
Microbiological Findings and Clinical Outcomes in Ugandan Patients with Infected Burn Wounds
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Procedures
2.3. Data Management and Analysis
3. Results
3.1. Study Population
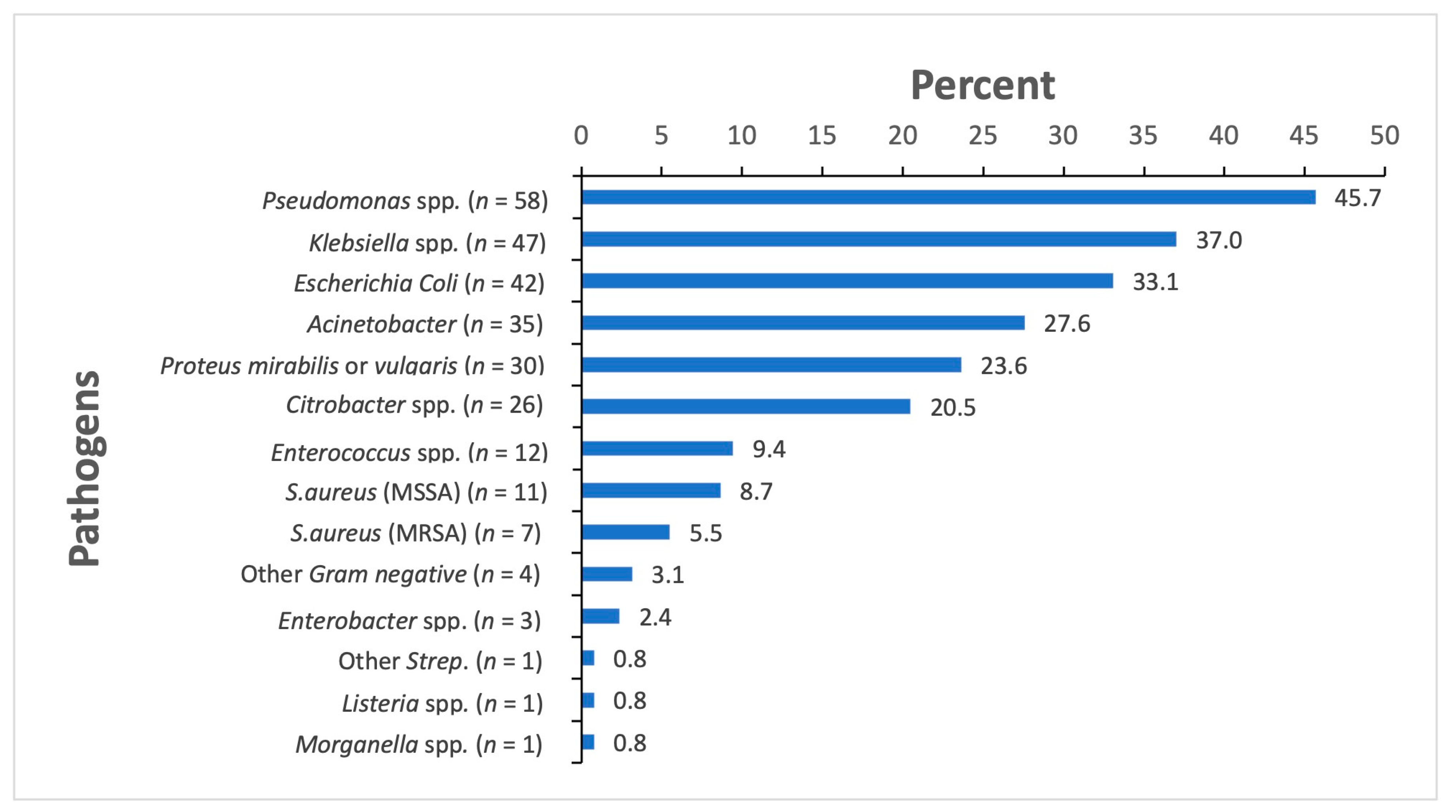
3.2. Microbiological Findings
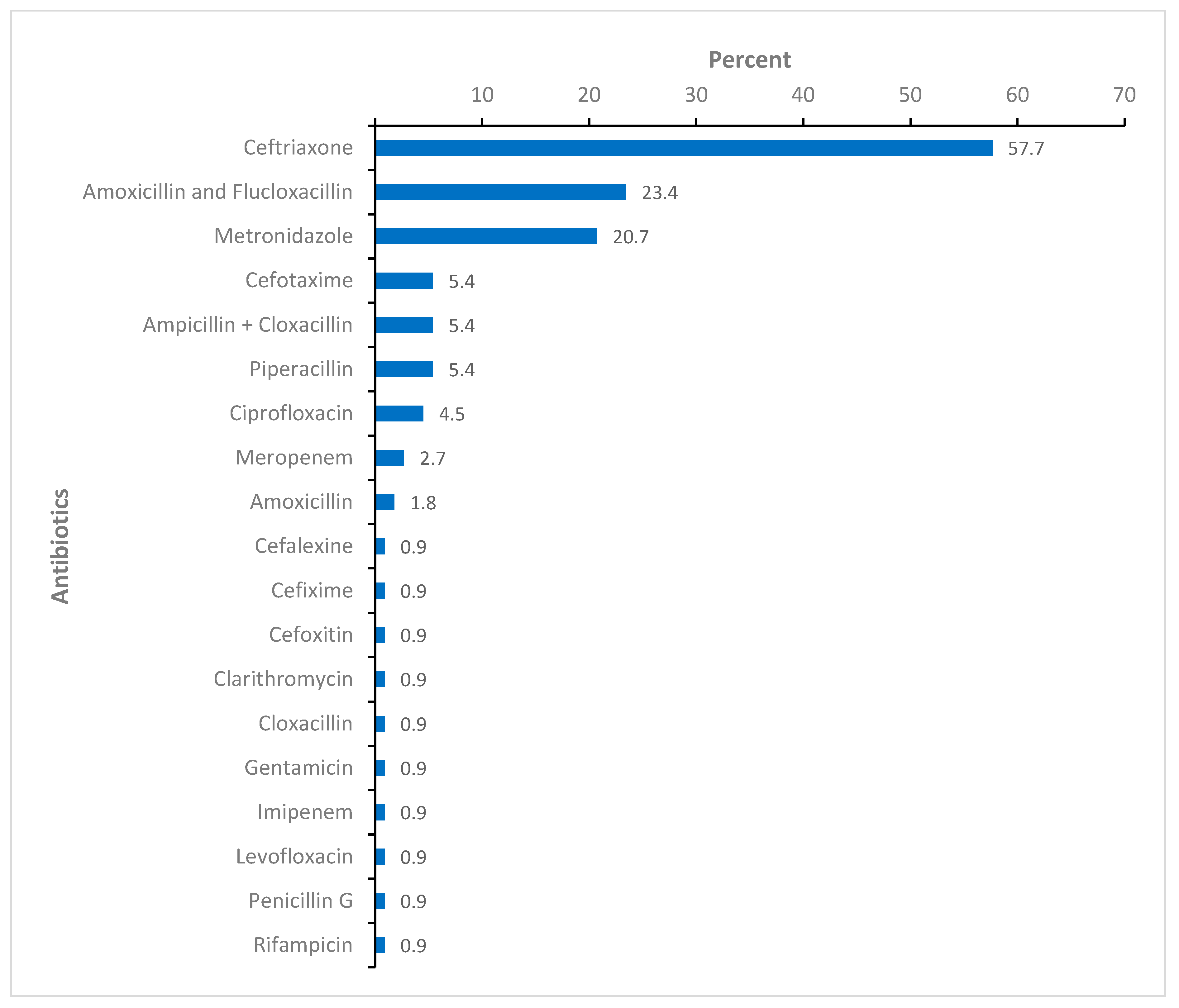
3.3. Targeted Antibiotic Treatment
3.4. Surgical Treatment and Clinical Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hu, Y.; Li, D.; Xu, L.; Hu, Y.; Sang, Y.; Zhang, G.; Dai, H. Epidemiology and outcomes of bloodstream infections in severe burn patients: A six-year retrospective study. Antimicrob. Resist. Infect. Control 2021, 10, 98. [Google Scholar] [CrossRef] [PubMed]
- McMahon, H.A.; Ndem, I.; Gampper, L.; Gampper, T.J.; DeGeorge, B.R. Quantifying Burn Injury-Related Disability and Quality of Life in the Developing World: A Primer for Patient-Centered Resource Allocation. Ann. Plast. Surg. 2019, 82 (Suppl 5), S433–S436. [Google Scholar] [CrossRef] [PubMed]
- Wanjeri, J.K.; Kinoti, M.; Olewe, T.H. Risk factors for burn injuries and fire safety awareness among patients hospitalized at a public hospital in Nairobi, Kenya: A case control study. Burns 2018, 44, 962–968. [Google Scholar] [CrossRef] [PubMed]
- Peck, M.D. Epidemiology of burns throughout the world. Part I: Distribution and risk factors. Burns 2011, 37, 1087–1100. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Naik, A.K.; Singh, S.K. Bacteriological profile and antimicrobial resistance patterns of burn wound infections in a tertiary care hospital. Heliyon 2019, 5, e02956. [Google Scholar] [CrossRef]
