1. Introduction
Chronic rhinosinusitis (CRS) can be defined broadly as a chronic (>12 weeks duration) inflammatory condition of the nose and paranasal sinus mucosa associated or not with nasal polyposis and it should be recognised irrespective of treatment status [
1]. This disease entity has a broad and vague symptomatology. This can be easily accepted from the fact that the disease involves an anatomically complex area, which is located in the central face and has a close relationship with other important structures. Owing to the area involved in CRS, it is not uncommon in clinical practice to encounter similar symptomatology in other diseases. Thus, attempts to diagnose it with symptomatology alone are futile. There have been infrequent amendments in the defined diagnostic criteria for CRS, and the most updated and widely followed are the recent recommendations for CRS by the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS). The recommendations by AAO-HNS include both subjective and objective parameters of more than a 12-week duration. The subjective component considers two or more of the four main symptoms (anterior and/or posterior mucopurulent discharge, nasal stuffiness, pressure-fullness-pain in face, and hyposmia), and the objective component includes inflammation, which is characterized by one or more of the following: purulent character of mucus/edema present in middle meatus or the ethmoid area, nasal polyps (NPs) or polyps in middle meatus, and/or radiological imaging showing inflamed paranasal sinuses (PNS) [
2,
3,
4].
To evaluate the objective components of CRS diagnosis, diagnostic nasal endoscopy (DNE) and the computed tomography (CT) scan play important roles. CRS affects a significant population worldwide, imposing a huge toll on the human economy as well as on quality of life [
4,
5]. Thus, it is particularly important to define a cost-effective and easily available diagnostic tool for it. The available literature that compares the two modalities on the diagnosing of CRS offers variable opinions [
6,
7,
8]. A meta-analysis of the available literature comparing DNE and CT favors DNE for the accurate qualitative diagnosis of CRS (especially when the Lund–Kennedy endoscopy score is >2); however, it demands further studies [
9]. Thus, in an attempt to supplement the concerned literature, we conducted this study with the aims of assessing the effectiveness of DNE in evaluating CSR and correlating it with the CT of the nose and PNS. We also had an objective to assess the various clinical symptoms in patients presenting with CRS.
2. Material and Methods
2.1. Study Design and Study Population
This cross-sectional study was conducted in the Department of Otorhinolaryngology in a tertiary care teaching hospital, from September 2018 to April 2020. Considering the low specificity (approximately 28.57%) for diagnostic accuracy with 95% confidence level and an 80% power for the detection of a difference of 15%, the minimum required sample size was 76; therefore, we included 80 patients. To conduct this study, ethical clearance was obtained from the Institutional Ethical Committee. Eighty patients, above 18 years of age, who fulfilled the subjective diagnostic criteria for CRS (that is, two or more of the four main symptoms: anterior and/or posterior mucopurulent discharge, nasal stuffiness, pressure-fullness-pain in face, and hyposmia) and gave their consent to participate were included in the study. These patients were referred by primary care physicians and most of them had received some form of medical management. We excluded patients having cystic fibrosis, fungal sinusitis, autoimmune disease, bronchial asthma, or an immuno-compromised state. Pregnant females and patients having a history suggestive of sinonasal surgery/malignancy or facial trauma were also excluded.
2.2. Detailed Methodology
All participants underwent CT of the nose and PNS, as well as DNE. All participants were subjected to non-contrast CT of the nose and PNS and axial, coronal, and sagittal reconstruction images were obtained. Computed tomography of the nose and PNS was then staged with the help of the Lund–Mackay CT scoring system by a radiologist. Involvement of the PNS (frontal, anterior, and posterior ethmoids, sphenoid and maxillary) was evaluated on the basis of opacity and was scored as 0, 1, or 2 for nil, partial, or complete opacification, respectively. The osteomeatal complex was graded as 1 (no obstruction) or 2 (obstruction present) [
10]. Bilateral evaluation was done for all, with the final score equivalent of points added from the right and left sides, which fell in a range from 0 to 24. A Lund–Mackay CT score of 4 or more was defined as the diagnostic evidence of CRS. All the anatomical variations were also noted, but they did not contribute to the score.
