
Dyslipidemia in Renal Transplant Recipients


1
Faculty of Medicine, Medical University of Gdansk, 80-210 Gdańsk, Poland
2
Department of Nephrology, Transplantology and Internal Medicine, Medical University of Gdansk, 80-211 Gdańsk, Poland
*
Author to whom correspondence should be addressed.
Transplantology 2022, 3(2), 188-199; https://doi.org/10.3390/transplantology3020020
Submission received: 14 April 2022
/
Revised: 12 May 2022
/
Accepted: 17 May 2022
/
Published: 23 May 2022
(This article belongs to the Special Issue Advances in Cardiovascular Complications After Renal Transplantation)
Abstract
:Dyslipidemia is a frequent complication after kidney transplantation (KT) and is an important risk factor for cardiovascular disease (CVD). Renal transplant recipients (RTRs) are considered at high, or very high, risk of CVD, which is a leading cause of death in this patient group. Despite many factors of post-transplant dyslipidemia, the immunosuppressive treatment has the biggest influence on a lipid profile. There are no strict dyslipidemia treatment guidelines for RTRs, but the ones proposing an individual approach regarding CVD risk seem most suitable. Proper diet and physical activity are the main general measures to manage dyslipidemia and should be introduced initially in every patient after KT. In the case of an insufficient correction of lipemia, statins are the basis for hypolipidemic treatment. Statins should be introduced with caution to avoid serious side-effects (e.g., myopathy) or drug-drug interactions, especially with immunosuppressants. To lower the incidence of adverse effects, and improve medication adherence, ezetimibe in combination with statins is recommended. Fibrates and bile sequestrants are not recommended due to their side-effects and variable efficacy. However, several new lipid-lowering drugs like Proprotein convertase subtilisin/Kexin type9 (PCSK9) inhibitors may have promising effects in RTRs, but further research assessing efficacy and safety is yet to be carried out.
1. Introduction
Dyslipidemia is frequent amongst renal transplant recipients (RTRs) and is considered an important cardiovascular disease (CVD) risk factor [1]. About 60% of RTRs have post-transplant lipid abnormalities [2] and almost 40% have a CV-related event within 36 months after transplantation [3]. CVD has emerged as the leading death cause in this patient group [4].
Post-transplant dyslipidemia is characterized by elevated plasma levels of total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), very-low-density lipoprotein cholesterol (VLDL-C) and triglycerides, (TG) but reduced high-density lipoprotein cholesterol (HDLC) [5]. Dyslipidemia may develop de novo after transplantation, as well as a complication of a chronic kidney disease (CKD) (eGFR 15–59 mL/min/1.73 m2) [6]. Prolonged hemodialysis or peritoneal dialysis significantly alters the lipid profile (characterized by very high TG concentrations) [7], and worsens patients’ post-transplant outcomes [8]. Dyslipidemia treatment should be considered an important intervention to improve overall patient post-transplant survival. Statins have become the mainstay of treatment for dyslipidemia, but other therapeutic methods should also be considered [9,10,11].
2. Dyslipidemia Prevalence
Hyperlipidemia is the most common type of dyslipidemia in RTRs [1,12,13]. TC concentration rises by about 27% compared with results preceding KT [14]. Moreover, VLDL and LDL with higher concentrations of TG are observed [15]. Triglyceride-rich LDLs are prone to oxidation, and thus have a more atherogenic character [16]. HDL-C levels in RTRs are usually comparable or slightly reduced compared to the general population [12,13].
3. Causes of Post-Transplant Dyslipidemia
The pathophysiology of post-transplant dyslipidemia is multicausal and includes modifiable and nonmodifiable risk factors (Table 1) [2]. After transplantation, the sudden improvement of life quality can lead to an alleviation of dietary restrictions, previously dictated by impaired kidney function [17]. Following cholesterol- and fructose-rich diets is frequent amongst RTRs [18]. Obesity incidence rises by 34% after KT, and obesity is considered to be a factor of long-term graft dysfunction [19]. Weight gain may also contribute to the development of insulin resistance, and new-onset diabetes after transplantation (NODAT) thereafter [20]. Therefore, maintenance of a healthy weight should be an effective tool to reduce post-transplant complications.
A sedentary lifestyle is a frequently omitted factor leading to dyslipidemia [21]. Patients on prolonged hemodialysis prior to transplantation exhibit extremely low physical performance, caused by an underlying disease, sarcopenia, malnutrition, and total body weakness [22]. After KT, many patients are also concerned about the safety of physical activity and its potentially detrimental effect on the graft [23].
Deficient doctor-patient communication could hinder patients’ understanding of their illness; thus, comprehensive post-transplant health and lifestyle recommendations should be created and implemented [24]. Despite all this, immunosuppressive therapy is considered the main reason for the post-transplant lipid characteristics [13,25]. Widely used medications conducive to dyslipidemia include calcineurin inhibitors (CNI) (cyclosporine in particular), mTOR inhibitors, and glucocorticoids. Numerous studies indicate higher drug doses and the intensity of treatment in positive correlation with dyslipidemia [13,25].
4. Role of Immunosuppression in Dyslipidemia Development
New immunosuppressive therapy schemes emphasize the individualization of treatment. It is especially important in the elderly RTRs population where the probability of adverse effects of treatment is relatively high [26]. Medications with the most dyslipidemic potential are glucocorticoids, calcineurin inhibitors (CNI) particularly cyclosporine, and mTOR inhibitors (Table 2) [1,2,13,27]. Immunosuppression plays an important role in preserving the graft, however, medication schemes should be optimized in order to prevent dyslipidemia and drug-drug interactions causing worsening of CVD.
4.1. Glucocorticoids
Glucocorticoids may alter the lipid profile via multiple pathways. Glucocorticoids elevate TG concentration by induction of hepatic lipogenesis (mainly VLDL), inhibition of lipoprotein lipase (LPL), hepatic lipase (HL), and downregulation of hepatic LDL receptors (LDL-R). It results in more intensive lipid production and diminished LDL and VLDL clearance. Increased TC levels are caused by steroid stimulation of HMG CoA reductase—a rate-limiting enzyme in cholesterol production [1,13]. Moreover, glucocorticoids induce insulin resistance and sudden post-operative weight gain through increased appetite [28,29]. VLDL, TC, and TG levels have been reported to be elevated in a dose-dependent manner [29]. More recent studies report relatively lower TG concentration in RTRs due to a glucocorticoid withdrawal tendency [1,21]. Steroid withdrawal is associated with significantly reduced cholesterol concentrations, and slight weight reduction but may be responsible for the higher rate of early acute graft rejection. It also depends on immunosuppressive agents and dosage used in treatment protocol [30,31]. Moreover, steroid avoidance and steroid maintenance therapy have comparable outcomes on lipid profiles in immunologically low-risk RTRs [32].