- Bahemia, I.; Muganza, A.; Moore, R.; Sahid, F.; Menezes, C. Microbiology and antibiotic resistance in severe burns patients: A 5 year review in an adult burns unit. Burns 2015, 41, 1536–1542. [Google Scholar] [CrossRef] [PubMed]
- Forjuoh, S. Burns in low- and middle-income countries: A review of available literature on descriptive epidemiology, risk factors, treatment, and prevention. Burns 2006, 32, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Zumla, A.; Memish, Z.A.; Maeurer, M.; Bates, M.; Mwaba, P.; Al-Tawfiq, J.A.; Denning, D.W.; Hayden, F.G.; Hui, D.S. Emerging novel and antimicrobial-resistant respiratory tract infections: New drug development and therapeutic options. Lancet Infect. Dis. 2014, 14, 1136–1149. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey. Available online: https://apps.who.int/iris/handle/10665/194460 (accessed on 20 December 2022).
- World Health Organization. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report: 2022. Available online: https://www.who.int/publications/i/item/9789240062702 (accessed on 20 December 2022).
- Holmes, A.H.; Moore, L.S.P.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J.V. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Akpan, M.R.; Isemin, N.U.; Udoh, A.E.; Ashiru-Oredope, D. Implementation of antimicrobial stewardship programmes in African countries: A systematic literature review. J. Glob. Antimicrob. Resist. 2020, 22, 317–324. [Google Scholar] [CrossRef]
- Ampaire, L.; Muhindo, A.; Orikiriza, P.; Mwanga-Amumpaire, J.; Bebell, L.; Boum, Y. A review of antimicrobial resistance in East Africa. Afr. J. Lab. Med. 2016, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Tadesse, B.T.; Ashley, E.A.; Ongarello, S.; Havumaki, J.; Wijegoonewardena, M.; González, I.J.; Dittrich, S. Antimicrobial resistance in Africa: A systematic review. BMC Infect. Dis. 2017, 17, 616. [Google Scholar] [CrossRef] [PubMed]
