
Venous Thromboembolism in Severe Burns Patients with Intravascular Warming Catheter: A Retrospective Cohort Study
 , and
, and
Abstract
:1. Introduction
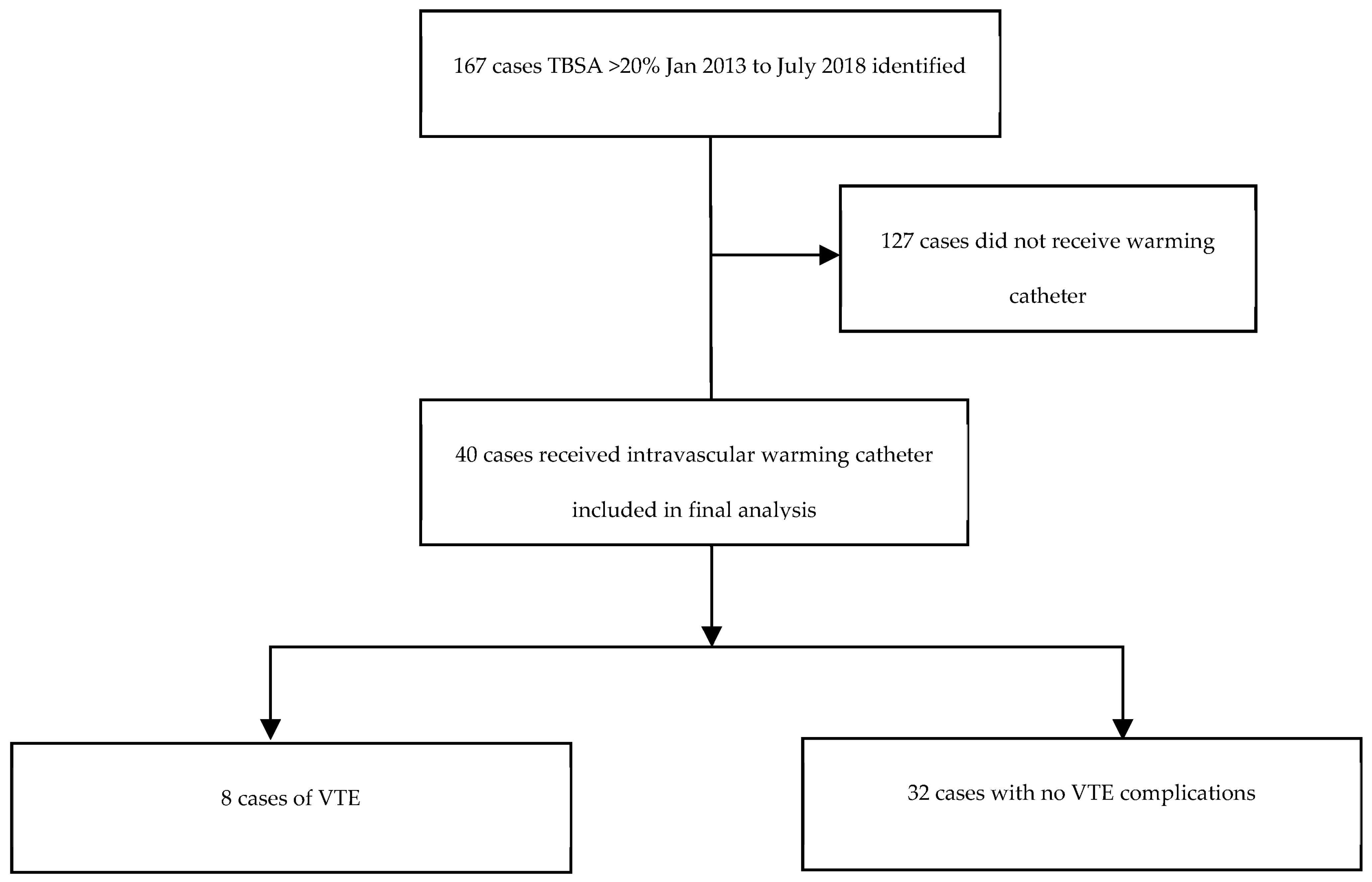
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sessler, D.I. Perioperative thermoregulation and heat balance. Lancet 2016, 387, 2655–2664. [Google Scholar] [CrossRef] [PubMed]
- Perlman, R.; Callum, J.; Laflamme, C.; Tien, H.; Nascimento, B.; Beckett, A.; Alam, A. A recommended early goal-directed management guideline for the prevention of hypothermia-related transfusion, morbidity, and mortality in severely injured trauma patients. Crit. Care 2016, 20, 107. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, J.A.; Rowan, M.P.; Driscoll, I.R.; Chan, R.K.; Chung, K.K. Perioperative Temperature Management During Burn Care. J. Burn Care Res. 2017, 38, e277–e283. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.S.; Rodriguez, L.I.; Quintana, O.D. Use of a Warming Catheter to Achieve Normothermia in Large Burns. J. Burn Care Res. 2013, 34, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Prunet, B.; Asencio, Y.; Lacroix, G.; Bordes, J.; Montcriol, A.; D’Aranda, E.; Pradier, J.-P.; Dantzer, E.; Meaudre, E.; Goutorbe, P.; et al. Maintenance of normothermia during burn surgery with an intravascular temperature control system: A non-randomised controlled trial. Injury 2012, 43, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Prunet, B.; Lacroix, G.; Bordes, J.; Poyet, R.; D’Aranda, E.; Goutorbe, P. Catheter related venous thrombosis with cooling and warming catheters: Two case reports. Cases J. 2009, 2, 8857. [Google Scholar] [CrossRef] [PubMed]
- Gierman, J.L.; Shutze Sr, W.P.; Pearl, G.J.; Foreman, M.L.; Hohmann, S.E.; Shutze, W.P., Jr. Thermoregulatory catheter-associated inferior vena cava thrombus. Bayl. Univ. Med. Cent. Proc. 2013, 26, 100–102. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, H.K.; O’Donovan, S.; Yip, H.; Clements, W.; Koukounaras, J.; Goh, G.S.; Moriarty, H.K.; Goh, G.S. A warning for warming catheters: Interventional radiology’s role. Diagn. Interv. Radiol. 2020, 26, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Simosa, H.F.; Petersen, D.J.; Agarwal, S.K.; Burke, P.A.; Hirsch, E.F. Increased Risk of Deep Venous Thrombosis with Endovascular Cooling in Patients with Traumatic Head Injury. Am. Surg. 2007, 75, 461–464. [Google Scholar] [CrossRef]
- Maze, R.; Le May, M.R.; Froeschl, M.; Hazra, S.K.; Wells, P.S.; Osborne, C.; Labinaz, M.; Hibbert, B.; So, D.Y.F. Endovascular cooling catheter related thrombosis in patients undergoing therapeutic hypothermia for out of hospital cardiac arrest. Resuscitation 2014, 85, 1354–1358. [Google Scholar] [CrossRef] [PubMed]
