
Overexpression of ErbB-1 (EGFR) Protein in Eutopic Endometrium of Infertile Women with Severe Ovarian Endometriosis during the ‘Implantation Window’ of Menstrual Cycle


Abstract
:1. Introduction
2. Material and Methods
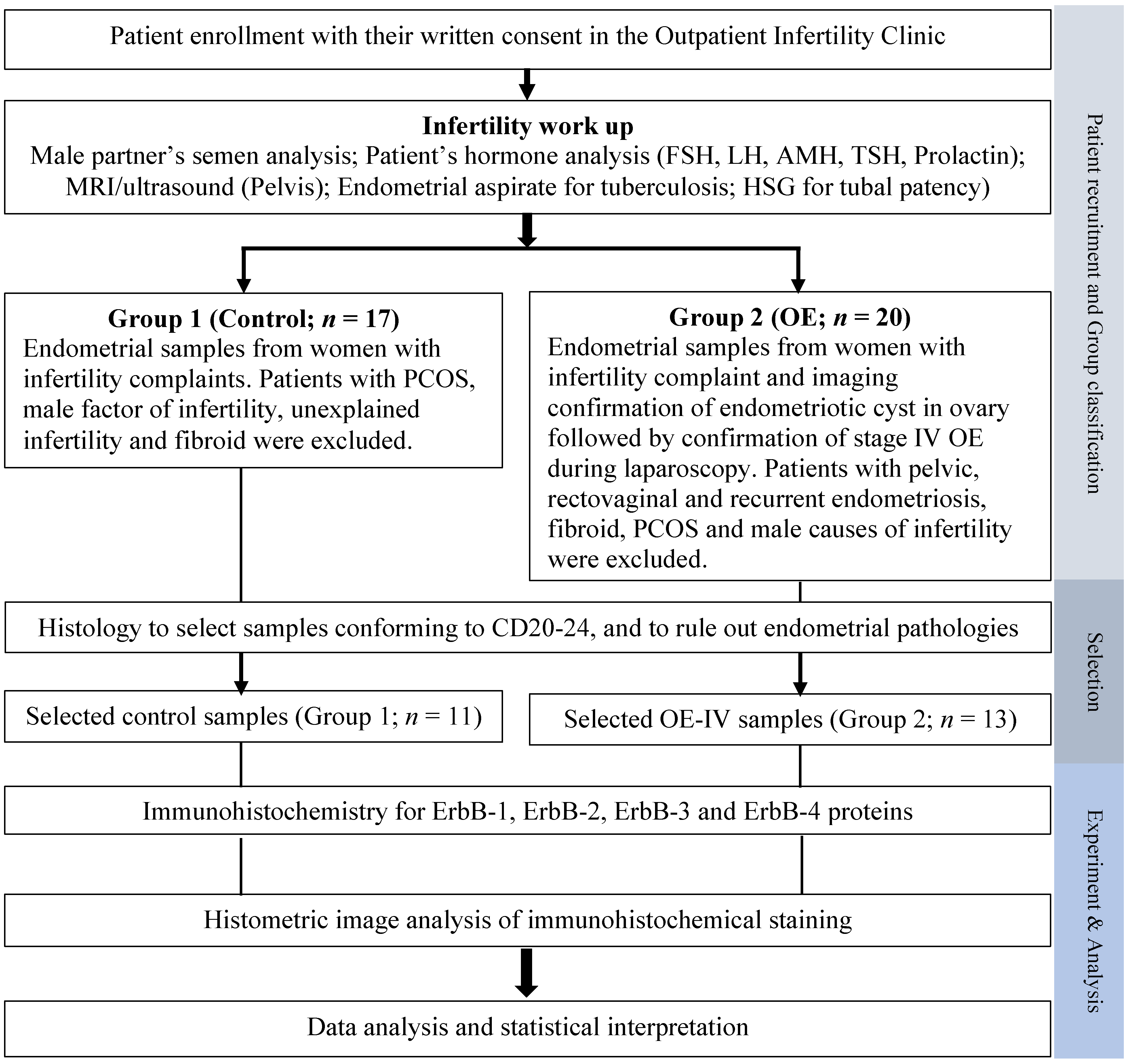
2.1. Patient Selection and Tissue Processing
2.2. Immunohistochemistry
2.3. Image and Data Analysis
3. Results
3.1. General
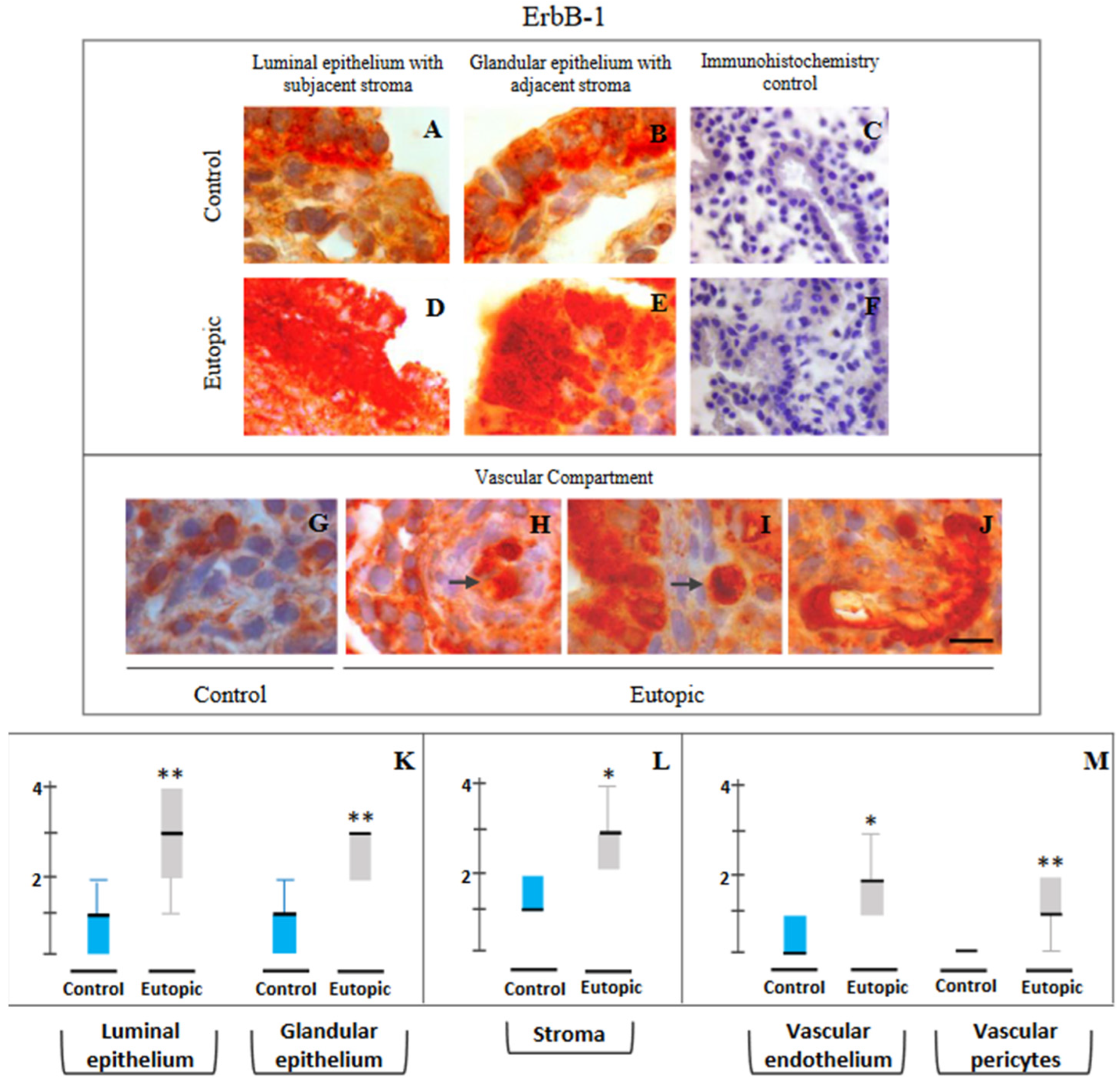
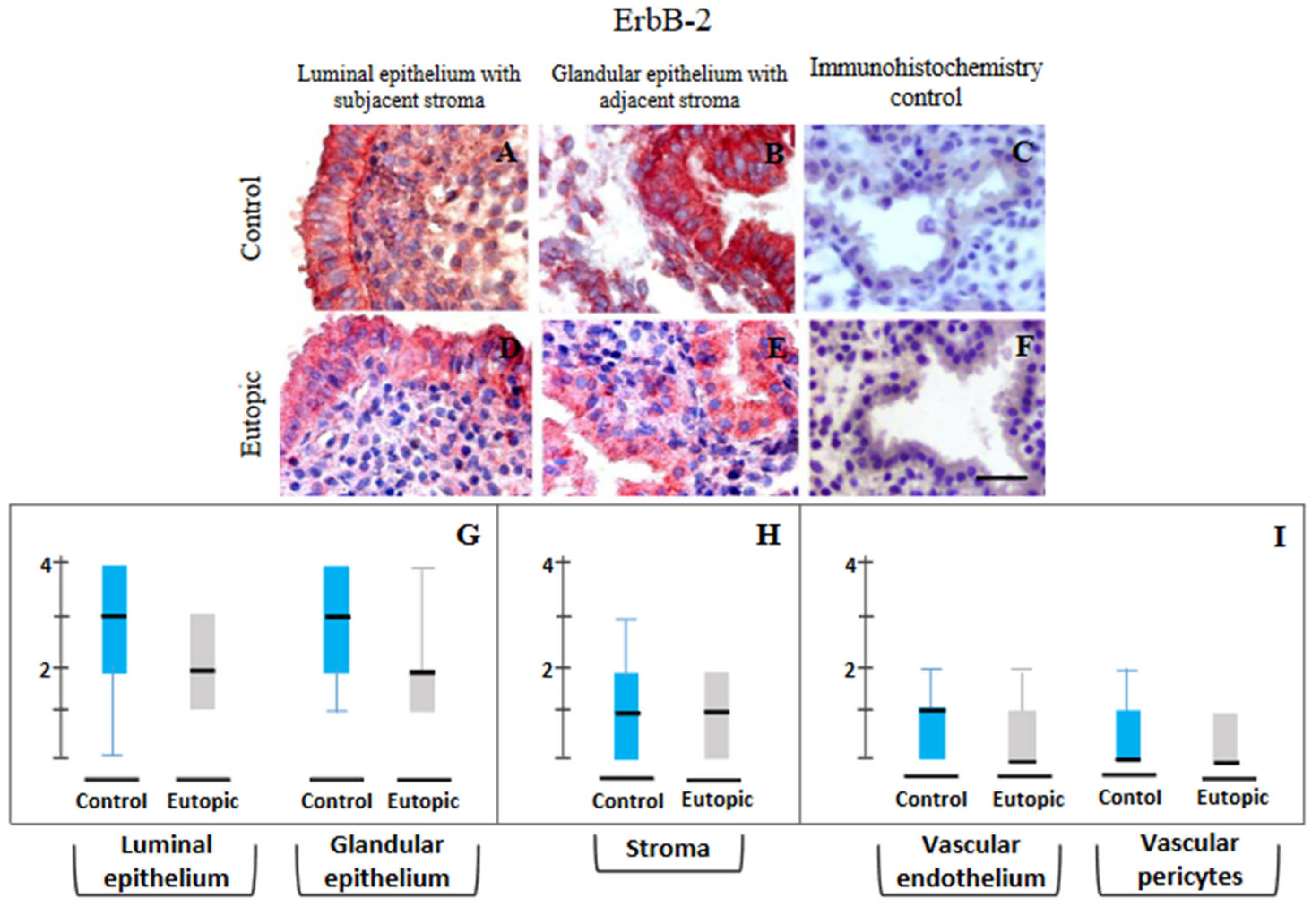
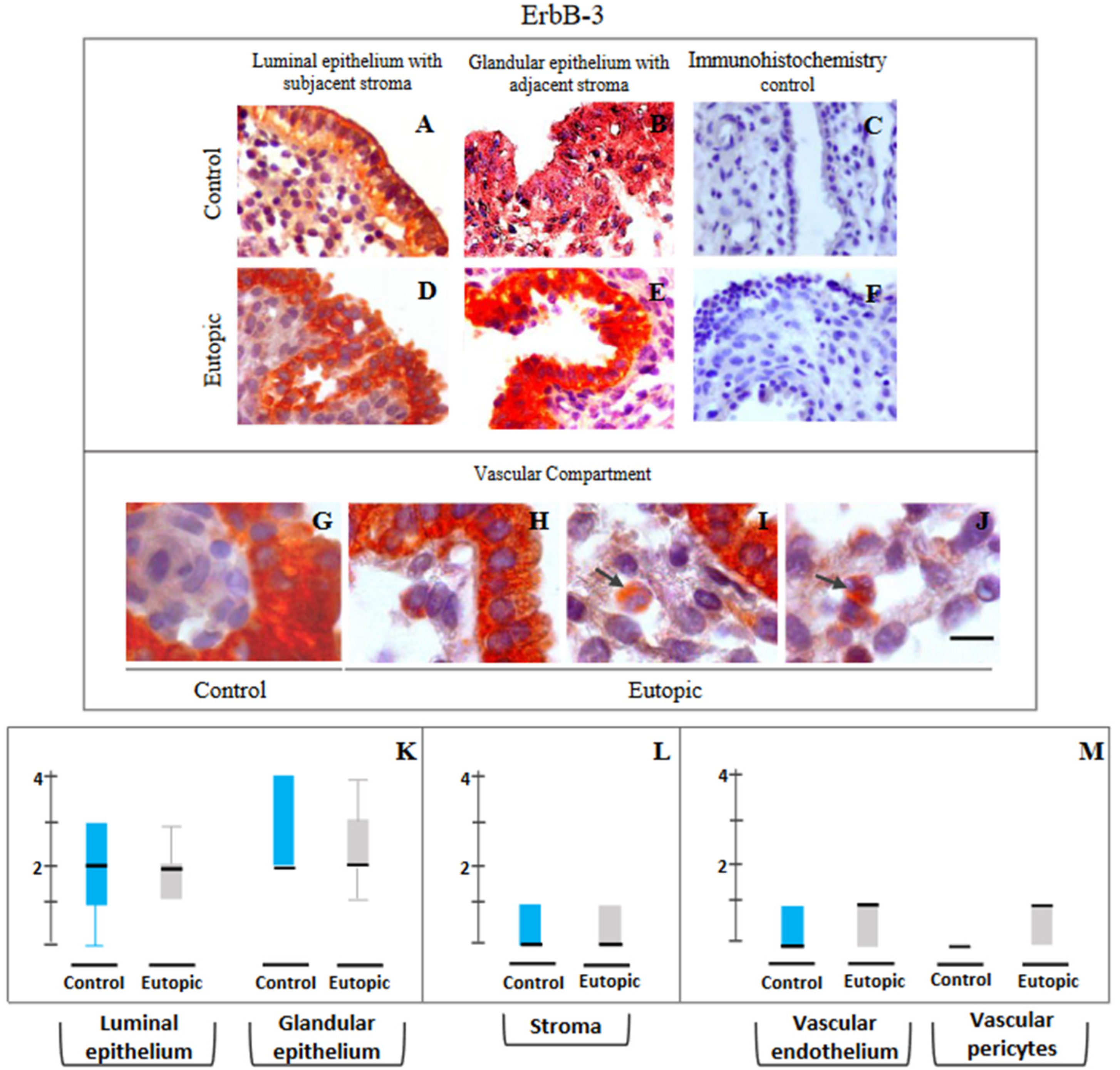
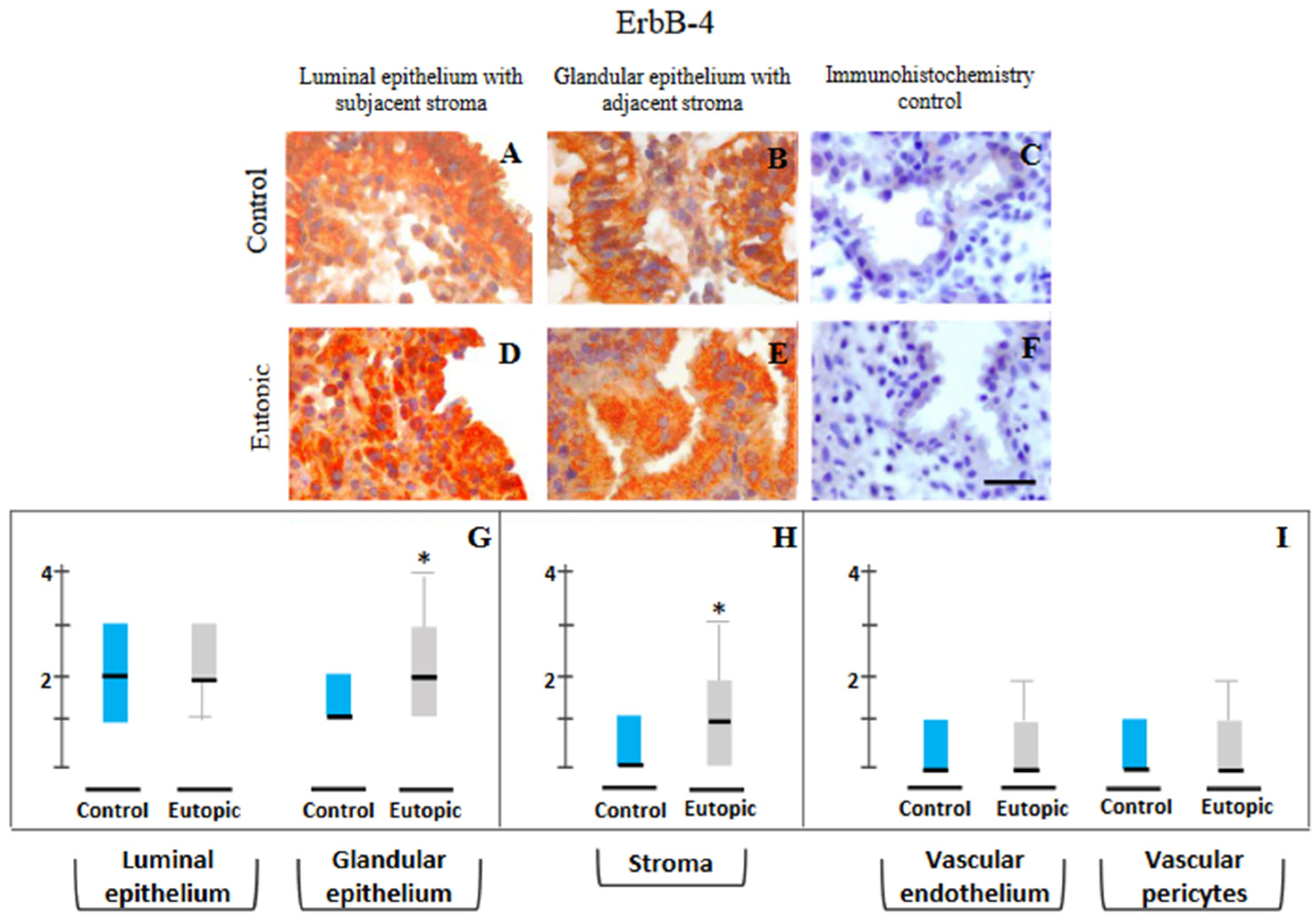
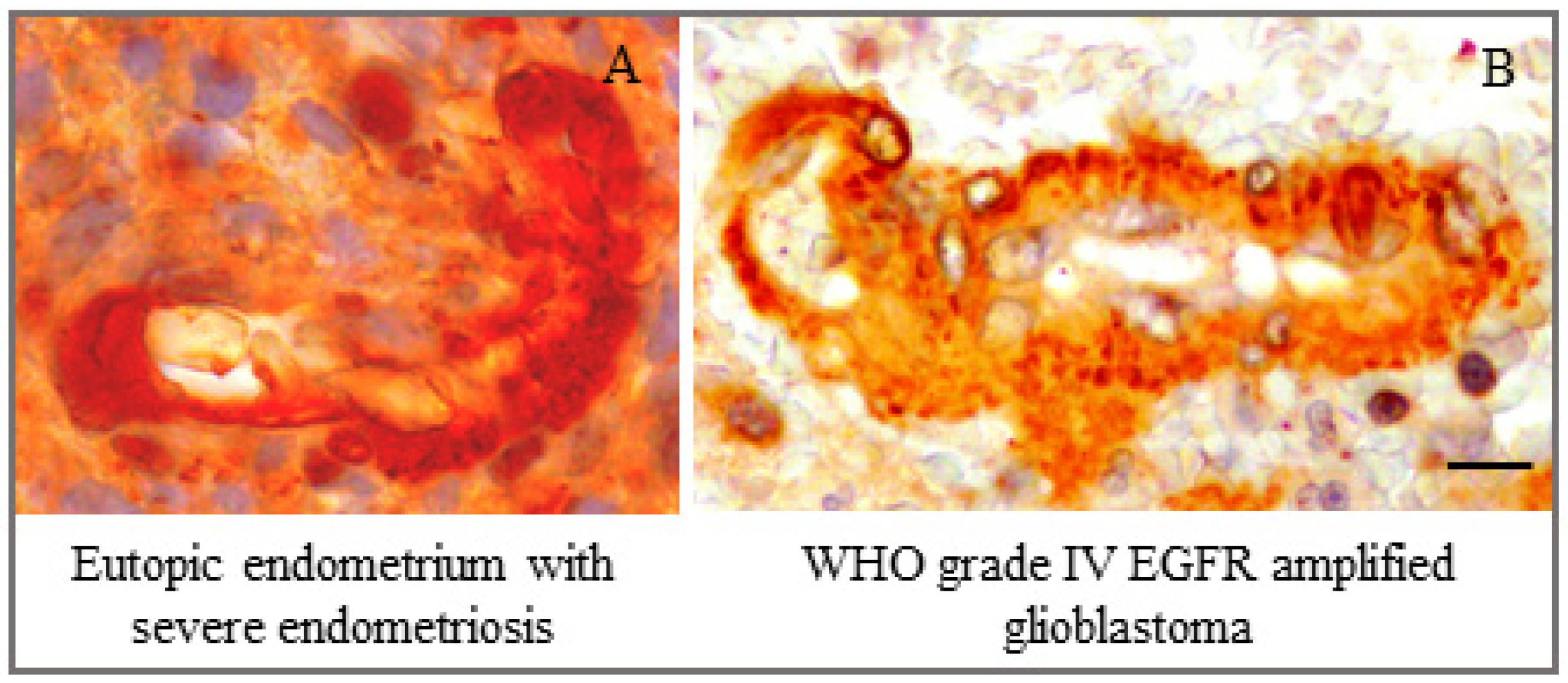
3.2. Immunohistochemical Localization
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sampson, J.A. Heterotopic or misplaced endometrial tissue. Am. J. Obstet. Gynecol. 1925, 10, 649–664. [Google Scholar] [CrossRef]
- Liu, D.T.; Hitchcock, A. Endometriosis: Its association with retrograde menstruation, dysmenorrhoea and tubal pathology. Br. J. Obstet. Gynaecol. 1986, 93, 859–862. [Google Scholar] [CrossRef]
- Brosens, I.; Brosens, J.J.; Benagiano, G. The eutopic endometrium in endometriosis: Are the changes of clinical significance? Reprod. Biomed. Online 2012, 24, 496–502. [Google Scholar] [CrossRef] [Green Version]
- Anupa, G.; Sharma, J.B.; Roy, K.K.; Sengupta, J.; Ghosh, D. An assessment of the multifactorial profile of steroid-metabolizing enzymes and steroid receptors in the eutopic endometrium during moderate to severe ovarian endometriosis. Reprod. Biol. Endocrinol. 2019, 17, 111. [Google Scholar] [CrossRef] [Green Version]
