
Infertility Treatment and Hypertension in Pregnancy: The Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
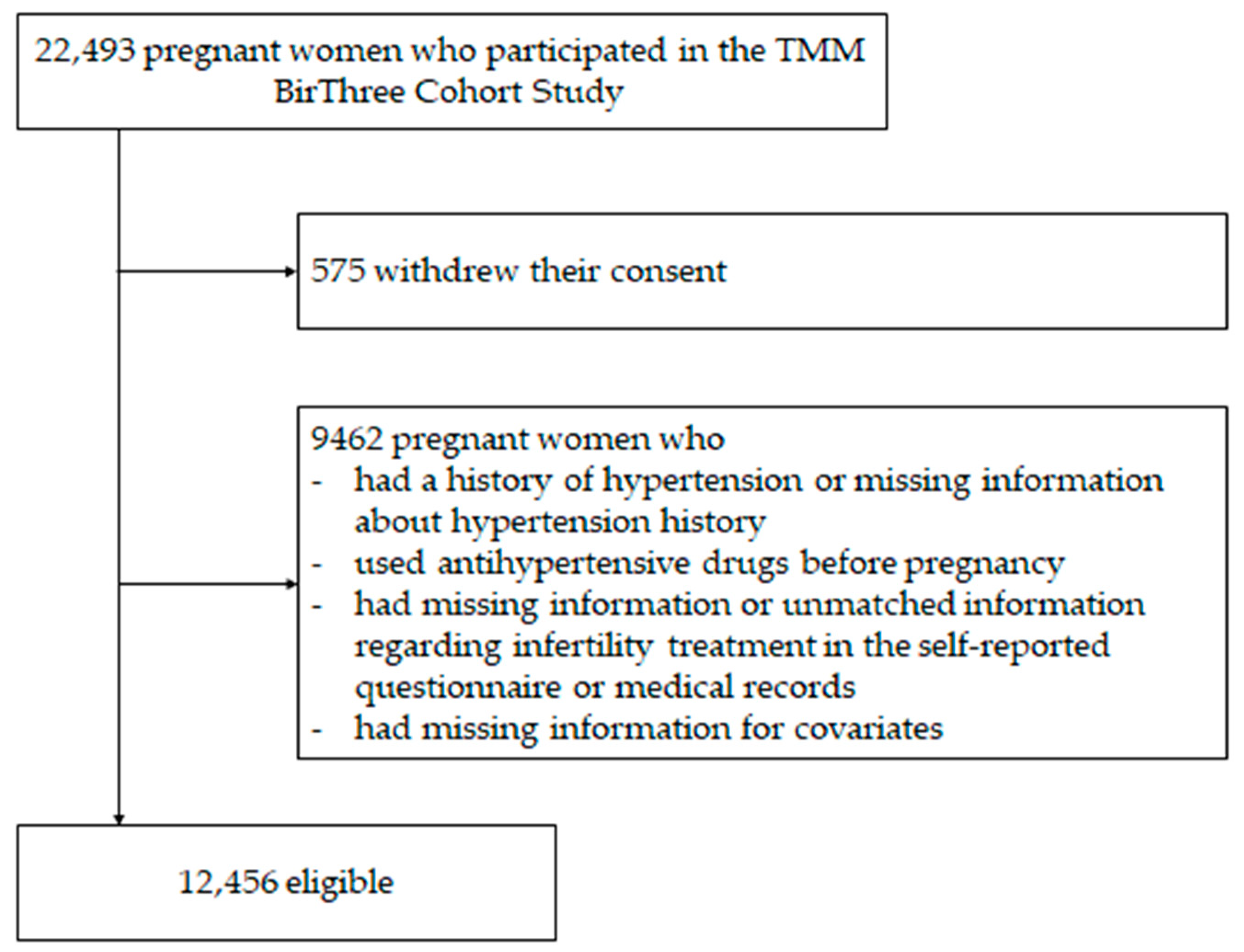
2.2. Participants
2.3. Measurements
2.4. Outcome
2.5. Statistical Analysis
3. Results
3.1. Maternal Characteristics
3.2. Infertility Treatment and HDP
3.3. Subgroup Analysis by Overweight and Smoking

{kind=link}
| Total (n = 12,456) | Single Pregnancy (n = 12,303) | Multiple Pregnancy (n = 153) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No Infertility Treatment | Underwent Infertility Treatment | p Value | No Infertility Treatment | Underwent Infertility Treatment | p Value | No Infertility Treatment | Underwent Infertility Treatment | p Value | ||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |||||
| Age at conception | <0.0001 | <0.0001 | <0.0001 | |||||||||||||
| <35 years | 8956 | 75.5 | 288 | 48.2 | 8861 | 75.5 | 272 | 48.0 | 95 | 77.9 | 16 | 51.6 | ||||
| ≥35 years | 2902 | 24.5 | 310 | 51.8 | 2875 | 24.5 | 295 | 52.0 | 27 | 22.1 | 15 | 48.4 | ||||
| Pre-pregnancy BMI | 0.06 | 0.1 | 0.08 | |||||||||||||
| <25 kg/m2 | 10,597 | 89.4 | 520 | 87.0 | 10,484 | 89.3 | 495 | 87.3 | 113 | 92.6 | 25 | 80.7 | ||||
| ≥25 kg/m2 | 1261 | 10.6 | 78 | 13.0 | 1252 | 10.7 | 72 | 12.7 | 9 | 7.4 | 6 | 19.4 | ||||
| Parity | <0.0001 | <0.0001 | 0.3 | |||||||||||||
| Nulliparous women | 5338 | 45.0 | 426 | 71.2 | 5277 | 45.0 | 406 | 71.6 | 61 | 50.0 | 20 | 64.5 | ||||
| Multiparous women with a history of HDP | 267 | 2.3 | 7 | 1.2 | 262 | 2.2 | 7 | 1.2 | 5 | 4.1 | 0 | 0 | ||||
| Multiparous women without a history of HDP | 6253 | 52.7 | 165 | 27.6 | 6197 | 52.8 | 154 | 27.2 | 56 | 45.9 | 11 | 35.5 | ||||
| Family history of hypertension | 0.007 | 0.002 | 0.2 | |||||||||||||
| No | 7837 | 66.1 | 363 | 60.7 | 7758 | 66.1 | 339 | 59.8 | 79 | 64.8 | 24 | 77.4 | ||||
| Yes | 4021 | 33.9 | 235 | 39.3 | 3978 | 33.9 | 228 | 40.2 | 43 | 35.3 | 7 | 22.6 | ||||
| Smoking | <0.0001 | <0.0001 | 0.02 | |||||||||||||
| Never/quit | 10,606 | 89.4 | 582 | 97.3 | 10,501 | 89.5 | 551 | 97.2 | 105 | 86.1 | 31 | 100 | ||||
| Continued in early pregnancy | 1252 | 10.6 | 16 | 2.7 | 1235 | 10.5 | 16 | 2.8 | 17 | 13.9 | 0 | 0 | ||||