- Joynt, G.M.; Kew, J.; Gomersall, C.D.; Leung, V.Y.F.; Liu, E.K.H. Deep Venous Thrombosis Caused by Femoral Venous Catheters in Critically Ill Adult Patients. Chest 2000, 117, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Vota, A.; Honig, J.; Chawla, L.; Satalin, M.; Jones, E.; Seneff, M. Intravascular Heat Exchange Femoral Catheters and Deep Vein Thrombosis Formation. Crit. Care Med. 2012, 40, U291–U292. [Google Scholar] [CrossRef]
- Taylor, E.E.; Carroll, J.P.; Lovitt, M.A.; Petrey, L.B.; Gray, P.E.; Mastropieri, C.J.; Foreman, M.L. Active Intravascular Rewarming for Hypothermia Associated with Traumatic Injury: Early Experience with a New Technique. Bayl. Univ. Med. Cent. Proc. 2007, 20, 2–8. [Google Scholar] [CrossRef]
- Nielson, C.B.; Duethman, N.C.; Howard, J.M.; Moncure, M.; Wood, J.G. Burns: Pathophysiology of Systemic Complications and Current Management. J. Burn Care Res. 2017, 38, e469–e481. [Google Scholar] [CrossRef] [PubMed]
- King, D.R.; Namias, N.; Andrews, D.M. Coagulation abnormalities following thermal injury. Blood Coagul. Fibrinolysis 2010, 21, 666–669. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.; Harms, K.-A.; Paul, E.; Bortz, H.; Lo, C.; Cleland, H. Venous thromboembolism in burns patients: Are we underestimating the risk and underdosing our prophylaxis? J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 1814–1823. [Google Scholar] [CrossRef] [PubMed]
- Wait, M.; Hunt, J.L.; Purdue, G.F. Duplex scanning of central vascular access sites in burn patients. Ann. Surg. 1990, 211, 499. [Google Scholar] [CrossRef] [PubMed]
- Merrer, J.; De Jonghe, B.; Golliot, F.; Lefrant, J.-Y.; Raffy, B.; Barre, E.; Rigaud, J.-P.; Casciani, D.; Misset, B.; Bosquet, C.; et al. Complications of Femoral and Subclavian Venous Catheterization in Critically Ill Patients: A Randomized Controlled Trial. JAMA 2001, 286, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Diringer, M.N.; Neurocritical Care Fever Reduction Trial Group. Treatment of fever in the neurologic intensive care unit with a catheter-based heat exchange system. Crit. Care Med. 2004, 32, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Braekkan, S.K.; Mathiesen, E.B.; Njølstad, I.; Wilsgaard, T.; Hansen, J.-B. Hematocrit and risk of venous thromboembolism in a general population. The Tromso study. In Haematologica; Ferrata Storti Foundation: Pavia, Italy, 2010; Volume 95, pp. 270–275. [Google Scholar]