4.2. Calcineurin Inhibitors (CNI)
CsA is metabolized in the liver and inhibits bile acid production and secretion—a way of cholesterol excretion. Biliary cholesterol elimination is a final phase of reverse cholesterol transport from peripheral cells to the liver. An impaired cholesterol clearance mechanism may cause atherogenic plaque formation [35,36]. CsA decrease the lipolytic activity of LPL and HL and stimulates hepatic lipogenesis. Apolipoprotein C-III (Apo-CIII) levels are elevated in RTRs treated with CNI. Since Apo-CIII interferes with multiple LPL, HL, and LDL-R functions, its role in triglyceridemia may be important [37]. Dyslipidemia occurs more frequently in RTRs receiving CsA compared to tacrolimus [38]. Another downside of CNI use is nephrotoxicity, which is more expressed in the elderly RTRs population, hence it should be used with caution [39].
4.3. Mammalian Target of Rapamycin (mTOR) Inhibitors
Sirolimus and everolimus are less potent than CNI immunosuppressants. They also have anti-proliferative properties, and are applied in oncology as well [40,41]. Regrettably, dyslipidemia is one of the most common adverse effects in patients treated with mTOR inhibitors [2,36]. Increased apolipoprotein B-100 (ApoB100) levels have been reported in RTRs receiving sirolimus with further elevation levels of VLDL and LDL. The exact pathogenesis remains unknown, though several mechanisms may participate like decreased catabolism of ApoB100, the increased secretion of VLDL, and the increased expression of adipose tissue lipase. Furthermore, sirolimus inhibits LDL-R and decreases LDL hepatic uptake and the incorporation of FFA into VLDL [42,43]. It is worth mentioning that everolimus and sirolimus have a similar effect on dyslipidemia, irrespective of combined immunosuppressants [44].
On the contrary, mTOR inhibitors improve the function of the endothelium through the inhibition of inflammatory cytokines and modulation of the T-cells and monocytes, which can result in less proliferation of the smooth cell, and stabilization of the atheromatous plaque [45]. However, due to the inconclusive results of the randomized controlled trials on mTOR inhibitors and their influence on the CVD, an unequivocal advantage of anti-inflammatory effects over dyslipidemic potential cannot be proven [46,47].
4.4. Purine Synthesis Inhibitors
Antiproliferative medication such as mycophenolate-mofetil or azathioprine has little impact on lipid levels [48].
4.5. Belatacept—An Upcoming Revolution?
In 2011, a new CD28/CTLA-4 co-stimulation pathway blocker was administered and since then has been shown as an up-and-coming option for maintenance immunosuppression [49]. Compared with CNI, belatacept has positively influenced graft survival and elevated the glomerular filtration rate (GFR). Additionally, belatacept is associated with fewer incidents of hypertension, dyslipidemia, and NODAT [50,51]. However, due to qualification criteria (such as positive EBV-IgG status), low availability, little data on treatment outcomes, and conservative treatment methods, a low proportion of patients receive this drug both in America and Europe [52].
5. Measures to Prevent Dyslipidemia
Physical activity and a proper diet are vital determinants of the lower incidence of CVD in patients of all ages [9]. Physical activity before KT predicts all-cause mortality in RTRs [53] and is associated with better graft function after KT [54]. Regular physical performance positively correlates with elevated HDL-C (i.a. elderly population) [55], lower levels of TG (in overweight and obese adults), and positive qualitative changes in lipoproteins [56].
RTRs exhibit decreased physical activity compared to the general population, yet were higher than the dialysis population [57]. A systematic review of 24 studies of exercise programs for RTRs concluded that 20–60 min of aerobic and resistance training up to three times a week for approx. six months resulted in substantially increased cardiorespiratory capacity, maximum heart rate, and muscle strength [58].
A healthy diet has been proven to lower cardiovascular risk [9,59]. Obesity is frequent amongst RTRs, although weight loss should not be considered the main nutritional goal. National Kidney Foundation Guidelines from 2020 recommend 25–35 kcal/kg/d intake for RTRs [60]. No specific eating patterns have been created besides the suggested micro and macronutrients intake. Less than 30% of the total caloric intake should come from fats. Reference values for carbohydrate intake vary from 45 to 60%, yet, most importantly, additive sugars should not exceed 10% [61]. Immediately after surgery, protein demand ranges between 1.2 g/kg/d to 2 g/kg/d to compensate for the negative nitrogen balance [62].
The average transplanted patient may have difficulties understanding and implementing isolated nutrients references. Hence, patients should be educated and provided with dietary patterns. After all, the DASH diet and Mediterranean diet (MD) have been demonstrated to be the most beneficial for RTRs due to the emphasis on less meat and processed foods consumption, and an increased intake of fresh and plant-based foods [61].
Moreover, high adherence to an MD improves the endothelial function and decreases inflammation [18].
6. Pharmacological Treatment of Dyslipidemia
Reduction of cardiovascular risk by lowering LDL-C is the main target of hypolipidemic treatment in RTRs, and dyslipidemia management is similar to that recommended for non-transplant patients with CKD. American 2018 [10] and European 2019 [9] guidelines both recommend identifying RTRs at high, or very high, risk of CVD, particularly those with LDL-C ≥ 1.8 mmol/L (70 mg/dL), and consider statins first-line drugs with ezetimibe being the second-line treatment. In order to estimate the patients’ risk of CVD, physicians may use a calculator based on several readily-available pieces of information about the patient [59].
