1. Introduction
Prompt and adequate fluid resuscitation is considered essential for survival in patients presenting with greater than 20% TBSA (total body surface area) thermal burns [
1]. Under-resuscitation has been associated with worsened organ failure and increased mortality [
2,
3]. To promote adequate fluid resuscitation in burn patients, clinicians have traditionally used a calculation based on a patient’s weight and TBSA burn size to target a fluid resuscitation goal in the first 24 h. This original formula was developed more than 50 years ago, and calculates a targeted fluid rate at 4 mL/kg/%TBSA administered over 24 h (with the first half of that volume in the first 8 h) [
4].
It has been increasingly recognized, however, that too much fluid resuscitation can be associated with complications in burn victims. These complications include the development of ARDS (acute respiratory distress syndrome), pneumonia, and compartment syndrome [
5,
6]. In 2008, the American Burn Association published practice guidelines that decreased the recommended fluid goal in the first 24 h to the 2–4 mL/kg/%TBSA range. This guideline acknowledged the insufficient evidence to make a strong recommendation regarding an initial fluid rate or type of fluid, but modified the calculation to help reduce the risks of over-resuscitation. The guideline additionally suggested that subsequent fluid management during the first 24 h should be adjusted to achieve a urine output of 0.5–1 cc/kg/h.
The objective of this study was to retrospectively assess the volume of fluids administered in the first 24 h to patients with greater than 20% TBSA burns over a 7.5-year period in a specialized Burn Intensive Care Unit (ICU). This included 4 years before and 3.5 years after a reduction in the targeted fluid goal (from 4 mL/kg/%TBSA to 2 mL/kg/TBSA) was incorporated into the standard resuscitation strategy in this ICU. The study evaluated the impact of this change on fluids received in the first 24 h before and after this change. Additionally, exploratory analyses evaluated the correlation of total fluids received and the type of fluid received with mortality or other secondary outcomes, paying particular attention to either over- or under-resuscitation.
2. Materials and Method
Medical charts of all patients admitted to the Grossman Burn Center with >20% TBSA burns from January 2014 to August 2021 were examined. The Grossman Burn Center is a 22-bed specialized burn unit located near Los Angeles, CA, USA. The data were compiled to record the age, weight, type of burns, time of injury, and percentage of total body surface area involved. The volume and type of fluid given at 24 and 48 h from the onset of injury were noted. ICU length of stay, hospital length of stay, development of pneumonia, acute renal failure, ARDS within one week of the onset of thermal injury, and mortality were also recorded.
2.1. Fluid Resuscitation Protocol
The fluid resuscitation protocol was nurse-driven, with physician input. From 2014–2018, the resuscitation goal was 4 mL/kg/%TBSA within the initial 24 h, which was then changed to 2 mL/kg/%TBSA at the end of 2018, except in cases of electrical burns. The protocol allowed for an increase and decrease in the lactated Ringer’s rate, aiming for a urine output goal of 30–50 mL/h. Albumin could also be ordered, at the discretion of the attending physician, both for difficult resuscitation and to decrease the overall fluid volume, within the first 24 h. The albumin protocol started with 5% albumin at one-third of the hourly fluid resuscitation rate, preferably 10 h after the burn. Albumin boluses could also be utilized as rescue measures, at the physician’s discretion.
2.2. Inhalational Injury
All of the burn patients with suspected inhalational injury (intubated prior to arrival to the burn center, rescued from fire in an enclosed space, with the presence of facial, perioral or nasal burns) underwent bronchoscopy within the first 48 h after sustaining burns. Inhalation injury was confirmed based on presence of carbonaceous deposits and/or erythema in the airways.
2.3. Statistical Analysis
The aforementioned data were compiled in a spreadsheet. For univariate analysis, a Student’s t-test was performed on continuous variables that followed a Gaussian distribution, while the Wilcoxon test was applied if the distribution was not Gaussian. Fisher’s exact test was utilized to test differences in proportions. For multivariate analysis, logistic regression was used if the outcome was discrete, without a time component. For survival analysis, the Cox proportional hazards model was used. For continuous variables, linear regression was used to develop the multivariate model. In multivariate models, we used a feature for approximately every ten cases to prevent overfitting the model. In exploratory analyses, we evaluated the further additional features of interest. In particular, we aimed to explore whether under and over-resuscitation were associated with mortality and ARDS development. In addition, we wanted to investigate the role of albumin administration in these outcomes.
