
Managing Thermal Injuries of the Penis and Scrotum: A Narrative Review

{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Discussion
3.1. Epidemiology
3.2. Anatomic Considerations
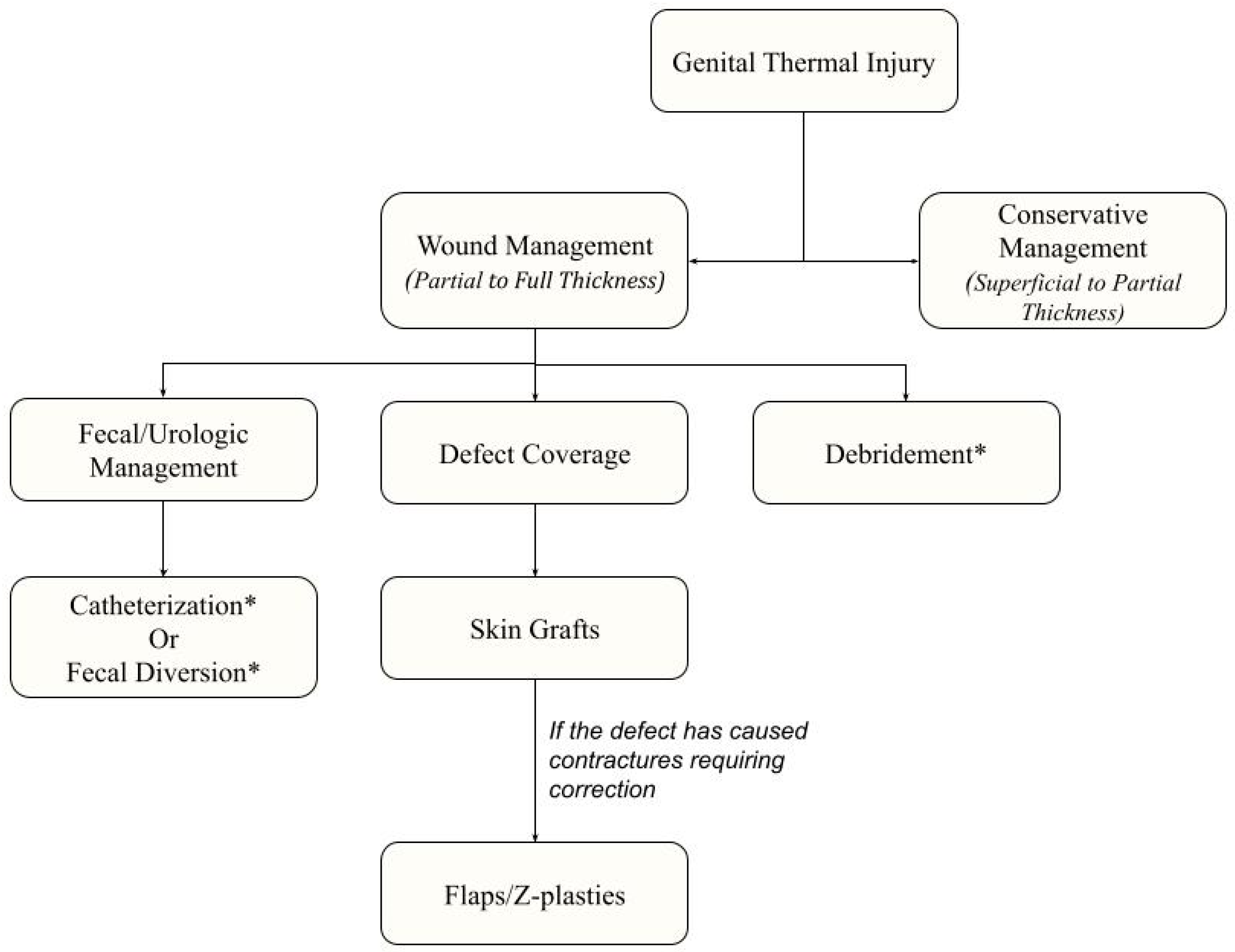
3.3. Acute Management of Genital Burns
3.4. Management of Deep-Dermal Partial or Full Thickness Burns
3.4.1. Debridement
3.4.2. Skin Grafts
3.4.3. Flaps
3.5. Urinary and Fecal Diversion
3.6. Management of Frostbite
3.7. Long-Term Sequelae
3.8. Future Directions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Center for Health Statistics. National Hospital Ambulatory Medical Care Survey: 2011 Emergency Department Summary Tables. 2011. Available online: http://www.census.gov/population/metro/ (accessed on 30 December 2022).
