
Effects of the Traditional Mediterranean Diet in Childhood Recurrent Acute Rhinosinusitis


1
Pediatrician at the Child and Adolescent Clinic “La Palma”, C/Palma 17, bajo A, 13001 Ciudad Real, Spain
2
Nutritionist at the Child and Adolescent Clinic “La Palma”, C/Palma 17, bajo A, 13001 Ciudad Real, Spain
3
Nurse and Nutritionist at the Child and Adolescent Clinic “La Palma”, C/Palma 17, bajo A, 13001 Ciudad Real, Spain
*
Author to whom correspondence should be addressed.
Sinusitis 2021, 5(2), 101-115; https://doi.org/10.3390/sinusitis5020011
Submission received: 29 July 2021
/
Revised: 20 August 2021
/
Accepted: 26 August 2021
/
Published: 2 September 2021
(This article belongs to the Special Issue Allergic Rhinosinusitis and Airway Diseases)
Abstract
:Introduction: There are more and more studies that demonstrate the anti-inflammatory effects of the traditional Mediterranean diet (TMD). The aim of the study was to assess the effects of an intervention with the TMD in patients with recurrent acute and chronic rhinosinusitis. Material and Methods: We performed a pretest–posttest comparison study in 114 patients (56 girls and 58 boys) aged one to five years who had three or more acute rhinosinusitis episodes in the period of 1 year. They were included for a year in the nutritional program “Learning to eat from the Mediterranean”. The anthropometric, clinical, and therapeutic characteristics were studied. Results: All the studied indicators showed a positive and statistically significant evolution. Of the patients, 53.5% did not have any episode of acute rhinosinusitis, and 26.3% had only one, compared to the 3.37 they had on average in the previous year. The use of antibiotics decreased by 87.6%. The degree of satisfaction of the families was very high. The Mediterranean Diet Quality Index (KIDMED) that assesses the quality of the TMD rose from 7.7 to 11 points. Conclusions: The adoption of the TMD could have promising effects in the prevention and treatment of recurrent acute and chronic rhinosinusitis, limiting the pharmacological and surgical intervention in many of these patients.
1. Introduction
At the beginning of the school year and with the arrival of winter, young children are prone to illness from upper respiratory tract infections (URTI), which can range between six and eight episodes a year. Most of these colds tend to resolve spontaneously within a week or two. However, 5–10% of patients develop bacterial complications, including acute rhinosinusitis (ARS) and acute otitis media (AOM). It is estimated that between 6% and 13% of children will have had an episode of ARS by three years of age [1,2]. Although it is usually a self-limited disease, it becomes one of the most frequent causes of antibiotic prescription in childhood, behind otitis and tonsillitis [3,4]. ARS is mainly characterized by the excessive prolongation of the symptoms of the common cold beyond 10 days, with difficulty in nasal breathing, mucopurulent discharge, persistent cough predominantly at night, difficulty in falling asleep, loss of appetite, and sometimes vomiting of phlegm [5]. Often there is a spontaneous improvement after conservative treatment with hypertonic saline sprays or irrigations [6]. When the general condition is more affected, or in young children, it may be necessary to use antibiotics [7]. Some patients lengthen the usual colds over and over again, causing recurrent ARS (RARS), which do not usually cause fever, and thus predisposes some parents not to come to the consultation and ends up turning into chronic rhinosinusitis (CRS). They are patients who have persistent green mucus, significant nasal obstruction, difficulty falling asleep and a persistent cough, although with little effect on the general condition. This persistent inflammatory state contributes to the enlargement of the local lymphatic tissue, such as the palatine tonsils and the adenoids, leading to a space conflict [8]. They often present with worsening clinical attacks or other complications, such as recurrent acute otitis media (RAOM), otitis media with effusion (OME), persistent nasal obstruction (PNO) and recurrent wheezing or childhood asthma (SR) [9,10]. The diagnosis of ARS is not straightforward and can be considered as a clinical challenge, as it is generally performed on subtle clinical grounds, with the absence of specific tests. It is difficult to distinguish when a viral process has become bacterial [11]. Routine imaging is not recommended precisely because of its lack of specificity [12,13,14]. Pharyngeal exudates are also not useful since they do not correlate with sinus exudates. The most common bacterial species are: streptococcus pneumoniae, Hemophilus influenzae, Moraxella catarrhalis, and streptococcus pyogenes [15,16]. The treatment of RARS and CRS is controversial; several types of antibiotics have been used with limited results, since after initial improvement, patients eventually relapse [9,17]. Corticosteroid irrigations through the nasal passages and oral corticosteroids have also been used based on the few studies conducted in children with different results [1,18,19,20]. Mucolytics, expectorants, and antihistamines have not been shown to be helpful [21,22]. The pneumococcal vaccine does not appear to have decreased the incidence of ARS [13]. In the last case and after having failed with the pharmacological treatment, surgical intervention is usually indicated, with the oblation of the adenoids and/or the palatine tonsils, without the results being entirely satisfactory [23].
There are more and more studies that demonstrate the anti-inflammatory effects of the Mediterranean diet [24], which has allowed us to develop the hypothesis that recurrent inflammatory episodes of the respiratory mucosa are closely related to the abandonment of the traditional diet. This anti-inflammatory action is based on the reduction of pathologies related to oxidative stress, chronic inflammation, and the inflammatory system. Our hypothesis is that diet and individual nutrients can influence the resolution of RARS by stabilizing the inflammatory and immune mechanisms. We have previously conducted studies on the effects of the Mediterranean diet on URTI and their frequent bacterial complications [25], such as recurrent acute otitis media [26], otitis media with effusion [27], persistent nasal obstruction [28], and childhood asthma [29], with satisfactory results. We have also applied the Mediterranean diet in infants since birth and have observed a lower incidence of habitual inflammatory pathology [30]. Following our main line of argument in which we relate recurrent inflammatory episodes with the abandonment of the traditional diet, we have carried out this study on the effects of a traditional Mediterranean diet (TMD) in patients diagnosed with recurrent acute and chronic rhinosinusitis.
2. Material and Methods
2.1. Study Design
The design corresponded to a prospective quasi-experimental study of the comparison of before and after (pre/posttest) of a single group, with each patient examined for one year. The study consecutively included patients aged 1 to 5, diagnosed with RARS and CRS, attending a primary attention pediatrics office between May 2010 and November 2018, with the informed consent of the parents or legal guardians. This study was carried out in the Mediterranean area, in the community of Castilla la Mancha (Spain).
Patients with anatomical abnormalities, allergies, or who had been treated surgically were excluded from the study. The study consisted of comparing the incidence of RARS and CRS in the previous and subsequent years after applying the TMD. The intervention focused on food re-education based on the TMD through the use of the nutritional education program “Learning to eat from the Mediterranean”, which was used in previous studies [12,13]. This program consists of a series of visits with the nutritionist and the pediatrician, who propose to assist the family. Visits are monthly for the first 4 months and bimonthly until the year is completed. The first visit evaluates the diet made by each child and his/her family, and changes in the usual diet are proposed by making schemes, culinary recipes, example menus, etc. Most of the families were accustomed to the traditional (Mediterranean) diet, although its implementation was highly contaminated by industrial pressure. Thus, it was necessary to help them differentiate one from the other. A baseline anthropometric assessment is also performed. Patients were monitored over the course of a year, valuing weight, stature, growth, clinical evolution, treatment needs, adherence to the TMD, and the degree of satisfaction of the families. An explanatory diagram is shown in Figure 1. The study was approved by the Research Committee of the University General Hospital of Ciudad Real (Internal code: C-95, Act 03/2017).
2.2. Study Variables: Clinical Evolution and Treatment Parameters
The study variables were the number of ARS episodes per person and year. RARS is characterized by ARS episodes that last less than 30 days and are separated from each other by at least 10 days, during which the patient is asymptomatic. The patient must present 3 ARS episodes in a period of less than 6 months, or 4 or more in a period of less than 12 months. We also took into account patients with CRS, when episodes of rhino-sinus inflammation lasted more than 90 days, with persistent residual respiratory symptoms [4,5,31].