4. Discussion
This study evaluated consecutive admissions of large TBSA burns to an adult burn ICU over a 7.5-year period. Analysis of our demographic data showed a majority of these patients were males. This is consistent with findings from other adult burn ICUs in the United States [
7,
8,
9]. We also noted the majority of the admissions to our burn center were transferred from outside medical facilities, which is not surprising given that our center specializes in the comprehensive treatment of burns.
With regard to the etiology of burns, flame burns were the major cause of severe burns among our patients, with 46% of the patients having a concurrent inhalational injury. The incidence of inhalational injury in this study (46%) is higher than the range of 6–20% typically seen in burn ICUs [
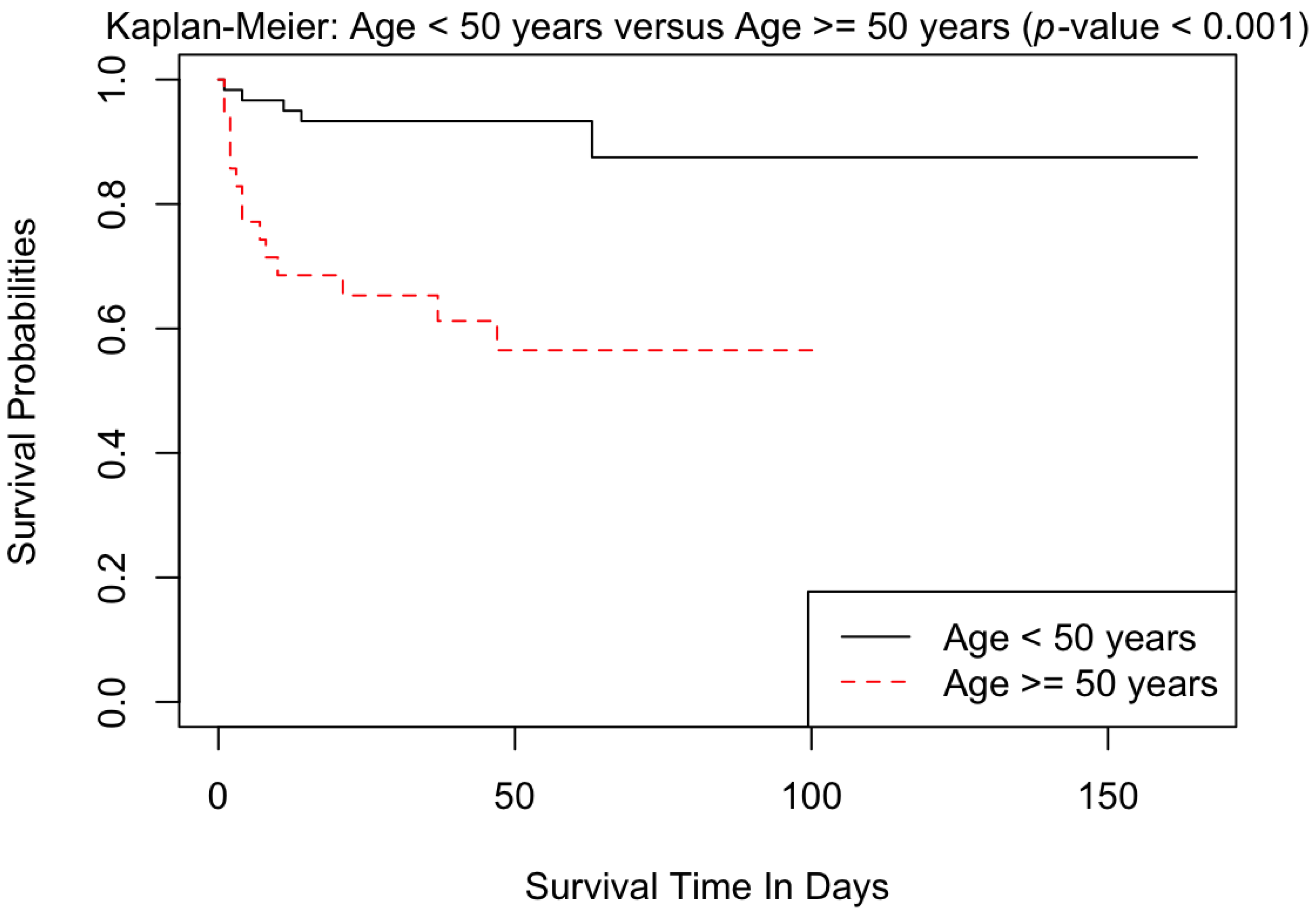
10]. The high rate of inhalational injury observed in this study may be related to the burn’s mechanism, such as fire, which was a frequent cause in this sample. Additionally, patients in this study were older, with the median age being 41 years. Increased age and large TBSA burn size are known risks for developing inhalational injury [
11,
12]. The median length of hospital stay for our patients was 37 days over this time period.