Every individual participant was subjected to endoscopic nasal evaluation on the same day of his/her CT evaluation. CT scan was done first and then endoscopy, so that the mucosal changes following endoscopy did not affect the CT findings. DNE (using 0°/30° rigid nasal endoscope) was done in all individuals under local anesthesia using topical 4% Xylocaine and nasal decongestant (xylometazoline/oxymetazoline) by an otorhinolaryngologist, who was kept unaware of the CT results of participants. The findings obtained were scored with the help of a Lund–Kennedy endoscopy system with respect to these three parameters: (1) nasal mucosal edema (0 = absent, 1 = mild to moderate, 2 = polypoid degeneration), (2) secretion (0 = absent, 1 = hyaline, 2 = thick or mucopurulent or both), (3) polyp (0 = absent, 1 = middle meatus only, 2 = nasal cavity extension) [
11]. Evaluation was carried out on a bilateral basis, with the final score equivalent to points added from the right and left sides. A Lund–Kennedy endoscopic score greater than or equal to 2 was defined as the diagnostic evidence of CRS.
Statistical Analysis: Quantitative variables and qualitative variables were compared with the help of a Mann–Whitney test and chi-square test, respectively. For the assessment of correlation and strength of agreement between the Lund–Kennedy and Lund–MacKay scores with the CRS, the Spearman rank correlation coefficient and the inter-rater kappa agreement were utilized. Comparison of the receiver operating characteristic curves of the Lund–MacKay and Lund–Kennedy scores was performed to compare their area under the curves, to predict the CRS. A p-value < 0.05 was taken as statistically significant. SPSS version 23.0 was used for the analysis.
3. Results: The Following Results Were Obtained from this Study
3.1. Demography
Out of 80 participants, 19 (23.75%) were female and 61 (76.25%) were male. The age range for the participants was 18–56 years. Thirty-five (43.75%) patients belonged to age group <30 years, while 33 (41.25%) were in 31–40 years of age group. Age groups of 41–50 and 51–60 years had six (7.50%) patients in each.
