
Variation in Anti-Mullerian Hormone Levels with Age in Women Accessing In Vitro Fertilization Services in Ghana


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Site
2.2. Study Population
2.3. Blood Collection and AMH Analysis in Serum
3. Statistical Analysis
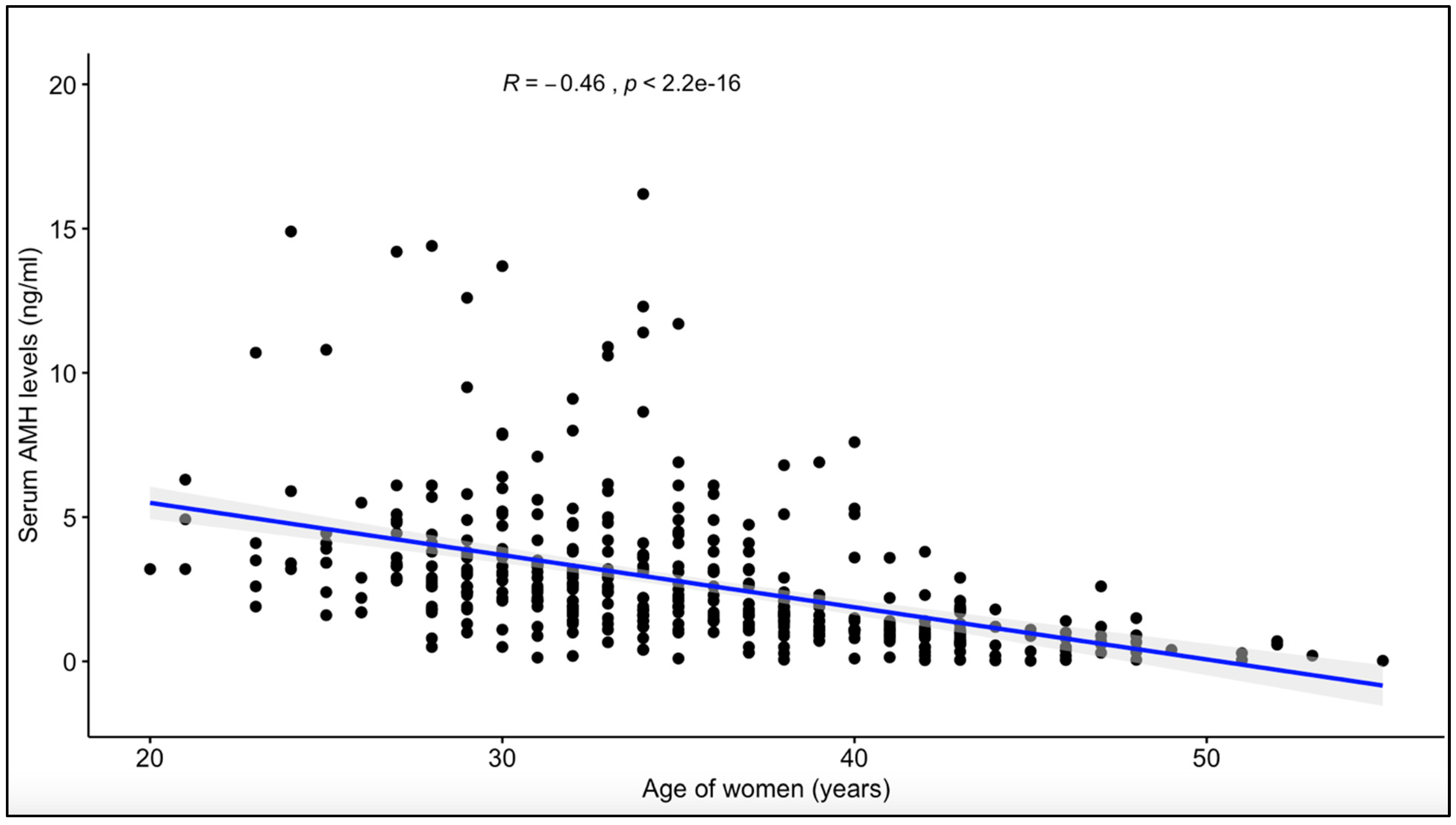
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seifer, D.B.; Golub, E.T.; Lambert-Messerlian, G.; Benning, L.; Anastos, K.; Watts, D.H.; Cohen, M.H.; Karim, R.; Young, M.A.; Minkoff, H.; et al. Variations in serum müllerian inhibiting substance between White, Black, and Hispanic women. Fertil. Steril. 2009, 92, 1674–1678. [Google Scholar] [CrossRef] [PubMed]
- Ebner, T.; Sommergruber, M.; Moser, M.; Shebl, O.; Schreier-Lechner, E.; Tews, G. Basal level of anti-Müllerian hormone is associated with oocyte quality in stimulated cycles. Hum. Reprod. 2006, 21, 2022–2026. [Google Scholar] [CrossRef] [PubMed]
- Broer, S.L.; Dólleman, M.; van Disseldorp, J.; Broeze, K.A.; Opmeer, B.C.; Bossuyt, P.M.M.; Eijkemans, M.J.C.; Mol, B.W.; Broekmans, F.J.M.; IPD-EXPORT Study Group. Prediction of an excessive response in in vitro fertilization from patient characteristics and ovarian reserve tests and comparison in subgroups: An individual patient data meta-analysis. Fertil. Steril. 2013, 100, 420–429. [Google Scholar] [CrossRef]
- Lee, M.M.; Donahoe, P.K.; Hasegawa, T.; Silverman, B.; Crist, G.B.; Best, S.; Hasegawa, Y.; Noto, R.; Schoenfeld, D.; MacLaughlin, D.T. Mullerian inhibiting substance in humans: Normal levels from infancy to adulthood. J. Clin. Endocrinol. Metab. 1996, 81, 571–576. [Google Scholar] [PubMed]