The following variables were considered, as they are closely related to the pathology studied: upper respiratory tract infections (URTI), acute otitis media (AOM), otitis media with effusion (OME), persistent nasal obstruction (PNO), and recurrent wheezing (RW). Likewise, emergency care, symptomatic drugs, and prescribed antibiotics were assessed, all of which were assessed by person and year. A basic otorhinolaryngological examination was performed that included rhinoscopy, pharyngoscopy, otoscopy, the assessment of the presence of trans-tympanic fluid with a portable tympanometer (MicroTymp’3®, Welch Allyn, New York, NY, USA), an audiometry assessment in the collaborating children with a portable audiometer (Audioscope®, Welch Allyn, New York, NY, USA), the intentional assessment of the face (adenoid facies), a cervical lymphadenopathy, and finally a clinical assessment was made of the degree of involvement of the PNO (mild, moderate, or severe). An episode of URTI was defined by two or more of the following criteria: fever greater than 38 °C measured with a tympanic thermometer, nasal congestion or mouth breathing, runny nose, odynophagia, and cough [25]. AOM was defined following the criteria of the American Pediatric Association Guide: (1) acute presentation; (2) presence of exudate in the middle cavity of the ear demonstrated by tympanic bulging, pathological pneumatoscopy, or otorrhea; (3) inflammatory signs and symptoms such as earache or obvious redness of the eardrum [26,32]. OME was considered when the bilateral exudate or effusion persisted for more than 3 months, or more than 6 if it is unilateral [27]. PNO was defined as persistent difficulty in breathing adequately through the nose, with associated respiratory symptoms, such as mouth breathing, snoring, difficult breathing in sleep, respiratory arrest when sleeping (apnea), restless sleep, hyperflexion postures of the neck in order to sleep, drowsiness or a feeling of not having rested properly, adenoid facies, and swallowing difficulties [28]. RS or childhood asthma was defined as a situation in which three or more episodes of wheezing and/or coughing occur, in a clinical setting in which the diagnosis of asthma is the most likely, after excluding other less frequent processes [29]. In patients suspected of allergic processes, tests were carried out to rule them out.
2.3. Clinical and Therapeutic Evaluation Rate Performed on Parents or Guardians
To assess the clinical evolution of the patients, a questionnaire was designed, addressed to the parents or guardians, in which the symptoms related to RARS and CRS were evaluated, such as nasal breathing, nocturnal cough, difficulties falling asleep, recurrent colds and their complications, the intensity of the clinical symptoms, tolerance and difficulties with the diet carried out, and the degree of satisfaction with the therapeutic effects of the nutritional intervention. For each question in the questionnaire, one can answer the improvement observed with: 3: much, 2: quite, 1: something, 0: nothing. Ten questions referred to the clinic and treatment in the previous four weeks and a maximum of 30 (good control) to a minimum of 0 (poor control) was scored. A patient was considered to be poorly controlled when the total score was equal to or less than 20 (Table 1).
2.4. Parameters of Weight Statural Evolution
By limiting foods that are part of the new Western food culture, we have evaluated the correct weight statural development of the patients included in the study. To do this, we collected anthropometric data, such as weight, height, skinfolds, and perimeters of the arms, abdomen, and waist, and with them, we calculated the body mass index, lean mass, and body fat mass [33].
2.5. Parameters of Adherence to the TMD
To evaluate the dietary habits of patients and their families, we used the Mediterranean Diet Quality Index (KIDMED) test [34,35] and the TMD test that we presented in previous works with the intention of covering the proposed changes by the TMD [33]. The KIDMED test is one of the most prestigious for evaluating the quality of children’s nutritional intake based on the TMD. It consists of a questionnaire of 16 questions that must be answered affirmatively/negatively (yes/no). Affirmative answers to the questions that represent a negative connotation in relation to the Mediterranean diet (there are four) are worth −1 point, and affirmative answers to the questions that represent a positive aspect in relation to the Mediterranean diet (there are 12) are worth +1 point. Negative answers do not score. Therefore, this index can range from 0 (minimum adherence) to 12 (maximum adherence). In order to measure the newly proposed points, we developed a complementary test (the traditional Mediterranean diet test or the TMD test) with the same structure, to which we have added nutritional and behavioral questions that—in our opinion—are not reflected in the KIDMED test. This test consists of 20 questions that must be answered affirmatively/negatively. Unlike the KIDMED test, in the TMD test, all the questions are positive. They are therefore scored with one point for each affirmative answer, and the results can range between 0 and 20 points. A test score below or equal to 7 points is considered ‘poor quality’, a score between 8 and 14 points is considered as ‘need to improve’, and scores above 15 points are considered as ‘optimal traditional Mediterranean diet’. At each visit, we evaluate the nutritional tests, and together with the patients and their parents we analyze any difficulties that may have arisen and examine how we could modify the behavior to obtain the best results. Both questionnaires allow the KIDMED index and the TMD index to be calculated. According to scores obtained in the KIDMED questionnaire, three degrees of the quality of the Mediterranean diet can be obtained: (a) ‘good’ or ‘optimal’, when the score is equal to or greater than eight; (b) ‘average’ or ‘need to improve diet or nutritional habits’, when the score is between four and seven, inclusive; and (c) ‘poorly adapted’ or ‘low-quality diet’, when the score is equal to or less than three. According to the scores obtained in the TMD index, three grades are obtained: low quality ≤7, moderate quality 8–14, optimal quality >14. Physical activity and other variables of the Mediterranean lifestyle were not considered, programmed, or monitored, but rather were included only as general recommendations.
2.6. Foundations of the Traditional Mediterranean Diet
This diet is characterized by a high content of fresh, raw, perishable, and seasonal foods, rich in vegetable fiber, minerals, vitamins, enzymes, and antioxidants; an abundance of fruits, vegetables, legumes, and whole grains, one of whose characteristics is its low to moderate glycemic index; sufficient polyunsaturated fats from crude oils, nuts, seeds, and fish; low protein and saturated fat content of animal origin; and a low use of precooked and industrial foods. This means, in daily practice, the limitation of products such as white bread, industrial pastries, cow’s milk, red and processed meats, sugary industrial beverages, and precooked fast food [36]. The TMD is based on the Decalogue that the Foundation of the Mediterranean diet proposes to us through its website (Table 2) [37].
This has been proclaimed a cultural heritage and an intangible heritage of humanity by Unesco [38]. In Table 3, we expose the differences between the TMD and the diet promoted by “Western civilization”.
Sample size and statistical analysis: To calculate the sample size, a significance level of 0.05 and a power of 80% was used, assuming a decrease in the degree of involvement of ARS per patient and year of 1 unit, and a standard deviation of 3.5 units, adjusting to a 25% loss, which resulted in a sample size of 80 patients. For the analysis of the results, the statistical package SPSS 15.0 was used. A descriptive analysis was carried out with statistics of central tendency and dispersion for the quantitative variables and absolute and relative frequencies for the qualitative variables. The comparison of the results of the different variables before and after the intervention was carried out by means of the Student’s t-test for paired data when the variables followed a normal distribution, or by the Wilcoxon test when they did not adjust to normal, after checking with the Shapiro–Wilk test.
3. Results
Participation was proposed in a program called ‘Learning to eat from the Mediterranean’. The families of 131 patients met the RARS and RSC inclusion criteria. Nine refused to participate. From the 122 patients included, eight left the program after the first sessions. Three were due to social or personal difficulties in implementing the diet, two were due to the disagreement with the limitations of certain foods, and three were due to surgical interventions indicated by the otorhinolaryngology service and not coordinated with our team. The study was thus completed with a total of 114 patients (56 girls and 58 boys) with an average age of 2.9 years. All of the patients included in the study were evaluated at 4 and 12 months after the initial visit. The results obtained were similar in both sexes, and are thus collated together (Table 4).
