
Premature Cardiovascular Misdiagnosis of Senior Endurance-Trained Athletes
Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC V6T 1Z3, Canada
Hearts 2023, 4(1), 28-37; https://doi.org/10.3390/hearts4010004
Submission received: 15 November 2022
/
Revised: 6 March 2023
/
Accepted: 7 March 2023
/
Published: 15 March 2023
Abstract
:A mature Caucasian patient, an endurance-trained triathlete (age group), had a routine ECG. The patient was immediately referred to Emergency based on supposed ECG abnormalities indicating a heart attack. This diagnosis was quickly dismissed based on no symptoms, heart rate of 50 BPM, athletic status, excellent health, and no prior cardiovascular problems. The patient had a history of severe white coat hypertension and underwent a further stress test and echocardiogram. The stress test showed exaggerated systolic blood pressures (over 225 mmHg) and high in-clinic basal blood pressures (160/90 mmHg), and the patient was diagnosed as hypertensive with exercise blood pressure close to stroke territory. He was told to stop racing, reduce training, and was prescribed antihypertensive drugs (which he did not take). Subsequent at-home 24 h (values close to 120/80 mmHg) and stress blood pressure measurements reversed that decision when considered in combination with an excellent echocardiogram result. The literature clearly describes endurance-trained athletes with systolic pressures over 225 mmHg Hg as being conditioned with no pathological aspects. Endurance-trained athletes should be examined as special cases in the field of cardiovascular medicine as trained physiological responses often present as cardiac abnormalities, and misdiagnosis can inappropriately change the athlete’s life.
1. Introduction
The concept of an “athlete’s heart” with training-induced remodeling is well known, but the concept of an “athlete’s vasculature” and blood pressure aspects is less well known [1,2]. Possible heart changes in elite athletes are usually first encountered in apparently abnormal ECG recordings, with approximately half of older endurance athletes with no coronary pathology having abnormal ECGs [1]. These abnormalities include ST-T abnormalities and isolated high voltage values (indicative of left ventricular hypertrophy), which might indicate a danger of a heart attack. This overlap between pathological and endurance athlete-modified changes is well documented, but at first sight, it is very worrying and requires immediate further examination. The objective of this paper was to explore a diagnosis of cardiovascular disease in an endurance-trained athlete, which was later reversed based on well-established literature reports of the non-pathological nature of the symptoms, supported by blood pressure and heart data. The patient presented as a late 60′s man with no cardiac symptoms who was sent for an ECG screen prior to an abdominal operation. He had a history of extreme white coat syndrome with in-clinic blood pressure readings close to 160/90 (systolic-mmHg/diastolic-mmHg) as compared to at-home, with calm readings of 120/80. The patient was a long-term endurance athlete of 45 years who still trained daily at heart rates of 140–150 BPM, vegetarian, 173 cm and 64 kg, still competing at the world level (age group) in triathlons with a basal heart rate around 50 BPM. The patient was in excellent health with no history of any cardiovascular abnormalities.