- Coccia, M.E.; Nardone, L.; Rizzello, F. Endometriosis and infertility: A long-life approach to preserve reproductive integrity. Int. J. Environ. Res. Public Health 2022, 19, 6162. [Google Scholar] [CrossRef]
- Ghosh, D.; Filaretova, L.; Bharti, J.; Roy, K.K.; Sharma, J.B.; Sengupta, J. Pathophysiological basis of endometriosis-linked stress associated with pain and infertility: A conceptual review. Reprod. Med. 2020, 1, 32–61. [Google Scholar] [CrossRef]
- Agrawal, S.; Jayant, K. Why endometriosis causes infertility? Br. J. Adv. Med. Med. Res. 2016, 18, 1–7. [Google Scholar] [CrossRef]
- Wingfield, M.; Macpherson, A.; Healy, D.L.; Rogers, P.A. Cell proliferation is increased in the endometrium of women with endometriosis. Fertil. Steril. 1995, 64, 340–346. [Google Scholar] [CrossRef]
- Johnson, M.C.; Torres, M.; Alves, A.; Bacallao, K.; Fuentes, A.; Vega, M.; Boric, M.A. Augmented cell survival in eutopic endometrium from women with endometriosis: Expression of c-myc, TGF-beta1 and bax genes. Reprod. Biol. Endocrinol. 2005, 3, 45. [Google Scholar] [CrossRef] [Green Version]
- Velarde, M.C.; Aghajanova, L.; Nezhat, C.R.; Giudice, L.C. Increased mitogen activated protein kinase kinase/extracellularly regulated kinase activity in human endometrial stromal fibroblasts of women with endometriosis reduces 3′,5′-cyclic adenosine 5′-monophosphate inhibition of cyclin D1. Endocrinology 2009, 150, 4701–4712. [Google Scholar] [CrossRef]
