
Obstructive Sleep Apnea and Risk of Miscarriage
by
 , , and
, , and
Jeannette M. Larson
1, 
Mihaela H. Bazalakova
2,
Amy Godecker
1,
Laura Cooney
1,
Melanie DelBeccaro
3,4,
Kjersti M. Aagaard
4 and
Kathleen M. Antony
1,4,*
1
Department of Obstetrics and Gynecology, University of Wisconsin School of Medicine and Public Health, 1010 Mound Street, Madison, WI 53715, USA
2
Wisconsin Sleep, UW Health Department of Neurology, University of Wisconsin School of Medicine and Public Health, 600 Highland Avenue, Madison, WI 53792, USA
3
Midwest Center for Women’s Healthcare, 350 South NW Highway, Suite 112, Park Ridge, IL 60068, USA
4
Baylor College of Medicine and Texas Children’s Hospital, Division of Maternal-Fetal Medicine, One Baylor Plaza, Houston, TX 77030, USA
*
Author to whom correspondence should be addressed.
Reprod. Med. 2023, 4(1), 1-12; https://doi.org/10.3390/reprodmed4010001
Submission received: 28 November 2022
/
Revised: 19 December 2022
/
Accepted: 30 December 2022
/
Published: 9 January 2023
Abstract
:The purpose of this project was to evaluate whether screening positive on obstructive sleep apnea questionnaires in the first trimester of pregnancy was associated with miscarriage. This was a secondary analysis of a prospective observational cohort study of participants who were screened for sleep apnea during pregnancy with the Epworth Sleepiness Scale, Berlin Questionnaire, and novel items related to sleep and napping. This secondary analysis was IRB exempt. Our primary outcome was miscarriage in the index pregnancy. An association between responses to the sleep apnea screening questions with miscarriage of the index pregnancy was queried via Poisson regression. We found that gravidae who had elevated scores on both the Epworth Sleepiness Scale and the Berlin Questionnaire were more likely to experience miscarriage than those who had elevated scores on only one questionnaire or neither (p = 0.018). Gravidae who reported snoring (p = 0.042) or hypertension (p = 0.013) in the first trimester were more likely to experience miscarriage than gravidae who did not. Gravidae who reported napping in the first trimester were less likely to experience miscarriage (p = 0.045), even after adjusting for confounding variables (p = 0.007). In conclusion, we found that screening positive on both the Berlin Questionnaire and Epworth Sleepiness Scale was statistically significantly associated with miscarriage prior to adjustment for confounding variables, as did snoring and hypertension. After adjusting for confounding variables, only not napping was associated with miscarriage. Given the small sample size, further investigation into this topic is warranted.
1. Introduction
Miscarriage is a common, and yet potentially personally devastating pregnancy outcome that occurs in 11% to 22% of recognized pregnancies [1]. The etiology of miscarriages is complex and often multifactorial with the most common identifiable cause linked to chromosomal aneuploidies and cytogenetic rearrangements. Recent hypotheses have also associated miscarriage with immunological and vascular phenomena, although causality remains poorly ascribed [2,3,4]. Miscarriage carries an appreciable cost to pregnant people and their families, healthcare systems, and society, resulting from both direct healthcare costs and indirect costs such as short-term loss of work and societal productivity [5]. Miscarriage is also associated with a risk for psychological morbidity, such as anxiety, depression, post-traumatic stress disorder, and suicide [5].
Obstructive sleep apnea is associated with increased body-mass index (BMI) and older age, both of which are risk factors for miscarriage. Obstructive sleep apnea itself has also been recognized as a potential risk factor for miscarriage itself due to sleep fragmentation and intermittent hypoxia [6]. The prevalence of obstructive sleep apnea within the reproductive age population has been estimated at 9% for women and between 3.6 and 32% during pregnancy [7,8,9,10]. Obstructive sleep apnea can result in upregulation of sympathetic nervous system activity, renin-angiotensin, aldosterone system activity, endothelial dysfunction, inflammation, oxidative stress, and metabolic dysregulation, which can result in serious morbidity, including hypertension and cardiovascular diseases in the general population [11,12]. Obstructive sleep apnea has also been associated with adverse outcomes, including hypertensive disorders of pregnancy, in the obstetric population [13,14]. Given the known effects of obstructive sleep apnea on vasculature and recent hypotheses associating miscarriage with immunologic and vascular phenomena, it is plausible that obstructive sleep apnea could be a potentially reversible or treatable cause of miscarriage.
We sought to examine the relationship between elevated scores on questionnaires used to screen for obstructive sleep apnea and excessive sleepiness, and miscarriage. Our hypothesis was that elevated Epworth Sleepiness Scale and Berlin Questionnaire scores, suggestive of higher pretest probability for obstructive sleep apnea, would be independently associated with miscarriage. We adjusted our analyses for age, smoking status, and history of miscarriage, given the known associations between these factors and risk of miscarriage.
2. Materials and Methods
The data for the parent prospective observational cohort study enabling the current analyses were collected from the Harris County Hospital District (now Harris Health System) between May 2010 and September 2012. The parent study was approved by the Institutional Review Board at Baylor College of Medicine (IRB H-19183, initial approval date 4 April 2006) and was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) [15,16]. Informed consent was obtained from all participants at the time of the parent study. This current secondary analysis was determined to be exempt from approval by the Minimal Risk Health Sciences Institutional Review Board at the University of Wisconsin–Madison. All unique identifiers were removed from the dataset prior to use in this current study.
In the parent study, gravidae presenting to two community clinics and one tertiary clinic were approached for enrollment, and gravidae who screened positive for sleep apnea in the parent study were referred for diagnostic sleep testing [15,16]. Gravidae of all gestational ages were recruited for the parent study which evaluated the association between screening measures of obstructive sleep apnea and adverse perinatal outcomes. Exclusion criteria were known sleep-disordered breathing, multifetal gestation, fatal fetal anomalies (if known), underlying pulmonary or cardiac conditions, and age < 18 or >50. For the current study, only gravidae completing the questionnaire in the first trimester were included for analysis.