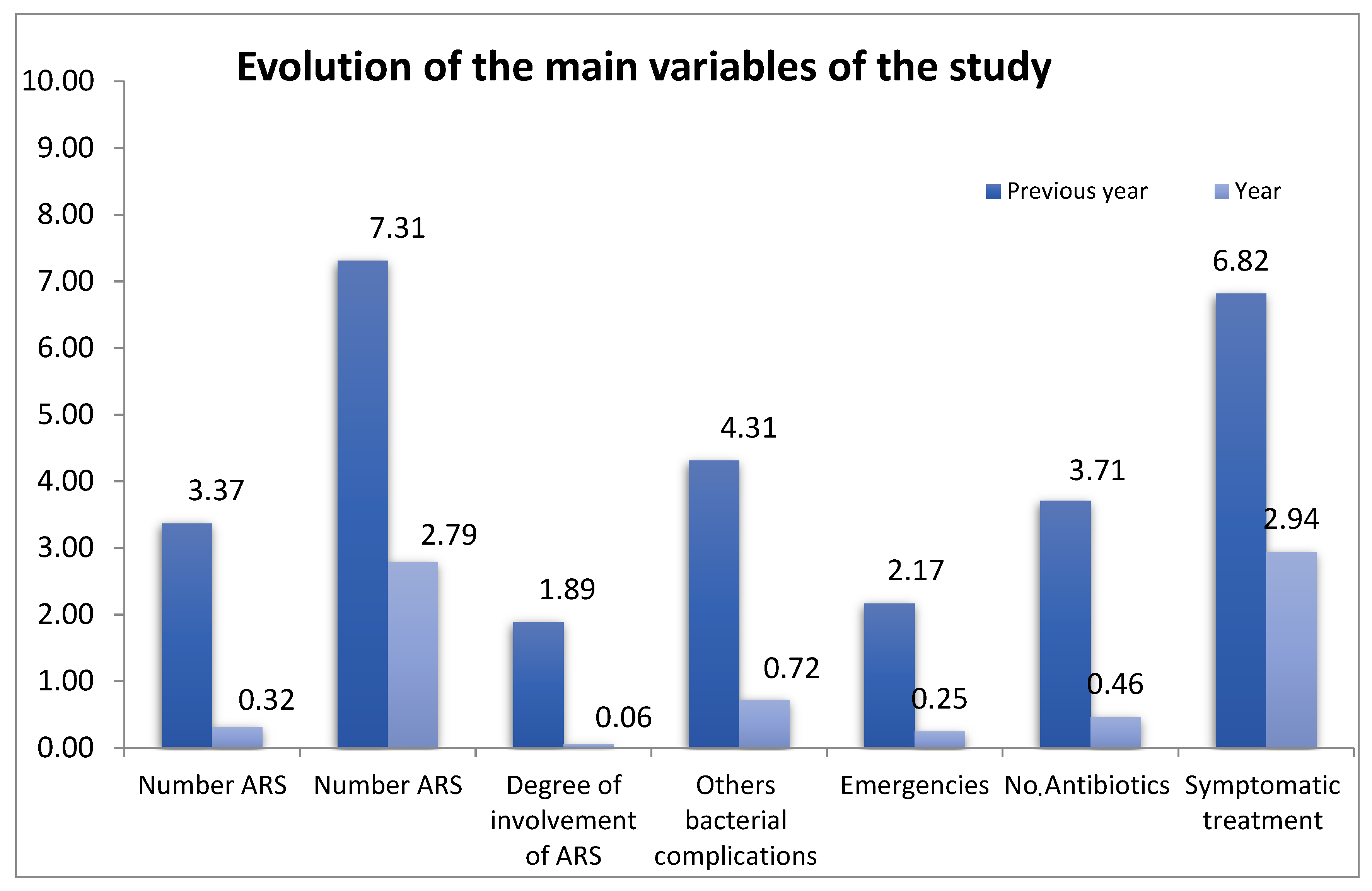
Table 5 shows the evolution of the patients with the number of ARS episodes in the previous year and the following year after the application of the nutritional program; ARS episodes per child and year were assessed. The evolution of other bacterial complications of the oropharynx is also exposed.
We have evaluated the degree of clinical involvement of children with RARS and CRS and we have recorded the mean of their total score before and after the treatment. We have also assessed the number of times the patients visited the emergency department in the previous year and the following year, as well as the antibiotic treatment cycles they received during their inflammatory processes and symptomatic treatment, such as paracetamol, saline sprays, anti-inflammatory drugs, or expectorant mucolytics (Figure 2).
The clinical evaluation test of the patients is shown in Table 1, which shows the assessment of the families regarding the evolution of the process and the difficulties of treatment. The anthropometric variables before, at four months, and after intervention, are set out in Table 6. The mean weight increase the year before the study was 2.33 kg compared to the current 2.64 kg, and the increase in average height was 8.8 cm compared to 9.4 cm today.
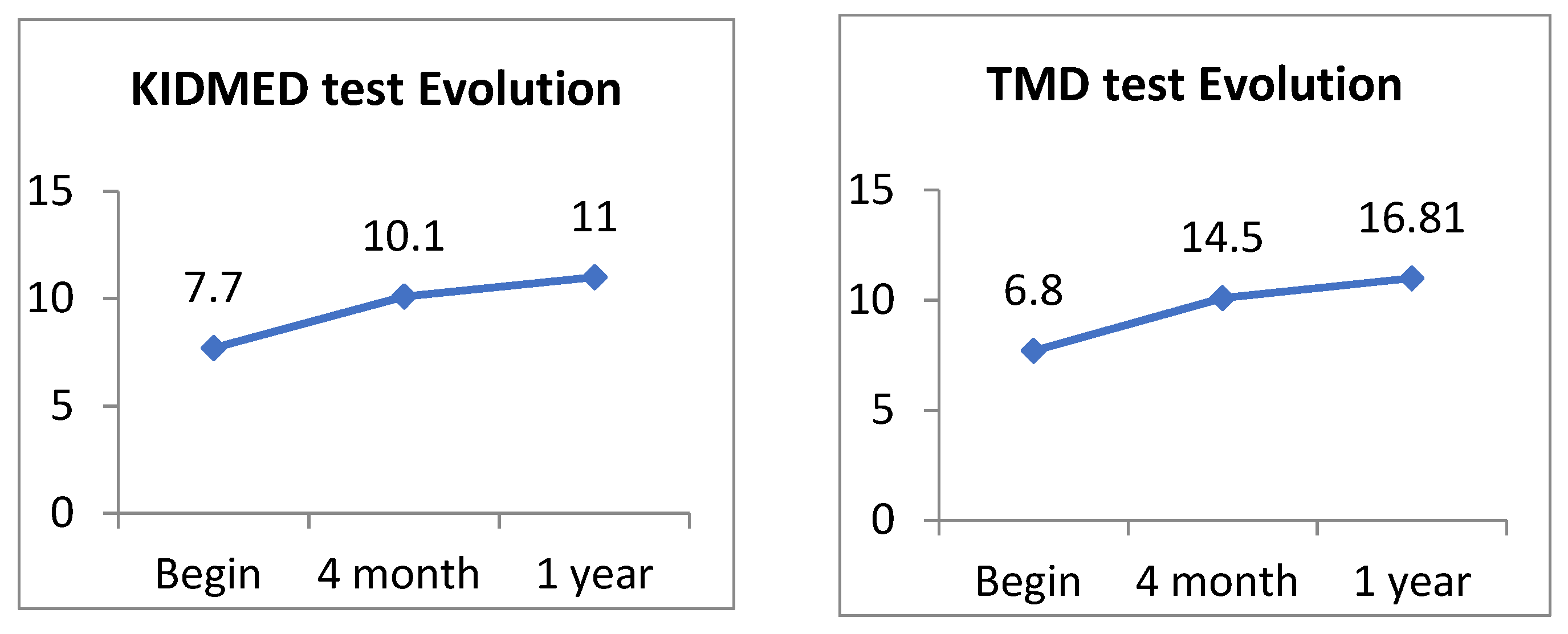
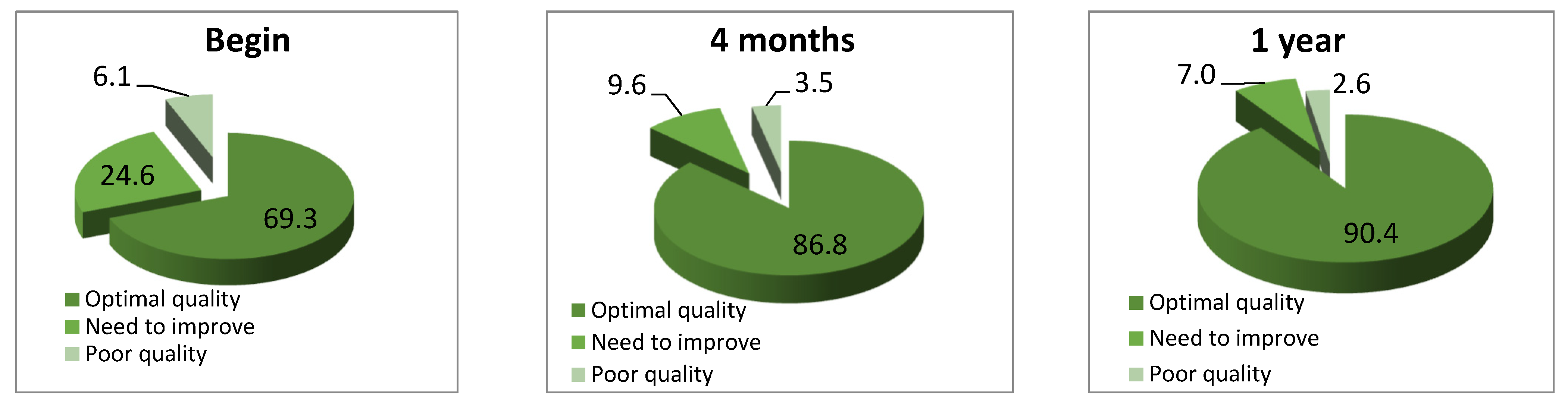
The mean value of the KIDMED index at the beginning of the program was 7.7 ± 1.82 points; 24.6% of the patients obtained a qualification according to the KIDMED test of “need to improve” and 69.3% obtained the qualification of “optimal diet”. At the end of the study, 90.4% of the children obtained optimal levels with a mean of 11 points, mean difference of 2.11 ± 0.10 (95% CI: 1.91–2.31 p < 0.01). According to this data, the average value of the KIDMED index evolved from a score considered medium-high at the beginning of the program to an optimal value at the end of the program (Table 7, Figure 3 and Figure 4).