- Franco-Murillo, Y.; Miranda-Rodríguez, J.A.; Rendón-Huerta, E.; Montaño, L.F.; Cornejo, G.V.; Gómez, L.P.; Valdez-Morales, F.J.; Gonzalez-Sanchez, I.; Cerbón, M. Unremitting cell proliferation in the secretory phase of eutopic endometriosis: Involvement of pAkt and pGSK3β. Reprod. Sci. 2015, 22, 502–510. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.J.; Yoo, J.Y.; Kim, T.H.; Fazleabas, A.T.; Young, S.L.; Lessey, B.A.; Jeong, J.W. Overexpression of Four Joint Box-1 Protein (FJX1) in eutopic endometrium from women with endometriosis. Reprod. Sci. 2018, 25, 207–213. [Google Scholar] [CrossRef]
- Anupa, G.; Poorasamy, J.; Bhat, M.A.; Sharma, J.B.; Sengupta, J.; Ghosh, D. Endometrial stromal cell inflammatory phenotype during severe ovarian endometriosis as a cause of endometriosis-associated infertility. Reprod. Biomed. Online 2020, 41, 623–639. [Google Scholar] [CrossRef]
- Tomassetti, C.; Meuleman, C.; Pexsters, A.; Mihalyi, A.; Kyama, C.; Simsa, P.; D’Hooghe, T.M. Endometriosis, recurrent miscarriage and implantation failure: Is there an immunological link? Reprod. Biomed. Online 2006, 13, 58–64. [Google Scholar] [CrossRef]
- Yarden, Y.; Sliwkowski, M.X. Untangling the ErbB signalling network. Nat. Rev. Mol. Cell Biol. 2001, 2, 127–137. [Google Scholar] [CrossRef]
- Linggi, B.; Carpenter, G. ErbB receptors: New insights on mechanisms and biology. Trend. Cell Biol. 2006, 16, 649–656. [Google Scholar] [CrossRef]