| Number of HDP/Pregnant Women Who Underwent Infertility Treatment, HDP/Pregnant Women Who Did Not Undergo Infertility Treatment | Crude OR | 95% CI | Adjusted OR | 95% CI | |
|---|---|---|---|---|---|
| Total | 87/598, 1120/11,858 | 1.63 | 1.29–2.07 | 1.34 | 1.05–1.72 |
| Single pregnancy | 79/567, 1103/11736 | 1.56 | 1.22–2.00 | 1.32 | 1.02–1.70 |
| Multiple pregnancy | 8/31, 17/122 | 2.15 | 0.83–5.58 | 3.21 | 0.97–10.61 |
| Number of HDP/Pregnant Women Who Underwent IVF/ICSI, HDP/Pregnant Women Who Did Not Undergo Infertility Treatment | Crude OR | 95% CI | Adjusted OR | 95% CI | |
|---|---|---|---|---|---|
| Total | 50/307, 1120/11,858 | 1.87 | 1.37–2.54 | 1.65 | 1.20–2.29 |
| Single pregnancy | 47/298, 1103/11,736 | 1.81 | 1.31–2.48 | 1.61 | 1.16–2.25 |
| Multiple pregnancy | 3/9, 17/122 | 3.09 | 0.71–13.53 | 4.31 | 0.74–25.16 |
| Infertility treatment | |||
| Pre-pregnancy BMI | Adjusted OR | 95% CI | p value for interaction |
| <25 kg/m2 | 1.36 | 1.03–1.80 | 0.5 |
| ≥25 kg/m2 | 1.25 | 0.74–2.11 | |
| Smoking | Adjusted OR | 95% CI | p value for interaction |
| Never/quit | 1.36 | 1.06–1.75 | 0.7 |
| Continued in early pregnancy | 1.79 | 0.49–6.58 | |
| IVF/ICSI | |||
| Pre-pregnancy BMI | Adjusted OR | 95% CI | p value for interaction |
| <25 kg/m2 | 1.78 | 1.27–2.51 | 0.12 |
| ≥25 kg/m2 | 0.90 | 0.35–2.29 | |
| Smoking | Adjusted OR | 95% CI | p value for interaction |
| Never/quit | 1.72 | 1.24–2.38 | NA |
| Continued in early pregnancy | <0.001 | <0.001–>999.9 | |
3.4. Proportion of HDP in Fresh or Frozen Embryo Transfer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, W.; Xie, X.; Yuan, T.; Wang, Y.; Zhao, F.; Zhou, Z.; Zhang, H. Epidemiological trends of maternal hypertensive disorders of pregnancy at the global, regional, and national levels: A population-based study. BMC Pregnancy Childbirth 2021, 21, 364. [Google Scholar] [CrossRef]
- Hasegawa, J.; Sekizawa, A.; Tanaka, H.; Katsuragi, S.; Osato, K.; Murakoshi, T.; Nakata, M.; Nakamura, M.; Yoshimatsu, J.; Sadahiro, T.; et al. Current status of pregnancy-related maternal mortality in Japan: A report from the Maternal Death Exploratory Committee in Japan. BMJ. Open 2016, 6, e010304. [Google Scholar] [CrossRef] [PubMed]