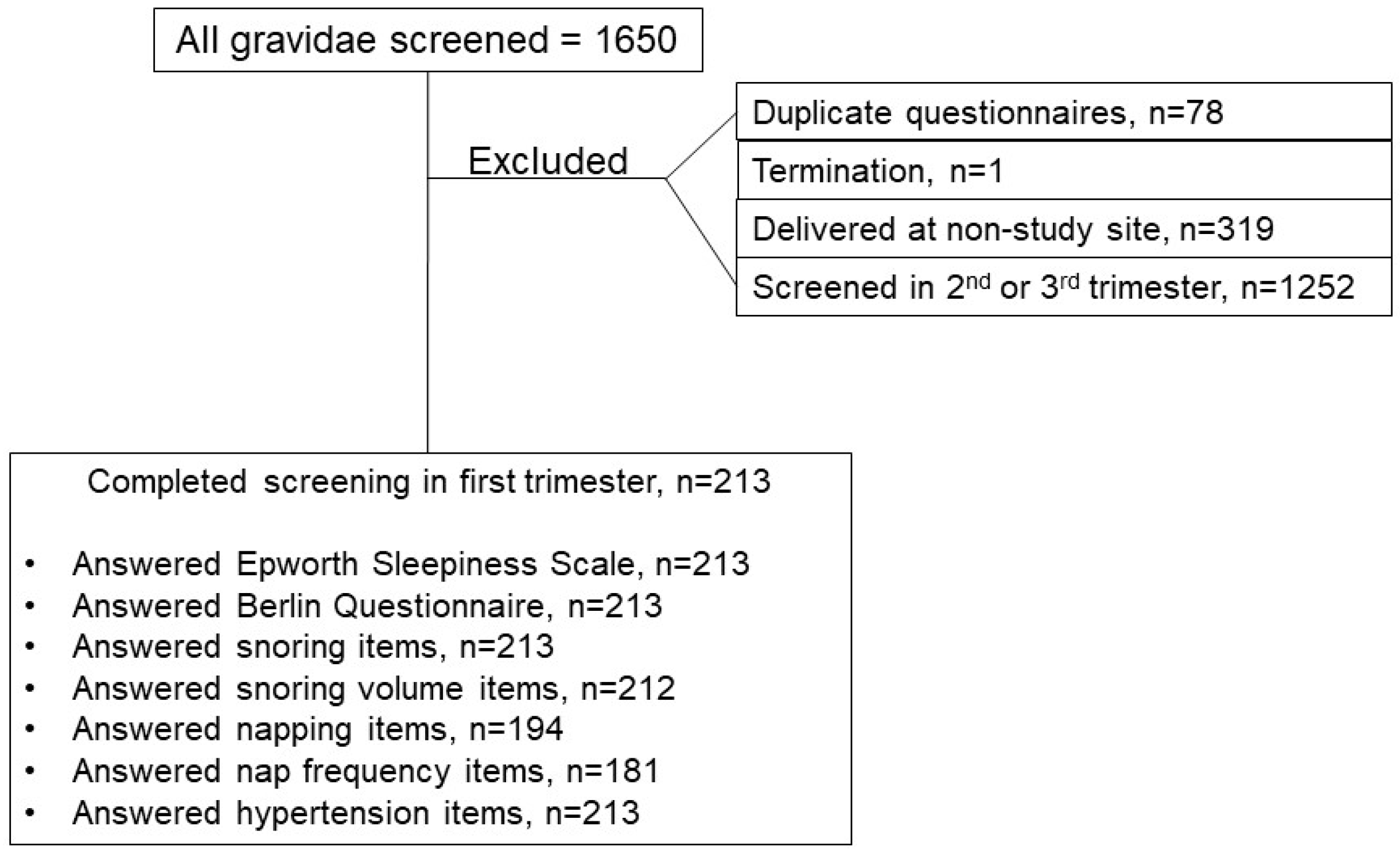
Consenting participants were administered a questionnaire (in English or Spanish), which comprised the Berlin Questionnaire (BQ) and the Epworth Sleepiness Scale (ESS), in addition to other sleep-related questions. The BQ is a 10-item questionnaire used to assess risk of obstructive sleep apnea (OSA) [17]. A higher score indicates higher risk of OSA. In studies performed in non-pregnant male populations, it has a high positive predictive value for OSA (0.866), but it performs less well in pregnancy [15,18,19]. The ESS is an 8-item questionnaire used to assess daytime sleepiness [20]. A higher score indicates a higher-than-average sleep propensity, and its intended use is to assess sleepiness rather than sleep apnea. While it has a low sensitivity and specificity as a screening tool for sleep apnea, it has been used both clinically and in research in the non-pregnant and pregnant population [21,22,23]. While it should not be used alone to screen for sleep apnea, it may be used to assess sleepiness in tandem with other tools [24]. A separate study was performed to evaluate the association between other adverse perinatal outcomes and these screening measures of obstructive sleep apnea [16]. Individual items related to snoring, snoring volumes, and hypertension reported here were taken from questions on the BQ. Additional question items related to napping and napping frequency were added to the ESS and BQ for this study. Gravidae who screened positive for sleep apnea were referred for diagnostic polysomnography; very few diagnostic tests were completed, therefore for this analysis only the screening data were used [15,16]. If participants completed a questionnaire more than once, duplicate questionnaires were excluded. Questionnaires with incomplete items were excluded from each respective analysis. Participants who subsequently terminated their pregnancy, who were screened in the second or third trimester, or who delivered or transferred care to a non-study site (who had no outcomes available for analysis) were excluded (Figure 1). The remaining 213 pregnant people screened in the first trimester were included in this analysis.
Each participant’s medical chart was reviewed (MD & KMA7). Miscarriage was defined as a spontaneous abortion at or before 19 6/7 weeks of gestation [2]. Covariates considered in these analyses were age, gravidity, ethnicity, smoking status and history of prior miscarriage. Prior history of miscarriage was defined by participant report of prior miscarriage and review of the medical record. Prepregnancy BMI data was collected where available, but not included in adjusted relative risk calculations due to the low percentage of participants with prepregnancy BMI data available.
Descriptive findings of study sample characteristics and outcomes by responses to questionnaire items are reported. Chi-square tests for independence were performed for categorical variables. Generalized linear models’ adjusted relative risks (aRRs) with 95% confidence intervals (CIs) were estimated for age categories, gravidity categories, and ethnicity for associations between questionnaire items and miscarriage or history of miscarriage using a modified Poisson regression approach [25]. When no association was present, aRRs were calculated with all covariates. Analysis stratified by advanced age was also completed. Stata (Stata 15.1, 2017, College Station, TX, USA) was used for analyses. Data related to this article will be shared upon reasonable request to the corresponding author.
3. Results
One thousand, six hundred fifty questionnaires were completed. Of those, two hundred thirteen were from participants who were screened in the first trimester and were included in this analysis. The majority of participants were Hispanic/Latinx (89.7%). One hundred seventy-nine participants had BMI data available for analysis. Over half of participants were overweight (32.4%) or had obesity (31.3%). Most participants were over 25 years of age (73.2%). Few participants reported smoking (2.8%). About one third of participants reported history of miscarriage (36.2%) (Table 1). Napping was most prevalent in the 20–24-year-old age group (65.9%) and least prevalent in the 25–29-year-old age group (34.5%). Snoring and hypertension were not significantly associated with age.