3.2. Clinical Presentation
Nasal obstruction was a complaint in a majority (71 or 88.75%) of the patients. Nasal Discharge was present in 58 (72.50%) patients. Hyposmia affected 34 (42.50%) patients and facial pain was a complaint of 16 (20.00%) patients. Patients presented with these symptoms in varying proportions.
Table 1 shows the frequency distribution of presenting complaints of study subjects. A maximum of 33 (41.25%) patients had nasal obstruction with nasal discharge as chief complaints, followed by 17 (21.25%) who complained of nasal obstruction, nasal discharge, and hyposmia together. Only three (3.75%) had all four symptoms (nasal obstruction, nasal discharge, facial pain, and hyposmia).
3.3. CT Evaluation Results of Study Subjects
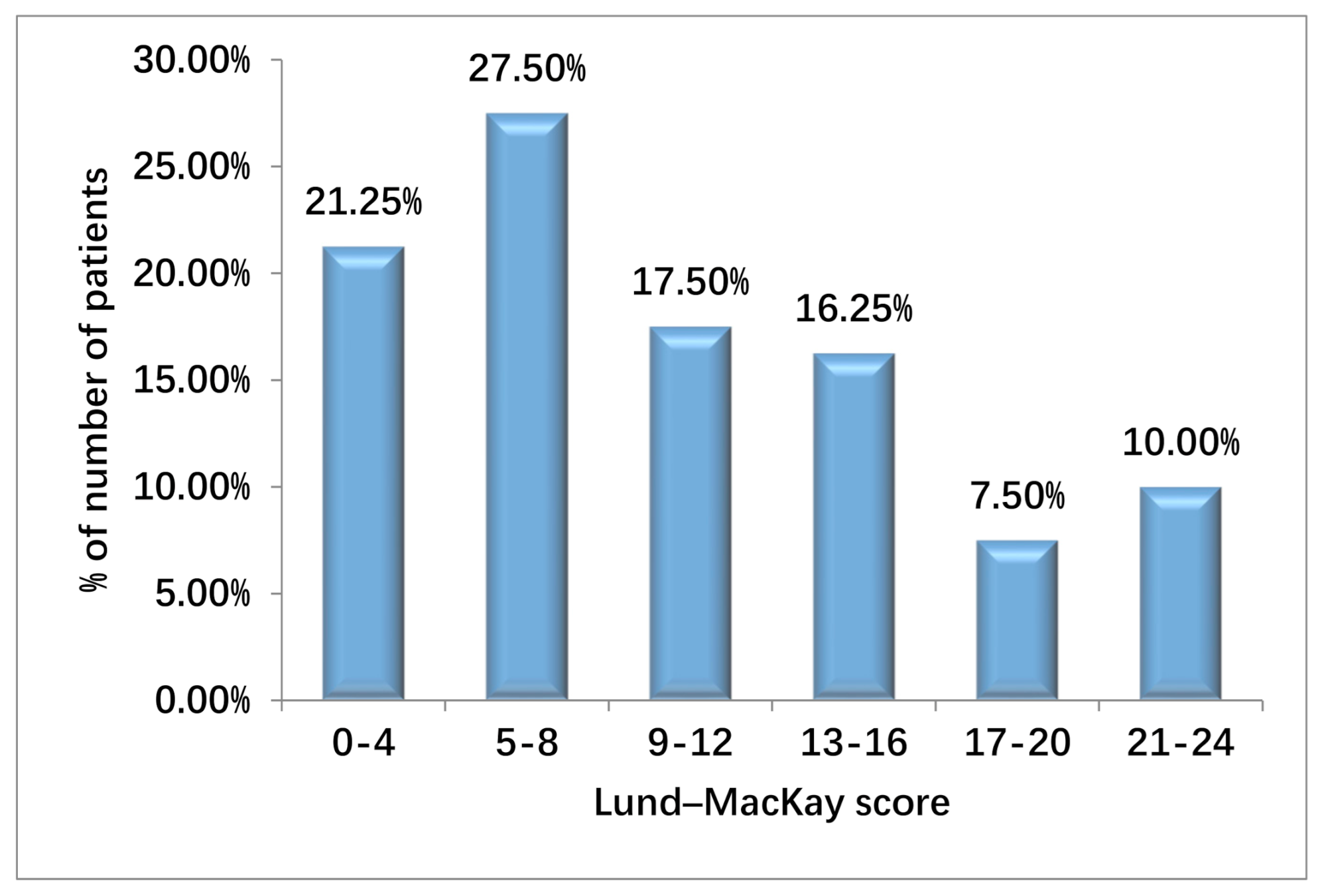
On CT evaluation, participants with Lund–Mackay CT scores < 4 were considered to have negative results for diagnosis of CRS. The remaining patients, who had Lund–Mackey scores equal to or more than 4, were diagnosed as having CRS. Two patients having a score of 4 were therefore included. Twenty-two participants had scores of 5–8; 14 scored in the range of 9–12; and 13 scored within a range of 13–16. Only 6 were given scores between 17 and 20, while 8 participants had maximum scores ranging from 21–24. (See
Figure 1 for the frequency distribution of Lund–MacKay scores of study subjects.) According to the CT findings, the distribution of patients with individual sinus involvement of at least one side each (maxillary sinus, anterior ethmoid sinus, posterior ethmoid sinus, frontal sinus, and sphenoid sinus) is shown in
Table 2. The Mean Lund–MacKay CT score was 9.69 ± 6.99 (mean ± SD). Thus, only 65 participants who were diagnosed as having CRS, based on symptom criteria, were confirmed on CT findings; the remaining 15 had negative CT results when diagnosing for CRS.