- Kanakatti Shankar, R.; Dowlut-McElroy, T.; Dauber, A.; Gomez-Lobo, V. Clinical utility of Anti-Mullerian Hormone in pediatrics. J. Clin. Endocrinol. Metab. 2022, 107, 309–323. [Google Scholar] [CrossRef]
- Yates, A.P.; Roberts, S.A.; Nardo, L.G. Anti-Müllerian hormone-tailored stimulation protocols improve outcomes whilst reducing adverse effects and costs of IVF. Hum. Reprod. 2012, 27. [Google Scholar] [CrossRef] [PubMed]
- Meczekalski, B.; Czyzyk, A.; Kunicki, M.; Podfigurna-Stopa, A.; Plociennik, L.; Jakiel, G.; Maciejewska-Jeske, M.; Lukaszuk, K. Fertility in women of late reproductive age: The role of serum anti-Müllerian hormone (AMH) levels in its assessment. J. Endocrinol. Investig. 2016, 39, 1259–1265. [Google Scholar] [CrossRef]
- Sills, E.S.; Alper, M.M.; Walsh, A.P. Ovarian reserve screening in infertility: Practical applications and theoretical directions for research. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 146, 30–36. [Google Scholar] [CrossRef]
- Gleicher, N.; Weghofer, A.; Barad, D.H. Defining ovarian reserve to better understand ovarian aging. Reprod. Biol. Endocrinol. 2011, 9, 23. [Google Scholar] [CrossRef]
- Bukulmez, O.; Arici, A. Assessment of ovarian reserve. Curr. Opin. Obstet. Gynecol. 2004, 16, 231–237. [Google Scholar] [CrossRef]
- Hamdine, O.; Eijkemans, M.; Lentjes, E.; Torrance, H.; Macklon, N.; Fauser, B.; Broekmans, F. Ovarian response prediction in GnRH antagonist treatment for IVF using anti-Müllerian hormone. Hum. Reprod. 2015, 30. [Google Scholar] [CrossRef] [PubMed]