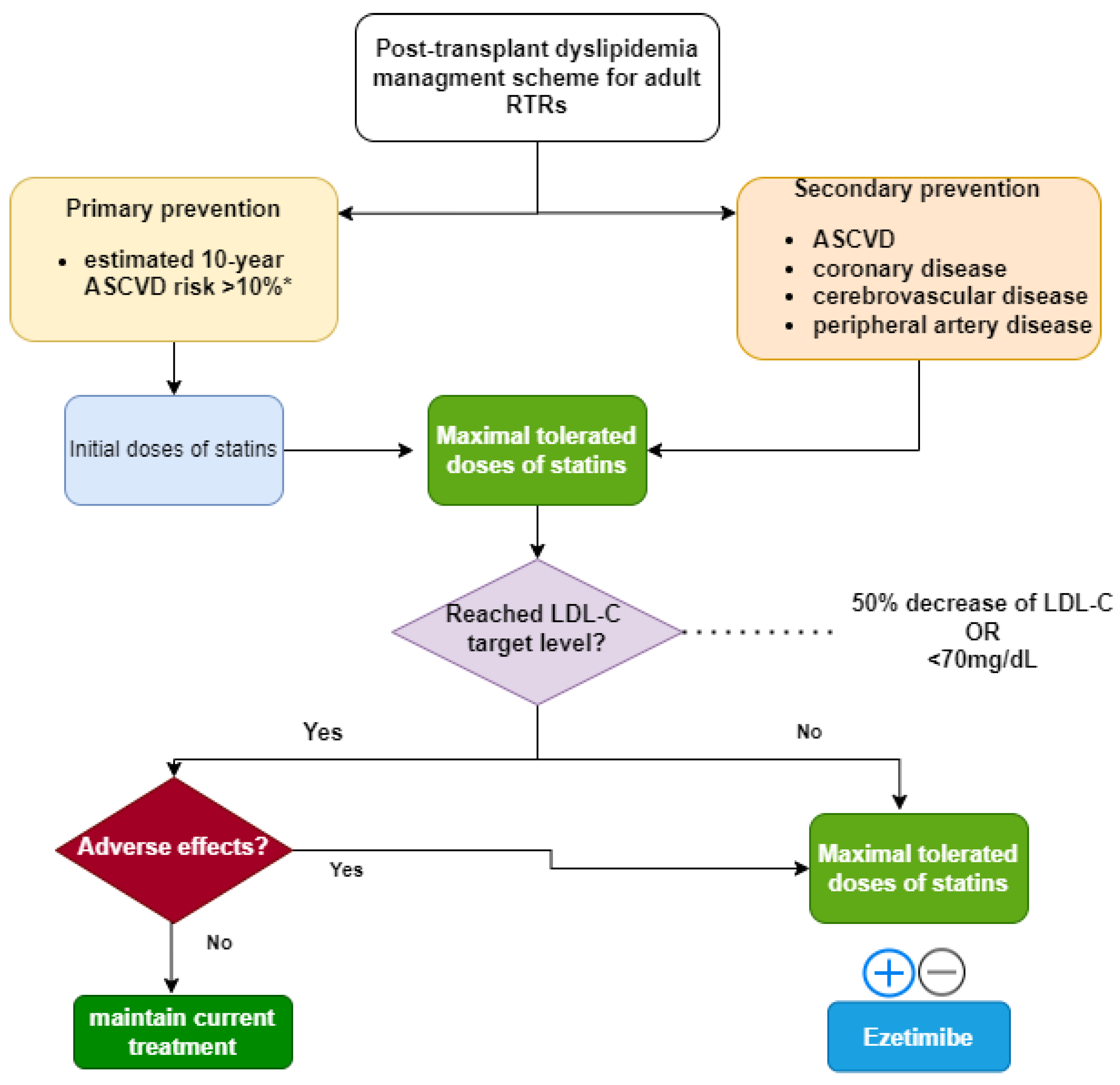
While European guidelines state a strict “treat-to-target” approach, the KDIGO 2013 guideline proposes a rather unrestricted approach, noting the polypharmacy problem and the potential adverse effects of lipid-lowering therapy in transplant patients. Hence, the American "fire and forget" [11,63] strategy will be discussed, owing to its holistic and patient-orientated character (Figure 1).
Management of dyslipidemia depends on whether the patient has established atherosclerotic cardiovascular disease (ASCVD) or not. A lipid profile measurement should be carried out before, and four to 12 weeks after, the introduction of pharmacological treatment of dyslipidemia to determine medication adherence, and then repeated every three to 12 months [64].
Due to the KDIGO 2013 guidelines, lower initial doses of statins are recommended and the dose may be increased, whether the patient receives cyclosporine or not, to avoid adverse effects like severe myopathy (Table 3) [11].
6.1. Statins
Statins are HMG-CoA (3-hydroxy-3-methyl-glutaryl-coenzyme A) reductase inhibitors and they are potent hypolipidemic drugs that markedly reduce LDL serum concentration. Reduction in intra-hepatocyte cholesterol levels causes enhanced LDL-R expression and increased uptake of LDL and, among others, TG rich ApoB particles. Statins are suggested to have a pleiotropic effect, as they inhibit the rate control enzyme of the mevalonate pathway, a precursor for non-steroid compounds. Some experimental studies suggest statins may have anti-inflammatory and antioxidative effects, important in CVD prevention [65,66,67].
Statins are generally well-tolerated, nonetheless, some adverse events like nausea, vomiting, and muscle and joint pain cannot be overlooked, thus this may contribute to poor medication adherence. Less frequent but serious side-effects of statin therapy include NODAT and hepatotoxicity [9]. In extreme cases, rhabdomyolysis may occur, a life-threatening condition that can lead to rapid kidney dysfunction [68].
Statins have no proven protective effect on graft rejection or patient post-transplant survival [69]. However, in the multicenter, double-blind study (ALERT) on 2102 RTRs treated with fluvastatin, the incidence of cardiac arrest deaths and non-fatal myocardial infarctions was reduced in favor of the research group, yet with no significant influence on the overall death rate [70]. The RTRs population is unique, taking into account the risk factors associated with transplantation itself. Therefore, even lacking outcomes in big controlled trials, RTRs with well-functioning grafts and increased risk of CVD may benefit from statin treatment [9,11,63].
Statins Drug-Drug Interactions
Drug-drug interactions may be frequent in the transplant population due to the high prevalence of polypharmacy [71]. Statins are extensively metabolized in the liver by cytochrome P450 complex, particularly CYP3A4. Fluvastatin, pravastatin, pitavastatin, and rosuvastatin are metabolized by different cytochromes and they rarely get into drug-drug interactions. Most statins are lipophilic except hydrophilic pravastatin and rosuvastatin, which underlies their high safety profile [72].
6.2. Ezetimibe
Ezetimibe inhibits the uptake of cholesterol in the intestines by interacting with NPC1 protein [75]. It lowers both TC and TG levels, yet has no influence on HDL-C. Ezetimibe is considered to be a second-line drug due to its lower hypolipidemic potential (lowers LDL-C by 13–20%) [11]. Both American and European guidelines recommend ezetimibe (10 mg) in combination with statins in patients at high, and very high, risk of CVD or in secondary prevention, in order to achieve target LDL concentrations [9,10]. Ezetimibe may be prescribed as an alternative in the case of statin intolerance on the inability to reach a therapeutic dose. Ezetimibe combined with maximal doses of statins may reduce hypercholesterolemia and triglyceridemia in RTRs [76], with no significant influence on creatine kinase concentration and kidney function [77].
6.3. Bile Sequestrants
Bile acid sequestrants like cholestyramine prevent bile reabsorption in the intestines and lower serum cholesterol levels [78]. Cholestyramine insignificantly affects renal function in the general population [79]. Due to side effects like constipation, the elevation of triglycerides, and interfering with the absorption of other drugs, bile sequestrants are rarely used [9].