3.4. Endoscopy Evaluation Results of Study Subjects
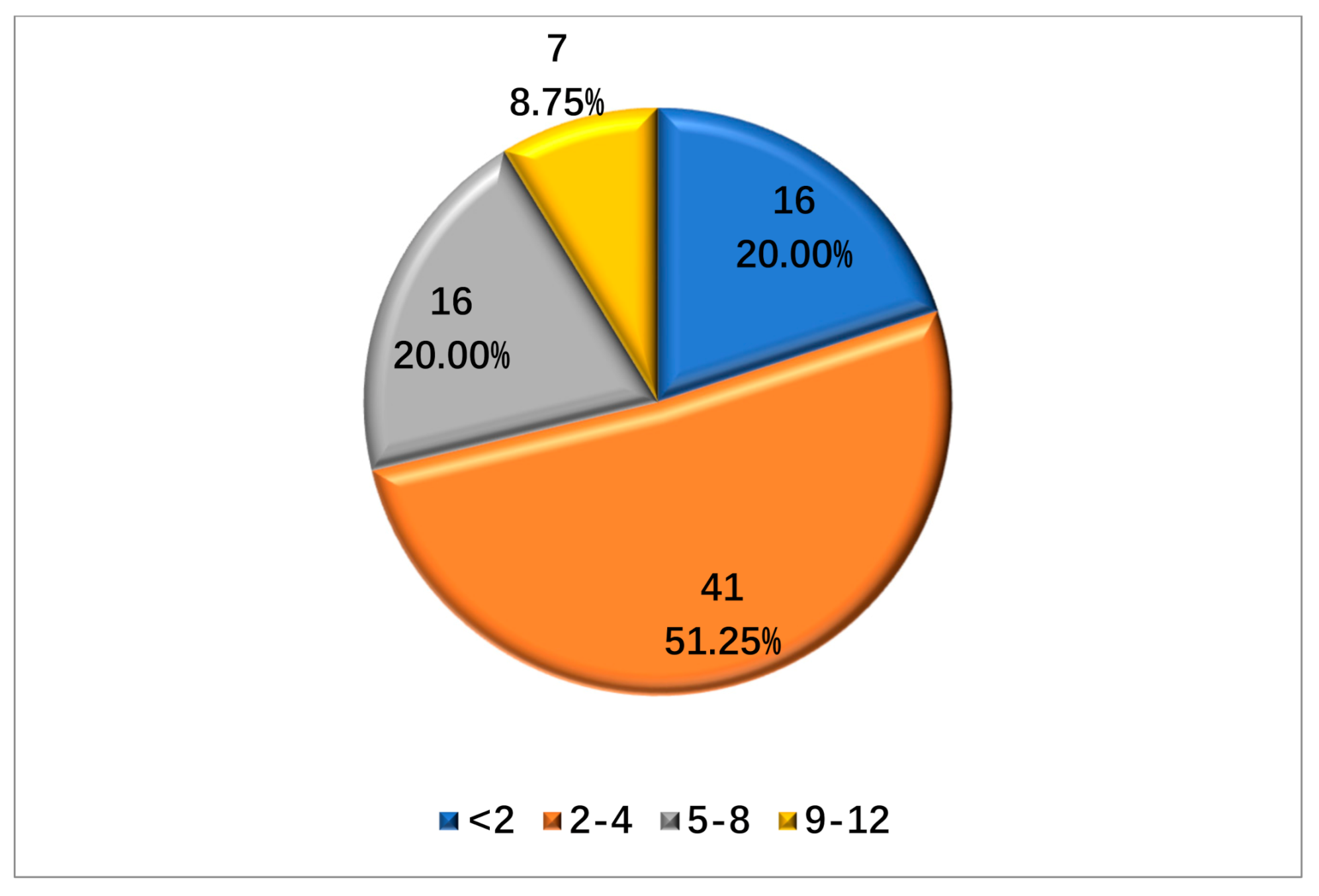
On endoscopic evaluation, 16 (20%) participants had no significant findings and the remaining 64 (80%) had varying combinations of findings. (See
Figure 2 for the distribution of Lund–Kennedy scores of study subjects.) Based on the nasal endoscopy findings, the total number of patients in whom polyps were seen was 44 (55%), while edema was seen in 25 patients (31.25%), and discharge was seen in 37 patients (46.25) (see
Table 3 for the results). The mean score was 3.08 ± 2.69 (mean ± SD). Hence, out of 80 patients who were diagnosed with CRS based on subjective parameters (symptom criteria), only 64 had endoscopic objective criteria as well, to confirm CRS.