In this population, 30.0% (N = 64) of gravidae screened positive on either the ESS or BQ. (Table 2A). Of those, 14.6% (N = 31) of gravidae screened positive on the BQ and 18.8% (N = 40) of gravidae screened positive on the ESS. Only 3.3% (N = 7) screened positive on both the ESS and the BQ (Table 2A). Almost half (N = 88) of gravidae reported napping, greater than half of whom reported napping three or more times weekly (N = 52) (Table 2B). One out of five (21.1%, N = 45) of gravidae reported snoring and 8.9% (N = 19) of gravidae reported hypertension.
The percentage of gravidae who miscarried by screening tool or item is shown in Table 3. Unadjusted analyses indicate that screening positive on both Epworth and Berlin (p = 0.018), snoring (p = 0.042) and hypertension (p = 0.013) were associated with increased miscarriage. Napping more than 3 times per week was associated with decreased miscarriage (p = 0.045). There was no association between napping and higher Epworth scores (p = 0.173). Results of stratified analysis for advanced maternal age (age ≥ 35) were similar to results of the overall analysis (results available upon request). Table 3 also shows relative risk for miscarriage by screening tool or item adjusted for confounding variables including age, ethnicity, gravidity, prior miscarriage history, and smoking status. Screening positive on both questionnaires, snoring, and hypertension were not associated with miscarriage after adjustment for confounding variables. Napping was not significantly associated with decreased miscarriage after adjustment for age alone (p = 0.066). After adjusting for age, ethnicity, gravidity, prior miscarriage history and smoking, napping was associated with decreased miscarriage with gravidae who napped one-third less likely to miscarry as gravidae who did not (p = 0.007) (Table 3).
4. Discussion
Elevated scores on screening questionnaires for both obstructive sleep apnea and excessive sleepiness in the first trimester of pregnancy were significantly associated with miscarriage in our study before adjustment for confounding variables. This finding aligns with the findings of recent publications and emerging hypotheses about the association between miscarriage and sleep disordered breathing [6,26], and suggest the “sleepy” apnea phenotype may be particularly relevant to likelihood of pregnancy loss [27]. One recent retrospective study found a significant association between apnea-hypopnea index and miscarriage, and between BMI and miscarriage [6]. It has been hypothesized that sleep disordered breathing may act as a mediating factor in the relationship between weight and miscarriage [26]. Gravidae with obstructive sleep apnea can experience intermittent hypoxemia, leading to increased oxidative stress [28]. This increase in oxidative stress can contribute to endothelial dysfunction and increased pro-inflammatory cytokines, which has been linked to adverse pregnancy outcomes, including miscarriage [29,30,31]. Furthermore, sleep disordered breathing has been demonstrated in multiple studies to be associated with placental abnormalities consistent with chronic hypoxia and underperfusion [32,33]. Recent in vitro studies have demonstrated that intermittent hypoxia inhibits trophoblast motility and proliferation and induces apoptosis via the endoplasmic reticulum stress signaling pathway [34].
However, our results did not support an association between elevated scores on screening questionnaires and miscarriage after adjusting for confounders. The lack of association between miscarriage and screening positive on the BQ or ESS individually here could mean that they are inadequate screening tools during pregnancy. Given these plausible hypotheses for how sleep disordered breathing may be associated with miscarriage, it is important to delineate how to best screen gravidae for sleep disordered breathing. In recent meta-analyses, the prevalence of sleep disordered breathing in pregnancy has been estimated to be between 4% to 32% [9]. However, the commonly used Berlin Questionnaire and Epworth Sleepiness Scale have been shown to perform poorly in the general obstetric population [14,15]. The lack of association between miscarriage and elevated scores on the BQ or ESS individually here could be due to their poor performance in this population as a screening tool for either obstructive sleep apnea or excessive sleepiness alone, but raise the interesting hypothesis that symptomatic gravidae at risk of sleep apnea who also have hypersomnolence are the specific population that should be prioritized for objective sleep apnea testing. Recent review articles have suggested using snoring and chronic hypertension as risk factors prompting testing of gravidae for obstructive sleep apnea [13,35]. These risk factors are consistent with our findings on individual item analysis. However, a standardized and validated questionnaire for the obstetric population could be an asset in detecting sleep disordered breathing in the clinical setting; one such questionnaire, published after the enrollment period of this prospective study, has been validated in pregnancy and is used clinically in some settings [19,36,37].
Any napping and napping three or more times weekly were associated with lower rates of miscarriage. The association of napping at all did persist after adjusting for all other potentially confounding variables. These findings could be explained by the small sample size screened in the first trimester or by the frequency of multifactorial fatigue in pregnancy, which may make these questions a poor indicator of objective hypersomnolence or sleep disturbance in pregnancy. It may also be that napping counteracts some effects of hypersomnolence.
Strengths of our study include a sample of participants with known histories and outcomes which were manually entered into the database by obstetric physicians (KMA7 and MD). The prospective nature of the study also ensured that responses to subjective questions, such as fatigue and napping, were accurate as minimal recall was required to answer questions.
The most significant limitation of this study was the small proportion of gravidae who completed the questionnaire in the first trimester. This may have particularly limited our ability to adjust for confounding variables. Prepregnancy BMI data was also missing for a substantial number of those included, thus we were not able to adjust for this potentially important factor. This is a limitation noted in recent meta-analyses of sleep disordered breathing in pregnancy [14]. Here, BMI data was missing for more gravidae with miscarriage than those with ongoing pregnancy. While referral for positive screens occurred within a few days of questionnaire completion, data entry was delayed. Confirming the pregravid weight required in-depth review of scanned paper records, and this step was unfortunately not always performed in pregnancies that had already miscarried because these pregnancies were not included in the primary analysis [16]. Additionally, because this questionnaire was completed at a prenatal visit, gravidae who miscarried prior to the first prenatal visit were not included in our sample. Gravidae with prior history of miscarriage may also be more likely to seek earlier pregnancy care and thus complete the questionnaire than gravidae with no history of miscarriage; however, the overall miscarriage rate in the study population (13.9%) is within the range of estimated rates in the general population (10–26%) [38,39,40]. In future studies, recruiting gravidae earlier in pregnancy or screening or testing prior to pregnancy could provide further evidence to elucidate the association between sleep disordered breathing and miscarriage. The lack of objective diagnostic data is a limitation of this study. Though gravidae were referred for polysomnography, few were able to undergo further testing, which is reflective of resource limitations at the study site [15,16]. Treatment of sleep disordered breathing and its effect on miscarriage was not evaluated in this analysis. This population was majority Hispanic/Latinx, which is an understudied population, so this contribution is needed. However, this also limits the generalizability of our findings. Future research evaluating treatment of objectively diagnosed sleep disordered breathing, especially associated with symptomatic excessive sleepiness in the obstetric population could address this limitation.