- Rolfe, R.; Kwobah, C.; Muro, F.; Ruwanpathirana, A.; Lyamuya, F.; Bodinayake, C.; Nagahawatte, A.; Piyasiri, B.; Sheng, T.; Bollinger, J.; et al. Barriers to implementing antimicrobial stewardship programs in three low- and middle-income country tertiary care settings: Findings from a multi-site qualitative study. Antimicrob. Resist. Infect. Control 2021, 10, 60. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef]
- Kajumbula, H.; Fujita, A.W.; Mbabazi, O.; Najjuka, C.; Izale, C.; Akampurira, A.; Aisu, S.; Lamorde, M.; Walwema, R.; Bahr, N.C.; et al. Antimicrobial Drug Resistance in Blood Culture Isolates at a Tertiary Hospital, Uganda. Emerg. Infect. Dis. 2018, 24, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Amissah, N.A.; Chlebowicz, M.A.; Ablordey, A.; Sabat, A.J.; Tetteh, C.S.; Prah, I.; Van Der Werf, T.S.; Friedrich, A.W.; Van Dijl, J.M.; Rossen, J.W.; et al. Molecular Characterization of Staphylococcus aureus Isolates Transmitted between Patients with Buruli Ulcer. PLoS Negl. Trop. Dis. 2015, 9, e0004049. [Google Scholar] [CrossRef]
- Afema, J.A.; Byarugaba, D.K.; Shah, D.H.; Atukwase, E.; Nambi, M.; Sischo, W.M. Potential Sources and Transmission of Salmonella and Antimicrobial Resistance in Kampala, Uganda. PLoS ONE 2016, 11, e0152130. [Google Scholar] [CrossRef]
- Ministry of Health Uganda. Uganda Clinical Guidelines 2016: National Guidelines for Management of Common Conditions. Available online: http://library.health.go.ug/sites/default/files/resources/Uganda%20Clinical%20Guidelines%202016_FINAL.pdf (accessed on 20 December 2022).