- Scaltriti, M.; Baselga, J. The epidermal growth factor receptor pathway: A model for targeted therapy. Clin. Cancer Res. 2006, 12, 5268–5272. [Google Scholar] [CrossRef] [Green Version]
- Wieduwilt, M.J.; Moasser, M.M. The epidermal growth factor receptor family: Biology driving targeted therapeutics. Cell. Mol. Life Sci. 2008, 65, 1566–1584. [Google Scholar] [CrossRef] [Green Version]
- Ejskjær, K.; Sørense, B.S.; Poulsen, S.S.; Mogensen, O.; Forman, A.; Nexø, E. Expression of the epidermal growth factor system in human endometrium during the menstrual cycle. Mol. Hum. Reprod. 2005, 11, 543–551. [Google Scholar] [CrossRef] [Green Version]
- Ejskjaer, K.; Sorensen, B.S.; Poulsen, S.S.; Mogensen, O.; Forman, A.; Nexo, E. Expression of the epidermal growth factor system in eutopic endometrium from women with endometriosis differs from that in endometrium from healthy women. Gynecol. Obstet. Investig. 2009, 67, 118–126. [Google Scholar] [CrossRef]
- Aghajanova, L.; Giudice, L.C. Molecular evidence for differences in endometrium in severe versus mild endometriosis. Reprod. Sci. 2011, 18, 229–251. [Google Scholar] [CrossRef]
- Khan, M.A.; Sengupta, J.; Mittal, S.; Ghosh, D. Genome-wide expressions in autologous eutopic and ectopic endometrium of fertile women with endometriosis. Reprod. Biol. Endocrinol. 2012, 10, 84. [Google Scholar] [CrossRef] [Green Version]
- Bergh, P.A.; Navot, D. The impact of embryonic development and endometrial maturity on the timing of implantation. Fertil. Steril. 1992, 58, 537–542. [Google Scholar] [CrossRef]