5. Conclusions
As noted in recent publications on sleep disordered breathing in pregnancy, data on obstructive sleep apnea in early pregnancy, and specifically miscarriage, are limited [6,14]. This study contributes to the available evidence on this topic. In the context of prior hypotheses and available evidence, our study suggests a possible association between obstructive sleep apnea, excessive sleepiness phenotype, and miscarriage. Although it is not known whether treatment would alter pregnancy outcomes, it is reasonable to consider screening gravidae for sleep disordered breathing at the initiation of prenatal care or at preconception consultations. Further studies are needed to clarify this association with larger sample sizes and more available data on confounding variables such as BMI, as well as to evaluate potential screening tools and feasible diagnostic and treatment modalities.
Author Contributions
Conceptualization, K.M.A. (Kathleen M. Antony) and J.M.L.; methodology, K.M.A. (Kathleen M. Antony), A.G. and J.M.L.; software, K.M.A. (Kathleen M. Antony), A.G. and J.M.L.; validation, K.M.A. (Kathleen M. Antony), K.M.A. (Kjersti M. Aagaard) and M.D.; formal analysis, A.G. and J.M.L.; investigation, K.M.A. (Kathleen M. Antony), M.H.B. and L.C.; resources, K.M.A. (Kathleen M. Antony), K.M.A. (Kjersti M. Aagaard) and M.H.B.; data curation, M.D. and K.M.A. (Kathleen M. Antony); writing—original draft preparation, J.M.L. and K.M.A. (Kathleen M. Antony); writing—review and editing, J.M.L., M.H.B., A.G., L.C., M.D., K.M.A. (Kathleen M. Antony) and K.M.A. (Kjersti M. Aagaard); visualization, A.G., J.M.L. and K.M.A. (Kathleen M. Antony); supervision, K.M.A. (Kathleen M. Antony); project administration, K.M.A. (Kathleen M. Antony) and M.D.; funding acquisition, K.M.A. (Kathleen M. Antony), K.M.A. (Kjersti M. Aagaard) and J.M.L. All authors have read and agreed to the published version of the manuscript.
Funding
This project was supported by a summer research award from the Herman and Gwendolyn Shapiro Foundation and University of Wisconsin School of Medicine and Public Health Dean’s Office Funds (J.M.L.). This project was further supported by the University of Wisconsin Department of Obstetrics & Gynecology and Department of Neurology (K.M.A. (Kathleen M. Antony) and M.H.B., respectively). The parent study was funded by residency research funds generously provided by Baylor College of Medicine (K.M.A. (Kathleen M. Antony)).
Institutional Review Board Statement
The parent study was approved by the Institutional Review Board at Baylor College of Medicine (IRB H-19183) and was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). Informed consent was obtained from all participants at the time of the parent study. This current secondary analysis was determined to be exempt from approval by the Minimal Risk Health Sciences Institutional Review Board at the University of Wisconsin–Madison.
Informed Consent Statement
Informed consent was obtained from all participants at the time of the parent study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We thank Robert Koehler, medical librarian, for his assistance with literature review and procurement of articles.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Avalos, L.A.; Galindo, C.; Li, D.-K. A systematic review to calculate background miscarriage rates using life table analysis. Birth Defects Res. Part A Clin. Mol. Teratol. 2012, 94, 417–423. [Google Scholar] [CrossRef]
- Keyhan, S.; Muasher, L.; Muasher, S.J. Spontaneous Abortion and Recurrent Pregnancy Loss: Etiology, Diagnosis, Treatment. In Comprehensive Gynecology; Elsevier: Philadelphia, PI, USA, 2017; pp. 329–347. [Google Scholar]
- Larsen, E.C.; Christiansen, O.B.; Kolte, A.M.; Macklon, N. New insights into mechanisms behind miscarriage. BMC Med. 2013, 11, 154. [Google Scholar] [CrossRef] [Green Version]
- Branch, D.W.; Gibson, M.; Silver, R.M. Recurrent Miscarriage. New Engl. J. Med. 2010, 363, 1740–1747. [Google Scholar] [CrossRef]
- Quenby, S.; Gallos, I.D.; Dhillon-Smith, R.K.; Podesek, M.; Stephenson, M.D.; Fisher, J.; Brosens, J.J.; Brewin, J.; Ramhorst, R.; Lucas, E.S.; et al. Miscarriage 1: Miscarriage matters: The epidemiological, physical, psychological, and economic costs of early pregnancy loss. The Lancet 2021, 397, 1658–1667. [Google Scholar] [CrossRef]
- Lee, E.K.; Gutcher, S.T.; Douglass, A.B. Is sleep-disordered breathing associated with miscarriages? An emerging hypothesis. Med. Hypotheses 2014, 82, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The Occurrence of Sleep-Disordered Breathing among Middle-Aged Adults. N. Engl. J. Med. 2010, 328, 1230–1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pamidi, S.; Kimoff, R.J. Maternal Sleep-Disordered Breathing. In Chest; Elsevier Inc.: Amsterdam, The Netherlands, 2018; Volume 153, pp. 1052–1066. [Google Scholar] [CrossRef]
- Louis, J.M.; Koch, M.A.; Reddy, U.M.; Silver, R.M.; Parker, C.B.; Facco, F.L.; Redline, S.; Nhan-Chang, C.-L.; Chung, J.H.; Pien, G.W.; et al. Predictors of sleep-disordered breathing in pregnancy. Am. J. Obstet. Gynecol. 2018, 218, 521.e1–521.e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Facco, F.L.; Parker, C.B.; Reddy, U.M.; Silver, R.M.; Koch, M.A.; Louis, J.; Basner, R.C.; Chung, J.H.; Nhan-Chang, C.-L.; Pien, G.W.; et al. Association between Sleep-Disordered Breathing and Hypertensive Disorders of Pregnancy and Gestational Diabetes Mellitus. Obstet. Gynecol. 2017, 129, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Salman, L.A.; Shulman, R.; Cohen, J.B. Obstructive Sleep Apnea, Hypertension, and Cardiovascular Risk: Epidemiology, Pathophysiology, and Management. Curr. Cardiol. Rep. 2020, 22, 6. [Google Scholar] [CrossRef]