3.5. Comparative Assessment of CT and Endoscopy
On assessing the inter-rater kappa agreement between Lund–MacKay CT score and Lund–Kennedy endoscopy score findings, the results suggested that a good agreement existed between CT and endoscopy, with kappa 0.64 and
p-value < 0.0001 (see
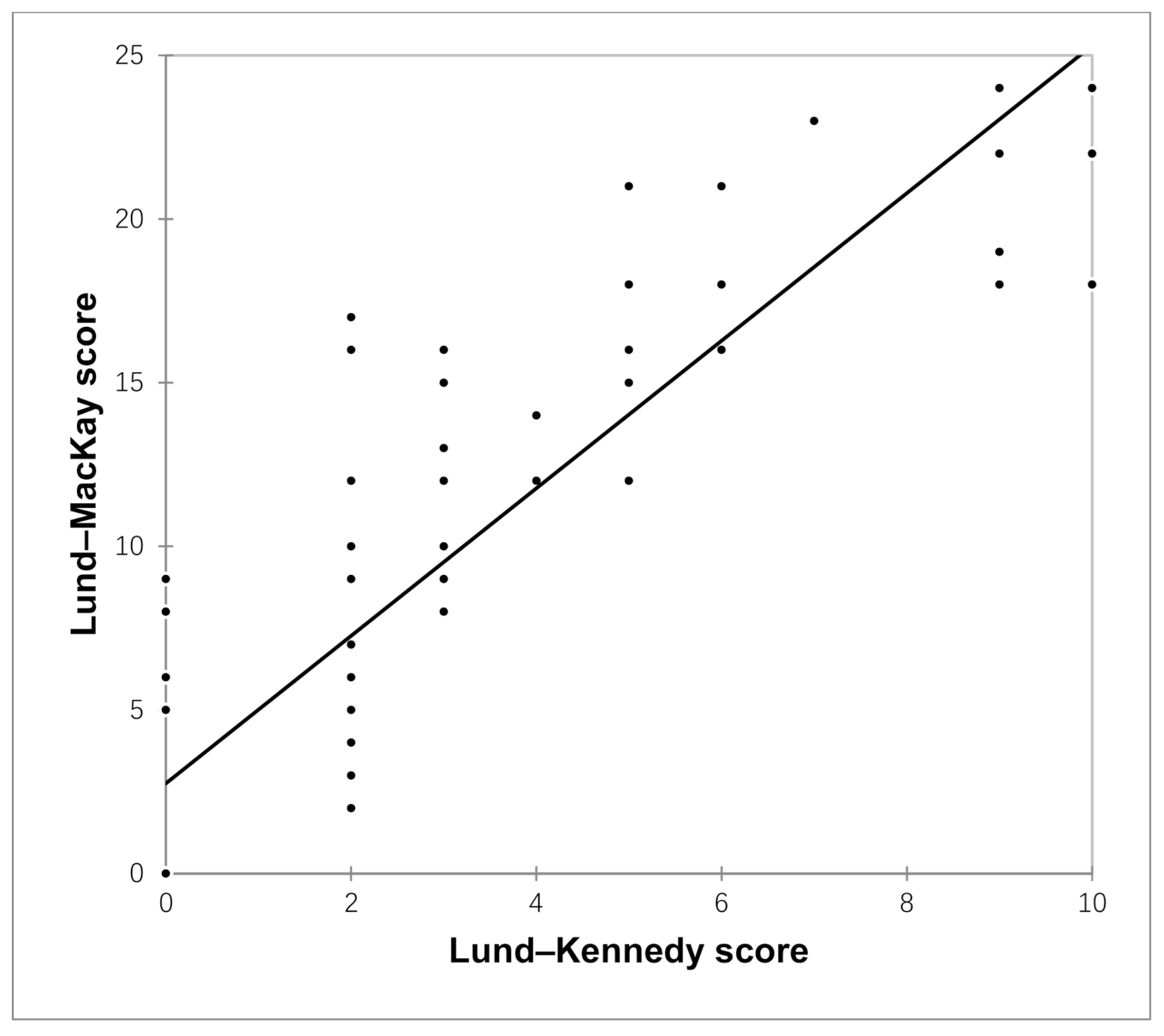
Table 4 for inter-rater kappa agreement between Lund–MacKay CT score and Lund–Kennedy endoscopy score findings). Among 15 patients diagnosed as negative via CT, 11 patients had similar findings with endoscopy. Among 65 patients diagnosed as positive via CT, 60 patients had similar findings with endoscopy. The overall concordance rate was 88.75%, and the overall discordance rate was 11.25%, between CT and Endoscopy. A significant positive correlation was seen between the Lund–Kennedy score and the Lund–MacKay score, with a correlation coefficient of 0.866 (
Figure 3 shows the results).