- Wilcox, A.J.; Baird, D.D.; Weinberg, C.R. Time of implantation of the conceptus and loss of pregnancy. N. Engl. J. Med. 1999, 340, 1796–1799. [Google Scholar] [CrossRef]
- Fassbender, A.; Rahmioglu, N.; Vitonis, A.F.; Viganò, P.; Giudice, L.C.; D’Hooghe, T.M.; Hummelshoj, L.; Adamson, G.D.; Becker, C.M.; Missmer, S.A.; et al. WERF EPHect Working Group. World Endometriosis Research Foundation endometriosis phenome and biobanking harmonisation project: IV. Tissue collection, processing, and storage in endometriosis research. Fertil. Steril. 2014, 102, 1244–1253. [Google Scholar] [CrossRef]
- Miller, L.M.; Johnson, N.P. EPHect—The Endometriosis Phenome (and Biobanking) Harmonisation Project—May be very helpful for clinicians and the women they are treating. F1000Research 2017, 6, 14. [Google Scholar] [CrossRef]
- Hofmann, G.E.; Scott, R.T., Jr.; Bergh, P.A.; Deligdisch, L. Immunohistochemical localization of epidermal growth factor in human endometrium, decidua, and placenta. J. Clin. Endocrinol. Metab. 1991, 73, 882–887. [Google Scholar] [CrossRef]
- Srinivasan, R.; Benton, E.; McCormick, F.; Thomas, H.; Gullick, W.J. Expression of the c-erbB-3/HER-3 and c-erbB-4/HER-4 growth factor receptors and their ligands, neuregulin-1 alpha, neuregulin-1 beta, and betacellulin, in normal endometrium and endometrial cancer. Clin. Cancer Res. 1999, 5, 2877–2883. [Google Scholar] [PubMed]
- GeneCards Home Page for Human Gene Database. Available online: http://www.genecards.org/ (accessed on 30 September 2022).