2. Cardiovascular Results
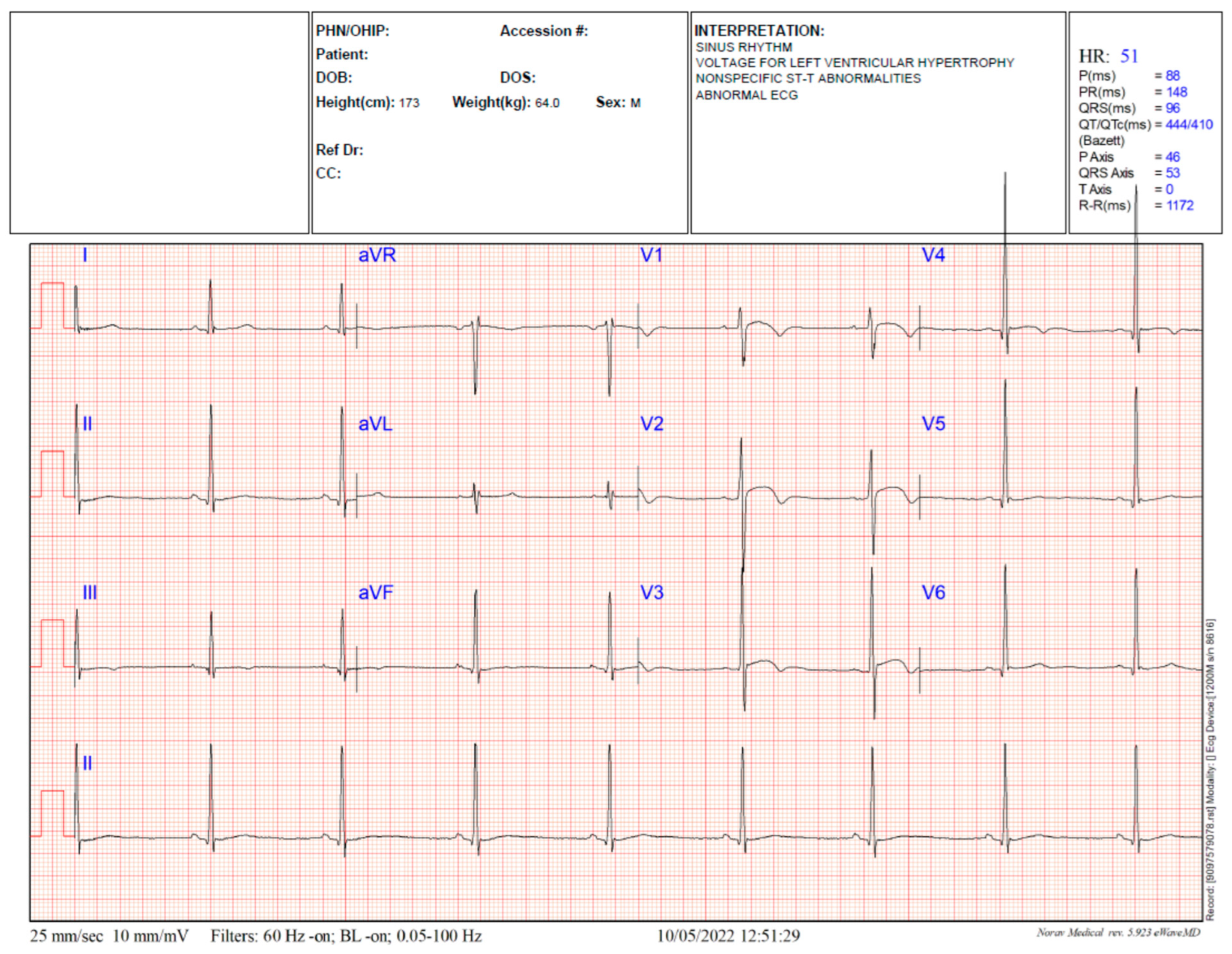
After the first ECG, the patient was immediately referred to the hospital emergency department as the diagnosis was a very abnormal ECG with the potential for a current or previous heart attack based on non-specific ST-T abnormalities (Figure 1). The patient had no current or previous record of any symptoms of a heart attack. At the emergency department, blood pressure was high, but all blood work was normal, including low troponin levels. Based on the patient’s excellent health and extended endurance training profile, a cardiologist’s observation on a repeated ECG declared the ST-T abnormality to be not significant, but the elevated blood pressure and high QRS voltages (potential left ventricular hypertrophy) warranted a full cardiology work up. The patient was discharged and allowed reasonable exercise.
2.1. Stress Test Investigation
The patient underwent a standard treadmill stress test. However, the starting blood pressure of 160/90 mmHg prevented the test until the patient rested long enough to bring the systolic pressure down closer to 150 mmHg. The patient easily held a running heart rate of 140 BPM, and ECGs were recorded. The technician got close to stopping the test as the systolic blood pressure initially rose to values of about 225 mmHg as the heart rate increased to 140 BPM before stabilizing a little lower.
2.2. Cardiologist Second Diagnosis
The cardiologist was alarmed at the basal high blood pressure in the clinic of approx. 160/90 mmHg. The patient showed the doctor his own at-home readings for the previous 10 years, which all showed average values close to 120/80 mmHg with a sub 50 BPM heart rate with the proviso that at home, it took 20 min and perhaps four readings for the pressure to stabilize from approximately 150/88 mmHg to the normal level. After repeated measurements in the clinic, the pressure was reduced only slightly. It was suggested that the at-home device might be flawed. The cardiologist warned the athlete that stress test systolic blood pressures of 225 mmHg were alarming as they were close to stroke territory. In addition, he declared the patient hypertensive and prescribed the ACE inhibitor Perindopril which the patient did not take. The patient was cautioned against fitness training and advised to withdraw from two upcoming races, which was advice he followed. He was told to have a holster 24 h blood pressure monitor fitted and to have a repeat appointment in a few months when the drug might have worked.