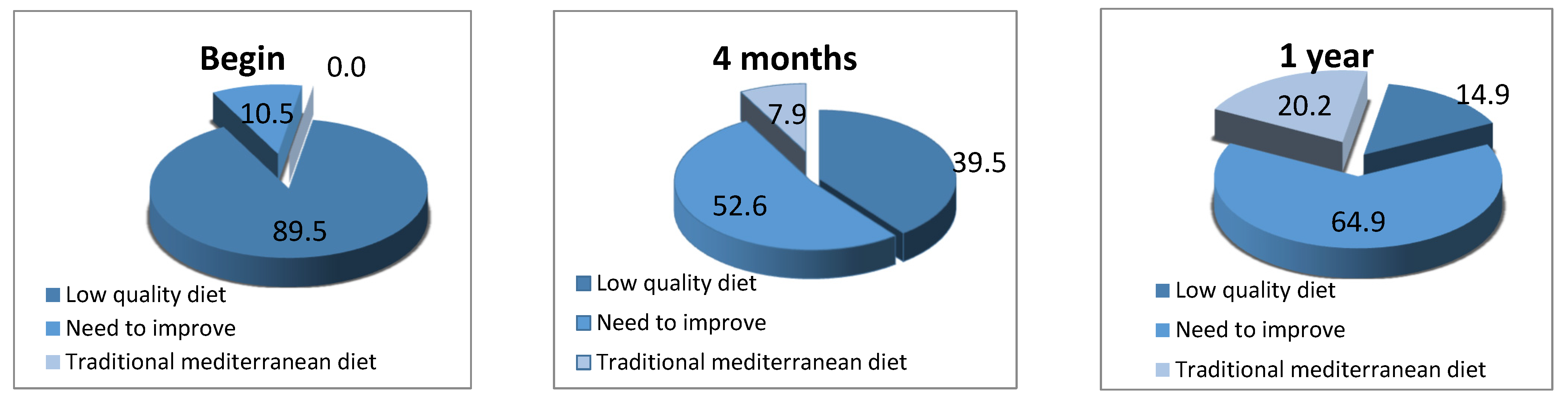
At the beginning of the study, the mean value of the TMD test was 6.79 ± 1.98, qualifying as a poor-quality diet; 89.5% of the sample obtained a score below eight points (poor-quality diet) and 10.5% obtained a score between eight and fourteen points (need for improvement). At the end of the study, the mean score was 16.78 ± 1.90 points, qualifying as an optimal traditional Mediterranean diet. The TMD test evolved from levels considered to be low quality to optimal levels (Table 8 and Figure 5). Despite the good score obtained with the KIDMED test, the patients maintained the incidence of ARS. However, when applying the TMD test, we obtained statistically significant results in the evolution of ARS.
4. Discussion
In view of these results, we suggest that the traditional Mediterranean diet could help in the prevention and also in the control of RARS and CRS, improve their treatment, and limit pharmacological and surgical intervention. At the end of the year of the intervention, less than 5% of the patients treated met the criteria to be classified as having RARS and CRS. Of the patients, 53.5% did not have any ARS, and 26.3% had only one, when the usual issue with the conventional treatment is that new episodes would have been repeated and would have ended up in the OR service. We had few episodes of CRS, probably because many of the patients already followed an acceptable Mediterranean diet, and because when they reached three to four annual episodes of ARS, we incorporated them into the TMD. RARS and CRS often overlap and it is difficult to know when a new rhinosinusitis episode starts or when it is a relapse of a process that has not yet been resolved [5]. In our study, most of the patients were diagnosed with RARS.
The number of ARS episodes decreased by 90.5%, from a mean of 3.37 to less than 0.32% episodes per year. Although with age the effectiveness of the immune system increases and recurrent inflammatory episodes tend to disappear spontaneously, such a rapid evolution in the disappearance of symptoms could not be anticipated, which resulted in preventing the patients from having prolonged pharmacological treatments and undergoing surgery. Thus, we deduce that the nutritional intervention was beneficial for them. The degree of intensity of the ARS decreased significantly, so that not only did the total number of ARS episodes decrease, but there was also less involvement and fewer symptoms in the patients who followed the nutritional guidelines. It is important to note that during the time that the patients were enrolled in the study, we were extending the application of the TMD to the entire pediatric population (siblings, relatives, patients with other recurrent pathologies, and infants under two years of age). This led to a progressive decrease in the number of patients diagnosed with ARS, thus delaying the achievement of the sample size [30]. As we had already verified in previous studies, the URTI [25], which are one of the precipitating reasons for bacterial involvement of the paranasal sinuses, decreased significantly. In our study, there was 60% less URTI than in the previous year.
The number of other bacterial complications decreased by 88.8% (4.31 in the previous year versus 0.72 in the year of intervention); 61% of the patients did not have any bacterial complication during the nutritional intervention period, 28% had only one in the entire year, and 10% had two, compared to the more than four episodes they had on average in the previous year. Children with PNO went from a mild-moderate intensity profile to not at all-mild [28]. Likewise, one of the most frequent reasons for attending pediatric emergencies is the discomfort caused by ARS, with worsening of the URTI and difficulties in breathing through the nose and being able to fall asleep; there was a significant reduction of 88.5% in emergencies compared to the previous year. As a consequence of the decrease in URTI, ARS, and other bacterial complications, symptomatic treatment decreased by 57%. Likewise, antibiotic treatment was reduced by 87.6%, which allows us to verify a greater benignity of the infectious processes. The degree of satisfaction shown by the parents in the clinical evaluation test was high, with scores indicating a good clinical and therapeutic evolution. In the first four months, improvements were already observed compared to the situation of the previous year, so that loyalty increased and monitoring was easier.
There was a good tolerance to the proposed diet, with easy adaptation and without great culinary difficulties. The main difficulty was the fulfillment of the diet, as they were proposed to make a homemade, familiar diet of fresh products that must be prepared, and the parents did not always have the time and dedication to do it properly. The presence of a dietitian-nutritionist was essential to guarantee the compliance with the the TMD. By the end of the program, the dietary habits of the patients had improved in the sample as a whole; an increase in the number of patients consuming fruits, vegetables, nuts, whole grains, and fermented dairy products was observed. In general, the consumption of proteins of animal origin was reduced considerably, especially cow’s milk, red meat, and meat products. The consumption of processed foods also decreased, especially industrial pastries. Prior to the development of our study, we promoted the application of a validated test, such as the KIDMED test [34], with the intention of preventing and treating inflammatory and recurrent diseases, as well as preventing becoming overweight and obese [33]. Despite this, we did not obtain satisfactory results, so we decided to implement a new TMD test, which collected information about important aspects of the Mediterranean diet that had not previously been detailed. Many of the children who had an optimal KIDMED test failed on the TMD index. It was only when they began to show improved scores with the new test that we obtained satisfactory results. In the KIDMED test, some variables that we believe are important are not considered. For example, no differences are noted between refined cereals and whole grains, nor are there any references to the consumption of sugar or sugary industrial juices. Additionally, in general, glycemic index/glycemic load is not taken into account. In the lipid section, saturated fat consumption is neither limited nor evaluated. The test does not allow for the detection of an excess consumption of animal proteins. Additionally, no assessment is made of the consumption of raw food, nor is the minimum amount to be taken specified. Serving sizes and schedules are not taken into account. Completing the KIDMED test has not been shown to be effective in our study. We believe that these small nuances that we have proposed in the TMD test are important for obtaining satisfactory results in the examination of recurrent inflammatory diseases, in particular RARS. The patients showed satisfactory predicted growth rates. Their weight, height, and BMI percentile evolved as expected. A positive result was the slight decrease in the BMI and fat mass levels and a small increase in height and lean body mass.