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Bhat, M.A.; Sharma, J.B.; Roy, K.K.; Sengupta, J.; Ghosh, D. Genomic evidence of Y chromosome microchimerism in the endometrium during endometriosis and in cases of infertility. Reprod. Biol. Endocrinol. 2019, 17, 22. [Google Scholar] [CrossRef]
- Sharma, J.B.; Karmakar, D.; Hari, S.; Singh, N.; Singh, S.P.; Kumar, S.; Roy, K.K. Magnetic resonance imaging findings among women with tubercular tubo-ovarian masses. Int. J. Gynaecol. Obstet. 2011, 113, 76–80. [Google Scholar] [CrossRef]
- Noyes, R.W.; Hertig, A.T.; Rock, J. Dating the endometrial biopsy. Fertil. Steril. 1950, 1, 3–25. [Google Scholar] [CrossRef]
- Srivastava, A.; Sengupta, J.; Kriplani, A.; Roy, K.K.; Ghosh, D. Profiles of cytokines secreted by isolated human endometrial cells under the influence of chorionic gonadotropin during the window of embryo implantation. Reprod. Biol. Endocrinol. 2013, 11, 116. [Google Scholar] [CrossRef] [Green Version]
- Bhat, M.A.; Khan, M.A.; Lalitkumar, P.G.L.; Poorasamy, J.; Sengupta, J.; Ghosh, D. Preimplantation endometrial transcriptomics in natural conception cycle of the rhesus monkey. Reprod. Med. 2022, 3, 16–35. [Google Scholar] [CrossRef]
- Bondarenko, A.; Angrisani, N.; Meyer-Lindenberg, A.; Seitz, J.M.; Waizy, H.; Reifenrath, J. Magnesium-based bone implants: Immunohistochemical analysis of peri-implant osteogenesis by evaluation of osteopontin and osteocalcin expression. J. Biomed. Mater. Res. Part A 2014, 102, 1449–1457. [Google Scholar] [CrossRef]
- Sim, J.; Wright, C.C. The kappa statistic in reliability studies: Use, interpretation, and sample size requirements. Phys. Ther. 2005, 85, 257–268. [Google Scholar] [CrossRef] [Green Version]
- Fitzgibbons, P.L.; Bradley, L.A.; Fatheree, L.A.; Alsabeh, R.; Fulton, R.S.; Goldsmith, J.D.; Haas, T.S.; Karabakhtsian, R.G.; Loykasek, P.A.; Marolt, M.J.; et al. College of American Pathologists Pathology and Laboratory Quality Center. Principles of analytic validation of immunohistochemical assays: Guideline from the College of American Pathologists Pathology and Laboratory Quality Center. Arch. Pathol. Lab. Med. 2014, 138, 1432–1443. [Google Scholar] [CrossRef] [Green Version]
- Moratin, J.; Mock, A.; Obradovic, S.; Metzger, K.; Flechtenmacher, C.; Zaoui, K.; Fröhling, S.; Jäger, D.; Krauss, J.; Hoffmann, J.; et al. Digital pathology scoring of immunohistochemical staining reliably identifies prognostic markers and anatomical associations in a large cohort of oral cancers. Front. Oncol. 2011, 11, 712944. [Google Scholar] [CrossRef]
- Dytham, C. Choosing and Using Statistics: A Biologist’s Guide, 3rd ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2010; pp. 145–150. [Google Scholar]
- Large, M.J.; Wetendorf, M.; Lanz, R.B.; Hartig, S.M.; Creighton, C.J.; Mancini, M.A.; Kovanci, E.; Lee, K.-F.; Threadgill, D.W.; Lydon, J.P.; et al. The epidermal growth factor receptor critically regulates endometrial function during early pregnancy. PLoS Genet. 2014, 10, e1004451. [Google Scholar] [CrossRef] [Green Version]
- Yoo, H.J.; Barlow, D.H.; Mardon, H.J. Temporal and spatial regulation of expression of heparin-binding epidermal growth factor-like growth factor in the human endometrium: A possible role in blastocyst implantation. Dev. Genet. 1997, 21, 102–108. [Google Scholar] [CrossRef]
- Möller, B.; Rasmussen, C.; Lindblom, B.; Olovsson, M. Expression of the angiogenic growth factors VEGF, FGF-2, EGF and their receptors in normal human endometrium during the menstrual cycle. Mol. Hum. Reprod. 2001, 7, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Chobotova, K.; Karpovich, N.; Carver, J.; Manek, S.; Gullick, W.J.; Barlow, D.H.; Mardon, H.J. Heparin-binding epidermal growth factor and its receptors mediate decidualization and potentiate survival of human endometrial stromal cells. J. Clin. Endocrinol. Metab. 2005, 90, 913–919. [Google Scholar] [CrossRef] [Green Version]
- Brys, M.; Semczuk, A.; Rechberger, T.; Krajewska, W.M. Expression of erbB-1 and erbB-2 genes in normal and pathological human endometrium. Oncol. Rep. 2007, 18, 261–265. [Google Scholar] [CrossRef] [Green Version]
- Burney, R.O.; Talbi, S.; Hamilton, A.E.; Vo, K.C.; Nyegaard, M.; Nezhat, C.R.; Lessey, B.A.; Giudice, L.C. Gene expression analysis of endometrium reveals progesterone resistance and candidate susceptibility genes in women with endometriosis. Endocrinology 2007, 148, 3814–3826. [Google Scholar] [CrossRef] [Green Version]
- Wee, P.; Wang, Z. Epidermal growth factor receptor cell proliferation signaling pathways. Cancers 2017, 5, 52. [Google Scholar] [CrossRef] [Green Version]
- Brar, A.K.; Frank, G.R.; Kessler, C.A.; Cedars, M.I.; Handwerger, S. Progesterone-dependent decidualization of the human endometrium is mediated by cAMP. Endocrine 1997, 6, 301–307. [Google Scholar] [CrossRef]
- Stadtmauer, D.J.; Wagner, G.P. Single-cell analysis of prostaglandin E2-induced human decidual cell in vitro differentiation: A minimal ancestral deciduogenic signal. Biol. Reprod. 2022, 106, 155–172. [Google Scholar] [CrossRef]