- Angel, C.; Shu, T.; French, D.; Orihuela, E.; Lukefahr, J.; Herndon, D.N. Genital and perineal burns in children: 10 years of experience at a major burn center. J. Pediatr. Surg. 2002, 37, 99–103. [Google Scholar] [CrossRef]
- McDougal, W.S.; Peterson, H.D.; Pruitt, B.A.; Persky, L. The Thermally Injured Perineum. J. Urol. 1979, 121, 320–323. [Google Scholar] [CrossRef]
- Harpole, B.G.; Wibbenmeyer, L.A.; Erickson, B.A. Genital Burns in the National Burn Repository: Incidence, Etiology, and Impact on Morbidity and Mortality. Urology 2014, 83, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Baba, P.U.F.; Shah, R.A.; Rasool, A.; Kaul, A.; Wani, A.H. Perineal burns: Epidemiology, severity factors, management issues and outcome. Burns Open 2022, 6, 97–104. [Google Scholar] [CrossRef]
- 2016 National Burn Repository. American Burn Association: National Burn Repository. 2016. Available online: www.ameriburn.org (accessed on 17 April 2023).
- Brusselaers, N.; Monstrey, S.; Vogelaers, D.; Hoste, E.; Blot, S. Severe burn injury in europe: A systematic review of the incidence, etiology, morbidity, and mortality. Crit. Care 2010, 14, R188. [Google Scholar] [CrossRef]
- Stylianou, N.; Buchan, I.; Dunn, K.W. A review of the international Burn Injury Database (iBID) for England and Wales: Descriptive analysis of burn injuries 2003–2011 A review of the international Burn Injury Database (iBID) for England and Wales: Descriptive analysis of burn injuries. BMJ Open 2003, 5, 6184. [Google Scholar] [CrossRef]
- Tresh, A.; Baradaran, N.; Gaither, T.W.; Fergus, K.B.; Liaw, A.; Balakrishnan, A.; Hampson, L.A.; Breyer, B.N. Genital burns in the United States: Disproportionate prevalence in the pediatric population. Burns 2018, 44, 1366–1371. [Google Scholar] [CrossRef] [PubMed]
- Peck, M.D.; Boileau, M.A.; Grube, B.J.; Heimbach, D.M. The Management of Burns to the Perineum and Genitals. J. Burn Care Rehabil. 1990, 11, 54–56. [Google Scholar] [CrossRef]
- Laitung, J.K.G.; Luthra, P.K. Isolated penile burns: A plea for early excision. Br. J. Plast. Surg. 1988, 41, 644–648. [Google Scholar] [CrossRef]
- American Burn Association. Immediate Consultation with Consideration for Transfer Consultation Recommendation. 2022. Available online: https://ameriburn.org/wp-content/uploads/2023/01/one-page-guidelines-for-burn-patient-referral-16.pdf (accessed on 4 April 2023).
- Burns. MedlinePlus Medical Encyclopedia. Available online: https://medlineplus.gov/ency/article/000030.htm (accessed on 29 November 2022).
- Michielsen, D.; Van Hee, R.; Neetens, C.; Lafaire, C.; Peeters, R. Burns to the Genitalia and the Perineum. J. Urol. 1998, 159, 418–419. [Google Scholar] [CrossRef] [PubMed]
- Ismail, E.; Aly, M.; Huang, T. Management of Burn Injuries of the Perineum. In Total Burn Care, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 55, pp. 609–617. Available online: https://www-clinicalkey-com.ezp1.lib.umn.edu/#!/content/book/3-s2.0-B9780323476614000551?scrollTo=%23hl0000200 (accessed on 28 November 2022).