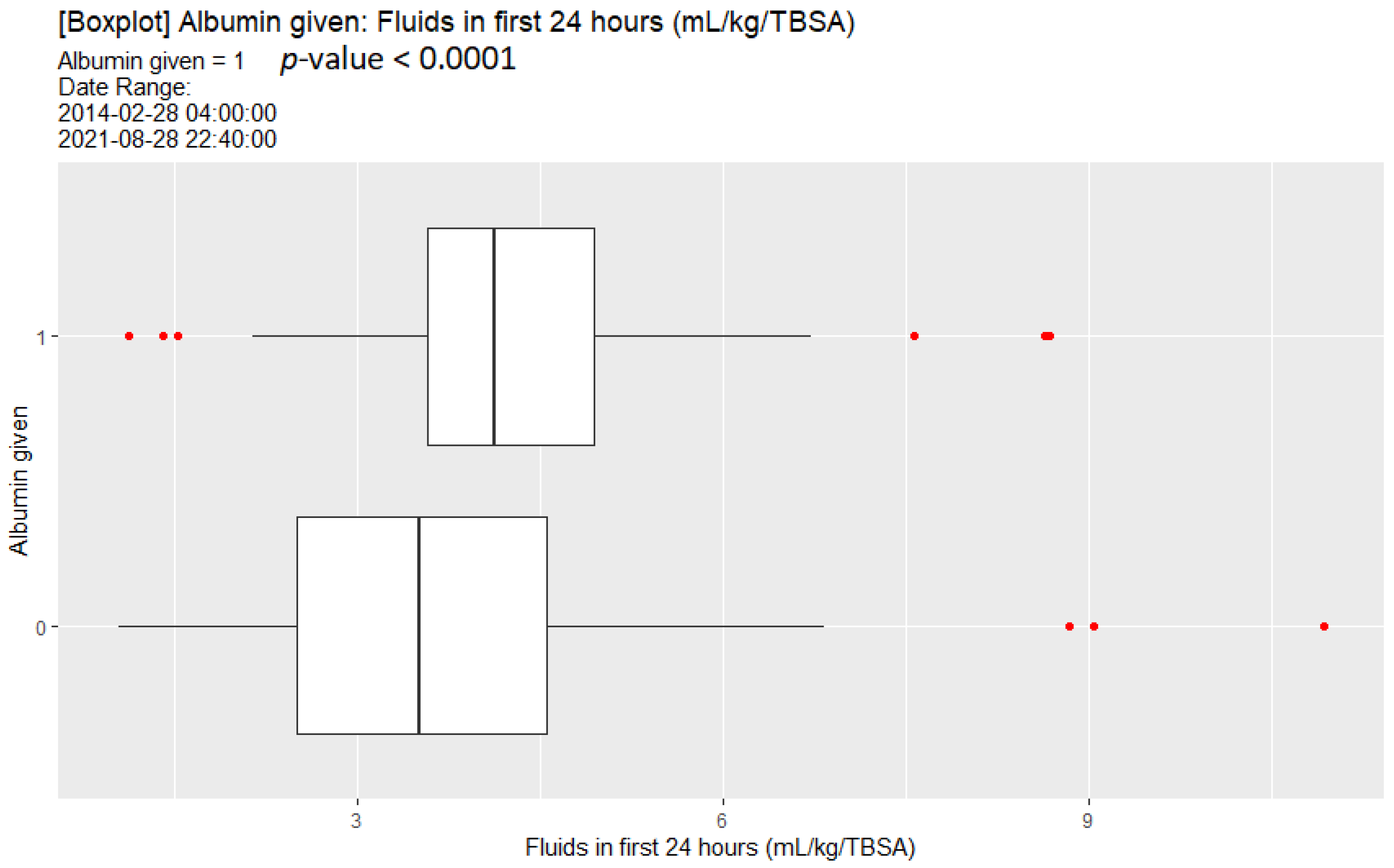
When analyzing the fluids administered to the patients in our ICU during this period, we were surprised that despite changes in our initial fluid resuscitation formula, the median fluid administered to our patients did not change, and remained near 4 mL/kg/%TBSA over the first 24 h. Post implementation of 2 mL/kg X TBSA fluid resuscitation formula, the patients initially received less fluid but because the protocol allowed the nurses to increase the fluid rate for goal UOP of 30–50 cc/h, the patients based on our study ended up receiving the same total amount. Interestingly, the analysis revealed that lighter patients received significantly more fluids than the heavier patients per kilogram, suggesting urine output goals were not adjusted for weight. This is consistent with the resuscitation protocol using an absolute urine output as a clinical goal rather than a urine output per weight-based goal. In addition, there may be barriers, such as nursing staff being hesitant to decrease the resuscitation fluid rate even if the protocol indicates to do so, resulting in overall increased fluid resuscitation. Furthermore, given the high