Although these data suggest that the intake of healthy foods and/or the avoidance of non-traditional foods may play an important role in the control of ARS, there are almost no bibliographic references in the scientific literature. We want to highlight that most of the studies published on the treatment of RARS and CRS are based on the application of actions external to the body, such as the use of drugs or surgical intervention. The nutritional factors have not been taken into account, when the deconfiguration of the inflammatory system and the immune system due to inadequate food is likely at the base of these pathologies. The etiology and pathogenesis of this inflammation are often unclear, although this is believed to represent an inappropriate or excessive immune response to an external stimulus inhaled through the nasal airways [1].
The research has suggested the protective effect of breastfeeding for at least 6 months, although other risk factors accumulate after that age [39]. Among them, the early introduction of adapted milk has been noted [40] as well as the abuse of antibiotics [41]. A pan-European study has shown that children consuming excessive refined flours and processed animal-based products and having a diet poor in fruit and vegetables have high inflammatory markers, and as a whole, they can be considered to be in a pro-inflammatory state [42]. Likewise, ARS patients have been shown to have an altered regulation of key immune mediators during good health and pathogenesis and are amenable to treatment by immunomodulatory intervention [43]. Predominantly eating foods with a low glycemic index/load—typical of the TMD—helps to control insulin levels; this hormone may interfere in the formation of anti-inflammatory eicosanoids, by blocking the ∆-desaturase enzyme [44]. Similarly, the TMD is rich in vitamins, minerals, and antioxidants, many of which are indispensable co-factors in the enzymatic chemical reactions involved in the body’s immune processes. Children with recurrent inflammatory infections have been shown to have poor responses to pro-inflammatory cytokines and antiviral chemokines [45,46]. High-mobility group box protein 1 (HMGB1), that acts as a mediator between innate and acquired immunity, is overexpressed and can play a role in the progression of CRS and RARS, acting as an inflammatory marker and cytokine [47].
There is a growing interest in understanding the alterations of the naso-sinus microbiome as a causative factor of the disease. Likewise, it has been considered that there is a dysfunctional naso-sinus mucosa, in which defects of the epithelial surface may be the basis of the etiology and pathogenesis of the disorder [48,49,50,51]. It has been shown that an inadequate diet, away from the traditional diet, can alter the rhino-sinus microbiota and cause intestinal dysbiosis [52]. Biofilms provide a protected environment for pathogens and can be responsible for persistent or recurrent diseases [1]. The immune system may not recognize foreign, infrequent, or foreign microbial germs, and cause the cytokines or other cell signaling molecules to react, which alter inflammatory mechanisms and leave the respiratory mucosa in a permanent pro-inflammatory state. In this way, in the face of small stimuli, such as simple catarrhal viruses, hyper-reactivity of the mucous membranes would be triggered, with flowery symptoms, which would end up causing the usual complications and in particular the RARS. Adenoid hypertrophy and adenoiditis contribute significantly to the pathogenesis of RARS, being one of the main differences between the involvement of children and adults [1,53]. The mechanisms by which the intestinal flora modulates the immune response are not clear, but it seems prudent to favor an intestinal microbiota typical of the human species, since evolution and genetic coding have had to configure a specific symbiosis between nutrition, the intestinal microbiota, and immunity that we should not modify.
The growing interest in the Mediterranean diet is based on its role in inflammatory diseases [54]. Several clinical and epidemiological studies, as well as experimental studies, show that the consumption of the TMD reduces the incidence of certain pathologies related to oxidative stress, chronic inflammation, and the immune system, such as cancer, atherosclerosis, or cardiovascular disease [55]. There is evidence that diet and individual nutrients can influence the systemic markers of immune function and inflammation [56]. The pro-inflammatory actions of platelet-activating factor (PAF), one of the most potent endogenous mediators of inflammation, can be favorably modulated by the TMD and regulate its metabolism [57]. The TMD is an ancient diet, dating back to way before documented history, and which has stood the test of time. Many of the foodstuffs eaten as part of the Western diet contain materials not recognized or assimilated by the human body. Many of these products are not absorbed by the intestine, thus encouraging non-specific microflora that is alien to the human intestinal microbiota. The excess “antigenic load” inherent in the Western diet of today—which has multiplied the available foodstuffs by the thousand—may misadjust our immune system, making it weaker and notably hyperplasic.
It has recently been proven that better adherence to the Mediterranean diet may be associated with a lower risk of COVID-19 [58,59], demonstrating its effect against virus infections. Secretory IgA antibodies are an important part of the immune defense against viral diseases. People who ingest Okinawan vegetables have high IgA levels and might be more likely to develop immunity against influenza RNA viruses [60].
One of the characteristics that every research study should have is that it is easily reproducible, using small groups, and with little economic cost. The work presented here is easy to reproduce in any primary care pediatric consultation, but it is not easy to perform due to the lack of nutritionists and the lack of effective monitoring of the diet.
We could not perform a study with a control group since most of our pediatric space was adhering to the Mediterranean diet and it did not seem ethical to promote a pro-inflammatory Western-type diet in a control group. Our hypothesis is precisely that the standard diet proposed by “Western civilization” is the origin of alterations in the inflammatory and immune mechanisms, and therefore the precipitating factor of most of the inflammatory and recurrent diseases of childhood. It would have been very interesting to perform analyses that measured the response of the immune system, inflammatory markers, and the data on the modification of the microbiota when making the nutritional change.
Most of our patients have been consecutively included in the program “Learning to eat from the Mediterranean” and we have verified how the prevalence of ARS and other inflammatory recurrent diseases has decreased considerably. The change of the “model of medicine” that these research studies entail should not go unnoticed. It is no longer about remedying a disease with external drugs or surgical interventions, but the therapeutic proposal is based on providing the body with everything it needs to solve their needs and eliminate that for which it is not ready.
We can conclude by saying that the application of the traditional Mediterranean diet could have promising effects in the prevention and treatment of acute recurrent and chronic rhinosinusitis, with a notable decrease in associated inflammatory diseases, limiting pharmacological and surgical intervention in many of these patients.