6.4. Fibrates
Fibrates are agonists of PPAR-a (Peroxisome Proliferator-Activated Receptor Alpha), regulating the lipid and lipoprotein metabolism. They are efficient in lowering fasting TG serum levels and slightly elevating HDL concentration. Their TG lowering effect is highly dependent on the initial TG level [9]. Fibrates modestly reduce CV events in primary prevention. However, a combination of statins with fibrates raises the risk of myopathy, thus the concomitant use of these drugs must be avoided [80]. In the case of the coexistence of triglyceridemia and hypercholesterolemia, the use of fenofibrate rather than gemfibrozil is recommended because of the lower risk of severe myopathy. Despite having a mild LDL-lowering potential, fibrates are not supported by RCTs as add-on drugs to statin therapy [10].
7. Future Perspectives to Reduce LDL-C
7.1. PCSK9 Inhibitors
Proprotein convertase subtilisin/Kexin 9 (PCSK9) is a protein expressed mainly in hepatocytes involved in the regulation of LDL-R. Higher circulating PCSK9 levels lead to a lower rate of LDL ApoB catabolism and increased risk of NODAT [81,82]. There is a new class of drugs, PCSK9 inhibitors, and two of them (alirocumab and evolocumab) have been approved for clinical use. PCSK9 inhibitors contribute to a significant reduction of LDL-C concentration (by 60% depending on the dose) [9] and are considered additional therapy to statin and ezetimibe for patients with ASCVD and familial hypercholesterolemia [83]. These agents also lower TG and Lp(a) concentrations. The ODYSSEY trial on 18,924 patients after hospitalization for acute MI or unstable angina reported a significant reduction of all-cause mortality, yet no significant outcome on the CV death rate [84]. Due to little adverse effects, like itching of the injection site, these drugs have high medication adherence [84]. It is worth mentioning that PCSK9 inhibitors have a strong safety profile compared with standard lipid-lowering therapy in solid organ transplantation [85]. In conclusion, PCSK9 inhibitors administration in RTRs may have promising outcomes in treating dyslipidemia. However, due to high costs, lack of big RCT trials, and guidance, these drugs are not recommended for RTRs.
7.2. Inclisiran
An alternative for targeting PCSK9 might be small interfering RNA (siRNA), which inhibits the synthesis of the protein on a molecular level [86]. Inclisiran is reported to lower LDL-C levels by 50% with no specific adverse effects observed. Currently, a five-year trial is testing inclisiran efficacy in patients prior to MI and stroke [9].
7.3. Bempedoic Acid
Bempedoic acid is an incoming molecule that inhibits cholesterol synthesis through interaction with ATP citrate lyase. It reduces LDL-C levels by 30% and 50% in monotherapy and in combination with ezetimibe, respectively. Bempedoic acid has been approved by the FDA for adults requiring additional lowering of LDL-C, and has been recommended for treating adults with primary hypercholesterolemia and mixed dyslipidemia [87] In comparison with statins, bempedoic acid has no muscular side effects, and can be seen as an alternative for RTRs with statin intolerance. However, bempedoic acid can elevate uric acid, and therefore should be prescribed with caution in patients with hyperuricemia and a history of gout. In December 2022, outcomes of the CLEAR trial will reveal if bempedoic acid lowers CVD incidence in patients with statin intolerance [88].
8. Conclusions
Dyslipidemia is frequent and has a unique scheme in RTRs. Guidelines consistently indicate that RTRs are at high, or very high, risk of CVD. A fasting lipid profile including TC, LDL-C, HDL-C, and TG should be obtained in every transplant patient, but further follow-up is not required in the majority of cases, since the main indication for treatment is individual CVD risk rather than LDL-C concentration. Lifestyle measures like proper diet, physical exercise, and the tailoring of immunosuppressive treatment should be introduced in every transplant patient case to prevent and treat dyslipidemia. If preventative measures are unsatisfactory, initial doses of statins should be introduced as the first-line treatment of dyslipidemia. Fluvastatin, rosuvastatin, atorvastatin, pravastatin, and simvastatin should be considered first due to their high safety profiles. Statin doses should be titrated with the caution of drug interactions and possible side effects like acute myopathy. In the case of severe hypercholesterolemia or statin intolerance, ezetimibe may be considered with lower doses of statins. When hypertriglyceridemia is a dominant issue, a dietitian consultation is advisable in order to introduce a Mediterranean or DASH diet. Fibrates should be avoided because they may cause transient serum creatinine elevation and reported cases of myositis and rhabdomyolysis. New dyslipidemia treatment with PCSK9 inhibitors or bempedoic acid might be an effective alternative for current dyslipidemia treatment, but further research is needed.
Author Contributions
Conceptualization, K.C. and Z.H.; methodology, K.C.; data curation, K.C.; writing—original draft preparation, K.C.; writing—review and editing, Z.H. and A.D.-Ś.; supervision, Z.H. and A.D.-Ś.; project administration, K.C. and Z.H.; funding acquisition, A.D.-Ś. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Agarwal, A.; Prasad, G.V.R. Post-Transplant Dyslipidemia: Mechanisms, Diagnosis and Management. World J. Transplant. 2016, 6, 125. [Google Scholar] [CrossRef] [PubMed]