- Bandi, G.; Santucci, R.A. Controversies in the management of male external genitourinary trauma. J. Trauma Inj. Infect. Crit. Care 2004, 56, 1362–1370. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.; Panthak, Z.J. Tangential excision of burn wounds. J. Craniofac. Surg. 2008, 19, 1056–1060. [Google Scholar] [CrossRef]
- Van Der Horst, C.; Martinez Portillo, F.J.; Seif, C.; Growth, W.; Jünemann, K.P. Male genital injury: Diagnostics and treatment. BJU Int. 2004, 93, 927–930. [Google Scholar] [CrossRef]
- Abel, N.J.; Klaassen, Z.; Mansour, E.H.; Marano, M.A.; Petrone, S.J.; Houng, A.P.; Chamberlain, R.S. Clinical outcome analysis of male and female genital burn injuries: A 15-year experience at a Level-1 Burn Center. Int. J. Urol. 2012, 19, 351–358. [Google Scholar] [CrossRef]
- Schulz, A.; Ribitsch, B.; Fuchs, P.C.; Lipensky, A.; Schiefer, J.L. Treatment of Genital Burn Injuries: Traditional Procedures and New Techniques. Adv. Ski. Wound Care. 2018, 31, 314–321. [Google Scholar] [CrossRef]
- Jaskille, A.D.; Shupp, J.W.; Jeng, J.C.; Jordan, M.H. Use of Integra® in the Treatment of Third Degree Burns to the Penile Shaft: A Case Series with 6-Month Follow-up. J. Burn. Care Res. 2009, 30, 524–528. [Google Scholar] [CrossRef] [PubMed]
- Alghanem, A.A.; McCauley, R.L.; Robson, M.C.; Rutan, R.L.; Herndon, D.N. Management of pediatric perineal and genital burns: Twenty-year review. J. Burn Care Rehabil. 1990, 11, 308–311. [Google Scholar] [CrossRef]
- Thakar, H.J.; Dugi, D.D. Skin grafting of the penis. Urol. Clin. N. Am. 2013, 40, 439–448. [Google Scholar] [CrossRef]
- Patino, G.; Zheng, M.Y.; Breyer, B.N.; Cohen, A.J. Skin Grafting Applications in Urology. Rev. Urol. 2019, 21, 8. [Google Scholar] [PubMed]
- Zhao, J.C.; Xian, C.J.; Yu, J.A.; Shi, K. Reconstruction of infected and denuded scrotum and penis by combined application of negative pressure wound therapy and split-thickness skin grafting. Int. Wound J. 2013, 10, 407–410. [Google Scholar] [CrossRef]
- Tan, B.K.; Rasheed, M.Z.; Wu, W.T.L. Scrotal reconstruction by testicular apposition and wrap-around skin grafting. J. Plast. Reconstr. Aesthet. Surg. 2011, 64, 944–948. [Google Scholar] [CrossRef]
- Maguiña, P.; Palmieri, T.L.; Greenhalgh, D.G. Split thickness skin grafting for recreation of the scrotum following Fournier’s gangrene. Burns 2003, 29, 857–862. [Google Scholar] [CrossRef]
- Furr, J.; Culkin, D. Injury to the male external genitalia: A comprehensive review. Int. Urol. Nephrol. 2017, 49, 553–561. [Google Scholar] [CrossRef]
- Fletcher, J.L.; Caterson, E.J.; Hale, R.G.; Cancio, L.C.; Renz, E.M.; Chan, R.K. Characterization of Skin Allograft Use in Thermal Injury. J. Burn. Care Res. 2013, 34, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Horch, R.E.; Jeschke, M.G.; Spilker, G.; Herndon, D.N.; Kopp, J. Treatment of second degree facial burns with allografts—Preliminary results. Burns 2005, 31, 597–602. [Google Scholar] [CrossRef]
- Puyana, S.; Ruiz, S.; Elkbuli, A.; Bernal, E.; McKenney, M.; Young, E.; Lim, R.; Askari, M.; Mir, H. Comparison Between Human Amniotic/Chorionic Membrane and Cryopreserved Allografts in the Treatment of Genital Burns. Ann. Plast. Surg. 2020, 85, 618–621. [Google Scholar] [CrossRef] [PubMed]
- Loss, M.; Wedler, V.; Künzi, W.; Meuli-Simmen, C.; Meyer, V.E. Artificial skin, split-thickness autograft and cultured autologous keratinocytes combined to treat a severe burn injury of 93% of TBSA. Burns 2000, 26, 644–652. [Google Scholar] [CrossRef]