Author Contributions
Conceptualization, F.M.C.-S.; and B.C.; methodology, F.M.C.-S.; software, B.C.; validation, F.M.C.-S.; B.C., and A.C.; formal analysis, B.C.; investigation, F.M.C.-S.; B.C., and A.C.; re-sources, F.M.C.-S.; data curation, B.C.; writing—original draft preparation, F.M.C.-S.; writing—review and editing, F.M.C.-S.; visualization, F.M.C.-S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Hospital General Universitario de Ciudad Real (Internal code: C-95, Act 03/2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Quintanilla-Dieck, L.; Lam, D.J. Chronic Rhinosinusitis in Children. Curr. Treat. Options Pediatr. 2018, 4, 413–424. [Google Scholar] [CrossRef]
- Gilani, S.; Shin, J.J. The Burden and Visit Prevalence of Pediatric Chronic Rhinosinusitis. Otolaryngol. Neck Surg. 2017, 157, 1048–1052. [Google Scholar] [CrossRef]
- Brietzke, S.E.; Shin, J.J.; Choi, S.; Lee, J.T.; Parikh, S.R.; Pena, M.; Prager, J.D.; Ramadan, H.; Veling, M.; Corrigan, M.; et al. Clinical Consensus Statement. Otolaryngol. Neck Surg. 2014, 151, 542–553. [Google Scholar] [CrossRef] [Green Version]
- Martínez, L.; Albañil, R.; De la Flor, J.; Piñeiro RCervera, J.; Baquero Artigao, F.; Alfayate Miguelez, S.; Moraga Llop, F.; Cilleruelo Ortega, M.J.; Calvo Rey, C. Consensus document on the aetiology, diagnosis and treatment of sinusitis. An. Pediatr. 2013, 79, 330.e1–330.e12. [Google Scholar]
- Orlandi, R.R.; Kingdom, T.T.; Hwang, P.H.; Smith, T.L.; Alt, J.A.; Baroody, F.M.; Batra, P.S.; Bernal-Sprekelsen, M.; Bhattacharyya, N.; Chandra, R.K.; et al. International Consensus Statement on Allergy and Rhinology: Rhinosinusitis. Int. Forum Allergy Rhinol. 2016, 6, S22–S209. [Google Scholar] [CrossRef] [Green Version]
- Gallant, J.-N.; Basem, J.; Turner, J.; Shannon, C.N.; Virgin, F.W. Nasal saline irrigation in pediatric rhinosinusitis: A systematic review. Int. J. Pediatr. Otorhinolaryngol. 2018, 108, 155–162. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. European position paper on rhinosinusitis and nasal polyps. Rhinology 2012, 50, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandy, Z.; Ference, E.; Lee, J.T. Clinical guidelines on chronic rhinosinusitis in children. Curr. Allergy Asthma Rep. 2019, 19, 14. [Google Scholar] [CrossRef] [PubMed]
- Wald, E.R.; Applegate, K.; Bordley, C.; Darrow, D.H.; Glode, M.P.; Marcy, S.M.; E Nelson, C.; Rosenfeld, R.M.; Shaikh, N.; Smith, M.J.; et al. Clinical Practice Guideline for the Diagnosis and Management of Acute Bacterial Sinusitis in Children Aged 1 to 18 Years. Pediatrics 2013, 132, e262–e280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Licari, A.; Brambilla, I.; Castagnoli, R.; Marseglia, A.; Paganelli, V.; Foiadelli, T.; Marseglia, G.L. Rhinosinutis and Asthma in Children. Sinusitis 2018, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Ebell, M.H.; McKay, B.; Guilbault, R.; Ermias, Y. Diagnosis of acute rhinosinusitis in primary care: A systematic review of test accuracy. Br. J. Gen. Pract. 2016, 66, e612–e632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, D.J.; Gonzales, R.; Cabana, M.D.; Hersh, A.l. National trends in visit rates and antibiotic prescribing for children whit acute sinusitis. Pediatrics 2011, 127, 28–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopp, R.J. Pediatric Chronic Rhinosinusitis: Unmet Needs. Sinusitis 2020, 4, 2–7. [Google Scholar] [CrossRef]
- Hopp, R.; Allison, J.; Brooks, D. Fifty Years of Chronic Rhinosinusitis in Children: The Accepted, the Unknown, and Thoughts for the Future. Pediatr. Allergy Immunol. Pulmonol. 2016, 29, 61–67. [Google Scholar] [CrossRef]
- Callén Blecua, M.; Garmendia Iglesias, M.A. Sinusitis. The Pediatrician of Care Primary and Sinusitis Protocols of the GVR (Publication P-GVR-7). Available online: https://www.respirar.org/images/sinusitis-2013.pdf (accessed on 22 June 2021).
- Hopp, R.J. Diagnosis and manging chronic pediatric rhinosinusitis: Still more questions than answers. Arch. Immunol. Allergy 2019, 2, 35–41. [Google Scholar]
- Head, K.; Chong, L.Y.; Piromchai, P.; Hopkins, C.; Philpott, C.; Schilder, A.G.; Burton, M.J. Systemic and topical antibiotics for chronic rhinosinusitis. Cochrane Database Syst. Rev. 2016, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, L.Y.; Head, K.; Hopkins, C.; Philpott, C.; Schilder, A.G.M.; Burton, M.J. Intranasal steroids versus placebo or no intervention for chronic rhinosinusitis. Cochrane Database Syst. Rev. 2016, 4, CD011996. [Google Scholar] [CrossRef] [Green Version]
- Head, K.; Chong, L.Y.; Hopkins, C.; Philpott, C.; Burton, M.J.; Schillder, A.G. Short-course oral steroids alone for chronic rhinosinusitis. Cochrane Database Syst Rev. 2016. [Google Scholar] [CrossRef] [Green Version]
- Duse, M.; Santamaria, F.; Verga, M.C.; Bergamini, M.; Simeone, G.; Leonardi, L.; Tezza, G.; Bianchi, A.; Capuano, A.; Cardinale, F.; et al. Inter-society consensus for the use of inhaled corticosteroids in infants, children and adolescents with airway diseases. Ital. J. Pediatr. 2021, 47, 97. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, N.; Wald, E.R. Decongestants, antihistamines and nasal irrigation for acute sinusitis in children. Cochrane Database Syst. Rev. 2014, 2014, CD007909. [Google Scholar] [CrossRef]
- Runkle, K. Decongestants, antihistamines and nasal irrigation for acute sinusitis in children. Paediatr. Child Health 2016, 21, 143–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beswick, D.M.; Messner, A.H.; Hwang, P.H. Pediatric Chronic Rhinosinusitis Management in Rhinologists and Pediatric Otolaryngologists. Ann. Otol. Rhinol. Laryngol. 2017, 126, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Kargın, D.; Tomaino, L.; Serra-Majem, L. Experimental Outcomes of the Mediterranean Diet: Lessons Learned from the Predimed Randomized Controlled Trial. Nutrients 2019, 11, 2991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calatayud, F.; Calatayud, B.; Gallego, J.; González-Martín, C.; Alguacil, L. Effects of Mediterranean diet in patients with recurring colds and frequent complications. Allergol. Immunopathol. 2017, 45, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Calatayud-Sáez, F.M.; Calatayud, B.; Calatayud, A. Recurrent acute otitis media could be related to the pro-inflammatory state that causes an incorrect diet. Prog. Nutr. Pending publication.
- Calatayud-Sáez, F.; Calatayud, B.; Calatayud, A. Effects of the Traditional Mediterranean Diet in Patients with Otitis Media with Effusion. Nutrients 2021, 13, 2181. [Google Scholar] [CrossRef]
- Calatayud-Sáez, F.; Calatayud, B.; Calatayud, A. Persistent Nasal Obstruction: An Expression of the Pro-Inflammatory State? Sinusitis 2021, 5, 90–100. [Google Scholar] [CrossRef]
- Calatayud-Sáez, F.M.; del Prado, B.C.M.; Fernández-Pacheco, J.G.; González-Martín, C.; Merino, L.A. Mediterranean diet and childhood asthma. Allergol. Immunopathol. 2016, 44, 99–105. [Google Scholar] [CrossRef]
- Calatayud-Sáez, F.M.; Calatayud, B.; Luque, M.; Calatayud, A.; Gallego, J.G.; Rivas, F. Effects of affinity to the Mediterranean Diet pattern along with breastfeeding on childhood asthma, inflammatory and recurrent diseases in an intervention study. Authorea 2020. Preprit, pending review. [Google Scholar] [CrossRef]
- Callén, M.; Garmendia, M.A. Sinusitis. The Primary Care Pediatrician and Sinusitis GVR Protocols. (publication P-GVR-7). Available online: https://www.respirar.org/images/sinusitis-2013.pdf (accessed on 26 June 2021).
- American Academy of Pediatrics and American Academy of Family Physicians. Diagnosis and management of acute otitis media. Pediatrics 2004, 113, 1451–1465. [Google Scholar] [CrossRef] [Green Version]
- Calatayud-Sáez, F.M.; Calatayud, B. Efficacy of the recommendation of a Mediterranean diet pattern in preschoolers with overweight and obesity. Acta Pediátr. Esp. 2020, 78, e101–e110. [Google Scholar]
- Serra, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; Pérez, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of the KIDMED, quality index of the Mediterranean diet in childhood and adolescence. In Infant and Youth Nutrition. I Study enKid. Barcelona: Masson; Serra, L., Aranceta, J., Eds.; 2002; Available online: https://www.casadellibro.com/libro-alimentacion-infantil-y-juvenil-estudio-enkid/9788445812549/856399 (accessed on 28 June 2021).
- Serra, L.; Ribas, L.; Aranceta, J.; Pérez, C.; Saavedra, P.; Peña, L. Childhood and youth obesity in Spain. EnKid study results (1998–2000) Med. Clin. 2003, 121, 725–732. [Google Scholar]
- Márquez-Sandoval, F.; Bulló, M.; Vizmanos, B.; Casas-Agustench, P.; Salas-Salvadó, J. A healthy eating pattern: The traditional Mediterranean diet. Antropo 2008, 16, 11–22. [Google Scholar]
- Foundation of the Mediterranean Diet. 10 Basic Recommendations of the Mediterranean Diet. Available online: http://fdmed.org/dieta-mediterranea/decalogo/ (accessed on 28 June 2021).
- WHO. Overweight and Obesity; World Health Organization: Geneva, Switzerland, 2006; Available online: https://ich.unesco.org/en/RL/mediterranean-diet-00884?RL=00884 (accessed on 28 June 2021).
