in Kidney Transplant Recipients with COVID-19 Disease: An Update and Systematic Review of the Literature. Medicina 2021, 57, 435. [Google Scholar] [CrossRef]
- Karruli, A.; Spiezia, S.; Boccia, F.; Gagliardi, M.; Patauner, F.; Salemme, A.; Maiello, C.; Zampino, R.; Durante-Mangoni, E. Effect of immunosuppression maintenance in solid organ transplant recipients with COVID-19: Systematic review and meta-analysis. Transpl. Infect. Dis. 2021, 23, e13595. [Google Scholar] [CrossRef]
- Kronbichler, A.; Gauckler, P.; Windpessl, M.; Shin, J.I.; Jha, V.; Rovin, B.H.; Oberbauer, R. COVID-19: Implications for immunosuppression in kidney disease and transplantation. Nat. Rev. Nephrol. 2020, 16, 365–367. [Google Scholar] [CrossRef] [PubMed]
- Rammohan, A. Post-transplant immunosuppression and COVID-19: From a double whammy to a mixed blessing. World J. Transplant. 2020, 10, 267–276. [Google Scholar] [CrossRef] [PubMed]
- The Canadian Donation and Transplantation Research Program. COVID-19 International Recommendations for ODT. Available online: https://cdtrp.ca/en/covid-19-international-recommendations-for-odt/ (accessed on 31 July 2021).
- International Society of Heart and Lung Transplantation. Guidance from the International Society of Heart and Lung Transplanation regarding the SARS-CoV-2 Pandemic. Available online: https://ishlt.org/ishlt/media/documents/SARS-CoV-2_Guidance-for-Cardiothoracic-Transplant-and-VAD-center.pdf (accessed on 26 May 2022).
- Gottlieb, R.L.; Nirula, A.; Chen, P.; Boscia, J.; Heller, B.; Morris, J.; Huhn, G.; Cardona, J.; Mocherla, B.; Stosor, V.; et al. Effect of Bamlanivimab as Monotherapy or in Combination with Etesevimab on Viral Load in Patients with Mild to Moderate COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Hasan, L.; Hardgrave, H.; Dare, R.; Giorgakis, E. Risk Factors for Hospital Admissions after Monoclonal Antibodies for COVID-19 Infection in Solid Organ Transplant Recipients. Transpl. Int. 2021, 34, 265–266. [Google Scholar]
- Yetmar, Z.A.; Beam, E.; O’Horo, J.C.; Ganesh, R.; Bierle, D.M.; Brumble, L.; Seville, M.T.; Razonable, R.R. Monoclonal Antibody Therapy for COVID-19 in Solid Organ Transplant Recipients. Open Forum Infect. Dis. 2021, 8, ofab255. [Google Scholar] [CrossRef]
- Dodge, Y. The Concise Encylopedia of Statistics, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Siegel, C. Nonparametric Statistics for Behavioral Sciences; McGraw-Hill: New York, NY, USA, 1988. [Google Scholar]
- Center for Disease Control. Weekly Updates by Select Demographic and Geographics Characteristics. Available online: https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm#SexAndAge (accessed on 19 January 2022).