2.3. Further Investigation
The patient was a medical research scientist and decided to self-investigate further. The patient bought a new expensive home blood pressure device (Bios) to complement and test (side by side) against his previous device (Omron). He measured his blood pressure at various times over 24 h using both blood pressure devices to compare. The patient set up a bicycle training wheel where he performed repeated stress tests of sustained heart rate vs. blood pressure using both blood pressure devices.
2.4. The 24 h Blood Pressure Measurements
These tests were performed during a normal at-home day with the patient relaxing for five minutes in an easy chair prior to measurements with the second of the two repeat measurements reported. The study was repeated on two separate days and reported in the data in Figure 2 and Figure 3. The first study started at 9 a.m. (Figure 2) and showed that the two devices showed very similar results over most of the 24 h period. Diastolic blood pressures were all generally well below 90 mmHg and mostly at or below 80 mmHg. The heart rates were consistently below 60 BPM and often sub-50 BPM. Systolic pressures were more variable. They started at 150 mmHg (reflective of measurement anxiety) at 9 a.m. but rapidly dropped to 120 mmHg at the one-hour time point. The patient went for a five-mile run at noon (3 h) and measured blood pressure ten minutes after finishing, giving a slightly elevated systolic pressure of 145 mmHg. This systolic pressure quickly returned to 120–130 mmHg levels over the next few hours. Values taken in the 7 to 11 h time period reflected the patient’s involvement in household activities and were slightly elevated, with systolic values close to 130 mmHg. The measurements taken at 16, 19, and 22 h are those taken in sleep mode (waking to take measurements on one device only).
The second 18 h test (Figure 3) commenced at 3 a.m. and reported blood pressures of approximately 120/75 mmHg with a heart rate of 45 BPM for the next four readings. At five hours, the patient performed a very fast 30 min bike ride holding approx. 140 BPM and then proceeded with normal household duties (cleaning gardening, etc.) for the rest of the day. The heart rate values were approximately 50 BPM and diastolic pressures close to 80 mmHg. Systolic pressures were close to 130 mmHg over the 7–18 h period. Both blood pressure devices gave similar readings.
2.5. General Day Time Activity Measurement
The patient interrupted his daily activities and sat down for a minute before taking the blood pressure measurements. Results are shown in Table 1. Both the BIOS and OMRON devices showed approximately similar values remembering that these were single measurements taken close to stopping exercise, so they were likely to show variation. For all activities, the systolic values were elevated to approximately 140 mmHg and diastolic were normal at approximately 80 mmHg.