- Sheridan, R.L.; Hegarty, M.; Tompkins, R.G.; Burke, J.F. Artificial skin in massive burns—Results to ten years. Eur. J. Plast. Surg. 1994, 17, 91–93. [Google Scholar] [CrossRef]
- Grishkevich, V.M. Burned perineum reconstruction: A new approach. J. Burn Care Res. 2009, 30, 620–624. [Google Scholar] [CrossRef]
- Maurya, R.; Mir, M.A.; Mahajan, S. Various Options for Scrotal Reconstruction: A Prospective Observational Study. Cureus 2022, 14, e22671. [Google Scholar] [CrossRef]
- Karian, L.S.; Chung, S.Y.; Lee, E.S. Reconstruction of Defects After Fournier Gangrene: A Systematic Review. Eplasty 2015, 15, e18. [Google Scholar] [PubMed]
- Hsu, H.; Lin, C.M.; Sun, T.B.; Cheng, L.F.; Chien, S.H. Unilateral gracilis myofasciocutaneous advancement flap for single stage reconstruction of scrotal and perineal defects. J. Plast. Reconstr. Aesthet. Surg. 2007, 60, 1055–1059. [Google Scholar] [CrossRef]
- Guo, L.; Zhang, M.; Zeng, J.; Liang, P.; Zhang, P.; Huang, X. Utilities of scrotal flap for reconstruction of penile skin defects after severe burn injury. Int. Urol. Nephrol. 2017, 49, 1593–1603. [Google Scholar] [CrossRef] [PubMed]
- Karaçal, N.; Livaoglu, M.; Kutlu, N.; Arvas, L. Scrotum reconstruction with neurovascular pedicled pudendal thigh flaps. Urology 2007, 70, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, F.M.; Sinha, J.K.; Choudhury, A.K.; Bhattacharya, V. Repair of burns of the scrotum using a gracilis myocutaneous flap. Burns 1989, 15, 181–182. [Google Scholar] [CrossRef]
- El-Khatib, H.A. V-Y fasciocutaneous pudendal thigh flap for repair of perineum and genital region after necrotizing fasciitis: Modification and new indication. Ann. Plast. Surg. 2002, 48, 370–375. [Google Scholar] [CrossRef]
- Lin, C.-T.; Chang, S.-C.; Chen, S.-G.; Tzeng, Y.-S. Reconstruction of perineoscrotal defects in Fournier’s gangrene with pedicle anterolateral thigh perforator flap. ANZ J. Surg. 2016, 86, 1052–1055. [Google Scholar] [CrossRef]
- Spyropoulou, G.A.; Jeng, S.F.; Demiri, E.; Dionyssopoulos, A.; Feng, K.M. Reconstruction of perineoscrotal and vaginal defects with pedicled anterolateral thigh flap. Urology 2013, 82, 461–465. [Google Scholar] [CrossRef]
- Riva, F.M.G.; Tan, N.C.; Liu, K.W.; Hsieh, C.H.; Jeng, S.F. Anteromedial thigh perforator free flap: Report of 41 consecutive flaps and donor-site morbidity evaluation. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 1405–1414. [Google Scholar] [CrossRef]
- Wang, A.M.Q.; Tsang, V.; Mankowski, P.; Demsey, D.; Kavanagh, A.; Genoway, K. Outcomes Following Gender Affirming Phalloplasty: A Systematic Review and Meta-Analysis. Sex. Med. Rev. 2022, 10, 499–512. [Google Scholar] [CrossRef]
- Casoli, V.; Verolino, P.; Castede, J.C.; Pelissier, P.; Martin, D.; Baudet, J. One-stage complete phalloplasty with forearm free flap after severe electrical burns. Plast. Reconstr. Surg. 2004, 113, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Nozaki, M.; Morioka, K.; Huang, T.T. Penile reconstruction: Combined use of an innervated forearm osteocutaneous flap and big toe pulp. Plast. Reconstr. Surg. 1999, 104, 1054–1058. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Fu, J.P.; Chen, T.M.; Chen, S.G. Reconstruction of scrotal and perineal defects in Fournier’s gangrene. J. Plast. Reconstr. Aesthet. Surg. 2011, 64, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Jordan, G.H.; Gilbert, D.A. Male Genital Trauma. Clin. Plast. Surg. 1988, 15, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Mosier, M.; Gibran, N. Surgical Excision of the Burn Wound. In Clinics in Plastic Surgery, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2009; Volume 36, pp. 617–625. [Google Scholar]