- World Health Organization (WHO). Report on the Burden of Endemic Health Care-Associated Infection Worldwide: A Systematic Review of the Literature. Available online: https://apps.who.int/iris/bitstream/handle/10665/80135/9789241501507_eng.pdf;jsessionid=2DF456D12FAFCB4EC95C903454967144?sequence=1 (accessed on 18 January 2023).
- Qin, X.; Weissman, S.J.; Chesnut, M.F.; Zhang, B.; Shen, L. Kirby-Bauer disc approximation to detect inducible third-generation cephalosporin resistance in Enterobacteriaceae. Ann. Clin. Microbiol. Antimicrob. 2004, 3, 13. [Google Scholar] [CrossRef]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- Mboowa, G.; Aruhomukama, D.; Sserwadda, I.; Kitutu, F.; Davtyan, H.; Owiti, P.; Kamau, E.; Enbiale, W.; Reid, A.; Bulafu, D.; et al. Increasing Antimicrobial Resistance in Surgical Wards at Mulago National Referral Hospital, Uganda, from 2014 to 2018—Cause for Concern? Trop. Med. Infect. Dis. 2021, 6, 82. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Norbury, W.; Herndon, D.N.; Tanksley, J.; Jeschke, M.G.; Finnerty, C.C. Infection in Burns. Surg. Infect. (Larchmt) 2016, 17, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.; Namuwenge, P.M.; Okure, G.; Mwesige, B.; Namusisi, O.K.; Mukanga, D. Over-the-counter suboptimal dispensing of antibiotics in Uganda. J. Multidiscip. Health 2013, 6, 303–310. [Google Scholar] [CrossRef]
- Belachew, S.A.; Hall, L.; Selvey, L.A. Non-prescription dispensing of antibiotic agents among community drug retail outlets in Sub-Saharan African countries: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2021, 10, 13. [Google Scholar] [CrossRef]
- Nabaweesi, I.; Olum, R.; Sekite, A.B.; Suubi, W.T.; Nakiwunga, P.; Machali, A.; Katagirya, E. Antibiotic Practices, Perceptions and Self-Medication among Patients at a National Referral Hospital in Uganda. Infect. Drug Resist. 2021, 14, 2155–2164. [Google Scholar] [CrossRef]
- Lima, W.G.; Alves, G.C.S.; Sanches, C.; Fernandes, S.O.A.; de Paiva, M.C. Carbapenem-resistant Acinetobacter baumannii in patients with burn injury: A systematic review and meta-analysis. Burns 2019, 45, 1495–1508. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Action Plan on Antimicrobial Resistance. 2016. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 20 December 2022).




{kind=link}
{kind=link}
{kind=link}
| Demographics | |
|---|---|
| Sex, n (%) | |
| Male | 78 (55.7) |
| Female | 62 (44.3) |
| Age in years, median (IQR) | 26 (7–35) |
| Length of hospital stay at enrollment in days, median (IQR) | 8.5 (4–15.5) |
| Length of hospital stay at termination in days, median (IQR) | 45.5 (28.5–66.0) |
| Reason for admission, n (%) | |
| Plastic reconstruction after burn injury | 101 (72.2) |
| Orthopedic/Trauma | 36 (25.7) |
| Post-operative | 3 (2.1) |
| Type of Orthopedic/Trauma case 1 | |
| Trauma without fractures | 15 (41.7) |
| Fracture of lower limbs | 9 (25.0) |
| Other trauma | 7 (19.4) |
| Polytrauma | 5 (13.9) |
| Causes of burns 2 | |
| Flames | 42 (41.6) |
| Hot other liquids | 23 (22.8) |