- Belli, L.S.; Fondevila, C.; Cortesi, P.A.; Conti, S.; Karam, V.; Adam, R.; Coilly, A.; Ericzon, B.G.; Loinaz, C.; Cuervas-Mons, V.; et al. Protective Role of Tacrolimus, Deleterious Role of Age and Comorbidities in Liver Transplant Recipients with Covid-19: Results From the ELITA/ELTR Multi-center European Study. Gastroenterology 2021, 160, 1151–1163.e3. [Google Scholar] [CrossRef]
- Yin, S.; Wang, X.; Song, T. Tacrolimus Use and COVID-19 Infection in Patients After Solid Organ Transplantation. Gastroenterology 2021, 161, 728–730.e1. [Google Scholar] [CrossRef]
- Bertrand, D.; Terrec, F.; Etienne, I.; Chavarot, N.; Sberro, R.; Gatault, P.; Garrouste, C.; Bouvier, N.; Grall-Jezequel, A.; Jaureguy, M.; et al. Opportunistic Infections and Efficacy Following Conversion to Belatacept-Based Therapy after Kidney Transplantation: A French Multicenter Cohort. J. Clin. Med. 2020, 9, 3479. [Google Scholar] [CrossRef]
- Marx, D.; Moulin, B.; Fafi-Kremer, S.; Benotmane, I.; Gautier, G.; Perrin, P.; Caillard, S. First case of COVID-19 in a kidney transplant recipient treated with belatacept. Am. J. Transplant. 2020, 20, 1944–1946. [Google Scholar] [CrossRef]
- Oto, O.A.; Ozturk, S.; Turgutalp, K.; Arici, M.; Alpay, N.; Merhametsiz, O.; Sipahi, S.; Ogutmen, M.B.; Yelken, B.; Altiparmak, M.R.; et al. Predicting the outcome of COVID-19 infection in kidney transplant recipients. BMC Nephrol. 2021, 22, 100. [Google Scholar] [CrossRef]
- Requião-Moura, L.R.; de Sandes-Freitas, T.V.; Viana, L.A.; Cristelli, M.P.; de Andrade, L.G.M.; Garcia, V.D.; de Oliveira, C.M.C.; Esmeraldo, R.D.M.; Filho, M.A.; Pacheco-Silva, A.; et al. High mortality among kidney transplant recipients diagnosed with coronavirus disease 2019: Results from the Brazilian multicenter cohort study. PLoS ONE 2021, 16, e0254822. [Google Scholar] [CrossRef] [PubMed]
- Udomkarnjananun, S.; Kerr, S.J.; Townamchai, N.; Susantitaphong, P.; Tulvatana, W.; Praditpornsilpa, K.; Eiam-Ong, S.; Avihingsanon, Y. Mortality risk factors of COVID-19 infection in kidney transplantation recipients: A systematic review and meta-analysis of cohorts and clinical registries. Sci. Rep. 2021, 11, 20073. [Google Scholar] [CrossRef] [PubMed]
- Yanez, N.D.; Weiss, N.S.; Romand, J.-A.; Treggiari, M.M. COVID-19 mortality risk for older men and women. BMC Public Health 2020, 20, 1742. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Deaths N = 10 (%) | Survivors N = 93 (%) | Total N = 103 (%) | Mortality Rate (%) | p Value | |
|---|---|---|---|---|---|
| Age | 67 (62, 70) | 52 (42, 59) | 54 (42, 62) | <0.001 | |
| Gender | >0.900 | ||||
| Male | 6 (60.0) | 52 (56.0) | 58 (56.3) | 10.3 | |
| Female | 4 (40.0) | 41 (44.0) | 45 (43.7) | 8.9 | |
| Transplant Type | 0.600 | ||||
| Liver | 1 (10.0) | 22 (24.0) | 23 (22.3) | 4.3 | |
| Kidney | 9 (90.0) | 67 (72.0) | 76 (73.8) | 11.8 | |
| SLK | 0 | 4 (4.3) | 4 (3.9) | 0.0 | |
| Total | 10 | 93 | 103 | 9.7 | |
| Comorbidities | |||||