- Andersen, A.N.; Witjes, H.; Gordon, K.; Mannaerts, B. Predictive factors of ovarian response and clinical outcome after IVF/ICSI following a rFSH/GnRH antagonist protocol with or without oral contraceptive pre-treatment. Hum. Reprod. 2011, 26, 3413–3423. [Google Scholar] [CrossRef] [PubMed]
- Mawusi, D.; Yakass, M.B.; Abaidoo, C.S.; Addai, F.K. Use of Anti-Mullerian Hormone (AMH) for Testing of Ovarian Reserve: A Survey of Fifteen (15) Fertility Centres in Ghana. Adv. Reprod. Sci. 2021, 9, 9. [Google Scholar] [CrossRef]
- Arce, J.-C.; La Marca, A.; Klein, B.M.; Andersen, A.N.; Fleming, R. Antimüllerian hormone in gonadotropin releasing-hormone antagonist cycles: Prediction of ovarian response and cumulative treatment outcome in good-prognosis patients. Fertil. Steril. 2013, 99, 48. [Google Scholar] [CrossRef] [PubMed]
- Tuck, M.K.; Chan, D.W.; Chia, D.; Godwin, A.K.; Grizzle, W.E.; Krueger, K.E.; Rom, W.; Sanda, M.; Sorbara, L.; Stass, S.; et al. Standard operating procedures for serum and plasma collection: Early detection research network consensus statement standard operating procedure integration working group. J. Proteome Res. 2009, 8, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Gassner, D.; Jung, R. First fully automated immunoassay for anti-Müllerian hormone. Clin. Chem. Lab. Med. (CCLM) 2014, 52, 1143–1152. [Google Scholar] [CrossRef]
- Di Paola, R.; Garzon, S.; Giuliani, S.; Laganà, A.S.; Noventa, M.; Parissone, F.; Zorzi, C.; Raffaelli, R.; Ghezzi, F.; Franchi, M.; et al. Are we choosing the correct FSH starting dose during controlled ovarian stimulation for intrauterine insemination cycles? Potential application of a nomogram based on woman’s age and markers of ovarian reserve. Arch. Gynecol. Obstet. 2018, 298. [Google Scholar] [CrossRef]