percentage of patients with inhalational injury in this study, the patients may have received more fluid than the level predicted by the initial calculation (which does not adjust for inhalational injury). We also found that the patients receiving albumin received more fluid. We postulate that this may have been because of ongoing clinical deterioration despite adequate fluid resuscitation, with the use of albumin serving as salvage therapy. As such, it may not be that albumin usage is related to increased mortality, but that it serves as a surrogate for decompensation despite adequate fluid resuscitation. We compared the mortality and rate of ARDS and AKI before and after the change in fluid resuscitation goals and found no statistical difference in the outcomes, likely because the group pre and post change in resuscitation goals ended up receiving the same amount of fluid within the first 24 h of their burn injury
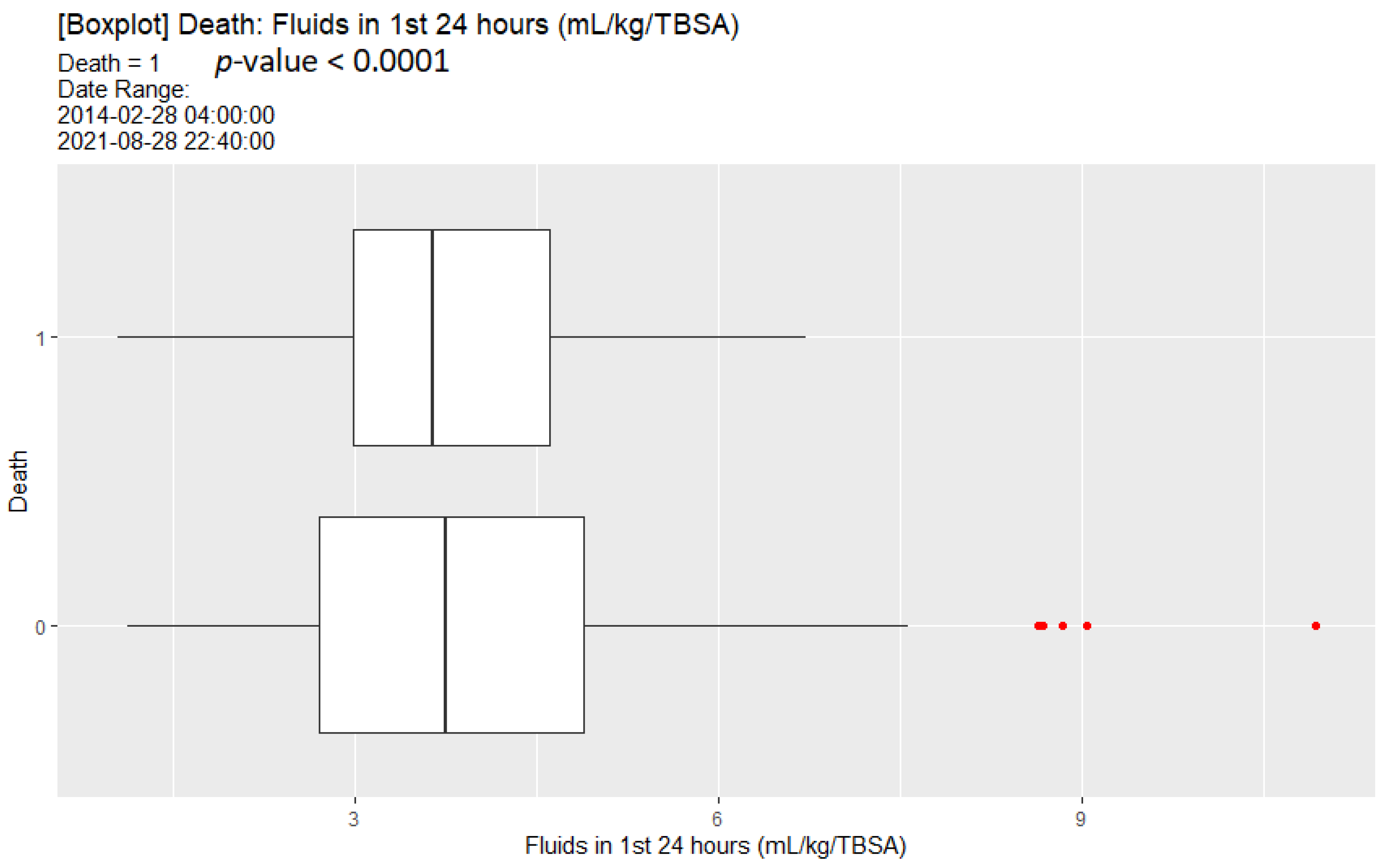
A univariate analysis of our data did show that increased mortality was associated with less fluid resuscitation (although this was still significantly higher than 2 mL/kg/%TBSA). While close to but not statistically significant, multivariate analysis noted an association between under-resuscitation and mortality, but did not find such an association between over-resuscitation and mortality.