- Badiou, S.; Cristol, J.P.; Mourad, G. Dyslipidemia Following Kidney Transplantation: Diagnosis and Treatment. Curr. Diabetes Rep. 2009, 9, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Shirali, A.C.; Bia, M.J. Management of Cardiovascular Disease in Renal Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2008, 3, 491–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heleniak, Z.T.; Illersperger, S.; Brakemeier, S.; Dębska-Ślizień, A.; Bach, P.; Budde, K.; Halleck, F. Influence of Lipid Profile and Statin Administration on Arterial Stiffness in Renal Transplant Recipients. Cardiol. J. 2022, 29, 263–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikolasevic, I.; Žutelija, M.; Mavrinac, V.; Orlic, L. Dyslipidemia in Patients with Chronic Kidney Disease: Etiology and Management. Int. J. Nephrol. Renov. Dis. 2017, 10, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Kosugi, T.; Eriguchi, M.; Yoshida, H.; Tasaki, H.; Fukata, F.; Nishimoto, M.; Matsui, M.; Samejima, K.I.; Iseki, K.; Fujimoto, S.; et al. Association between Chronic Kidney Disease and New-Onset Dyslipidemia: The Japan Specific Health Checkups (J-SHC) Study. Atherosclerosis 2021, 332, 24–32. [Google Scholar] [CrossRef]
- Piecha, G.; Adamczak, M.; Ritz, E. Dyslipidemia in Chronic Kidney Disease: Pathogenesis and Intervention. Pol. Arch. Med. Wewn. 2009, 119, 487–492. [Google Scholar] [CrossRef]
- Dębska-Ślizień, A.; Bzoma, B.; Rutkowski, B. Wyprzedzające Przeszczepianie Nerek. Forum Nefrol. 2009, 2, 84–89. [Google Scholar]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; de Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular RiskThe Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, E1082–E1143. [Google Scholar] [CrossRef]
- Wanner, C.; Tonelli, M. KDIGO Clinical Practice Guideline for Lipid Management in CKD: Summary of Recommendation Statements and Clinical Approach to the Patient. Kidney Int. 2014, 85, 1303–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pannu, H.S.; Singh, D.; Sandhu, J.S. Lipid Profile before and after Renal Transplantation—A Longitudinal Study. Ren. Fail. 2003, 25, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Massy, Z.A.; Kasiske, B.L. Post-Transplant Hyperlipidemia: Mechanisms and Management. J. Am. Soc. Nephrol. 1996, 7, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Corsini, A. The Safety of HMG-CoA Reductase Inhibitors in Special Populations at High Cardiovascular Risk. Cardiovasc. Drugs Ther. 2003, 17, 265–285. [Google Scholar] [CrossRef] [PubMed]
- Quaschning, T.; Mainka, T.; Nauck, M.; Rump, L.C.; Wanner, C.; Krämer-Guth, A. Immunosuppression Enhances Atherogenicity of Lipid Profile after Transplantation. Kidney Int. Suppl. 1999, 56, S235–S237. [Google Scholar] [CrossRef] [Green Version]
- Van den Dorpel, M.A.; Ghanem, H.; Rischen-Vos, J.; Man In’t Veld, A.J.; Jansen, H.; Weimar, W. Low-Density Lipoprotein Oxidation Is Increased in Kidney Transplant Recipients. Transplant. Int. 1996, 9, S54–S57. [Google Scholar] [CrossRef]
- Sabbatini, M.; Ferreri, L.; Pisani, A.; Capuano, I.; Morgillo, M.; Memoli, A.; Riccio, E.; Guida, B. Nutritional Management in Renal Transplant Recipients: A Transplant Team Opportunity to Improve Graft Survival. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Kluch, M.; Kurnatowska, I.; Matera, K.; Łokieć, K.; Puzio, T.; Czkwianianc, E.; Grzelak, P. Nutrition Trends in Patients over the Long Term after Kidney Transplantation. Transplant. Proc. 2020, 52, 2357–2362. [Google Scholar] [CrossRef]
- Nöhre, M.; Schieffer, E.; Hanke, A.; Pape, L.; Schiffer, L.; Schiffer, M.; de Zwaan, M. Obesity After Kidney Transplantation—Results of a KTx360°Substudy. Front. Psychiatry 2020, 11, 399. [Google Scholar] [CrossRef]
- Zielińska, K.; Kukulski, L.; Wróbel, M.; Przybyłowski, P.; Zakliczyński, M.; Strojek, K. Prevalence and Risk Factors of New-Onset Diabetes After Transplantation (NODAT). Ann. Transplant. 2021, 26, e926556-1. [Google Scholar] [CrossRef]
- Ponticelli, C.; Favi, E. Physical Inactivity: A Modifiable Risk Factor for Morbidity and Mortality in Kidney Transplantation. J. Pers. Med. 2021, 11, 927. [Google Scholar] [CrossRef] [PubMed]
- Moorthi, R.N.; Avin, K.G. Clinical Relevance of Sarcopenia in Chronic Kidney Disease. Curr. Opin. Nephrol. Hypertens. 2017, 26, 219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, E.J.; Prohaska, T.R.; Gallant, M.; Siminoff, L.A. Self-Care Strategies and Barriers among Kidney Transplant Recipients: A Qualitative Study. Chronic Illn. 2009, 5, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballesteros, F.; Allard, J.; Durand, C.; Cardinal, H.; Lalonde, L.; Fortin, M.-C. Kidney Transplant Recipients’ Perspectives on Cardiovascular Disease and Related Risk Factors After Transplantation: A Qualitative Study. Transplant. Direct 2017, 3, e162. [Google Scholar] [CrossRef]
- Ponticelli, C.; Arnaboldi, L.; Moroni, G.; Corsini, A. Treatment of Dyslipidemia in Kidney Transplantation. Expert Opin. Drug Saf. 2020, 19, 257–267. [Google Scholar] [CrossRef]
- Jankowska, M. Immunosuppressive Therapy Following Kidney Transplantation in Elderly Recipients. Ren. Dis. Transplant. Forum 2021, 14, 58–65. [Google Scholar] [CrossRef]
- Rostaing, L.; Vincenti, F.; Grinyõ, J.; Rice, K.M.; Bresnahan, B.; Steinberg, S.; Gang, S.; Gaite, L.E.; Moal, M.C.; Mondragõn-Ramirez, G.A.; et al. Long-Term Belatacept Exposure Maintains Efficacy and Safety at 5 Years: Results from the Long-Term Extension of the BENEFIT Study. Am. J. Transplant. 2013, 13, 2875–2883. [Google Scholar] [CrossRef]
- Ponticelli, C.; Favi, E.; Ferraresso, M. New-Onset Diabetes after Kidney Transplantation. Medicina 2021, 57, 250. [Google Scholar] [CrossRef]
- Geer, E.B.; Islam, J.; Buettner, C. Mechanisms of Glucocorticoid-Induced Insulin Resistance: Focus on Adipose Tissue Function and Lipid Metabolism. Endocrinol. Metab. Clin. N. Am. 2014, 43, 75. [Google Scholar] [CrossRef] [Green Version]