- Erikson, D.W.; Chen, J.C.; Piltonen, T.T.; Conti, M.; Irwin, J.C.; Giudice, L.C. Inhibition of epidermal growth factor receptor restores decidualization markers in stromal fibroblasts from women with endometriosis. J. Endometr. Pelvic Pain Disord. 2014, 6, 196–211. [Google Scholar] [CrossRef] [Green Version]
- Houshdaran, S.; Oke, A.B.; Fung, J.C.; Vo, K.C.; Nezhat, C.; Giudice, L.C. Steroid hormones regulate genome-wide epigenetic programming and gene transcription in human endometrial cells with marked aberrancies in endometriosis. PLoS Genet. 2020, 16, e1008601. [Google Scholar] [CrossRef]
- Chatterjee, K.; Jana, S.; DasMahapatra, P.; Swarnakar, S. EGFR-mediated matrix metalloproteinase-7 up-regulation promotes epithelial-mesenchymal transition via ERK1-AP1 axis during ovarian endometriosis progression. FASEB J. 2018, 32, 4560–4572. [Google Scholar] [CrossRef]
- Chan, G.; Nogalski, M.T.; Yurochko, A.D. Activation of EGFR on monocytes is required for human cytomegalovirus entry and mediates cellular motility. Proc. Natl. Acad. Sci. USA 2009, 106, 22369–22374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryzhov, S.; Matafonov, A.; Galindo, C.L.; Zhang, Q.; Tran, T.L.; Lenihan, D.J.; Lenneman, C.G.; Feoktistov, I.; Sawyer, D.B. ERBB signaling attenuates proinflammatory activation of nonclassical monocytes. Am. J. Physiol. Heart. Circ. Physiol. 2017, 312, H907–H918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardbower, D.M.; Singh, K.; Asim, M.; Verriere, T.G.; Olivares-Villagómez, D.; Barry, D.P.; Allaman, M.M.; Washington, M.K.; Peek, R.M., Jr.; Piazuelo, M.B.; et al. EGFR regulates macrophage activation and function in bacterial infection. J. Clin. Investig. 2016, 126, 3296–3312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lash, G.E.; Innes, B.A.; Drury, J.A.; Robson, S.C.; Quenby, S.; Bulmer, J.N. Localization of angiogenic growth factors and their receptors in the human endometrium throughout the menstrual cycle and in recurrent miscarriage. Hum. Reprod. 2012, 27, 183–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plate, K.H.; Risau, W. Angiogenesis in malignant gliomas. Glia 1995, 15, 339–347. [Google Scholar] [CrossRef]
- Turner, S.G. Angiogenesis in malignant gliomas and bevacizumab resistance. In Brain and Spinal Tumors—Primary and Secondary; Morgan, L.B., Sarica, F.B., Eds.; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef] [Green Version]
- Bergers, G.; Song, S. The role of pericytes in blood-vessel formation and maintenance. Neuro-Oncology 2005, 7, 452–464. [Google Scholar] [CrossRef] [Green Version]
- Turner, K.M.; Deshpande, V.; Beyter, D.; Koga, T.; Rusert, J.; Lee, C.; Li, B.; Arden, K.; Ren, B.; Nathanson, D.A.; et al. Extrachromosomal oncogene amplification drives tumour evolution and genetic heterogeneity. Nature 2017, 543, 122–125. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, D.; Anupa, G.; Bhat, M.A.; Bharti, J.; Mirdha, A.R.; Sharma, J.B.; Roy, K.K.; Sengupta, J. How benign is endometriosis: Multi-scale interrogation of documented evidence. Curr. Opin. Gynecol. Obstet. 2019, 2, 318–345. [Google Scholar]
- Farnsworth, D.A.; Chen, Y.T.; de Rappard Yuswack, G.; Lockwood, W.W. Emerging molecular dependencies of mutant EGFR-driven non-small cell lung cancer. Cell 2021, 10, 3553. [Google Scholar] [CrossRef]
- Franco Nitta, C.; Green, E.W.; Jhamba, E.D.; Keth, J.M.; Ortiz-Caraveo, I.; Grattan, R.M.; Schodt, D.J.; Gibson, A.C.; Rajput, A.; Lidke, K.A.; et al. EGFR transactivates RON to drive oncogenic crosstalk. eLife 2021, 10, e63678. [Google Scholar] [CrossRef]
- Raevskiy, M.; Sorokin, M.; Vladimirova, U.; Suntsova, M.; Efimov, V.; Garazha, A.; Drobyshev, A.; Moisseev, A.; Rumiantsev, P.; Li, X.; et al. EGFR pathway-based gene signatures of druggable gene mutations in melanoma, breast, lung, and thyroid cancers. Biochemistry 2021, 86, 1477–1488. [Google Scholar] [CrossRef] [PubMed]
- Augustine, T.A.; Baig, M.; Sood, A.; Budagov, T.; Atzmon, G.; Mariadason, J.M.; Aparo, S.; Maitra, R.; Goel, S. Telomere length is a novel predictive biomarker of sensitivity to anti-EGFR therapy in metastatic colorectal cancer. Br. J. Cancer 2015, 112, 313–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Offterdinger, M.; Schöfer, C.; Weipoltshammer, K.; Grunt, T.W. c-erbB-3: A nuclear protein in mammary epithelial cells. J. Cell Biol. 2002, 157, 929–939. [Google Scholar] [CrossRef] [Green Version]
- Tagliaferro, M.; Rosa, P.; Bellenchi, G.C. Nucleolar localization of the ErbB3 receptor as a new target in glioblastoma. BMC Mol. Cell Biol. 2022, 23, 13. [Google Scholar] [CrossRef] [PubMed]
- Giri, D.K.; Ali-Seyed, M.; Li, L.Y.; Lee, D.F.; Ling, P.; Bartholomeusz, G.; Wang, S.C.; Hung, M.C. Endosomal transport of ErbB-2: Mechanism for nuclear entry of the cell surface receptor. Mol. Cell. Biol. 2005, 25, 11005–110018. [Google Scholar] [CrossRef] [Green Version]