2.6. Stress Test
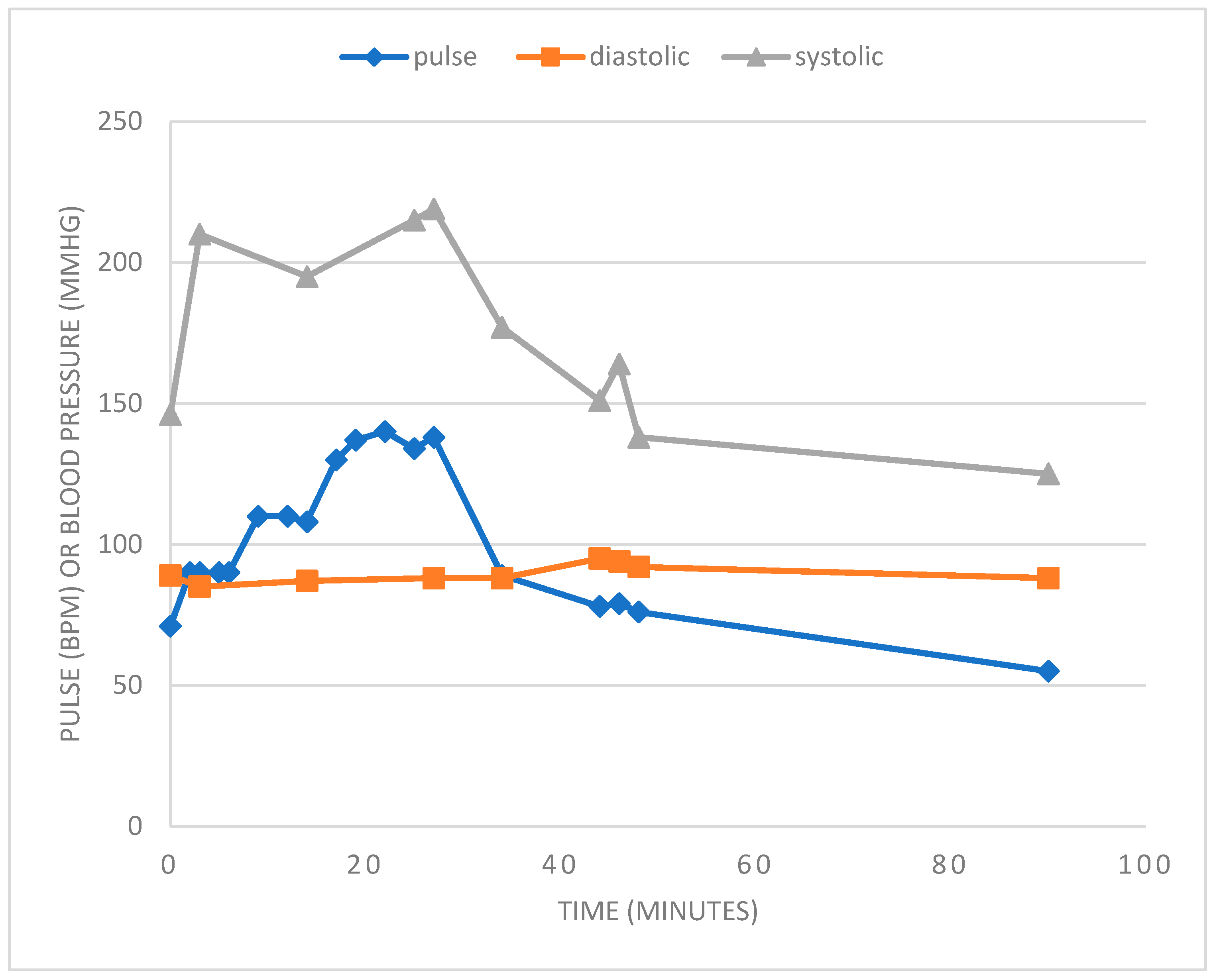
At the start (idle cycling), the pulse (71 BPM) and systolic pressure (146 mmHg) were elevated, as shown in Figure 4. Upon increasing the cycle rate to give a pulse of approximately 90 BPM for five minutes, the systolic pressure increased rapidly to 210 mmHg. On increasing the pulse to 110 BPM for six minutes and then to 140 BPM for 15 min, there was only a minor increase in systolic pressure to 215 mmHg. The cycling rate then slowly reduced over the next ten minutes, followed by idling speed for a short while. This stress test at peak BPM was only repeated on further days. Using 5–10 min of sustained cycling at 140 BPM peak, systolic values of 235 mmHg or 223 mmHg were recorded with diastolic values of 93 mmHg and 93 mmHg.
2.7. Echocardiogram
The echocardiogram showed normal heart function with no significant left ventricular hypertrophy, and the ventricle wall thickness in mm was right on the high end of the normal range. Both atria were reported as enlarged as expected, and there were no observed pathological aspects. A detailed report is included in Supplementary information. The information may be summarized as: Summary and Conclusions: 1. Normal LV size with normal LV systolic function. Visual LVEF estimated at 60%. 2. No LV regional wall motion abnormalities. 3. Normal LV wall thickness and mass. 4. Indeterminate LV diastolic function. Indeterminate LV filling pressure. 5. Normal size RV by linear dimension. Normal RV systolic function. 6. Severe biatrial enlargement. 7. No significant valve disease. 8. Normal PASP: 33 mmHg. Comparison to Previous Exam: No previous transthoracic echocardiogram for comparison.
2.8. Cardiologist Follow Up Appointment
The cardiologist was happy with the echocardiogram and the 24 h dual device blood pressure determinations, and he reversed his hypertensive diagnosis with no need for drugs at that time. He was still very concerned about the systolic pressures around 225 mmHg in the stress test, and he mentioned that being stroke territory, reiterating that concern from the first appointment. The patient showed the cardiologist some literature references showing elite endurance athletes having similar blood pressures at similar heart rates, with the context being that such pressures are not pathological in such people but probably trained responses. The cardiologist acknowledged the point and cleared the patient for the resumption of training and racing with the proviso that he made a third appointment with a specialist sports cardiologist for a second opinion. The patient resumed normal activity.