- La Marca, A.; Papaleo, E.; Grisendi, V.; Argento, C.; Giulini, S.; Volpe, A. Development of a nomogram based on markers of ovarian reserve for the individualisation of the follicle-stimulating hormone starting dose in in vitro fertilisation cycles. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 1171–1179. [Google Scholar] [CrossRef]
- Nelson, S.M.; Yates, R.W.; Fleming, R. Serum anti-Müllerian hormone and FSH: Prediction of live birth and extremes of response in stimulated cycles—Implications for individualization of therapy. Hum. Reprod. 2007, 22, 204. [Google Scholar] [CrossRef]
- Broer, S.L.; Dólleman, M.; Opmeer, B.C.; Fauser, B.C.; Mol, B.W.; Broekmans, F.J.M. AMH and AFC as predictors of excessive response in controlled ovarian hyperstimulation: A meta-analysis. Hum. Reprod. Update 2011, 17, 34. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Meng, Y.; Jiang, X.; Liu, C.; Zhang, H.; Cui, L.; Chen, Z.-J. IVF outcomes of women with discrepancies between age and serum anti-Müllerian hormone levels. Reprod. Biol. Endocrinol. 2019, 17, 83. [Google Scholar] [CrossRef] [PubMed]
- Papler, T.B.; Bokal, E.V.; Zmrzljak, U.P.; Stimpfel, M.; Laganà, A.S.; Ghezzi, F.; Jančar, N. PGR and PTX3 gene expression in cumulus cells from obese and normal weighting women after administration of long-acting recombinant follicle-stimulating hormone for controlled ovarian stimulation. Arch. Gynecol. Obstet. 2019, 299, 863–871. [Google Scholar] [CrossRef]