- Black, L.E.; Longo, J.F.; Carroll, S.L. Mechanisms of receptor tyrosine-protein kinase ErbB-3 (ERBB3) action in human neoplasia. Am. J. Pathol. 2019, 189, 1898–1912. [Google Scholar] [CrossRef] [Green Version]
- Moghbeli, M.; Makhdoumi, Y.; Soltani Delgosha, M.; Aarabi, A.; Dadkhah, E.; Memar, B.; Abdollahi, A.; Abbaszadegan, M.R. ErbB1 and ErbB3 co-over expression as a prognostic factor in gastric cancer. Biol. Res. 2019, 52, 2. [Google Scholar] [CrossRef]
- Uncu, G.; Kasapoglu, I.; Ozerkan, K.; Seyhan, A.; Oral Yilmaztepe, A.; Ata, B. Prospective assessment of the impact of endometriomas and their removal on ovarian reserve and determinants of the rate of decline in ovarian reserve. Hum. Reprod. 2013, 28, 2140–2145. [Google Scholar] [CrossRef]
- Kasapoglu, I.; Ata, B.; Uyaniklar, O.; Seyhan, A.; Orhan, A.; Yildiz Oguz, S.; Uncu, G. Endometrioma-related reduction in ovarian reserve (ERROR): A prospective longitudinal study. Fertil. Steril. 2018, 110, 122–127. [Google Scholar] [CrossRef]
- McBean, J.H.; Brumsted, J.R.; Stirewalt, W.S. In vivo estrogen regulation of epidermal growth factor receptor in human endometrium. J. Clin. Endocrinol. Metab. 1997, 82, 1467–1471. [Google Scholar] [CrossRef]
- Salvatori, L.; Ravenna, L.; Felli, M.P.; Cardillo, M.R.; Russo, M.A.; Frati, L.; Gulino, A.; Petrangeli, E. Identification of an estrogen-mediated deoxyribonucleic acid-binding independent transactivation pathway on the epidermal growth factor receptor gene promoter. Endocrinology 2000, 141, 2266–2274. [Google Scholar] [CrossRef] [PubMed]
- Skandalis, S.S.; Afratis, N.; Smirlaki, G.; Nikitovic, D.; Theocharis, A.D.; Tzanakakis, G.N.; Karamanos, N.K. Cross-talk between estradiol receptor and EGFR/IGF-IR signaling pathways in estrogen-responsive breast cancers: Focus on the role and impact of proteoglycans. Matrix Biol. 2014, 35, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Miturski, R.; Semczuk, A.; Postawski, K.; Jakowicki, J.A. Epidermal growth factor receptor immunostaining and epidermal growth factor receptor-tyrosine kinase activity in proliferative and neoplastic human endometrium. Tumour Biol. 2000, 21, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Poorasamy, J.; Sengupta, J.; Patil, A.; Ghosh, D. Progesterone resistance in endometriosis. Eur. Med. J. 2022, 8, 51–63. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name of ErbB Family Member (Alias *) | Salient Observations [References] |
|---|---|
| ErbB-1 (EGFR, HER1) | Epithelial as well as stromal compartment of human endometrium express EGF and ErbB-1 [19,27]. In endometriosis, EGFR (ErbB-1) mRNA is upregulated in endometriotic eutopic endometrium, especially during the secretory period, compared with normal endometrium [20,21,22]. |
| ErbB-2 (HER2/neu) | ErbB-2 showed high expression during the early secretory phase [19]. Endometrial mRNA for ErbB-2 was higher in endometriotic eutopic endometrium compared with normal endometrium [20]. |
| ErbB-3 (HER3) | ErbB-3 showed high expression during the secretory phase [19,28]. Endometrial mRNA for ErbB-3 was higher in endometriotic eutopic endometrium compared with normal endometrium [20,22]. |
| ErbB-4 (HER4) | ErbB-4 showed high expression during the secretory phase [19,28]. Endometrial mRNA for ErbB-4 was comparable between endometriotic eutopic endometrium and normal endometrium [20]. |
| Parameter | Group | |
|---|---|---|
| 1 | 2 | |
| Group description | Control | OE-IV |
| Fertility history | Infertile * | Infertile * |
| Duration of infertility (months) | 21 ± 9.0 | 21.1 ± 8.7 |
| Recruited (Number) | 17 | 20 |
| Selected ** (Number) | 11 | 13 |
| Age in years a | 29.1 ± 4.1 | 29.8 ± 4.7 |
| BMI (kg/m2) a | 20.4 ± 3.2 | 21.9 ± 4.2 |
| Length of menstrual cycle in days a | 28.7 ± 1.3 | 28.8 ± 1.5 |
| Cycle day of sample collection a | 22.6 ± 2.3 | 21.8 ± 2.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poorasamy, J.; Garg, D.; Bharti, J.; Nambirajan, A.; Patil, A.; Sengupta, J.; Ghosh, D. Overexpression of ErbB-1 (EGFR) Protein in Eutopic Endometrium of Infertile Women with Severe Ovarian Endometriosis during the ‘Implantation Window’ of Menstrual Cycle. Reprod. Med. 2022, 3, 280-296. https://doi.org/10.3390/reprodmed3040022
Poorasamy J, Garg D, Bharti J, Nambirajan A, Patil A, Sengupta J, Ghosh D. Overexpression of ErbB-1 (EGFR) Protein in Eutopic Endometrium of Infertile Women with Severe Ovarian Endometriosis during the ‘Implantation Window’ of Menstrual Cycle. Reproductive Medicine. 2022; 3(4):280-296. https://doi.org/10.3390/reprodmed3040022
Chicago/Turabian StylePoorasamy, Jeevitha, Deepali Garg, Juhi Bharti, Aruna Nambirajan, Asmita Patil, Jayasree Sengupta, and Debabrata Ghosh. 2022. "Overexpression of ErbB-1 (EGFR) Protein in Eutopic Endometrium of Infertile Women with Severe Ovarian Endometriosis during the ‘Implantation Window’ of Menstrual Cycle" Reproductive Medicine 3, no. 4: 280-296. https://doi.org/10.3390/reprodmed3040022