2.9. Sports Cardiologist Appointment
The cardiologist examined the various data on 24 h monitoring, general day activity measurements, and stress test results, and his first impression was that the patient was at least prehypertensive with general activity day measurements close to 140/80. He noted that some of the 24 h measurements were approximately 130 mmHg for systolic. Like the first cardiologist, he was immediately alarmed that the stress test showed values as high as 235 mmHg and mentioned the dangers of stroke. The patient then showed the cardiologist the literature on elite endurance athletes and values of this sort being considered non-dangerous and a product of training. Indeed, the patient pointed out that in 2018, the European Society of Cardiology had declared that there was no consensus on normal blood pressure responses during exercise and that the old panic limit of 250 mmHg (systolic) was redundant and transient levels over 250 mmHg were expected and permissible. The cardiologist commented that the blood pressure aspect of heart function in elite athletes was not something he came across often and agreed that pressures close to 370/280 mmHg were common in people doing heavy weights. The cardiologist also noted the continuous normal lipid profile in the patient over many years. The cardiologist agreed that the patient was cleared to continue training and racing with caution.
2.10. Current Conditions
The patient has recognized his age and the extended years of endurance training, and perhaps the need to back off extreme training. He resumed 95% effort training and completed one triathlon race coming in the top 25% overall, despite keeping his foot off the gas. He is unsure about continuing high-level racing despite his clean bill of cardiac health.
3. Discussion
The first point of contact of endurance athletes with cardiovascular clinicians usually arises from routine requests for an ECG test. However, since these athletes have had years of extreme heart pumping and blood pressure changes to force blood around the body at high rates, it seems likely that their ECGs might be different from normal people. For this patient, the first ECG resulted in an immediate transfer to an Emergency Department of a hospital as he was deemed to likely be in the process of having a heart attack. However, with an extended history of endurance training and with a sub-50 BPM basal heart rate, a subsequent ECG and overall blood profile analysis removed any worry of immediate risk. In light of the athletic status of the patient, this level of warning was perhaps excessive and could easily unnecessarily panic a different patient.
Similarly, the stress test work was associated with undue clinical panic based on large elevations in systolic blood pressure throughout the test and the in-clinic basal blood pressure measurements. The term “stoke territory” was used twice in relation to stress test systolic pressure recordings over 225 mmHg.
The patient has a long history of unverified white coat hypertension (WCH) as witnessed by his own at-home measurements (approximately 120/80 mmHg) and the in-clinic determinations over the years, which were usually closer to 150/88 mmHg or more recently closer to 160/90 mmHg. Whilst it is well established that a large percentage of the population has WCH, this is usually considered to be of the order of 10 mmHg elevations on the systolic side. However, in a study with over 2000 patients, Manios et al. [3] found that 564 patients (average age 51 and heart rate 78) had WCH with at-home mean readings of 124/76 mmHg but in clinic values of 144 (+/−14)/92 mm/Hg. Furthermore, Dolan et al. [4] studied 5616 patients and found that one-third had WCH with at-home values of 146/89 mmHg and in-clinic values of 162 (+/−28)/93 mmHg. Whilst these studies showed elevation of systolic pressure of the order of 16–20 units, it should be noted that the errors on the mean values are very large, capturing much higher values in some cases. In one extreme case of WHC, Nyvad et al. [5] reported a woman with WCH whose systolic pressure would jump to values well above 200 mmHg under in-clinic testing or during 24 h monitoring but would drop to 100 mmHg with deep breathing or being told the test was ending. Together these data point to the possibility of clinically irrelevant larger levels of systolic blood pressure increases in WCH patients than commonly quoted.
Most of the studies reporting exercise blood pressures during stress tests in the non-athletic population have investigated or commented on the correlation between an exaggerated blood pressure response in a stress test with the development of later life hypertension and risks of cardiovascular pathologies like strokes or heart attacks [6,7,8,9]. Using similar stress tests, maximal systolic pressures of 231 mmHg [6], 194 mmHg [7], 205 mmHg [8], and 190 mmHg [9] were reported with mean ages in each group of 65, 43, 53, and 28–79 years, respectively. Diastolic pressures do not usually increase much in stress tests, and increases above 10 mmHg at any point may cause some to terminate the test [7,10]. Kurl et al. [8] showed a graph demonstrating an almost linear increase in mean systolic blood pressure as a function of workload up to the 205 mmHg maximum but with the observation that standard deviations at all points are greater than 20 units demonstrating the large variation in values.