| Hot water | 15 (14.9) |
| Electricity | 15 (4.9) |
| Acid | 3 (3.0) |
| Others | 7 (6.9) |
| Degree of burn at enrollment, n (%) 3 | |
| 2b (deep partial thickness) | 73 (72.3) |
| 3 (full thickness without bone involvement) | 15 (14.9) |
| 2a (superficial partial thickness) | 8 (7.9) |
| 4 (full thickness with bone involved) | 5 (4.9) |
| Isolates | Pseudomonas spp. N = 56 n/N (%) | Klebsiella spp. N = 47 n/N (%) | E. coli N = 42 n/N (%) | Acinetobacter spp. N = 35 n/N (%) | Proteus spp. N = 30 n/N (%) | Citrobacter spp. N = 26 n/N (%) |
|---|---|---|---|---|---|---|
| Amoxicillin/Clavulanic Acid | - | 15/29 (51.7) | 15/33 (45.5) | - | 4/17 (23.5) | 9/14 (64.3) |
| Ampicillin | - | 32/32 (100) | 21/21 (100) | - | 14/17(82.3) | 16/16 (100) |
| Piperacillin | 30/48 (62.5) | 5/5 (100) | 4/4 (100.0) | 26/31(83.9) | 4/4 (100) | 2/2 |
| Piperacillin/Tazobactam | 15/41 (36.6) | 7/27 (25.9) | 9/19 (47.4) | 19/28 (67.9) | 1/16 (6.3) | 4/16 (25.0) |
| Cefuroxime | - | 42/44 (95.5) | 29/33 (87.9) | - | 18/25 (72.0) | 20/23 (86.9) |
| Cefotaxime OR Ceftriaxone | 1/1 | 44/46 (95.6) | 35/40 (87.5) | 8/11 (72.7) | 16/29 (55.2) | 17/24 (70.8) |
| Ceftazidime | 27/39 (69.2) | 34/39 (87.2) | 23/25 (92.0) | 23/28 (82.1) | 8/14 (57.1) | 12/20 (60.0) |
| Cefepime | 29/39 (74.4) | 2/2 (100.0 | 9/9 (100) | 21/27 (77.8) | - | 3/3 (100) |
| Imipenem OR Meropenem | 2/53 (3.8) | 4/47 (8.5) | 2/39 (5.1) | 15/33 (45.5) | 4/28 (14.3) | 6/26 (23.1) |
| Ciprofloxacin | 11/48 (22.9) | 14/45 (31.1) | 19/36 (52.8) | 24/31 (77.4) | 16/28 (57.1) | 8/26 (30.8) |
| Amikacin | 26/40 (65.0) | 1/20 (5.0) | 2/21 (9.5) | 8/25(32.0) | 1/13 (7.7) | 2/13 (15.4) |
| Cotrimoxazole | 2/2 | 28/28 (100) | 23/27 (85.2) | 10/10 (100) | 13/14 (92.9) | 15/18 (83.3) |
| Gentamicin | 29/44 (65.9) | 22/37 (59.5) | 13/30 (43.3) | 24/30 (80.0) | 12/25 (48.0) | 12/18 (66.7) |
| Chloramphenicol | 1/1 | 20/33 (60.6) | 10/30 (33.3) | - | 15/22 (68.2) | 8/12 (66.7) |
| Colistin/Polymyxin B | - | - | - | - | - | 1/4 (25.0) |
| Tetracycline | - | - | - | 18/27 (66.7) | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weinreich, J.; Namatovu, C.; Nsibirwa, S.; Mbabazi, L.; Kajumbula, H.; Dietze, N.; Lübbert, C.; Nabajja, H.; Musaazi, J.; Kabugo, C.; et al. Microbiological Findings and Clinical Outcomes in Ugandan Patients with Infected Burn Wounds. Eur. Burn J. 2023, 4, 69-79. https://doi.org/10.3390/ebj4010007
Weinreich J, Namatovu C, Nsibirwa S, Mbabazi L, Kajumbula H, Dietze N, Lübbert C, Nabajja H, Musaazi J, Kabugo C, et al. Microbiological Findings and Clinical Outcomes in Ugandan Patients with Infected Burn Wounds. European Burn Journal. 2023; 4(1):69-79. https://doi.org/10.3390/ebj4010007
Chicago/Turabian StyleWeinreich, Johannes, Christina Namatovu, Sara Nsibirwa, Leah Mbabazi, Henry Kajumbula, Nadine Dietze, Christoph Lübbert, Hawah Nabajja, Joseph Musaazi, Charles Kabugo, and et al. 2023. "Microbiological Findings and Clinical Outcomes in Ugandan Patients with Infected Burn Wounds" European Burn Journal 4, no. 1: 69-79. https://doi.org/10.3390/ebj4010007