- Brennan-Jones, C.G.; Eikelboom, R.H.; Jacques, A.; Swanepoel, D.W.; Atlas, M.D.; Whitehouse, A.J.; Jamieson, S.E.; Oddy, W.H. Protective benefit of predominant breastfeeding against otitis media may be limited to early childhood: Results from a prospective birth cohort study. Clin. Otolaryngol. 2016, 42, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chonmaitree, T.; Trujillo, R.; Jennings, K.; Alvarez-Fernandez, P.; Patel, J.A.; Loeffelholz, M.J.; Nokso-Koivisto, J.; Matalon, R.; Pyles, R.B.; Miller, A.L.; et al. Acute Otitis Media and Other Complications of Viral Respiratory Infection. Pediatrics 2016, 137, e20153555. [Google Scholar] [CrossRef] [Green Version]
- Bezáková, N.; Damoiseaux, R.A.; Hoes, A.W.; Schilder, A.G.; Rovers, M.M. Recurrence up to 3.5 years after antibiotic treatment of acute otitis media in very young Dutch children: Survey of trial participants. BMJ 2009, 338, b2525. [Google Scholar] [CrossRef] [Green Version]
- González-Gil, E.M.; Tognon, G.; Lissner, L.; Intemann, T.; Pala, V.; Galli, C.; Wolters, M.; Siani, A.; Veidebaum, T.; Michels, N.; et al. Prospective associations between dietary patterns and high sensitivity C-reactive protein in European children: The IDEFICS study. Eur. J. Nutr. 2018, 57, 1397–1407. [Google Scholar] [CrossRef] [Green Version]
- Yaqoob, P. Mechanisms underlying the immunomodulatory effects of n-3 PUFA. Proc. Nutr. Soc. 2010, 69, 311–315. [Google Scholar] [CrossRef] [Green Version]
- Gil, A.; Sánchez de Medina, F. Intercellular communication: Hormones, eicosanoides and cytokines. Capit. 3 of de Treaty of Nutrition, Gil A. Volume I. Physiological and biochmical bases of nutrition. Ed. Panamericana. 2010. [Google Scholar]
- Ren, D.; Xu, Q.; Almudevar, A.L.; E Pichichero, M. Impaired Proinflammatory Response in Stringently Defined Otitis-prone Children During Viral Upper Respiratory Infections. Clin. Infect. Dis. 2018, 68, 1566–1574. [Google Scholar] [CrossRef]
- Guilleminault, L.; Williams, E.J.; Scott, H.A.; Berthon, B.S.; Jensen, M.; Wood, L.G. Diet and Asthma: Is It Time to Adapt Our Message? Nutrients 2017, 9, 1227. [Google Scholar] [CrossRef] [Green Version]
- Ciprandi, G.; Bellussi, L.M.; Passali, G.C.; Damiani, V.; Passali, D. HMGB1 in nasal inflammatory diseases: A reappraisal 30 years after its discovery. Expert Rev. Clin. Immunol. 2020, 16, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Hopp, R.J. Pediatric Chronic Sinusitis: What are thou? A Clinical Opinion. Sinusitis 2017, 2, 6. [Google Scholar] [CrossRef] [Green Version]
- Silviu-Dan, F.; Fanny, S.D. Pediatric Chronic Rhinosinusitis. Pediatr. Ann. 2014, 43, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Bose, S.; Grammer, L.C.; Peters, A.T. Infectious Chronic Rhinosinusitis. J. Allergy Clin. Immunol. Pract. 2016, 4, 584–589. [Google Scholar] [CrossRef]
- Pasha, M.A. State-of-the-Art Adult Chronic Rhinosinusitis Microbiome: Perspective for Future Studies in Pediatrics. Sinusitis 2018, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Hamilos, D.L. Pediatric Chronic Rhinosinusitis. Am. J. Rhinol. Allergy 2015, 29, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Rojas, V.; Ruz, P.; Valdés, C. Chronic rhinosinusitis in children: Review of the evaluation and current management. Rev. Otorrinolaringol. Cir. Cabeza Cuello 2020, 80, 237–246, ISSN 0718-4816. [Google Scholar] [CrossRef]
- Tsigalou, C.; Konstantinidis, T.; Paraschaki, A.; Stavropoulou, E.; Voidarou, C.; Bezirtzoglou, E. Mediterranean Diet as a Tool to Combat Inflammation and Chronic Diseases. An Overview. Biomedicines 2020, 8, 201. [Google Scholar] [CrossRef]
- Casas, R.; Estruch, R.; Sacanella, E. The Protective Effects of Extra Virgin Olive Oil on Immune-mediated Inflammatory Responses. Endocr. Metab. Immune Disord.-Drug Targets 2017, 18, 23–35. [Google Scholar] [CrossRef]
- Venter, C.; Eyerich, S.; Sarin, T.; Klatt, K.C. Nutrition and the Immune System: A Complicated Tango. Nutrients 2020, 12, 818. [Google Scholar] [CrossRef] [Green Version]
- Nomikos, T.; Fragopoulou, E.; Antonopoulou, S.; Panagiotakos, D.B. Mediterranean diet and platelet-activating factor; a systematic review. Clin. Biochem. 2018, 60, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Perez-Araluce, R.; Martinez-Gonzalez, M.; Fernández-Lázaro, C.; Bes-Rastrollo, M.; Gea, A.; Carlos, S. Mediterranean diet and the risk of COVID-19 in the ‘Seguimiento Universidad de Navarra’ cohort. Clin. Nutr. 2021, 15. in Press. [Google Scholar] [CrossRef]
- Iddir, M.; Brito, A.; Dingeo, G.; Del Campo, S.S.F.; Samouda, H.; La Frano, M.R.; Bohn, T. Strengthening the Immune System and Reducing Inflammation and Oxidative Stress through Diet and Nutrition: Considerations during the COVID-19 Crisis. Nutrients 2020, 12, 1562. [Google Scholar] [CrossRef]
- Gonda, K.; Kanazawa, H.; Maeda, G.; Matayoshi, C.; Hirose, N.; Katsumoto, Y.; Kono, K.; Takenoshita, S. Ingestion of Okinawa Island Vegetables Increases IgA Levels and Prevents the Spread of Influenza RNA Viruses. Nutrients 2021, 13, 1773. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study design diagram.

Figure 2.
Evolution of the main variables of the study.

Figure 3.
The KIDMED and the TMD tests evolution.

Figure 4.
Evolution of the quality of diet, measured using the KIDMED test.

Figure 5.
Evolution of the quality of diet, measured using the TMD test.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Clinical and therapeutic evaluation index in rhinosinusitis. Responses from the parents or guardians regarding the improvement observed: 3: much, 2: quite, 1: something, 0: nothing.
Table 1.
Clinical and therapeutic evaluation index in rhinosinusitis. Responses from the parents or guardians regarding the improvement observed: 3: much, 2: quite, 1: something, 0: nothing.
| * Average Score Obtained by All Patients | 4 Months * | 1 Year * |
|---|---|---|
| Has the number of episodes of rhinosinusitis decreased? | 2.27 | 2.53 |
| Have you noticed less intensity in the infectious processes? | 2.67 | 2.93 |
| Has the need to go to the emergency room decreased? | 2.27 | 2.88 |
| Have other complications decreased? | 2.87 | 2.91 |
| Has there been a greater recovery from the state of normality? | 2.32 | 2.92 |
| Have you noticed the least use of antibiotics? | 2.48 | 2.94 |
| Have you noticed the least use of symptomatic medications? | 2.92 | 2.92 |
| Has there been good diet tolerance on the part of the patient? | 2.92 | 2.92 |
| Has there been collaboration on dietary changes? | 2.93 | 2.93 |
| Are you satisfied with the results? | 2.45 | 2.91 |
* is set at 4 and 12 months.
Table 2.
The Mediterranean diet. Ten basic recommendations.
| 1. Use olive oil as your main source of added fat. |
| 2. Eat plenty of fruits and vegetables; fruits, vegetables, legumes, and nuts. |
| 3. Bread and other grain products (pasta, rice, and whole grains) should be a part of your everyday diet. |
| 4. Foods that have undergone minimal processing and that are fresh and locally produced are best. |
| 5. Consume dairy products on a daily basis, mainly yogurt and cheese. |
| 6. Red meat should be consumed in moderation and, if possible, as a part of stews and other recipes. |
| 7. Consume fish abundantly and eggs in moderation. |
| 8. Fresh fruit should be your everyday dessert, and sweets, cakes, and dairy desserts should be consumed only on occasion. |
| 9. Water is the beverage par excellence in the Mediterranean Diet. |
| 10. Be physically active every day since it is just as important as eating well. |
Table 3.
Differences between the traditional Mediterranean diet and the “Western civilization” diet.
Table 3.