It is well known that endurance athletes provide higher systolic blood pressures in stress tests as compared to non-athletes. Moreover, in the excellent review paper on systolic blood pressure in endurance athletes, Richard et al. [11] commented that in 2018, the European Society for Sports Medicine stated that there was no consensus on normal blood pressure responses during exercise. Furthermore, the American College of Sports Medicine stated that the 250 mmHg (systolic) limit for terminating stress tests was arbitrary and that no cardiovascular events had been reported. Baggish et al. [12] felt that SBPs of greater than 250 mmHg were expected and permissible without any pathological aspect. Richard [11] commented that SBP values of greater than 240 mmHg could be possible and that exaggerated blood pressure responses in stress tests were seen in some fit athletes with no associated pathological aspect. Furthermore, it was concluded that elevated SBP in endurance athletes probably arises from an adaptive response to training rather than having a pathological cause or outcome.
These literature observations and data on exaggerated blood pressure responses in stress tests question whether those observed in the patient in this study have any pathological aspect at all, especially as he is older with expected higher readings and has no heart remodeling or cardiovascular morbidities as witnessed by a good echocardiogram.
Generally, the relationship between elevated blood pressure and disease has been simplified down to the concept that chronic high blood pressure increases the chance of stroke, heart attack, or other problems such as renal disease [13]. The variables associated with developing disease include age, health (especially lipid health), athleticism, and background blood pressure condition (normo-, pre- or hyper-tensive). The “normal” values for blood pressure have dropped over the years to approximately 120/80 mmHg. The general public views the circulating blood system as similar to a household hot water heating system that pumps (heart) water around a series of pipes (blood vessels) and returns to the pump. There is a fear that the pump might stop (heart attack) or the pressure might get too high and rupture a pipe (similar to a stroke). Because pre- or full-hypertension is now diagnosed as systolic values over 130 mmHg or 140 mmHg, there is a general fear that values over 140 mmHg are immediately dangerous and, for example, severe preeclamptic values of 160/110 mmHg are considered highly dangerous.
In fact, the critical word in hypertension circles is “chronic”. Over shorter durations, blood pressure can increase considerably without incidence, and this is quite normal as the body needs to be able to frequently increase blood supply to tissues, especially during exercise, and does this by increasing the heart rate and increasing the blood pressure to push the blood quickly through the distant capillaries. For example, weight lifters doing double leg press record mean values of 320/250 mmHg, with one person recording 480/350 mmHg [14]. When one sees these extremely high values without heart attacks or strokes in the gym, then one realizes the robust nature of the heart and blood vessels. However, without such a knowledge of activity-related blood pressure increases, any patient warned that elevated blood pressure in a stress test is associated with an increased risk of stroke would incorrectly imagine the blood vessels rupturing under strain at 225 mmHg of pressure. Instead, the only relationship with stroke in the athlete might be the indication of a longer-term problem with developing hypertension with a subsequent increased risk of stroke. Clearly, these are quite different perspectives of immediate (deadly) or long-term (manageable) pathologies.
Interestingly, the ST dome and small T-wave inversions observed in the ECG (Figure 1), which prompted emergency diagnosis, have been previously observed in athletes. Uberoi A. et al. [15] reported that up to 50% of (younger) athletes had abnormal ECGs with ST elevation. Furthermore, T-wave inversion was common in many of those athletes, especially black athletes and perhaps 3% of Caucasian athletes. Little is known on this matter for older athletes. For this particular athlete, any immediate risk of ischemia and left ventricular hypertrophy (adaptive or pathological) was ruled out from the echocardiogram results. The lack of left ventricular hypertrophy despite long-term high-intensity training also argues to some degree against any diagnosis of true hypertension. Wilson M. et al. [16] explored T-wave inversion and gave the recommendation that for asymptomatic athletes with T-wave inversion but a normal detailed cardiac evaluation and no family history of hereditary heart disease, the athlete should be allowed unrestricted athletic competition and annual cardiac evaluation.