- Igawa, Y.; Wyndaele, J.J.; Nishizawa, O. Catheterization: Possible complications and their prevention and treatment. Int. J. Urol. 2008, 15, 481–485. [Google Scholar] [CrossRef]
- Thomsen, T.W.; Setnik, G.S. Male Urethral Catheterization. N. Engl. J. Med. 2006, 354, e22. [Google Scholar] [CrossRef]
- Bordes, J.; Le Floch, R.; Bourdais, L.; Gamelin, A.; Lebreton, F.; Perro, G. Perineal burn care: French working group recommendations. Burns 2013, 40, 655–663. [Google Scholar] [CrossRef]
- Farroha, A.; Frew, Q.; Philp, B.; Dziewulski, P. Improvement of survival in patients with extensive burns involving the perineum with use of a faecal management system. Ann. Burns Fire Disasters 2014, 27, 14. [Google Scholar]
- Mohr, W.; Jenabzadeh, K.; Ahrenholz, D. Cold Injury. In Hand Clinics, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2009; Volume 25, pp. 481–496. [Google Scholar]
- Travis, S.; Roberts, D. Arctic willy. BMJ 1989, 299, 1573. [Google Scholar] [CrossRef]
- Handford, C.; Thomas, O.; Imray, C.H.E.; Bs, M.B. Frostbite. Emerg. Med. Clin. North Am. 2017, 35, 281–299. [Google Scholar] [CrossRef]
- Murch, S. Arctic willy. BMJ 1990, 300, 263. [Google Scholar] [CrossRef] [PubMed]
- Hershkowitz, M. Penile Frostbite, an Unforeseen Hazard of Jogging. N. Engl. J. Med. 2010, 296, 178. [Google Scholar] [CrossRef]
- Kurosaki, Y.; Negi, O.; Takamori, K.; Suga, Y. Severe genital frostbite due to improper use of an aerosol spray: A case of raising awareness of the risk of skin necrosis with aerosol propellants. J. Dermatol. 2019, 46, e247–e248. [Google Scholar] [CrossRef]
- Druery, M.; Brown, T.L.H.; Muller, M. Long term functional outcomes and quality of life following severe burn injury. Burns 2005, 31, 692–695. [Google Scholar] [CrossRef] [PubMed]
- Michielsen, D.P.J.; Lafaire, C. Management of genital burns: A review. Int. J. Urol. 2010, 17, 755–758. [Google Scholar] [CrossRef]
- Sajad, W.; Hamid, R. Outcome of Split Thickness Skin Grafting and Multiple Z-Plasties in Postburn Contractures of Groin and Perineum: A 15-Year Experience. Plast. Surg. Int. 2014, 2014, 358526. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.J.; Brandes, S.B. Advances in Diagnosis and Management of Genital Injuries. Urol. Clin. NA 2013, 40, 427–438. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tople, T.; Skokan, A.; Ettinger, R.; Morrison, S. Managing Thermal Injuries of the Penis and Scrotum: A Narrative Review. Eur. Burn J. 2023, 4, 184-194. https://doi.org/10.3390/ebj4020016
Tople T, Skokan A, Ettinger R, Morrison S. Managing Thermal Injuries of the Penis and Scrotum: A Narrative Review. European Burn Journal. 2023; 4(2):184-194. https://doi.org/10.3390/ebj4020016
Chicago/Turabian StyleTople, Tannon, Alexander Skokan, Russell Ettinger, and Shane Morrison. 2023. "Managing Thermal Injuries of the Penis and Scrotum: A Narrative Review" European Burn Journal 4, no. 2: 184-194. https://doi.org/10.3390/ebj4020016