| HTN | 10 (100.0) | 69 (74.0) | 79 (76.7) | 12.7 | 0.110 |
| Diabetes | 7 (70.0) | 37 (40.0) | 44 (42.7) | 15.9 | 0.094 |
| Obesity | 0 (0) | 16 (17.2) | 16 (15.5) | 0 | 0.354 |
| Coronary Artery Disease | 2 (20.0) | 8 (8.6) | 10 (9.7)) | 20.0 | 0.250 |
| Immunosuppression | |||||
| Tacrolimus | 6 (60.0) | 82 (88.0) | 88 (85.4) | 6.8 | 0.037 |
| Cyclosporine | 3 (30.0) | 5 (5.4) | 8 (7.8) | 37.5 | 0.029 |
| Prednisone | 7 (70.0) | 48 (52.0) | 55 (54.4) | 12.7 | 0.300 |
| MMF | 7 (70.0) | 66 (71.0) | 77 (70.9) | 9.1 | >0.900 |
| Sirolimus | 1 (10.0) | 5 (5.4) | 6 (5.8) | 16.7 | 0.500 |
| Belatacept | 2 (20.0) | 3 (3.2) | 5 (4.9) | 40.0 | 0.073 |
| Azathioprine | 0 | 3 (3.2) | 3 (2.9) | 0.0 | >0.900 |
| Beta | HR | 95% CI | p Value | |
|---|---|---|---|---|
| Age > 60 | 2.30 | 10.00 | (2.10–48.00) | 0.003 |
| Immunosuppression | ||||
| Tacrolimus | −1.50 | 0.23 | (0.06–0.81) | 0.022 |
| Cyclosporine | 1.80 | 6.10 | (1.60–24.00) | 0.009 |
| Prednisone | 0.72 | 2.10 | (0.53–7.90) | 0.300 |
| MMF | −0.05 | 0.95 | (0.25–3.70) | 0.950 |
| Sirolimus | 0.59 | 1.80 | (0.23–14.00) | 0.570 |
| Belatacept | 1.80 | 6.10 | (1.30–29.00) | 0.022 |
| Azathioprine | −17.00 | 3.90 × 10−8 | (0-Inf) | 1.000 |
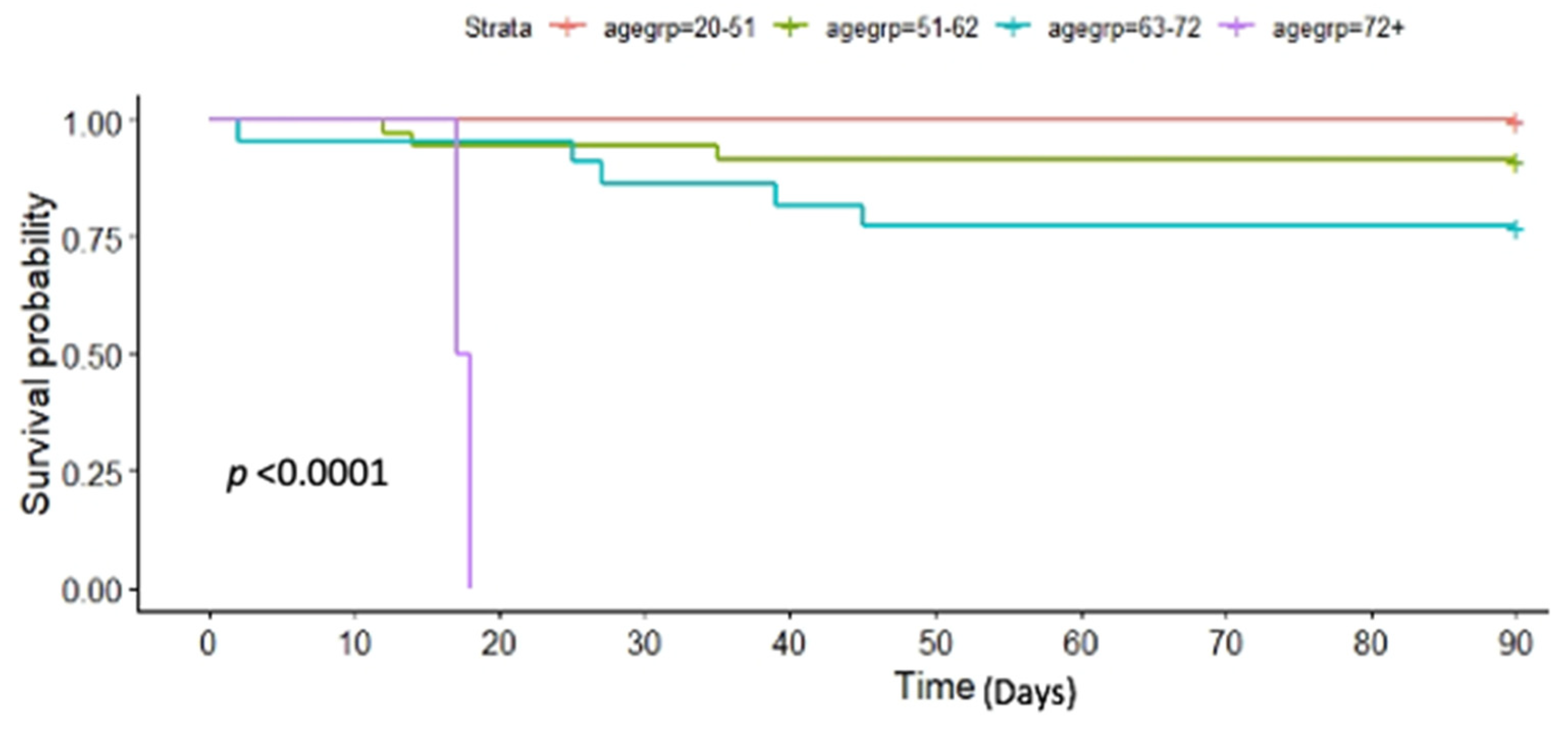
| Number at Risk | ||||
| Age Group (years) | 0-Days | 30-Days | 60-Days | 90-Days |
| 21–51 years | 44 | 44 | 44 | 44 |
| 51–62 years | 35 | 33 | 32 | 32 |
| 63–72 years | 22 | 19 | 17 | 17 |
| 72+ years | 2 | 0 | 0 | 0 |
| Survival (%) | ||||
| Age Group (years) | 0-Days | 30-Days | 60-Days | 90-Days |
| 21–51 years | 100 | 100 | 100 | 100 |
| 51–62 years | 100 | 94.29 | 91.43 | 91.43 |
| 63–72 years | 100 | 86.36 | 77.27 | 77.27 |
| 72+ years | 100 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hardgrave, H.; Wells, A.; Nigh, J.; Osborn, T.; Klutts, G.; Krinock, D.; Rude, M.K.; Bhusal, S.; Burdine, L.; Giorgakis, E. SARS-CoV-2 Infection of Unvaccinated Liver- and Kidney-Transplant Recipients: A Single-Center Experience of 103 Consecutive Cases. Transplantology 2022, 3, 200-207. https://doi.org/10.3390/transplantology3020021
Hardgrave H, Wells A, Nigh J, Osborn T, Klutts G, Krinock D, Rude MK, Bhusal S, Burdine L, Giorgakis E. SARS-CoV-2 Infection of Unvaccinated Liver- and Kidney-Transplant Recipients: A Single-Center Experience of 103 Consecutive Cases. Transplantology. 2022; 3(2):200-207. https://doi.org/10.3390/transplantology3020021
Chicago/Turabian StyleHardgrave, Hailey, Allison Wells, Joseph Nigh, Tamara Osborn, Garrett Klutts, Derek Krinock, Mary Katherine Rude, Sushma Bhusal, Lyle Burdine, and Emmanouil Giorgakis. 2022. "SARS-CoV-2 Infection of Unvaccinated Liver- and Kidney-Transplant Recipients: A Single-Center Experience of 103 Consecutive Cases" Transplantology 3, no. 2: 200-207. https://doi.org/10.3390/transplantology3020021