The literature on cardiac abnormalities in endurance athletes largely covers younger athletes. These athletes can be monitored in future years to obtain conclusions about pathological outcomes. Obviously, it is much harder to generate meaningful long-term data from older athletes. Therefore, a more balanced diagnostic protocol might be to take guidance from the data on younger athletes (ECG abnormalities, stress test-related elevations in blood pressure) in combination with general health and echocardiogram analysis of heart pathologies like hypertrophy. Such an approach seems particularly relevant now where, after 40 years of marathon and triathlon popularity, an increasing number of elderly athletes are likely to present at cardiac centers. One might argue that since no apparent damage had been made to the athlete’s heart from 45 years of endurance training, the observed abnormalities might reflect the non-pathological ones often observed in younger athletes.
Generally, exercise is good for cardiovascular health and is now strongly encouraged by governments. Clearly, then, the transient increased heart rate and blood pressure during exercise have no detrimental effect on health but rather the reverse. Traditionally, “common sense” wisdom would argue this was true but within reason. However, the reason part was not science-based. Common sense with no scientific base prevented women from competing in the Olympics at distances greater than 800 m until 1972 based on the idea that they would find the exercise too strenuous. Presumably, training for and completing a long race marathon, which involves holding a high heart rate and blood pressure for many hours, would be well outside the boundaries of “good reason”, yet the incidence of cardiac arrest during or after a race is approximately 0.5 per 100,000 runners as compared to 3 per 100,000 in a day for the general public of the USA. One wonders if older endurance-trained athletes should carry a footnote on their medical records alerting physicians to the possibility of “special” cardiovascular status to avoid panicked or premature misdiagnosis.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/hearts4010004/s1, File S1: A detailed report of echocardiogram.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived as not required by case reports.
Informed Consent Statement
Informed consent was obtained from the subject in the study. The author is the subject patient described in the paper.
Data Availability Statement
Data are available at the University of British Columbia.
Conflicts of Interest
The author declares no conflict of interest.
References
- George, K.; Whyte, G.; Green, D.; Oxborough, D.; Shave, R.; Gaze, D.; Somauroo, J. The endurance athletes heart: Acute stress and chronic adaptation. Br. J. Sports Med. 2012, 46 (Suppl. 1), 29–36. [Google Scholar] [CrossRef] [PubMed]
- Green, D.J.; Spence, A.; Rowley, N.; Thijssen, D.H.J.; Naylor, L.H. Vascular adaptation in athletes: Is there an ‘athlete’s artery’? Exp. Physiol. 2012, 97, 295–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manios, E.D.; Koroboki, E.A.; Tsivgoulis, G.K.; Spengos, K.M.; Spiliopoulou, I.K.; Brodie, F.G.; Vemmos, K.N.; Zakopoulos, N.A. Factors influencing white-coat effect. Am. J. Hypertens. 2008, 21, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolan, E.; Stanton, A.; Atkins, N.; Den Hond, E.; Thijs, L.; McCormack, P.; Staessen, J.; O’Brien, E. Determinants of white-coat hypertension. Blood Press. Monit. 2004, 9, 307–309. [Google Scholar] [CrossRef] [PubMed]
- Nyvad, J.; Reinhard, M.; Christensen, K.L. A case of an extreme white coat effect. Blood Press. 2020, 29, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Stewart, K.J.; Sung, J.; Silber, H.A.; Fleg, J.L.; Kelemen, M.D.; Turner, K.L.; Bacher, A.C.; Dobrosielski, D.A.; DeRegis, J.R.; Shapiro, E.P.; et al. Exaggerated exercise blood pressure is related to impaired endothelial vasodilator function. Am. J. Hypertens. 2004, 17, 314–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyai, N.; Arita, M.; Miyashita, K.; Morioka, I.; Shiraishi, T.; Nishio, I. Blood pressure response to heart rate during exercise test and risk of future hypertension. Hypertension 2002, 39, 761–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurl, S.; Laukkanen, J.A.; Rauramaa, R.; Lakka, T.A.; Sivenius, J.; Salonen, J.T. Systolic blood pressure response to exercise stress test and risk of stroke. Stroke 2001, 32, 2036–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaney, R.H.; Eyman, R.K. Blood pressure at rest and during maximal dynamic and isometric exercise as predictors of systemic hypertension. Am. J. Cardiol. 