- Stanek, A.; Brożyna-Tkaczyk, K.; Myśliński, W. Oxidative Stress Markers among Obstructive Sleep Apnea Patients. Oxid Med. Cell Longev. 2021, 2021, 9681595. [Google Scholar] [CrossRef]
- Cain, M.A.; Louis, J.M. Sleep Disordered Breathing and Adverse Pregnancy Outcomes. Clin. Lab. Med. 2016, 36, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Su, G.; Wang, S.; Zhu, B. The prevalence of obstructive sleep apnea and its association with pregnancy-related health outcomes: A systematic review and meta-analysis. Sleep Breath. 2019, 23, 399–412. [Google Scholar] [CrossRef]
- Antony, K.M.; Agrawal, A.; Arndt, M.E.; Murphy, A.M.; Alapat, P.M.; Guntupalli, K.K.; Aagaard, K.M. Obstructive sleep apnea in pregnancy: Reliability of prevalence and prediction estimates. J. Perinatol. 2014, 34, 587–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antony, K.M.; Agrawal, A.; Arndt, M.E.; Murphy, A.M.; Alapat, P.M.; Guntupalli, K.K.; Aagaard, K.M. Association of adverse perinatal outcomes with screening measures of obstructive sleep apnea. J. Perinatol. 2014, 34, 441–448. [Google Scholar] [CrossRef]
- Netzer, N.C.; Stoohs, R.A.; Netzer, C.M.; Clark, K.; Strohl, K.P. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann. Intern. Med. 1999, 131, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Mm, Z.Z.; Sun, X.; Chen, R.; Lei, W.; Peng, M.; Li, X.; Zhang, N.; Cheng, J. Comparison of six assessment tools to screen for obstructive sleep apnea in patients with hypertension. Clin. Cardiol. 2021, 44, 1526–1534. [Google Scholar] [CrossRef]
- Facco, F.L.; Ouyang, D.W.; Zee, P.C.; Grobman, W. Development of a pregnancy-specific screening tool for sleep apnea. J. Clin. Sleep Med. 2012, 8, 389–394. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Rosenthal, L.D.; Dolan, D.C. The Epworth sleepiness scale in the identification of obstructive sleep apnea. J. Nerv. Ment. Dis. 2008, 196, 429–431. [Google Scholar] [CrossRef]
- Ulasli, S.S.; Gunay, E.; Koyuncu, T.; Akar, O.; Halici, B.; Ulu, S.; Unlu, M. Predictive value of Berlin Questionnaire and Epworth Sleepiness Scale for obstructive sleep apnea in a sleep clinic population. Clin. Respir. J. 2014, 8, 292–296. [Google Scholar] [CrossRef]
- Stajić, D.; Ilić, D.; Vuković, J.; Baturan, B.; Ilić, A.; Milovančev, A. The effect of continuous positive airway pressure treatment on hypertensive disorder in pregnant women with obstructive sleep apnea. Sleep Breath. 2021, 26, 297–305. [Google Scholar] [CrossRef]
- National Guideline Center (UK). Assessment Tools for People with Suspected OSAHS, OHS or COPD–OSAHS Overlap Syndrome: Obstructive Sleep Apnoea/Hypopnoea Syndrome and Obesity Hypoventilation Syndrome in Over 16 s; NICE Evidence Reviews Collection: London, UK, 2021. [Google Scholar]
- Zou, G. A Modified Poisson Regression Approach to Prospective Studies with Binary Data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Fung, A.M.; Wilson, D.L.; Barnes, M.; Walker, S.P. Obstructive sleep apnea and pregnancy: The effect on perinatal outcomes. J. Perinatol. 2012, 32, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Zinchuk, A.; Gentry, M.; Concato, J.; Yaggi, K. Phenotypes in obstructive sleep apnea: A definition, examples and evolution of approaches. Sleep Med. Rev. 2017, 35, 113. [Google Scholar] [CrossRef] [PubMed]
- Robertson, N.T.; Turner, J.M.; Kumar, S. Pathophysiological changes associated with sleep disordered breathing and supine sleep position in pregnancy. Sleep Med. Rev. 2019, 46, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Balserak, B.I. Sleep disordered breathing in pregnancy. Breathe 2015, 11, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Majid, S.; Ali, M.N.; Taing, S. Evaluation of T cell cytokines and their role in recurrent miscarriage. Int. Immunopharmacol. 2020, 82, 106347. [Google Scholar] [CrossRef]
- AbdulHussain, G.; Azizieh, F.; Makhseed, M.; Raghupathy, R. Effects of Progesterone, Dydrogesterone and Estrogen on the Production of Th1/Th2/Th17 Cytokines by Lymphocytes from Women with Recurrent Spontaneous Miscarriage. J. Reprod. Immunol. 2020, 140, 103132. [Google Scholar] [CrossRef]
- Kidron, D.; Bar-Lev, Y.; Tsarfaty, I.; Many, A.; Tauman, R. The effect of maternal obstructive sleep apnea on the placenta. Sleep 2019, 42, zsz072. [Google Scholar] [CrossRef] [PubMed]
- Ravishankar, S.; Bourjeily, G.; Lambert-Messerlian, G.; He, M.; De Paepe, M.E.; Gündoğan, F. Evidence of Placental Hypoxia in Maternal Sleep Disordered Breathing. Pediatr. Dev. Pathol. 2015, 18, 380–386. [Google Scholar] [CrossRef]
- Song, W.; Chang, W.-L.; Shan, D.; Gu, Y.; Gao, L.; Liang, S.; Guo, H.; Yu, J.; Liu, X. Intermittent Hypoxia Impairs Trophoblast Cell Viability by Triggering the Endoplasmic Reticulum Stress Pathway. Reprod. Sci. 2020, 27, 477–487. [Google Scholar] [CrossRef] [PubMed]
- Bazalakova, M. Sleep Disorders in Pregnancy. Semin Neurol. 2017, 37, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Antony, K.M.; Jacobson, N.M.; Rice, A.L.; Wiedmer, A.M.; Mourey, H.; Bazalakova, M. Obstructive Sleep Apnea in Pregnancy: Early Lessons from Our Sleep Pregnancy Clinic. WMJ 2021, E1, 1–7. [Google Scholar]
- Rice, A.L.; Bajaj, S.; Wiedmer, A.M.; Jacobson, N.; Stanic, A.K.; Antony, K.M.; Bazalakova, M.H. Continuous positive airway pressure treatment of obstructive sleep apnea and hypertensive complications in high-risk pregnancy. Sleep Breath 2022. [Google Scholar] [CrossRef] [PubMed]
- Dugas, C.; Slane, V. Miscarriage. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Practice Committe of the American Society for Reproductive Medicine, Evaluation and treatment of recurrent pregnancy loss: A committee opinion. Fertil. Steril. 2012, 98, 1103–1111. [CrossRef]
- American College of Obstetricians and Gynecologists. ACOG practice bulletin no 200: Early pregnancy loss. Obstet. Gynecol. 2018, 132, e197–e207. [Google Scholar] [CrossRef]
Figure 1.