- Nelson, S.M.; Yates, R.W.; Lyall, H.; Jamieson, M.; Traynor, I.; Gaudoin, M.; Mitchell, P.; Ambrose, P.; Fleming, R. Anti-Müllerian hormone-based approach to controlled ovarian stimulation for assisted conception. Hum. Reprod. 2009, 24, 867–875. [Google Scholar] [CrossRef] [PubMed]
- Rustamov, O.; Smith, A.; Roberts, S.A.; Yates, A.P.; Fitzgerald, C.; Krishnan, M.; Nardo, L.G.; Pemberton, P.W. The measurement of anti-Mullerian hormone: A critical appraisal. J. Clin. Endocrinol. Metab. 2014, 99, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Smeenk, J.M.J.; Sweep, F.C.G.J.; Zielhuis, G.A.; Kremer, J.M.; Thomas, C.M.G.; Braat, D.D.M. Antimüllerian hormone predicts ovarian responsiveness, but not embryo quality or pregnancy, after in vitro fertilization or intracytoplasmic sperm injection. Fertil. Steril. 2007, 87, 223–226. [Google Scholar] [CrossRef]
- Fong, S.L.; Baart, E.B.; Martini, E.; Schipper, I.; Visser, J.A.; Themmen, A.P.N.; de Jong, F.H.; Fauser, B.J.C.M.; Laven, J.S.E. Anti-Müllerian hormone: A marker for oocyte quantity, oocyte quality and embryo quality? Reprod. Biomed. Online 2008, 16, 664–670. [Google Scholar] [CrossRef]
- Tal, R.; Tal, O.; Seifer, B.J.; Seifer, D.B. Antimüllerian hormone as predictor of implantation and clinical pregnancy after assisted conception: A systematic review and meta-analysis. Fertil. Steril. 2015, 103, 119–130. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
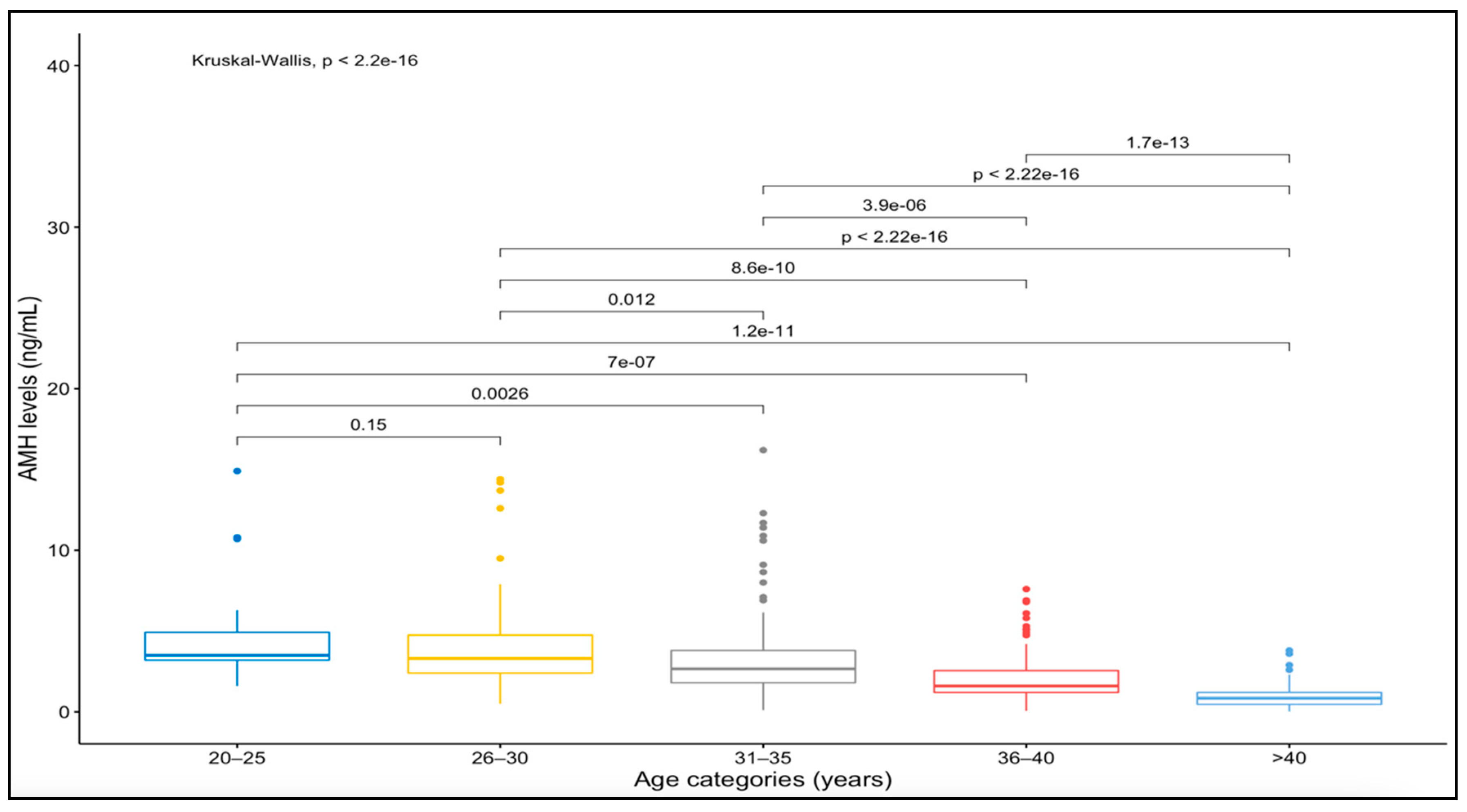
| Age Groups | N = 411; n (%) | Median AMH (IQR) | Mean AMH ± SD | 95% CI |
|---|---|---|---|---|
| 20–25 | 21 (5.1) | 3.5 (1.72) | 4.85 ± 3.34 | 3.33–6.37 |
| 26–30 | 79 (19.2) | 3.3 (2.35) | 3.98 ± 2.83 | 3.34–4.61 |