1988, 62, 1058–1061. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.; Pate, R.; Jackson, K.; Ward, D.; Macera, C.; Kohl, H.; Blair, S. Exaggerated blood pressure response to dynamic exercise and risk of future hypertension. J. Clin. Epidemiol. 1998, 51, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Richard, N.A.; Hodges, L.; Koehle, M.S. Elevated peak systolic blood pressure in endurance-trained athletes: Physiology or pathology? Scand. J. Med. Sci. Sports 2021, 31, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Baggish, A.L.; Battle, R.W.; Beckerman, J.G.; Bove, A.A.; Lampert, R.J.; Levine, B.D.; Link, M.S.; Martinez, M.W.; Molossi, S.M.; Salerno, J.; et al. Sports Cardiology: Core Curriculum for Providing Cardiovascular Care to Competitive Athletes and Highly Active People. J. Am. Coll. Cardiol. 2017, 70, 1902–1918. [Google Scholar] [CrossRef] [PubMed]
- Foëx, P.; Sear, J.W. Hypertension: Pathophysiology and treatment. Contin. Educ. Anaesth. Crit. Care Pain 2004, 4, 71–75. [Google Scholar] [CrossRef]
- MacDougall, J.D.; Tuxen, D.; Sale, D.G.; Moroz, J.R.; Sutton, J.R. Arterial blood pressure response to heavy resistance exercise. J. Appl. Physiol. 1985, 58, 785–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uberoi, A.; Stein, R.; Perez, M.V.; Freeman, J.; Wheeler, M.; Dewey, F.; Peidro, R.; Hadley, D.; Drezner, J.; Sharma, S.; et al. Interpretation of the electrocardiogram of young athletes. Circulation 2011, 124, 746–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, M.G.; Sharma, S.; Carré, F.; Charron, P.; Richard, P.; O’Hanlon, R.; Prasad, S.K.; Heidbuchel, H.; Brugada, J.; Salah, O.; et al. Significance of deep T-wave inversions in asymptomatic athletes with normal cardiovascular examinations: Practical solutions for managing the diagnostic conundrum. Br. J. Sports Med. 2012, 46 (Suppl. 1), i51–i58. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
ECG of patient. Abnormalities interpreted as: Sinus Rhythm, voltage for left ventricular hypertrophy, non-specific ST-T abnormalities. Abnormal ECG.
Figure 1.
ECG of patient. Abnormalities interpreted as: Sinus Rhythm, voltage for left ventricular hypertrophy, non-specific ST-T abnormalities. Abnormal ECG.

Figure 2.
Twenty-four-hour blood pressure measurements beginning at 9 am using two different devices (Bios and Omron).
Figure 2.
Twenty-four-hour blood pressure measurements beginning at 9 am using two different devices (Bios and Omron).

Figure 3.
Night and daytime blood pressure measurements beginning at 3 am using two different devices (Bios and Omron).
Figure 3.
Night and daytime blood pressure measurements beginning at 3 am using two different devices (Bios and Omron).

Figure 4.
Blood pressure and heart rate determinations of bicycle trainer stress test.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Blood pressure (mmHg) and pulse measurements (BPM) taken at interrupted times during daily activities using both the Omron and Bios devices. Patient stopped doing the task and sat down for 30 s prior to measurements.
Table 1.
Blood pressure (mmHg) and pulse measurements (BPM) taken at interrupted times during daily activities using both the Omron and Bios devices. Patient stopped doing the task and sat down for 30 s prior to measurements.
| Activity | Omron Systolic | Omron Diastolic | Omron Pulse | Bios Systolic | Bios Diastolic | Bios Pulse |
|---|---|---|---|---|---|---|
| housework | 139 | 84 | 60 | 139 | 89 | 59 |
| housework | 137 | 82 | 58 | 135 | 77 | 61 |
| gardening | 144 | 80 | 47 | 137 | 78 | 46 |
| housework | 136 | 84 | 50 | 136 | 74 | 48 |
| gardening | 149 | 87 | 46 | 145 | 81 | 66 |
| power spraying | 140 | 85 | 57 | 149 | 75 | 58 |
| heavy caffeine | 144 | 89 | 59 | 141 | 79 | 57 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Jackson, J.K. Premature Cardiovascular Misdiagnosis of Senior Endurance-Trained Athletes. Hearts 2023, 4, 28-37. https://doi.org/10.3390/hearts4010004
AMA Style
Jackson JK. Premature Cardiovascular Misdiagnosis of Senior Endurance-Trained Athletes. Hearts. 2023; 4(1):28-37. https://doi.org/10.3390/hearts4010004
Chicago/Turabian StyleJackson, John K. 2023. "Premature Cardiovascular Misdiagnosis of Senior Endurance-Trained Athletes" Hearts 4, no. 1: 28-37. https://doi.org/10.3390/hearts4010004