{kind=link}
| Patients with Catheter (n = 40) | Patients without Catheter (n = 127) | p-Value | |
|---|---|---|---|
| Age (years) | 44 (33, 59) | 41 (25, 56) | 0.279 |
| %TBSA Burn | 55 (40, 65) | 28 (22, 44) | <0.01 * |
| Mechanical Ventilation (hours) | 261 (133, 600) | 3 (0, 44) | <0.01 * |
| ICU Length of Stay (hours) | 405 (274, 828) | 9.8 (0, 107) | <0.01 * |
| Total Length of Stay (days) | 62 (39, 81) | 16 (3, 27) | <0.01 * |
| VTE | 8 (20%) | 5 (4%) | <0.01 * |
| Mortality | 9 (23%) | 35 (28%) | 0.68 |
| VTE n = 8 | No VTE n = 32 | p-Value | |
|---|---|---|---|
| Age (years) | 49 (33, 62) | 52 (31, 59) | 0.883 |
| %TBSA burn | 60 (41, 69) | 54 (40, 65) | 0.461 |
| Male | 5 (63%) | 26 (81%) | 0.348 |
| Weight (kg) | 95 (70, 107) | 85 (74, 96) | 0.9745 |
| ICU admission | 8 (100%) | 32 (100%) | >0.999 |
| Mechanical ventilation | 8 (100%) | 32 (100%) | >0.999 |
| Catheter duration (days) | 4 (3, 5) | 4 (3, 5.5) | 0.556 |
| Prophylactic anticoagulation administered whilst catheter in situ | 6 (75%) | 28 (88%) | 0.580 |
| Hct at time of catheter insertion (L/L) normal range = 0.36–0.50 L/L | 0.49 (0.44, 0.57) | 0.46 (0.39, 0.50) | 0.07 |
| Hb at time of catheter insertion (g/L) normal range = 128–175 g/L | 161 (144, 188) | 152 (133.5, 164.5) | 0.09 |
| Platelets at time of catheter insertion (×109/L) | 255 (199, 302) | 221.5 (144.5, 243.3) | 0.123 |
| pRBC transfusion | 5 (63%) | 18 (56.25%) | 0.709 |
| Number of pRBC transfusions whilst catheter in situ | 2 (0, 6.25) | 1.5 (0, 4) | 0.920 |
| Site of VTE: | |||
| Upper limb DVT | 4 (50%) | ||
| Lower limb DVT | 1 (12.5%) | ||
| Inferior Vena Cava DVT | 1 (12.5%) | ||
| PE | 2 (25%) | ||
| Mortality | 1 (12.5%) | 8 (25%) | 0.655 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reid, I.; Bortz, H.; Burrell, A.; Gantner, D.; Rosenblum, S.; Cleland, H. Venous Thromboembolism in Severe Burns Patients with Intravascular Warming Catheter: A Retrospective Cohort Study. Eur. Burn J. 2023, 4, 80-86. https://doi.org/10.3390/ebj4010008
Reid I, Bortz H, Burrell A, Gantner D, Rosenblum S, Cleland H. Venous Thromboembolism in Severe Burns Patients with Intravascular Warming Catheter: A Retrospective Cohort Study. European Burn Journal. 2023; 4(1):80-86. https://doi.org/10.3390/ebj4010008
Chicago/Turabian StyleReid, Isabella, Hadley Bortz, Aidan Burrell, Dashiell Gantner, Samara Rosenblum, and Heather Cleland. 2023. "Venous Thromboembolism in Severe Burns Patients with Intravascular Warming Catheter: A Retrospective Cohort Study" European Burn Journal 4, no. 1: 80-86. https://doi.org/10.3390/ebj4010008