Differences between the traditional Mediterranean diet and the “Western civilization” diet.
| Traditional Mediterranean Diet | Western Civilization Diet |
|---|---|
| ● Breastfeeding | ● Adapted milk |
| ● Varied, seasonal fruit | ● Baby food jars and canned fruits |
| ● Vegetables and leafy vegetables | ● Baby food jars and canned vegetables and leafy vegetables |
| ● Pulses and non-processed nuts | ● Canned pulses and dried, fried, or salted nuts |
| ● Minimally processed and fermented whole grains | ● Refined, processed cereals with industrial fermenting agents |
| ● Fermented milk, principally goat’s and sheep’s | ● Whole, processed milks, mainly from cows |
| ● Occasional lean meat, in small quantities | ● High consumption of red, processed meats |
| ● Minimally processed, perishable, fresh, and local foods | ● Non-perishable processed and ultra-processed foods |
| ● Limits on products with added chemicals | ● Presence of chemical agents and enzyme disrupters |
Table 4.
Sample characteristics. The average age is 2.6 years.
| Boys (n = 56) * | Girls (n = 58) * | |
|---|---|---|
| Weight (kg) | 14.93 ± 3.35 | 13.91 ± 3.21 |
| Height (m) | 0.94 ± 0.10 | 0.93 ± 0.11 |
| BMI (kg/m2) | 16.47 ± 1.36 | 15.80 ± 1.29 |
| Fat mass (%) | 14.94 ± 2.67 | 14.90 ± 2.05 |
| Lean mass (%) | 12.61 ± 2.78 | 11.77 ± 2.37 |
* Mean ± standard deviation; BMI: body mass index.
Table 5.
Evolution during the previous year and during the year of treatment.
| Previous Year * | Year of Treatment * | p | |
|---|---|---|---|
| Number of episodes of acute rhinosinusitis (ARS) per child and year | 3.37 ± 1.21 | 0.32 ± 0.47 | 0.01 |
| Number of upper respiratory tract infections (URTI) per child and year | 7.31 ± 1.43 | 2.79 ± 0.67 | 0.01 |
| Degree of involvement of persistent nasal obstruction (PNO): 0 (mild); 1 (moderate); 2 (intense). | 1.89 ± 0.30 | 0.06 ± 0.08 | 0.03 |
| Others bacterial complications of the oropharynx, by child and year | 4.31 ± 0.25 | 0.72 ± 0.31 | 0.02 |
| Emergencies per child and year | 2.17 ± 0.75 | 0.25 ± 0.14 | 0.03 |
| Antibiotics treatment cycles per child and year | 3.71 ±0.67 | 0.46 ±0.28 | 0.01 |
| Number of symptomatic treatment per child and year | 6.82 ±1.26 | 2.94 ±0.89 | 0.02 |
* Mean ± standard deviation.
Table 6.
Anthropometric assessment at the start, after four months, and after one year.
| At the Start of Treatment * | 4 Months of Treatment * | 1 Year of Treatment * | p | |
|---|---|---|---|---|
| BMI (body mass index) | 16.13 ± 1.42 | 15.91 ± 1.23 | 15.80 ± 1.38 | 0.02 |
| Fat mass (%) | 14.91 ± 2.72 | 14.72 ± 2.55 | 14.80 ± 2.39 | 0.02 |
| Lean mass (%) | 12.19 ± 2.49 | 13.00 ± 2.28 | 14.44 ± 2.18 | 0.03 |
* Mean ± standard deviation.
Table 7.
The KIDMED test (%).
| At the Start | After 4 Months | After 1 Year | |
|---|---|---|---|
| One piece of fruit per day | 75.4 | 66.2 | 85.1 |
| One+ piece of fruit per day | 20.2 | 17.7 | 78.9 |
| One vegetable per day | 71.9 | 63.1 | 84.2 |
| Vegetables more than once per day | 10.5 | 9.2 | 63.2 |
| Regularly eats fresh fish (2–3 times/week) | 76.3 | 66.9 | 84.2 |
| Visits fast food restaurant once or more per week | 17.5 | 15.4 | 0.9 |
| Legumes 1–2 times/week | 78.9 | 69.3 | 85.1 |
| Pasta and rice every week | 78.1 | 68.5 | 84.2 |
| Cereal or derivative for breakfast | 81.6 | 71.6 | 84.2 |
| Regularly eats dried fruit and nuts | 14.9 | 13.1 | 42.1 |
| Olive oil used at home | 82.5 | 72.3 | 85.1 |
| No breakfast | 10.5 | 9.2 | 4.4 |
| Dairy at breakfast | 82.5 | 72.3 | 84.2 |
| Factory-baked goods for breakfast | 33.3 | 29.2 | 0.9 |
| Two yoghurts or 40 g cheese/day | 78.1 | 68.5 | 84.2 |
| Sweets and snacks every day | 27.2 | 23.9 | 4.4 |
Table 8.
The traditional Mediterranean diet test (%).
| Start | 4 Months | Year | |
|---|---|---|---|
| Minimum two pieces of fruit every day. | 28.9 | 76.3 | 92.1 |
| Fresh vegetables at every meal, as a first course, or as part of the main course | 32.5 | 58.8 | 71.9 |
| Limited sugar intake (sweetened breakfast cereal, sweetened yoghurts or milkshakes, cakes, soft drinks, sugary biscuits, sweets, ice-cream, etc.). | 12.3 | 72.8 | 80.7 |
| Sporadic use of potatoes (1–2 times/week) and preferably not fried. | 26.3 | 77.2 | 86.0 |
| Enjoys legumes and eats them one or more times a week, not always accompanied by meat. | 23.7 | 69.3 | 79.8 |
| Regular intake of white fish, oily fish, and seafood (2–3 times/week). | 73.7 | 77.2 | 88.6 |
| Consumes whole grains (whole wheat pasta, brown rice, whole wheat bread, etc.) in a controlled way, and limits the consumption of refined flour, such as white bread, to less than 40g per day. | 14.0 | 72.8 | 83.3 |
| Limit the consumption of preservatives and hydrogenated vegetable fats, regularly using unprocessed homemade foods. | 21.9 | 64.9 | 83.3 |
| Dairy: ingested, preferably skimmed in the form of natural yogurt, and preferably goat or sheep cheese, avoiding the use of sugary yogurts, dairy desserts, creams, margarines, ice creams, etc. | 13.2 | 66.7 | 80.7 |
| Only lean processed meats, less than twice per week. | 14.9 | 70.2 | 85.1 |
| Preferably white meat, less than three times per week (lean). | 24.6 | 77.2 | 73.7 |
| 30–50% of your daily menu consists of raw or undercooked foods (fruits, vegetables, greens, soups, purees, raw nuts, extra virgin olive oil, etc.), preferably choosing seasonal ones. | 6.1 | 36.0 | 56.1 |
| Junk food (indoors or outdoors) no more than one time per week. | 37.7 | 78.9 | 80.7 |
| Consumes, as main fats, extra virgin olive oil and raw nuts. Avoids poor quality industrial greases. | 39.5 | 80.7 | 85.1 |
| Has a quality breakfast or lunch. | 35.1 | 60.5 | 84.2 |
| Does not peck between meals. | 23.7 | 58.8 | 88.6 |
| Adapts to the food made at home (family) and alternatives not offered. | 28.9 | 46.5 | 87.7 |
| Mealtimes together, avoiding the television or other technology. | 57.9 | 80.7 | 82.5 |
| Regular physical exercise (running, playing, walking, climbing, etc.) or sport. | 73.7 | 76.3 | 81.6 |
| Gets 7–9 h of sleep daily. | 68.1 | 85.1 | 89.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Calatayud-Sáez, F.M.; Calatayud, B.; Calatayud, A. Effects of the Traditional Mediterranean Diet in Childhood Recurrent Acute Rhinosinusitis. Sinusitis 2021, 5, 101-115. https://doi.org/10.3390/sinusitis5020011
AMA Style
Calatayud-Sáez FM, Calatayud B, Calatayud A. Effects of the Traditional Mediterranean Diet in Childhood Recurrent Acute Rhinosinusitis. Sinusitis. 2021; 5(2):101-115. https://doi.org/10.3390/sinusitis5020011
Chicago/Turabian StyleCalatayud-Sáez, Fernando M., Blanca Calatayud, and Ana Calatayud. 2021. "Effects of the Traditional Mediterranean Diet in Childhood Recurrent Acute Rhinosinusitis" Sinusitis 5, no. 2: 101-115. https://doi.org/10.3390/sinusitis5020011