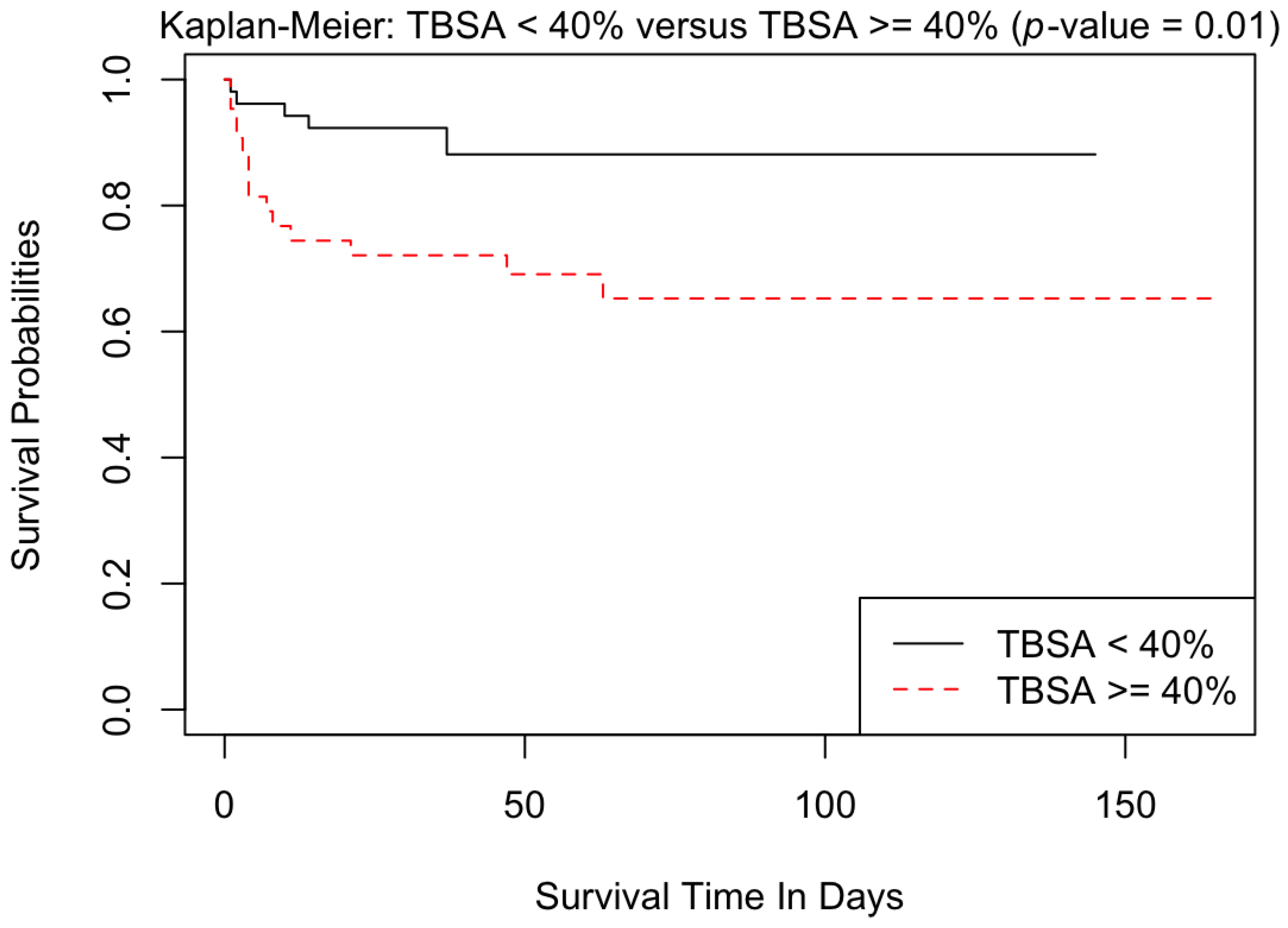
Not surprisingly, increased age, high TBSA % burn, and inhalational injury were all associated with decreased survival in our data. This has been well documented in other studies of adult burn victims [
13]. Patients with more severe burns had increased initial creatinine levels. While our numbers were not sufficient, upon multivariate analysis, acute kidney injury was independently associated with increased mortality. Upon exploratory analysis, we found that albumin administration within the first 24 h was associated with decreased survival; however, the time of albumin administration in the resuscitation course was not analyzed. Given our limited cases, we would consider this result a potential hypothesis-generating event for future studies, rather than a causal inference.
The study looked at both ARDS and pneumonia as possible secondary outcomes from excessive fluid administration. The classification of ARDS used the Berlin definition [