- Ratcliffe, P.J.; Dudley, C.R.K.; Higgins, R.M.; Firth, J.D.; Smith, B.; Morris, P.J. Randomised Controlled Trial of Steroid Withdrawal in Renal Transplant Recipients Receiving Triple Immunosuppression. Lancet 1996, 348, 643–648. [Google Scholar] [CrossRef]
- Kato, Y.; Tojimbara, T.; Iwadoh, K.; Koyama, I.; Nanmoku, K.; Kai, K.; Sannomiya, A.; Nakajima, I.; Fuchinoue, S.; Teraoka, S. Early Steroid Withdrawal Protocol with Basiliximab, Cyclosporine and Mycophenolate Mofetil in Renal-Transplant Recipients. Int. Immunopharmacol. 2006, 6, 1984–1992. [Google Scholar] [CrossRef] [PubMed]
- Ekberg, J.; Baid-Agrawal, S.; Jespersen, B.; Källén, R.; Rafael, E.; Skov, K.; Lindnér, P. A Randomized Controlled Trial on Safety of Steroid Avoidance in Immunologically Low-Risk Kidney Transplant Recipients. Kidney Int. Rep. 2022, 7, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Arnol, M.; Naumovic, R.; Dimitrov, E.P.; Racki, S.; Bucsa, C.A.; Covic, A.; Mitic, I.; Vavic, N.; Radovanovic, R.M.V.; Zibar, L.; et al. Immunosuppressive Regimens Following Kidney Transplantation in Five European Countries: The Observational RECORD Study. Transplant. Rep. 2020, 5, 100061. [Google Scholar] [CrossRef]
- Neuwirt, H.; Rudnicki, M.; Schratzberger, P.; Pirklbauer, M.; Kronbichler, A.; Mayer, G. Immunosuppression after Renal Transplantation. Memo-Mag. Eur. Med. Oncol. 2019, 12, 216–221. [Google Scholar] [CrossRef] [Green Version]
- Dikkers, A.; Tietge, U.J. Biliary Cholesterol Secretion: More than a Simple ABC. World J. Gastroenterol. 2010, 16, 5936–5945. [Google Scholar] [CrossRef] [PubMed]
- Riella, L.V.; Gabardi, S.; Chandraker, A. Dyslipidemia and Its Therapeutic Challenges in Renal Transplantation. Am. J. Transplant. 2012, 12, 1975–1982. [Google Scholar] [CrossRef] [PubMed]
- Badiou, S.; Garrigue, V.; Dupuy, A.M.; Chong, G.; Cristol, J.P.; Mourad, G. Small Dense Low-Density Lipoprotein in Renal Transplant Recipients: A Potential Target for Prevention of Cardiovascular Complications? Transplant. Proc. 2006, 38, 2314–2316. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.O.; Barr, M.L.; Radovancevic, B.; Renlund, D.G.; Mentzer, R.M.; Smart, F.W.; Tolman, D.E.; Frazier, O.H.; Young, J.B.; Vanveldhuisen, P. A Randomized, Multicenter Comparison of Tacrolimus and Cyclosporine Immunosuppressive Regimens in Cardiac Transplantation: Decreased Hyperlipidemia and Hypertension with Tacrolimus. J. Heart Lung Transplant. 1999, 18, 336–345. [Google Scholar] [CrossRef]
- Naesens, M.; Kuypers, D.R.J.; Sarwal, M. In-Depth Review Calcineurin Inhibitor Nephrotoxicity. Clin. J. Am. Soc. Nephrol. 2009, 4, 481–508. [Google Scholar] [CrossRef] [Green Version]
- Baroja-Mazo, A.; Revilla-Nuin, B.; Ramírez, P.; Pons, J.A. Immunosuppressive Potency of Mechanistic Target of Rapamycin Inhibitors in Solid-Organ Transplantation. World J. Transplant. 2016, 6, 183. [Google Scholar] [CrossRef]
- Zou, Z.; Tao, T.; Li, H.; Zhu, X. mTOR Signaling Pathway and mTOR Inhibitors in Cancer: Progress and Challenges. Cell Biosci. 2020, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Morrisett, J.D.; Abdel-Fattah, G.; Hoogeveen, R.; Mitchell, E.; Ballantyne, C.M.; Pownall, H.J.; Opekun, A.R.; Jaffe, J.S.; Oppermann, S.; Kahan, B.D. Effects of Sirolimus on Plasma Lipids, Lipoprotein Levels, and Fatty Acid Metabolism in Renal Transplant Patients. J. Lipid Res. 2002, 43, 1170–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoogeveen, R.C.; Ballantyne, C.M.; Pownall, H.J.; Opekun, A.R.; Hachey, D.L.; Jaffe, J.S.; Oppermann, S.; Kahan, B.D.; Morrisett, J.D. Effect of Sirolimus on the Metabolism of ApoB100-Containing Lipoproteins in Renal Transplant Patients. Transplantation 2001, 72, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Klawitter, J.; Nashan, B.; Christians, U. Everolimus and Sirolimus in Transplantation-Related but Different. Expert Opin. Drug Saf. 2015, 14, 1055. [Google Scholar] [CrossRef]
- Kasiske, B.L.; de Mattos, A.; Flechner, S.M.; Gallon, L.; Meier-Kriesche, H.-U.; Weir, M.R.; Wilkinson, A. Mammalian Target of Rapamycin Inhibitor Dyslipidemia in Kidney Transplant Recipients. Am. J. Transplant. 2008, 8, 1384–1392. [Google Scholar] [CrossRef] [PubMed]
- Legendre, C.; Campistol, J.M.; Squifflet, J.P.; Burke, J.T. Cardiovascular Risk Factors of Sirolimus Compared with Cyclosporine: Early Experience from Two Randomized Trials in Renal Transplantation. Transplant. Proc. 2003, 35, S151–S153. [Google Scholar] [CrossRef]
- Topilsky, Y.; Hasin, T.; Raichlin, E.; Boilson, B.A.; Schirger, J.A.; Pereira, N.L.; Edwards, B.S.; Clavell, A.L.; Rodeheffer, R.J.; Frantz, R.P.; et al. Sirolimus as Primary Immunosuppression Attenuates Allograft Vasculopathy with Improved Late Survival and Decreased Cardiac Events after Cardiac Transplantation. Circulation 2012, 125, 708–720. [Google Scholar] [CrossRef]
- Akman, B.; Uyar, M.; Afsar, B.; Sezer, S.; Ozdemir, F.N.; Haberal, M. Lipid Profile during Azathioprine or Mycophenolate Mofetil Combinations with Cyclosporine and Steroids. Transplant. Proc. 2007, 39, 135–137. [Google Scholar] [CrossRef]
- Crepeau, R.L.; Ford, M.L. Challenges and Opportunities in Targeting the CD28/CTLA-4 Pathway in Transplantation and Autoimmunity. Expert Opin. Biol. Ther. 2017, 17, 1001. [Google Scholar] [CrossRef]
- Vanrenterghem, Y.; Bresnahan, B.; Campistol, J.; Durrbach, A.; Grinyó, J.; Neumayer, H.H.; Lang, P.; Larsen, C.P.; Mancilla-Urrea, E.; Pestana, J.M.; et al. Belatacept-Based Regimens Are Associated with Improved Cardiovascular and Metabolic Risk Factors Compared with Cyclosporine in Kidney Transplant Recipients (BENEFIT and BENEFIT-EXT Studies). Transplantation 2011, 91, 976–983. [Google Scholar] [CrossRef]