- Giorgione, V.; Ridder, A.; Kalafat, E.; Khalil, A.; Thilaganathan, B. Incidence of postpartum hypertension within 2 years of a pregnancy complicated by pre-eclampsia: A systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2021, 128, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Monseur, B.C.; Morris, J.R.; Hipp, H.S.; Berghella, V. Hypertensive disorders of pregnancy and infertility treatment: A population-based survey among United States women. J. Assist Reprod Genet. 2019, 36, 1449–1456. [Google Scholar] [CrossRef]
- Thomopoulos, C.; Tsioufis, C.; Michalopoulou, H.; Makris, T.; Papademetriou, V.; Stefanadis, C. Assisted reproductive technology and pregnancy-related hypertensive complications: A systematic review. J. Hum Hypertens. 2013, 27, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Qin, J.; Liu, X.; Sheng, X.; Wang, H.; Gao, S. Assisted reproductive technology and the risk of pregnancy-related complications and adverse pregnancy outcomes in singleton pregnancies: A meta-analysis of cohort studies. Fertil Steril. 2016, 105, 73–85.e6. [Google Scholar] [CrossRef]
- Pinborg, A. Short- and long-term outcomes in children born after assisted reproductive technology. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, O.; Jwa, S.C.; Kuwahara, A.; Katagiri, Y.; Kuwabara, Y.; Hamatani, T.; Harada, M.; Osuga, Y. Assisted reproductive technology in Japan: A summary report for 2018 by the Ethics Committee of the Japan Society of Obstetrics and Gynecology. Reprod. Med. Biol. 2020, 20, 3–12. [Google Scholar] [CrossRef]
- Art Registry of Japan. Available online: https://plaza.umin.ac.jp/~jsog-art/ (accessed on 18 September 2021).
- Adamson, G.D.; de Mouzon, J.; Chambers, G.; Zegers-Hochschild, F.; Mansour, R.; Ishihara, O.; Banker, M.; Dyer, S.; Kupka, M. International Committee for Monitoring Assisted Reproductive Technology: World Report on Assisted Reproductive Technology. 2016. Available online: https://www.icmartivf.org/wp-content/uploads/ICMART-ESHRE-WR2016-FINAL-20200901.pdf (accessed on 17 March 2023).