14]. We found that increased TBSA burn and age were associated with the development of ARDS. This supports the role of tissue injury, inflammatory response, and burn shock in the possible genesis of ARDS [
15,
16,
17]. Contrary to other studies [
18,
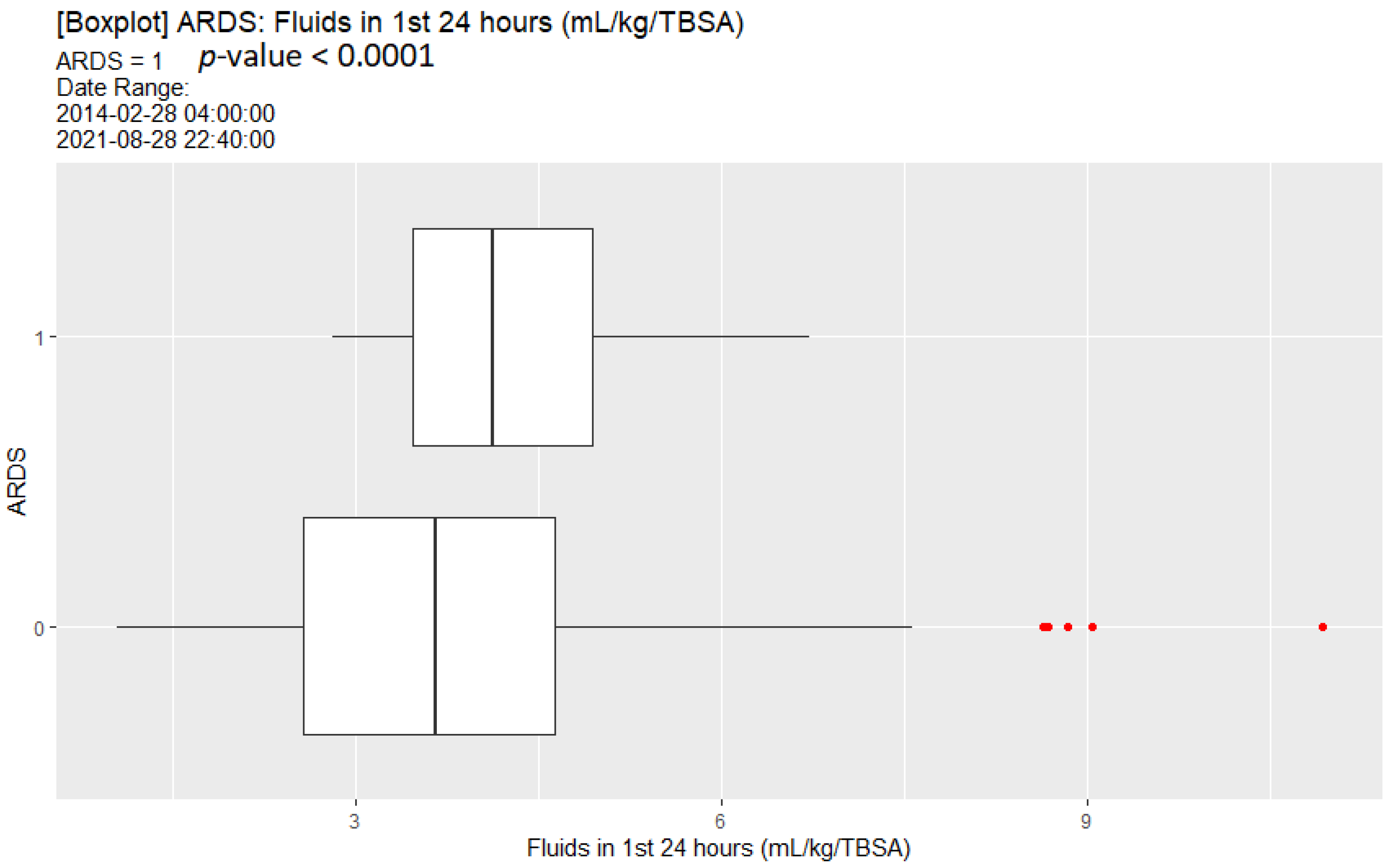
19], the presence of inhalational injury did not appear to be associated with development of ARDS in our patients. We did, however, find a relationship between fluid resuscitation volume and development of ARDS. Patients who received more than twice their predicted volume (2 mL/kg/BSA) within the first 48 h of burn injury were at higher risk of developing ARDS. Other studies have supported the benefit of limiting fluid administration to improve outcomes in ARDS patients in mixed populations of ICU patients [
20,
21]. Excessive fluids are thought to be harmful due to the increased permeability of the pulmonary membranes in this condition.
We did not find that pneumonia was correlated with excessive fluid volume administered early in the hospital course, but we did find that the presence of inhalational injury increased the risk of pneumonia by more than 2-fold within the first week of injury. Several other studies have found an association between pneumonia and the presence of inhalational injuries [
22,
23,
24,
25]. We did not find a statistical correlation between TBSA and pneumonia, however, as has been seen in some of these studies [
23]. It is possible that the high incidence of pneumonia in our sample (53.7%) could be attributed to an over diagnosis, as the criteria defining pneumonia are not specific enough to differentiate it from tracheobronchitis, or the radiographic changes typically seen with smoke inhalational injury alone.
The main limitation of the present study is that it was a single-center study with a relatively small number of patients. Using absolute urine output as a resuscitation goal rather than weight-based urine output is another major limitation of the study. The small sample size might have underestimated the effect of risk factors relevant for the studied outcomes. Furthermore, we did not control for provider preferences in the study. There exists a core of both physicians and providers, and since they often cross-over for each other, we postulate that the care averages out statistically.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}