Gravidae included for analysis. Of 1650 gravidae screened, 213 completed screening in the first trimester and were included in the analysis.
Figure 1.
Gravidae included for analysis. Of 1650 gravidae screened, 213 completed screening in the first trimester and were included in the analysis.


{kind=link}
Table 1.
Characteristics of the study population.
| Total | Miscarriage | No Miscarriage | p * | |
|---|---|---|---|---|
| N = 213 | N = 28 (13.1%) | N = 185 (86.9%) | ||
| Age | ||||
| <19 | 12 (5.6%) | 2 (7.1%) | 10 (5.4%) | 0.659 |
| 20–24 | 45 (21.1%) | 5 (17.9%) | 40 (21.6%) | |
| 25–29 | 64 (30.1%) | 6 (21.4%) | 58 (31.4%) | |
| 30–34 | 48 (22.5%) | 9 (32.1%) | 39 (21.1%) | |
| 35+ | 44 (20.7%) | 6 (21.4%) | 38 (20.5%) | |
| Gravidity | ||||
| 1 | 31 (14.6%) | 9 (32.1%) | 22 (11.9%) | 0.006 |
| 2 | 48 (22.5%) | 5 (17.7%) | 43 (23.2%) | |
| 3–5 | 120 (56.3%) | 10 (35.7%) | 110 (59.5%) | |
| 6+ | 14 (6.6%) | 4 (14.3%) | 10 (5.4%) | |
| Race/Ethnicity | ||||
| Hispanic | 191 (89.7%) | 22 (78.6%) | 169 (91.4%) | 0.116 |
| Black | 15 (7.04%) | 4 (14.2%) | 11 (6.0%) | |
| Other † | 7 (3.3%) | 2 (7.14%) | 5 (2.7%) | |
| Smoking | ||||
| Yes | 6 (2.7%) | 3 (10.7%) | 3 (1.7%) | 0.007 |
| No | 204 (97.1%) | 25 (89.3%) | 179 (98.4%) | |
| Prior Miscarriage | ||||
| Yes | 77 (36.2%) | 12 (42.9%) | 65 (35.1%) | 0.428 |
| No | 136 (63.9%) | 16 (57.1%) | 120 (64.9%) | |
| BMI ‡ | ||||
| <24.9 | 65 (30.5%) | 1 (3.6%) | 64 (34.6%) | <0.001 |
| 25.0–29.9 | 58 (27.2%) | 0 (0%) | 58 (31.4%) | |
| 30+ | 56 (26.3%) | 0 (0%) | 56 (30.3%) | |
| Missing | 34 (16.0%) | 27 (96.4%) | 7 (3.8%) | |
| Pregestational DM ‡ | ||||
| Yes | 12 (5.7%) | 4 (14.3%) | 8 (4.3%) | 0.034 |
| No | 212 (94.3%) | 24 (85.7%) | 176 (95.7%) | |
| Chronic HTN ‡ | ||||
| Yes | 16 (7.5%) | 5 (17.9%) | 11 (5.9%) | 0.026 |
| No | 197 (92.5%) | 23 (82.1%) | 174 (94.1%) |
*: p-values based on chi-square tests for independence. Bold font denotes statistical signifance by p < 0.05. † Other races included non-Hispanic White, Asian, and American Indian or Alaska Native. ‡ Body mass index (BMI), diabetes mellitus (DM), hypertension (HTN).
Table 2.
Participant characteristics by screening questionnaire and by individual questions.
| A: Characteristics by Screening Questionnaire | ||||||||||||
| Either+ * | Both− * | p | BQ+ † | BQ− | p | ESS+ † | ESS− | p | Both+ ‡ | Either– + | p § | |
| N = 64 (30.0%) | N = 149 (70.0%) | N = 31 (14.6%) | N = 182 (85.4%) | N = 40 (18.8%) | N = 173 (81.2%) | N = 7 (3.29%) | N = 206 (96.7%) | |||||
| Age | 0.954 | 0.466 | 0.486 | 0.641 | ||||||||
| <19 | 4 (6.3%) | 8 (5.4%) | 0 (0%) | 12 (6.6%) | 4 (10.0%) | 8 (4.6%) | 0 (0%) | 12 (5.8%) | ||||
| 20–24 | 14 (21.9%) | 31 (20.8%) | 5 (16.1%) | 40 (22.0%) | 10 (25.0%) | 35 (20.2%) | 1 (14.3%) | 44 (21.4%) | ||||
| 25–29 | 21 (32.8%) | 43 (28.9%) | 12 (38.7%) | 52 (28.6%) | 11 (27.5%) | 53 (30.6%) | 2 (28.6%) | 62 (30.1%) | ||||
| 30–34 | 13 (20.3%) | 35 (23.5%) | 8 (25.8%) | 40 (22.0%) | 6 (15.0%) | 42 (24.3%) | 1 (14.3%) | 47 (22.8%) | ||||
| 35+ | 12 (18.8%) | 32 (21.5%) | 6 (19.4%) | 38 (20.9%) | 9 (22.5%) | 35 (20.2%) | 3 (42.9%) | 41 (19.9%) | ||||
| Gravidity | 0.396 | 0.201 | 0.443 | 0.001 | ||||||||
| 1 | 6 (9.4%) | 25 (16.8%) | 3 (9.7%) | 28 (15.4%) | 3 (7.5%) | 28 (16.2%) | 0 (0%) | 31 (15.1%) | ||||
| 2 | 18 (28.1%) | 30 (20.1%) | 11 (35.5%) | 37 (20.3%) | 9 (22.5%) | 39 (22.5%) | 2 (28.6%) | 46 (22.3%) | ||||
| 3–5 | 36 (56.3%) | 84 (56.4%) | 14 (45.2%) | 106 (58.2%) | 24 (60.0%) | 96 (55.5%) | 2 (28.6%) | 118 (57.3%) | ||||
| 6+ | 4 (6.3%) | 10 (6.7%) | 3 (9.7%) | 11 (6.0%) | 4 (10.0%) | 10 (5.8%) | 3 (42.9%) | 11 (5.3%) | ||||
| Ethnicity | 0.086 | 0.051 | 0.247 | 0.176 | ||||||||
| Hispanic | 53 (82.8%) | 138 (92.6%) | 24 (77.4%) | 167 (91.8%) | 34 (85.0%) | 157 (90.8%) | 5 (71.4%) | 186 (90.3%) | ||||