- Chih, H.J.; Elias, F.T.S.; Gaudet, L.; Velez, M.P. Assisted reproductive technology and hypertensive disorders of pregnancy: Systematic review and meta-analyses. BMC Pregnancy Childbirth 2021, 21, 449. [Google Scholar] [CrossRef] [PubMed]
- Nagata, C.; Yang, L.; Yamamoto-Hanada, K.; Mezawa, H.; Ayabe, T.; Ishizuka, K.; Konishi, M.; Ohya, Y.; Saito, H.; Sago, H.; et al. Complications and adverse outcomes in pregnancy and childbirth among women who conceived by assisted reproductive technologies: A nationwide birth cohort study of Japan environment and children’s study. BMC Pregnancy Childbirth 2019, 19, 77. [Google Scholar] [CrossRef] [PubMed]
- Kuriyama, S.; Metoki, H.; Kikuya, M.; Obara, T.; Ishikuro, M.; Yamanaka, C.; Nagai, M.; Matsubara, H.; Kobayashi, T.; Sugawara, J.; et al. Cohort Profile: Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study (TMM BirThree Cohort Study): Rationale, progress and perspective. Int. J. Epidemiol. 2020, 49, 18–19m. [Google Scholar] [CrossRef]
- Kuriyama, S.; Yaegashi, N.; Nagami, F.; Arai, T.; Kawaguchi, Y.; Osumi, N.; Sakaida, M.; Suzuki, Y.; Nakayama, K.; Hashizume, H.; et al. The Tohoku Medical Megabank Project: Design and Mission. J. Epidemiol. 2016, 26, 493–511. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, J.; Ishikuro, M.; Obara, T.; Onuma, T.; Murakami, K.; Kikuya, M.; Ueno, F.; Noda, A.; Mizuno, S.; Kobayashi, T.; et al. Maternal Baseline Characteristics and Perinatal Outcomes: The Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study. J. Epidemiol. 2022, 32, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Ishikuro, M.; Obara, T.; Osanai, T.; Yamanaka, C.; Sato, Y.; Mizuno, S.; Miyashita, M.; Kikuya, M.; Sakurai, K.; Hozawa, A.; et al. Strategic Methods for Recruiting Grandparents: The Tohoku Medical Megabank Birth and Three-Generation Cohort Study. Tohoku J. Exp. Med. 2018, 246, 97–105. [Google Scholar] [CrossRef]
- Usuzaki, T.; Ishikuro, M.; Metoki, H.; Murakami, K.; Noda, A.; Ueno, F.; Kikuya, M.; Obara, T.; Kuriyama, S. Comparison among research, home, and office blood pressure measurements for pregnant women: The TMM BirThree Cohort Study. J. Clin. Hypertens. 2020, 22, 2004–2013. [Google Scholar] [CrossRef]
- Aizawa, M.; Murakami, K.; Takahashi, I.; Onuma, T.; Noda, A.; Ueno, F.; Matsuzaki, F.; Ishikuro, M.; Obara, T.; Hamada, H.; et al. Skipping breakfast during pregnancy and hypertensive disorders of pregnancy in Japanese women: The Tohoku medical megabank project birth and three-generation cohort study. Nutr. J. 2022, 21, 71. [Google Scholar] [CrossRef]
- Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet. Gynecol. 2013, 122, 1122–1131. [Google Scholar]
- Ishikuro, M.; Murakami, K.; Yokozeki, F.; Onuma, T.; Noda, A.; Ueno, F.; Obara, T.; Kuriyama, S. Hypertension in pregnancy as a possible factor for child autistic behavior at two years old. Pregnancy Hypertens. 2021, 25, 88–90. [Google Scholar] [CrossRef]
- Ishikuro, M.; Obara, T.; Murakami, K.; Ueno, F.; Noda, A.; Kikuya, M.; Sugawara, J.; Metoki, H.; Kuriyama, S. Relation between disaster exposure, maternal characteristics, and obstetric outcomes: The Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study. J. Epidemiol. 2021, 33, 127–135. [Google Scholar] [CrossRef]
- Umesawa, M.; Kobashi, G. Epidemiology of hypertensive disorders in pregnancy: Prevalence, risk factors, predictors and prognosis. Hypertens Res. 2017, 40, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Morisaki, N.; Obara, T.; Piedvache, A.; Kobayashi, S.; Miyashita, C.; Nishimura, T.; Ishikuro, M.; Sata, F.; Horikawa, R.; Mori, C.; et al. Association between smoking and hypertension in pregnancy among Japanese women: A meta-analysis of birth cohort studies in the Japan Birth Cohort Consortium (JBiCC) and JECS. J. Epidemiol. 2022; epub ahead of print. [Google Scholar] [CrossRef]