| 31–35 | 125 (30.4) | 2.7 (2.00) | 3.32 ± 2.63 | 2.86–2.26 |
| 36–40 | 98 (23.8) | 1.6 (1.35) | 2.15 ± 1.54 | 1.85–2.46 |
| >40 | 88 (21.4) | 0.85 (0.74) | 0.94 ± 0.73 | 0.78 –1.09 |
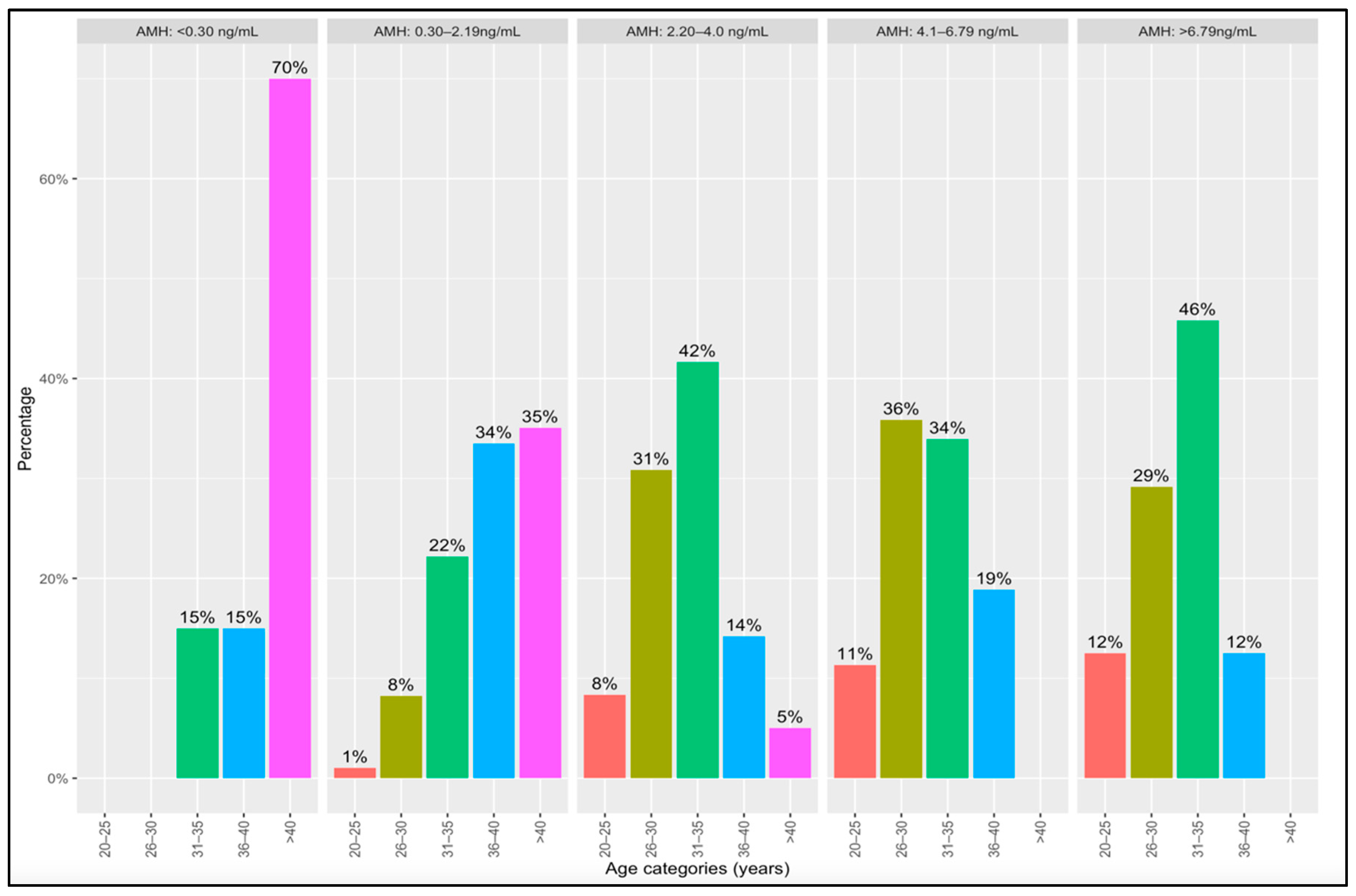
| AMH Categories | |||||
|---|---|---|---|---|---|
| Age Group in Years | (<0.30 ng/mL)n (%) | (0.30–2.19 ng/mL) n (%) | (2.20–4.0 ng/mL) n (%) | (4.1–6.79 ng/mL) n (%) | >6.79 ng/mL n (%) |
| 1 (20–25) | 0 | 2 (1.0) | 10 (8.3) | 6 (11.3) | 3 (12.5) |
| 2 (26–30) | 0 | 16 (8.3) | 37 (30.8) | 19 (35.8) | 7 (29.2) |
| 3 (31–35) | 3 (15.0) | 43 (22.2) | 50 (41.7) | 18 (34.0) | 11 (45.8) |
| 4 (36–40) | 3 (15.0) | 65 (33.5) | 17 (14.2) | 10 (18.9) | 3 (12.5) |
| 5 (>40) | 14 (70.0) | 68 (35.1) | 6 (5.0) | 0 | 0 |
| Total | 20 (100) | 194 (100) | 120 (100) | 53 (100) | 24 (100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mawusi, D.; Adu-Bonsaffoh, K.; Abaidoo, C.S.; Addai, F.K. Variation in Anti-Mullerian Hormone Levels with Age in Women Accessing In Vitro Fertilization Services in Ghana. Reprod. Med. 2022, 3, 253-262. https://doi.org/10.3390/reprodmed3030020
Mawusi D, Adu-Bonsaffoh K, Abaidoo CS, Addai FK. Variation in Anti-Mullerian Hormone Levels with Age in Women Accessing In Vitro Fertilization Services in Ghana. Reproductive Medicine. 2022; 3(3):253-262. https://doi.org/10.3390/reprodmed3030020
Chicago/Turabian StyleMawusi, Dickson, Kwame Adu-Bonsaffoh, Chrissie Stansie Abaidoo, and Frederick Kwaku Addai. 2022. "Variation in Anti-Mullerian Hormone Levels with Age in Women Accessing In Vitro Fertilization Services in Ghana" Reproductive Medicine 3, no. 3: 253-262. https://doi.org/10.3390/reprodmed3030020