| Black | 7 (10.9%) | 8 (5.4%) | 5 (16.1%) | 10 (5.5%) | 3 (7.5%) | 12 (6.9%) | 1 (14.3%) | 14 (6.8%) | ||||
| Other | 4 (6.3%) | 3 (2.0%) | 2 (6.5%) | 5 (2.7%) | 3 (7.5%) | 4 (2.3%) | 1 (14.3%) | 6 (2.9%) | ||||
| Smoking | 0.470 | 0.310 | 0.880 | 0.644 | ||||||||
| 1 (1.6%) | 5 (3.4%) | 0 (0%) | 6 (3.3%) | 1 (2.5%) | 5 (2.5%) | 0 (0%) | 6 (2.9%) | |||||
| No | 62 (96.9%) | 142 (95.3%) | 30 (100%) | 174 (95.6%) | 39 (97.5%) | 165 (97.1%) | 7 (100%) | 197 (97.0%) | ||||
| Prior Miscarriage | 0.130 | 0.006 | 0.574 | 0.006 | ||||||||
| Yes | 28 (43.8%) | 49 (32.9%) | 18 (58.1%) | 59 (32.4%) | 16 (40.0%) | 61 (35.3%) | 6 (85.7%) | 71 (34.5%) | ||||
| No | 36 (56.3%) | 100 (67.1%) | 13 (41.9%) | 123 (67.6%) | 24 (60.0%) | 112 (64.7%) | 1 (14.3%) | 135 (65.5%) | ||||
| BMI † | 0.502 | <0.001 | 0.105 | 0.132 | ||||||||
| <24.9 | 19 (29.7%) | 46 (30.9%) | 1 (3.2%) | 64 (35.2%) | 18 (45.0%) | 47 (27.2%) | 0 (0%) | 65 (31.6%) | ||||
| 25.0–29.9 | 16 (25.0%) | 42 (28.2%) | 6 (19.4%) | 52 (28.6%) | 11 (27.5%) | 47 (27.2%) | 1 (14.3%) | 57 (27.7%) | ||||
| 30+ | 21 (32.8%) | 35 (23.5%) | 18 (58.1%) | 38 (20.9%) | 6 (15.0%) | 50 (28.9%) | 3 (42.9%) | 53 (25.7%) | ||||
| Missing | 8 (12.5%) | 26 (17.4%) | 6 (19.4%) | 28 (15.4%) | 5 (12.5%) | 29 (16.8%) | 3 (42.9%) | 31 (15.1%) | ||||
| Pregestational DM † | 0.713 | 0.797 | 0.841 | 0.315 | ||||||||
| Yes | 3 (4.8%) | 9 (6.0%) | 2 (6.7%) | 10 (5.5%) | 2 (5.0%) | 10 (5.8%) | 1 (14.3%) | 11 (5.4%) | ||||
| No | 60 (95.2%) | 140 (94.0%) | 28 (93.3%) | 172 (94.5%) | 38 (95.0%) | 162 (94.2%) | 6 (85.7%) | 194 (94.6%) | ||||
| Chronic HTN † | 0.017 | <0.001 | 0.998 | <0.001 | ||||||||
| Yes | 9 (14.1%) | 7 (4.7%) | 9 (29.0%) | 7 (3.9%) | 3 (7.5%) | 13 (7.5%) | 3 (42.9%) | 13 (6.3%) | ||||
| No | 55 (85.9%) | 142 (95.3%) | 22 (71.0%) | 175 (96.2%) | 37 (92.5%) | 160 (92.5%) | 4 (57.1%) | 193 (93.7%) | ||||
| B: Characteristics by Screening Question | ||||||||||||
| Nap+ | Nap− | p § | Nap 3+ | Nap < 3 | p | Snore+ | Snore− | p | HTN+ † | HTN− | p | |
| N = 88 (45.4%) | N = 106 (54.6%) | N = 52 (49.8%) | N = 129 (50.2%) | N = 45 (21.1%) | N = 168 (78.9%) | N = 19 (8.92%) | N = 194 (91.1%) | |||||
| Age | 0.030 | 0.036 | 0.310 | 0.172 | ||||||||
| <19 | 5 (5.7%) | 6 (5.7%) | 2 (3.9%) | 8 (6.2%) | 0 (0%) | 12 (7.1%) | 1 (5.3%) | 11 (5.7%) | ||||
| 20–24 | 29 (33.0%) | 15 (14.2%) | 19 (36.5%) | 22 (17.1%) | 11 (24.4%) | 34 (20.2%) | 0 (0%) | 45 (23.2%) | ||||
| 25–29 | 20 (22.7%) | 38 (35.9%) | 10 (19.2%) | 45 (34.9%) | 13 (28.9%) | 51 (30.4%) | 6 (31.6%) | 58 (29.9%) | ||||
| 30–34 | 17 (19.3%) | 25 (23.6%) | 9 (17.3%) | 29 (22.5%) | 13 (28.9%) | 35 (20.8%) | 6 (31.6%) | 42 (21.7%) | ||||
| 35+ | 17 (19.3%) | 22 (20.8%) | 12 (23.1%) | 25 (19.4%) | 8 (17.8%) | 36 (21.4%) | 6 (31.6%) | 38 (19.6%) | ||||
| Gravidity | 0.154 | 0.724 | 0.016 | 0.276 | ||||||||
| 1 | 17 (19.3%) | 12 (11.3%) | 7 (13.5%) | 19 (14.7%) | 9 (20.0%) | 22 (13.1%) | 5 (26.3%) | 26 (13.4%) | ||||
| 2 | 23 (26.1%) | 20 (18.9%) | 15 (28.9%) | 27 (20.9%) | 16 (35.6%) | 32 (19.1%) | 2 (10.5%) | 46 (23.7%) | ||||
| 3–5 | 42 (47.7%) | 67 (63.2%) | 27 (51.9%) | 74 (57.4%) | 16 (35.6%) | 104 (61.9%) | 10 (52.6%) | 110 (56.7%) | ||||
| 6+ | 6 (6.8%) | 7(6.6%) | 3 (5.8%) | 9 (7.0%) | 4 (8.9%) | 10 (6.0%) | 2 (10.5%) | 12 (6.2%) | ||||
| Ethnicity | 0.126 | 0.261 | 0.055 | 0.006 | ||||||||
| Hispanic | 75 (85.2%) | 98 (92.5%) | 45 (86.5%) | 116 (89.9%) | 36 (80.0%) | 155 (92.3%) | 13 (68.4%) | 178 (91.8%) | ||||
| Black | 10 (11.4%) | 4 (3.8%) | 6 (11.5%) | 7 (5.4%) | 6 (13.3%) | 9 (5.4%) | 4 (21.1%) | 11 (5.7%) | ||||
| Other | 3 (3.4%) | 4 (3.8%) | 1 (1.9%) | 6 (4.7%) | 3 (6.7%) | 4 (2.4%) | 2 (10.5%) | 5 (2.6%) | ||||
| Smoking | 0.815 | 0.789 | 0.201 | 0.035 | ||||||||
| Yes | 3 (3.5%) | 3 (2.9%) | 2 (3.9%) | 4 (3.1%) | 0 (0%) | 6 (3.6%) | 2 (10.5%) | 4 (2.1%) | ||||
| No | 84 (96.6%) | 102 (97.1%) | 49 (96.1%) | 124 (96.9%) | 44 (100%) | 160 (96.4%) | 17 (89.5%) | 187 (97.9%) | ||||