- Dayan, N.; Fell, D.B.; Guo, Y.; Wang, H.; Velez, M.P.; Spitzer, K.; Laskin, C.A. Severe maternal morbidity in women with high BMI in IVF and unassisted singleton pregnancies. Hum. Reprod. 2018, 33, 1548–1556. [Google Scholar] [CrossRef]
- Wang, Y.A.; Chughtai, A.A.; Farquhar, C.M.; Pollock, W.; Lui, K.; Sullivan, E.A. Increased incidence of gestational hypertension and preeclampsia after assisted reproductive technology treatment. Fertil. Steril. 2016, 105, 920–926.e2. [Google Scholar] [CrossRef]
- Dobrosavljevic, A.; Rakic, S. Risk of gestational hypertension in pregnancies complicated with ovarian hyperstimulation syndrome. J. Pak. Med. Assoc. 2020, 70, 1897–1900. [Google Scholar]
- Luke, B. Pregnancy and birth outcomes in couples with infertility with and without assisted reproductive technology: With an emphasis on US population-based studies. Am. J. Obstet. Gynecol. 2017, 217, 270–281. [Google Scholar] [CrossRef] [PubMed]
- Ombelet, W. The revival of intrauterine insemination: Evidence-based data have changed the picture. Facts. Views Vis. Obgyn. 2017, 9, 131–132. [Google Scholar]
- Opdahl, S.; Henningsen, A.A.; Tiitinen, A.; Bergh, C.; Pinborg, A.; Romundstad, P.R.; Wennerholm, U.B.; Gissler, M.; Skjærven, R.; Romundstad, L.B. Risk of hypertensive disorders in pregnancies following assisted reproductive technology: A cohort study from the CoNARTaS group. Hum. Reprod. 2015, 30, 1724–1731. [Google Scholar] [CrossRef] [PubMed]
- Luke, B.; Brown, M.B.; Eisenberg, M.L.; Callan, C.; Botting, B.J.; Pacey, A.; Sutcliffe, A.G.; Baker, V.L. In vitro fertilization and risk for hypertensive disorders of pregnancy: Associations with treatment parameters. Am. J. Obstet. Gynecol. 2020, 222, 350.e1–350.e13. [Google Scholar] [CrossRef]
- von Versen-Höynck, F.; Schaub, A.M.; Chi, Y.Y.; Chiu, K.H.; Liu, J.; Lingis, M.; Stan Williams, R.; Rhoton-Vlasak, A.; Nichols, W.W.; Fleischmann, R.R.; et al. Increased Preeclampsia Risk and Reduced Aortic Compliance With In Vitro Fertilization Cycles in the Absence of a Corpus Luteum. Hypertension 2019, 73, 640–649. [Google Scholar] [CrossRef]
- Sites, C.K.; Bachilova, S.; Gopal, D.; Cabral, H.J.; Coddington, C.C.; Stern, J.E. Embryo biopsy and maternal and neonatal outcomes following cryopreserved-thawed single embryo transfer. Am. J. Obstet. Gynecol. 2021, 225, 285.e1–285.e7. [Google Scholar] [CrossRef]
- Bortoletto, P.; Cagino, K.; McCarter, K.; Forlenza, K.; Yau, A.; Prabhu, M.; Melnick, A.P. Association of transfer of frozen embryos in the programmed cycle with hypertensive disorders of pregnancy. Am. J. Obstet. Gynecol. 2022, 226, 861–862. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wang, H.; Zhang, Y.; Niu, J.; Li, Z.; Tang, R. Effect of pregravid obesity on perinatal outcomes in singleton pregnancies following in vitro fertilization and the weight-loss goals to reduce the risks of poor pregnancy outcomes: A retrospective cohort study. PLoS ONE 2020, 15, e0227766. [Google Scholar] [CrossRef]
- Chang, J.J.; Strauss, J.F., 3rd; Deshazo, J.P.; Rigby, F.B.; Chelmow, D.P.; Macones, G.A. Reassessing the impact of smoking on preeclampsia/eclampsia: Are there age and racial differences? PLoS ONE 2014, 9, e106446. [Google Scholar] [CrossRef]
- Tanaka, K.; Nishigori, H.; Watanabe, Z.; Tanoue, K.; Iwama, N.; Satoh, M.; Murakami, T.; Hoshiai, T.; Saito, M.; Mizuno, S.; et al. Secondhand smoke exposure is associated with the risk of hypertensive disorders of pregnancy: The Japan Environment and Children’s Study. Hypertens. Res. 2023, 46, 834–844. [Google Scholar] [CrossRef]