- Vincenti, F.; Charpentier, B.; Vanrenterghem, Y.; Rostaing, L.; Bresnahan, B.; Darji, P.; Massari, P.; Mondragon-Ramirez, G.A.; Agarwal, M.; di Russo, G.; et al. A Phase III Study of Belatacept-Based Immunosuppression Regimens versus Cyclosporine in Renal Transplant Recipients (BENEFIT Study). Am. J. Transplant. 2010, 10, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Westhoff, T.H. Belatacept in Renal Transplantation—Quo Vadis? Transl. Androl. Urol. 2016, 5, 953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosas, S.E.; Reese, P.P.; Huan, Y.; Doria, C.; Cochetti, P.T.; Doyle, A. Pretransplant Physical Activity Predicts All-Cause Mortality in Kidney Transplant Recipients. Am. J. Nephrol. 2012, 35, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, E.J.; Prohaska, T.R.; Gallant, M.P.; Sehgal, A.R.; Strogatz, D.; Yucel, R.; Conti, D.; Siminoff, L.A. Longitudinal Analysis of Physical Activity, Fluid Intake, and Graft Function among Kidney Transplant Recipients. Transpl. Int. 2009, 22, 990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landi, F.; Russo, A.; Cesari, M.; Pahor, M.; Bernabei, R.; Onder, G. HDL-Cholesterol and Physical Performance: Results from the Ageing and Longevity Study in the Sirente Geographic Area (IlSIRENTE Study). Age Ageing 2007, 36, 514–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelley, G.A.; Kelley, K.S.; Vu Tran, Z. Aerobic Exercise, Lipids and Lipoproteins in Overweight and Obese Adults: A Meta-Analysis of Randomized Controlled Trials. Int. J. Obes. 2005, 29, 881. [Google Scholar] [CrossRef] [Green Version]
- De Smet, S.; van Craenenbroeck, A.H. Exercise Training in Patients after Kidney Transplantation. Clin. Kidney J. 2021, 14, ii15–ii24. [Google Scholar] [CrossRef]
- Calella, P.; Hernández-Sánchez, S.; Garofalo, C.; Ruiz, J.R.; Carrero, J.J.; Bellizzi, V. Exercise Training in Kidney Transplant Recipients: A Systematic Review. J. Nephrol. 2019, 32, 567–579. [Google Scholar] [CrossRef]
- Goff, D.C.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, 49–73. [Google Scholar] [CrossRef] [Green Version]
- Akbulut, G.; Gencer-Bingol, F. Medical Nutritional Therapy for Renal Transplantation in the COVID-19 Pandemic. World J. Transplant. 2021, 11, 212–219. [Google Scholar] [CrossRef]
- Goldfarb Cyrino, L.; Galpern, J.; Moore, L.; Borgi, L.; Riella, L.V. A Narrative Review of Dietary Approaches for Kidney Transplant Patients. Kidney Int. Rep. 2021, 6, 1764–1774. [Google Scholar] [CrossRef] [PubMed]
- Fong, J.V.N.; Moore, L.W. Nutrition Trends in Kidney Transplant Recipients: The Importance of Dietary Monitoring and Need for Evidence-Based Recommendations. Front. Med. 2018, 5, 302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massy, Z.A.; Kolla, E.; Ferrières, J.; Bruckert, E.; Lambert, O.; Mansencal, N.; Laville, M.; Frimat, L.; Fouque, D.; Combe, C.; et al. Is a Treat-to-Target Approach to Lipid-Lowering Therapy Appropriate in Patients with Chronic Kidney Disease? A Prospective French Cohort Study. J. Nephrol. 2021, 34, 1467–1477. [Google Scholar] [CrossRef] [PubMed]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, 2889–2934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginsberg, H.N. REVIEW: Efficacy and Mechanisms of Action of Statins in the Treatment of Diabetic Dyslipidemia. J. Clin. Endocrinol. Metab. 2006, 91, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Chapman, M.J.; McTaggart, F. Optimizing the Pharmacology of Statins: Characteristics of Rosuvastatin. Atheroscler. Suppl. 2002, 2, 33–37. [Google Scholar] [CrossRef]
- Davignon, J. Beneficial Cardiovascular Pleiotropic Effects of Statins. Circulation 2004, 109, III-39–III-43. [Google Scholar] [CrossRef] [Green Version]
- Stroes, E.S.; Thompson, P.D.; Corsini, A.; Vladutiu, G.D.; Raal, F.J.; Ray, K.K.; Roden, M.; Stein, E.; Tokgözoʇlu, L.; Nordestgaard, B.G.; et al. Statin-Associated Muscle Symptoms: Impact on Statin Therapy-European Atherosclerosis Society Consensus Panel Statement on Assessment, Aetiology and Management. Eur. Heart J. 2015, 36, 1012–1022. [Google Scholar] [CrossRef]
- Palmer, S.C.; Navaneethan, S.D.; Craig, J.C.; Perkovic, V.; Johnson, D.W.; Nigwekar, S.U.; Hegbrant, J.; Strippoli, G.F.M. HMG CoA Reductase Inhibitors (Statins) for Kidney Transplant Recipients. Cochrane Database Syst. Rev. 2014, 2014, CD005019. [Google Scholar] [CrossRef]
- Holdaas, H.; Fellström, B.; Jardine, A.G.; Holme, I.; Nyberg, G.; Fauchald, P.; Grönhagen-Riska, C.; Madsen, S.; Neumayer, H.H.; Cole, E.; et al. Effect of Fluvastatin on Cardiac Outcomes in Renal Transplant Recipients: A Multicentre, Randomised, Placebo-Controlled Trial. Lancet 2003, 361, 2024–2031. [Google Scholar] [CrossRef]
- Woron, J. Interactions of Immunosuppressive Drugs: Why They Are so Important in Clinical Practice? Forum Nefrol. 2019, 12, 106–113. [Google Scholar]
- Oscanoa Espinoza, T.J.; Paredes-Pérez, N.; Lizaraso-Soto, F. Safety of Statins. Indian J. Endocrinol. Metab. 2013, 17, 636. [Google Scholar] [CrossRef]
- Scarfia, R.V.; Clementi, A.; Granata, A. Rhabdomyolysis and Acute Kidney Injury Secondary to Interaction between Simvastatin and Cyclosporine. Ren. Fail. 2013, 35, 1056–1057. [Google Scholar] [CrossRef] [Green Version]
- Monostory, K. Metabolic Drug Interactions with Immunosuppressants. In Organ Donation and Transplantation–Current Status and Future Challenges; IntechOpen: London, UK, 2018. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Wang, J.; Coutavas, E.; Shi, H.; Hao, Q.; Blobel, G. Structure of Human Niemann-Pick C1 Protein. Proc. Natl. Acad. Sci. USA 2016, 113, 8212–8217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohnle, M.; Pietruck, F.; Kribben, A.; Philipp, T.; Heemann, U.; Witzke, O. Ezetimibe for the Treatment of Uncontrolled Hypercholesterolemia in Patients with High-Dose Statin Therapy after Renal Transplantation. Am. J. Transplant. 2006, 6, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The Effects of Lowering LDL Cholesterol with Simvastatin plus Ezetimibe in Patients with Chronic Kidney Disease (Study of Heart and Renal Protection): A Randomised Placebo-Controlled Trial. Lancet 2011, 377, 2181. [Google Scholar] [CrossRef] [Green Version]