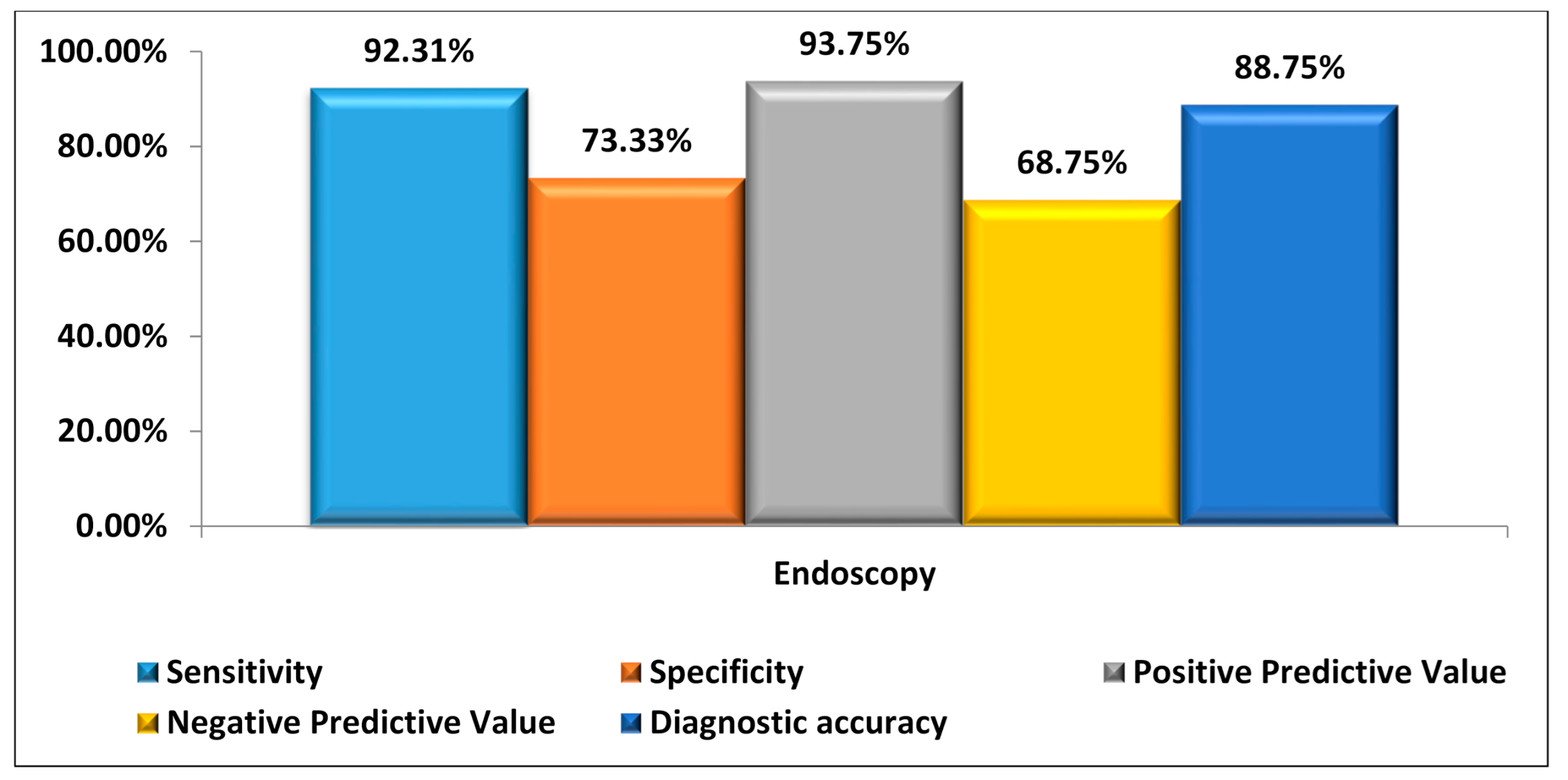
Considering CT to be more accurate and the gold standard for objective diagnosis of CRS, we calculated the sensitivity (92.31%), specificity (73.33%), positive predictive value (93.75%), and negative predictive value (68.75%) of endoscopy (
Figure 4 shows the results). The results of this study suggested that endoscopy, as a diagnostic modality for CRS in comparison with CT, had 88.75% diagnostic accuracy.
4. Discussion
Most patients had nasal obstruction with nasal discharge as the chief complaints in this study population. Other studies assessing the symptomatology of sinonasal diseases showed nasal discharge as the most common complaint, followed by nasal obstruction [
12].