- Petersen, S.H.; Bergh, C.; Gisr, M.; Åsvold, B.O.; Romundstad, L.B.; Tiitinen, A.; Spangmose, A.L.; Pinborg, A.; Wennerholm, U.B.; Henningsen, A.A.; et al. Time trends in placenta-mediated pregnancy complications after assisted reproductive technology in the Nordic countries. Am. J. Obstet. Gynecol. 2020, 223, 226.e1–226.e19. [Google Scholar] [CrossRef]
- Wagata, M.; Kogure, M.; Nakaya, N.; Tsuchiya, N.; Nakamura, T.; Hirata, T.; Narita, A.; Metoki, H.; Ishikuro, M.; Kikuya, M.; et al. Hypertensive disorders of pregnancy, obesity, and hypertension in later life by age group: A cross-sectional analysis. Hypertens. Res. 2020, 43, 1277–1283. [Google Scholar] [CrossRef]
- Stern, J.E.; Liu, C.L.; Hwang, S.S.; Dukhovny, D.; Farland, L.V.; Diop, H.; Coddington, C.C.; Cabral, H. Influence of Placental Abnormalities and Pregnancy-Induced Hypertension in Prematurity Associated with Various Assisted Reproductive Technology Techniques. J. Clin. Med. 2021, 10, 1681. [Google Scholar] [CrossRef]
- Li, F.; Wang, T.; Chen, L.; Zhang, S.; Chen, L.; Qin, J. Adverse pregnancy outcomes among mothers with hypertensive disorders in pregnancy: A meta-analysis of cohort studies. Pregnancy Hypertens. 2021, 24, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Gao, R.; Liu, Y.; Zhao, K.; Su, X.; Wong, H.C.; Li, L.; Xie, B.; Huang, Y.; Qiu, C.; et al. Hypertensive disorders of pregnancy and neonatal outcomes in twin vs. singleton pregnancies after assisted reproductive technology. Front. Pediatr. 2022, 10, 839882. [Google Scholar] [CrossRef] [PubMed]
- Iwama, N.; Oba, M.S.; Satoh, M.; Ohkubo, T.; Ishikuro, M.; Obara, T.; Sasaki, S.; Saito, M.; Murakami, Y.; Kuriyama, S.I.; et al. Association of maternal home blood pressure trajectory during pregnancy with infant birth weight: The BOSHI study. Hypertens. Res. 2020, 43, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S.; et al. Hypertensive Disorders of Pregnancy: ISSHP Classification, Diagnosis, and Management Recommendations for International Practice. Hypertension 2018, 72, 24–43. [Google Scholar] [CrossRef] [PubMed]
- Regitz-Zagrosek, V.; Roos-Hesselink, J.W.; Bauersachs, J.; Blomström-Lundqvist, C.; Cífková, R.; De Bonis, M.; Iung, B.; Johnson, M.R.; Kintscher, U.; Kranke, P.; et al. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy. Eur. Heart J. 2018, 39, 3165–3241. [Google Scholar] [CrossRef] [PubMed]
- Arvizu, M.; Minguez-Alarcon, L.; Stuart, J.J.; Mitsunami, M.; Rosner, B.; Rich-Edwards, J.W.; Chavarro, J.E. Physical activity before pregnancy and the risk of hypertensive disorders of pregnancy. Am. J. Obstet. Gynecol. MFM 2022, 4, 100556. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishikuro, M.; Obara, T.; Murakami, K.; Ueno, F.; Noda, A.; Onuma, T.; Matsuzaki, F.; Kikuya, M.; Watanabe, Z.; Shiga, N.; et al. Infertility Treatment and Hypertension in Pregnancy: The Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study. Reprod. Med. 2023, 4, 89-99. https://doi.org/10.3390/reprodmed4020010
Ishikuro M, Obara T, Murakami K, Ueno F, Noda A, Onuma T, Matsuzaki F, Kikuya M, Watanabe Z, Shiga N, et al. Infertility Treatment and Hypertension in Pregnancy: The Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study. Reproductive Medicine. 2023; 4(2):89-99. https://doi.org/10.3390/reprodmed4020010
Chicago/Turabian StyleIshikuro, Mami, Taku Obara, Keiko Murakami, Fumihiko Ueno, Aoi Noda, Tomomi Onuma, Fumiko Matsuzaki, Masahiro Kikuya, Zen Watanabe, Naomi Shiga, and et al. 2023. "Infertility Treatment and Hypertension in Pregnancy: The Tohoku Medical Megabank Project Birth and Three-Generation Cohort Study" Reproductive Medicine 4, no. 2: 89-99. https://doi.org/10.3390/reprodmed4020010