| Prior Miscarriage | 0.489 | 0.650 | 0.545 | 0.948 | ||||||||
| Yes | 29 (33.0%) | 40 (37.7%) | 20 (38.5%) | 45 (34.9%) | 18 (40.0%) | 59 (35.1%) | 7 (36.8%) | 70 (36.1%) | ||||
| No | 59 (67.1%) | 66 (62.3%) | 32 (61.5%) | 84 (65.1%) | 27 (60.0%) | 109 (64.9%) | 12 (63.2%) | 124 (63.9%) | ||||
| BMI † | 0.093 | 0.057 | 0.023 | 0.008 | ||||||||
| <24.9 | 32 (36.4%) | 27 (25.5%) | 22 (42.3%) | 33 (25.6%) | 7 (15.6%) | 58 (34.5%) | 3 (15.8%) | 62 (32.0%) | ||||
| 25.0–29.9 | 18 (20.5%) | 34 (32.1%) | 11 (21.2%) | 39 (30.2%) | 11 (24.4%) | 47 (28.0%) | 1 (5.3%) | 57 (29.4%) | ||||
| 30+ | 27 (30.7%) | 25 (23.6%) | 15 (28.9%) | 33 (25.6%) | 15 (33.3%) | 41 (24.4%) | 9 (47.4%) | 47 (24.2%) | ||||
| Missing | 11 (12.5%) | 20 (18.9%) | 4 (7.7%) | 24 (18.6%) | 12 (26.7%) | 22 (13.1%) | 6 (31.6%) | 28 (14.4%) | ||||
| Pregestational DM † | 0.351 | 0.763 | 0.709 | 0.045 | ||||||||
| Yes | 7 (8.0%) | 5 (4.7%) | 3 (5.8%) | 6 (4.7%) | 3 (6.8%) | 9 (5.4%) | 3 (15.8%) | 9 (4.7%) | ||||
| No | 81 (92.1%) | 101 (95.3%) | 49 (94.2%) | 122 (95.3%) | 41 (93.2%) | 159 (94.6%) | 16 (84.2%) | 184 (95.3%) | ||||
| Chronic HTN | † | 0.859 | 0.063 | 0.021 | NA | NA | ||||||
| Yes | 6 (6.8%) | 8 (7.5%) | 1 (1.9%) | 13 (10.1%) | 7 (15.6%) | 9 (5.4%) | ||||||
| No | 82 (93.2%) | 99 (92.5%) | 51 (98.1%) | 116 (89.9%) | 38 (84.4%) | 159 (94.6%) | ||||||
*: Either refers to screening positive on either BQ or ESS. †: Berlin Questionnaire (BQ), Epworth Sleepiness Scale (ESS), body mass index (BMI), diabetes mellitus (DM), hypertension (HTN). ‡: Both refers to screening positive on both BQ and ESS. §: Bold font signifies statistical significance by p < 0.05.
Table 3.
Miscarriage outcomes by OSA screening questionnaires and individual questions about snoring, hypertension, and napping.
Table 3.
Miscarriage outcomes by OSA screening questionnaires and individual questions about snoring, hypertension, and napping.
| Miscarriage | p | Adjusted RR * | p | |
|---|---|---|---|---|
| Either+ (N = 64) | 6 (9.38%) | 0.286 | 0.54 (0.22–1.33) | 0.182 |
| Both− (N = 149) | 22 (14.8%) | |||
| BQ+ ‡ (N = 31) | 4 (12.9%) | 0.966 | 0.59 (0.20–1.74) | 0.343 |
| BQ− (N = 182) | 24 (13.2%) | |||
| ESS+ ‡ (N = 40) | 5 (12.5%) | 0.893 | 0.97 (0.35–2.66) | 0.946 |
| ESS− (N = 173) | 23 (13.3%) | |||
| Both+ (N = 7) | 3 (42.9%) | 0.018 * | 1.95 (0.43–8.83) | 0.385 |
| Either− (N = 206) | 25 (12.1%) | |||
| Snore+ (N = 45) | 10 (22.2%) | 0.042 | 1.64 (0.79–3.38) | 0.183 |
| Snore− (N = 168) | 18 (10.7%) | |||
| HTN+ ‡ (N = 19) | 6 (31.6%) | 0.013 | 1.78 (0.82–3.90) | 0.144 |
| HTN− (N = 194) | 22 (11.3%) | |||
| Nap+ (N = 88) | 7 (7.95%) | 0.045 | 0.44 (0.18–1.05) | 0.007 |
| Nap− (N = 106) | 19 (17.9%) | |||
| Nap 3+ (N = 52) | 2 (3.85%) | 0.030 | 0.24 (0.05–1.03) | 0.055 |
| Nap < 3 (N = 129) | 20 (15.5%) |
* Adjusted using a modified Poisson regression for significant associations as seen in Table 2A,B or for all covariates if there was no significant association. ‡ Berlin questionnaire (BQ), Epworth sleepiness scale (ESS), hypertension (HTN).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Larson, J.M.; Bazalakova, M.H.; Godecker, A.; Cooney, L.; DelBeccaro, M.; Aagaard, K.M.; Antony, K.M. Obstructive Sleep Apnea and Risk of Miscarriage. Reprod. Med. 2023, 4, 1-12. https://doi.org/10.3390/reprodmed4010001
AMA Style
Larson JM, Bazalakova MH, Godecker A, Cooney L, DelBeccaro M, Aagaard KM, Antony KM. Obstructive Sleep Apnea and Risk of Miscarriage. Reproductive Medicine. 2023; 4(1):1-12. https://doi.org/10.3390/reprodmed4010001
Chicago/Turabian StyleLarson, Jeannette M., Mihaela H. Bazalakova, Amy Godecker, Laura Cooney, Melanie DelBeccaro, Kjersti M. Aagaard, and Kathleen M. Antony. 2023. "Obstructive Sleep Apnea and Risk of Miscarriage" Reproductive Medicine 4, no. 1: 1-12. https://doi.org/10.3390/reprodmed4010001