Considering CT as the gold standard for diagnosing CRS, we did a comparative evaluation of endoscopy with it. Our results favored the use of endoscopy as the first-line diagnostic modality for CRS. A high concordance rate (88.75%) supported the use of endoscopy as a cost-effective, alternative tool for diagnosing CRS.
Various studies were conducted in an attempt to compare the diagnostic accuracy of endoscopy and CT, and these studies produced variable results. Goel et al. conducted a study to correlate endoscopy and CT findings in CRS. This study showed a sensitivity of 76.47% and a high specificity of 92.86% with 95% CI. This study concluded that endoscopy was superior for the assessment of localized diseases, such as polyps, pathological secretion, and the condition of mucosa, even as the CT scan gave a better idea of the condition of the PNS and the osteomeatal complex [
13]. Lohiya et al. also conducted a study in an attempt to compare the two modalities in diagnosing CRS. Here also, a high sensitivity of 88.04% was reported; however, the specificity of endoscopy was reported as low (28.57%). This study concluded that for patients who met the guideline symptom criteria for CRS, the diagnostic accuracy could be improved by the addition of nasal endoscopy [
14]. A Lund–Kennedy score equal to or more than 2 was considered as the threshold parameter for CRS diagnosis in both these studies.
In a study by Ferguson, it was suggested that endoscopy had a high specificity (almost 100%) in diagnosing CRS, by confirming the absence of mucopurulence, but they found a low sensitivity (24%) of it in this respect [
15]. Another study also suggested a high specificity of endoscopy in diagnosing CRS by detecting the presence of nasal polyps, purulence, or edematous/congested mucosa. The results showed that negative endoscopic results correlated in 71% of the patients with negative CT results [
7].
Bhattacharyya and Lee, when evaluating the diagnosis of chronic rhinosinusitis based on clinical guidelines and endoscopy, suggested that when DNE was added to the AAO-HNS symptom-based guidelines for CRS, the diagnostic accuracy improved [
16]. A recent meta-analysis conducted by Kim et al. for assessing the usefulness of nasal endoscopy for diagnosing CRS concluded that nasal endoscopy in comparison to CT could diagnose CRS patients with qualitative accuracy. The diagnostic accuracy of nasal endoscopy was seen when CRS was associated with a Lund–Kennedy score equal to or more than 2 [
9].
A CT scan, besides being valuable in defining the objective component of CRS diagnosis, also helps in assessing the extent of the disease and the involvement of the adjacent structures, more so when a surgical intervention (FESS) is planned. Even though CT is known as a gold standard modality for diagnosing CRS, it cannot diagnose the disease with 100% accuracy [
5,
6]. Radiation exposure also remains a concern with CT. On the other hand, due to its minimally invasive nature, DNE remains a preferred modality for direct visualization of the nasal cavities, especially the osteomeatal complex. DNE also has its limitations, as it cannot look beyond certain confinements. Yet, on comparative evaluation of DNE and CT, our study results suggest that DNE can be an effective tool to diagnose CRS.
5. Conclusions
This study concludes that DNE has a high sensitivity (92.31%), specificity (93.75%), and diagnostic accuracy (88.75%) in evaluating CRS when compared with CT. We suggest that nasal endoscopy be used as an early diagnostic tool for the clinical assessment of suspected CRS patients (based on the diagnostic symptom criteria), especially in hospitals with a poor resource setup, heavy patient load, and limited healthcare expenses. DNE helps in decreasing the usage of CT, thereby decreasing the cost and radiation exposure. Therefore, based on symptoms and DNE findings, we can diagnose as well as treat most patients with CRS. Although, in specialty care centers with the availability of CT, it is a more favorable tool for diagnosing the proper extent of the disease, the involved sinuses, and the severity of the disease in each sinus. Even in patients with anatomical defects affecting endoscopic visualization, patients planned for surgery, and patients with refractory disease, despite maximum treatment, computed tomography may be added.
Author Contributions
All authors have significantly contributed in data collection and analysis, study design, result intepretation and literature review. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted after obtaining approval by the Institute Ethics Committee of VMMC and Safdarjung hospital on 31 October 2018.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Ethics Approval
Obtained from the Institutional Ethical Committee.
Consent to Participate
Obtained from all participants.