- Pontremoli, R.; Bellizzi, V.; Bianchi, S.; Bigazzi, R.; Cernaro, V.; del Vecchio, L.; de Nicola, L.; Leoncini, G.; Mallamaci, F.; Zoccali, C.; et al. Management of Dyslipidaemia in Patients with Chronic Kidney Disease: A Position Paper Endorsed by the Italian Society of Nephrology. J. Nephrol. 2020, 33, 417–430. [Google Scholar] [CrossRef] [Green Version]
- Kshirsagar, A.V.; Shoham, D.A.; Bang, H.; Hogan, S.L.; Simpson, R.J.; Colindres, R.E. The Effect of Cholesterol Reduction with Cholestyramine on Renal Function. Am. J. Kidney Dis. 2005, 46, 812–819. [Google Scholar] [CrossRef]
- Jakob, T.; Nordmann, A.J.; Schandelmaier, S.; Ferreira-González, I.; Briel, M. Fibrates for Primary Prevention of Cardiovascular Disease Events. Cochrane Database Syst. Rev. 2016, 11, CD009753. [Google Scholar] [CrossRef]
- Gallego-Colon, E.; Daum, A.; Yosefy, C. Statins and PCSK9 Inhibitors: A New Lipid-Lowering Therapy. Eur. J. Pharmacol. 2020, 878, 173114. [Google Scholar] [CrossRef]
- Eisenga, M.F.; Zelle, D.M.; Sloan, J.H.; Gaillard, C.A.J.M.; Bakker, S.J.L.; Dullaart, R.P.F. High Serum PCSK9 Is Associated with Increased Risk of New-Onset Diabetes after Transplantation in Renal Transplant Recipients. Diabetes Care 2017, 40, 894–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosmas, C.E.; Skavdis, A.; Sourlas, A.; Papakonstantinou, E.J.; Genao, E.P.; Uceta, R.E.; Guzman, E. Safety and Tolerability of PCSK9 Inhibitors: Current Insights. Clin. Pharmacol. 2020, 12, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Brégeault, M.F.; Dalby, A.J.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; et al. Effect of Alirocumab on Mortality after Acute Coronary Syndromes: An Analysis of the ODYSSEY OUTCOMES Randomized Clinical Trial. Circulation 2019, 140, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warden, B.A.; Kaufman, T.; Minnier, J.; Duell, P.B.; Fazio, S.; Shapiro, M.D. Use of PCSK9 Inhibitors in Solid Organ Transplantation Recipients. JACC Case Rep. 2020, 2, 396–399. [Google Scholar] [CrossRef]
- Fitzgerald, K.; White, S.; Borodovsky, A.; Bettencourt, B.R.; Strahs, A.; Clausen, V.; Wijngaard, P.; Horton, J.D.; Taubel, J.; Brooks, A.; et al. A Highly Durable RNAi Therapeutic Inhibitor of PCSK9. N. Engl. J. Med. 2017, 376, 41–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeed, A.; Ballantyne, C.M. Bempedoic Acid (ETC-1002): A Current Review. Cardiol. Clin. 2018, 36, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Bays, H.E.; Catapano, A.L.; Lalwani, N.D.; Bloedon, L.T.; Sterling, L.R.; Robinson, P.L.; Ballantyne, C.M. Safety and Efficacy of Bempedoic Acid to Reduce LDL Cholesterol. N. Engl. J. Med. 2019, 380, 1022–1032. [Google Scholar] [CrossRef]
Figure 1.
Post-transplant dyslipidemia management scheme for adult RTRs, suitable for patients who are 40–75 years, who are not on dialysis and do not receive cyclosporine. Scheme based on KDIGO [11], ACC/AHA [10], and ESC/EAS [9] guidelines. RTRs—renal transplant recipients; ASCVD—atherosclerotic cardiovascular disease; LDL-C-low-density lipoprotein cholesterol; * 10-year ASCVD risk calculator criteria: race, sex, age, TC concentration, HDL-C, sys-BP, hypertensive treatment, diabetes mellitus, smoking [59].
Figure 1.
Post-transplant dyslipidemia management scheme for adult RTRs, suitable for patients who are 40–75 years, who are not on dialysis and do not receive cyclosporine. Scheme based on KDIGO [11], ACC/AHA [10], and ESC/EAS [9] guidelines. RTRs—renal transplant recipients; ASCVD—atherosclerotic cardiovascular disease; LDL-C-low-density lipoprotein cholesterol; * 10-year ASCVD risk calculator criteria: race, sex, age, TC concentration, HDL-C, sys-BP, hypertensive treatment, diabetes mellitus, smoking [59].


{kind=link}
Table 1.
Dyslipidemia post-transplant risk factors.
| Modifiable | Non-Modifiable |
|---|---|
| Obesity | Age |
| Reduced physical activity | Gender |
| Hypothyroidism | Genetic predispositions |
| Diabetes | Chronic liver disease |
| Smoking | Renal insufficiency |
| Therapy for hypertension 1 | |
| Pretransplant lipid level | |
| Immunosuppressive agents |
1 beta-blockers, diuretics.
| Drug | TC | LDL-C | HDL-C | TG |
|---|---|---|---|---|
| Cyclosporine | ↑↑ | ↑↑ | ↓ | ↑↑ |
| Tacrolimus | ↑ | ↑ | ↓ | ↑ |
| Sirolimus | ↑↑ | ↑↑ | ↓ | ↑↑↑ |
| Prednisone | ↑ | ↑ | ↑ | ↑ |
| Mycophenolate mofetil | - | - | - | - |
| Azathioprine | - | - | - | - |
| Belatacept | ↓ | ↓ | ↑ | ↓ |
TC—total cholesterol; LDL-C—low-density lipoprotein cholesterol; HDL-C—high-density lipoprotein cholesterol; TG—triglycerides.
Table 3.
Recommended doses (mg/d) of statins in adult transplant recipients.
| Statin | Initial Dose | Target Dose * |
|---|---|---|
| Fluvastatin | 40 | 80 |
| Atorvastatin | 10 | 20 |
| Rosuvastatin | 5 | 10 |
| Pravastatin | 20 | 40 |
| Simvastatin | 20 | 40 |
* patients not receiving cyclosporine treatment.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chmielnicka, K.; Heleniak, Z.; Dębska-Ślizień, A. Dyslipidemia in Renal Transplant Recipients. Transplantology 2022, 3, 188-199. https://doi.org/10.3390/transplantology3020020
AMA Style
Chmielnicka K, Heleniak Z, Dębska-Ślizień A. Dyslipidemia in Renal Transplant Recipients. Transplantology. 2022; 3(2):188-199. https://doi.org/10.3390/transplantology3020020
Chicago/Turabian StyleChmielnicka, Karolina, Zbigniew Heleniak, and Alicja Dębska-Ślizień. 2022. "Dyslipidemia in Renal Transplant Recipients" Transplantology 3, no. 2: 188-199. https://doi.org/10.3390/transplantology3020020