Consent for Publication
Obtained from all participants.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lanza, D.C.; Kennedy, D.W. Adult rhinosinusitis defined. Otolaryngol. Neck Surg. 1997, 117, S1–S7. [Google Scholar] [CrossRef]
- Benninger, M.S.; Ferguson, B.J.; Hadley, J.A.; Hamilos, D.L.; Jacobs, M.; Kennedy, D.W.; Lanza, D.C.; Marple, B.F.; Osguthorpe, J.D.; Stankiewicz, J.A.; et al. Adult chronic rhinosinusitis: Definitions, diagnosis, epidemiology, and pathophysiology. Otolaryngol. Head Neck Surg. 2003, 129 (Suppl. 3), S1–S32. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, C.; Browne, J.P.; Slack, R.; Lund, V.; Brown, P. The Lund-Mackay staging system for chronic rhinosinusitis: How is it used and what does it predict? Otolaryngol. Neck Surg. 2007, 137, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, R.M.; Andes, D.; Neil, B.; Cheung, D.; Eisenberg, S.; Ganiats, T.G.; Gelzer, A.; Hamilos, D.; Haydon, R.C.; Hudgins, P.A.; et al. Clinical practice guideline: Adult sinusitis. Otolaryngol. Neck Surg. 2007, 137, S1–S31. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, N. Clinical and Symptom Criteria for the Accurate Diagnosis of Chronic Rhinosinusitis. Laryngoscope 2006, 116, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Pokharel, M.; Karki, S.; Shrestha, B.; Shrestha, I.; Amatya, R. Correlations Between Symptoms, Nasal Endoscopy Computed Tomography and Surgical Findings in Patients with Chronic Rhinosinusitis. Kathmandu Univ. Med. J. 2015, 11, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Stankiewicz, J.A.; Chow, J.M. Nasal Endoscopy and the Definition and Diagnosis of Chronic Rhinosinusitis. Otolaryngol. Neck Surg. 2002, 126, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Stankiewicz, J.A.; Chow, J.M. A Diagnostic Dilemma for Chronic Rhinosinusitis: Definition Accuracy and Validity. Am. J. Rhinol. 2002, 16, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Seo, Y.; Kim, K.M.; Lee, S.; Hwang, S.H. Usefulness of Nasal Endoscopy for Diagnosing Patients with Chronic Rhinosinusitis: A Meta-Analysis. Am. J. Rhinol. Allergy 2019, 34, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.G.; Trope, M.; Blasetti, M.; Doghramji, L.; Parasher, A.; Glicksman, J.T.; Kennedy, D.W.; Thaler, E.R.; Cohen, N.A.; Palmer, J.N.; et al. Preoperative Lund-Mackay computed tomography score is associated with preoperative symptom severity and predicts quality-of-life outcome trajectories after sinus surgery. Int. Forum Allergy Rhinol. 2018, 8, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Lund, V.J.; Kennedy, D.W. Staging for rhinosinusitis. Otolaryngol. Neck Surg. 1997, 117, S35–S40. [Google Scholar] [CrossRef]
- Shelkar, R.; Vedi, J.; Patel, S.; Dasgupta, K.; Lanjewar, K. Role of Nasal Endoscopy in Sinonasal Diseases. Int. J. Clin. Rhinol. 2015, 8, 8–11. [Google Scholar] [CrossRef]
- Ashiya Goel, A.; Gupta, V.; Raheja, V.; Goel, S. A study to correlate the endoscopic and CT findings in chronic rhinosinusitis. Indian J. Anat. Surg. Head Neck Brain 2018, 4, 114–117. [Google Scholar]
- Lohiya, S.S.; Patel, S.V.; Pawde, A.M.; Bokare, B.D.; Sakhare, P.T. Comparative Study of Diagnostic Nasal Endoscopy and CT Paranasal Sinuses in Diagnosing Chronic Rhinosinusitis. Indian J. Otolaryngol. Head Neck Surg. 2015, 68, 224–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, B.J.; Narita, M.; Yu, V.L.; Wagener, M.M.; Gwaltney, J.M. Prospective Observational Study of Chronic Rhinosinusitis: Environmental Triggers and Antibiotic Implications. Clin. Infect. Dis. 2011, 54, 62–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharyya, N.; Lee, L.N. Evaluating the diagnosis of chronic rhinosinusitis based on clinical guidelines and endoscopy. Otolaryngol. Neck Surg. 2010, 143, 147–151. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).








{kind=link}
{kind=link}
{kind=link}
{kind=link}