

Ageing-Oriented Prosthetic Treatment Plan: A Case Report


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
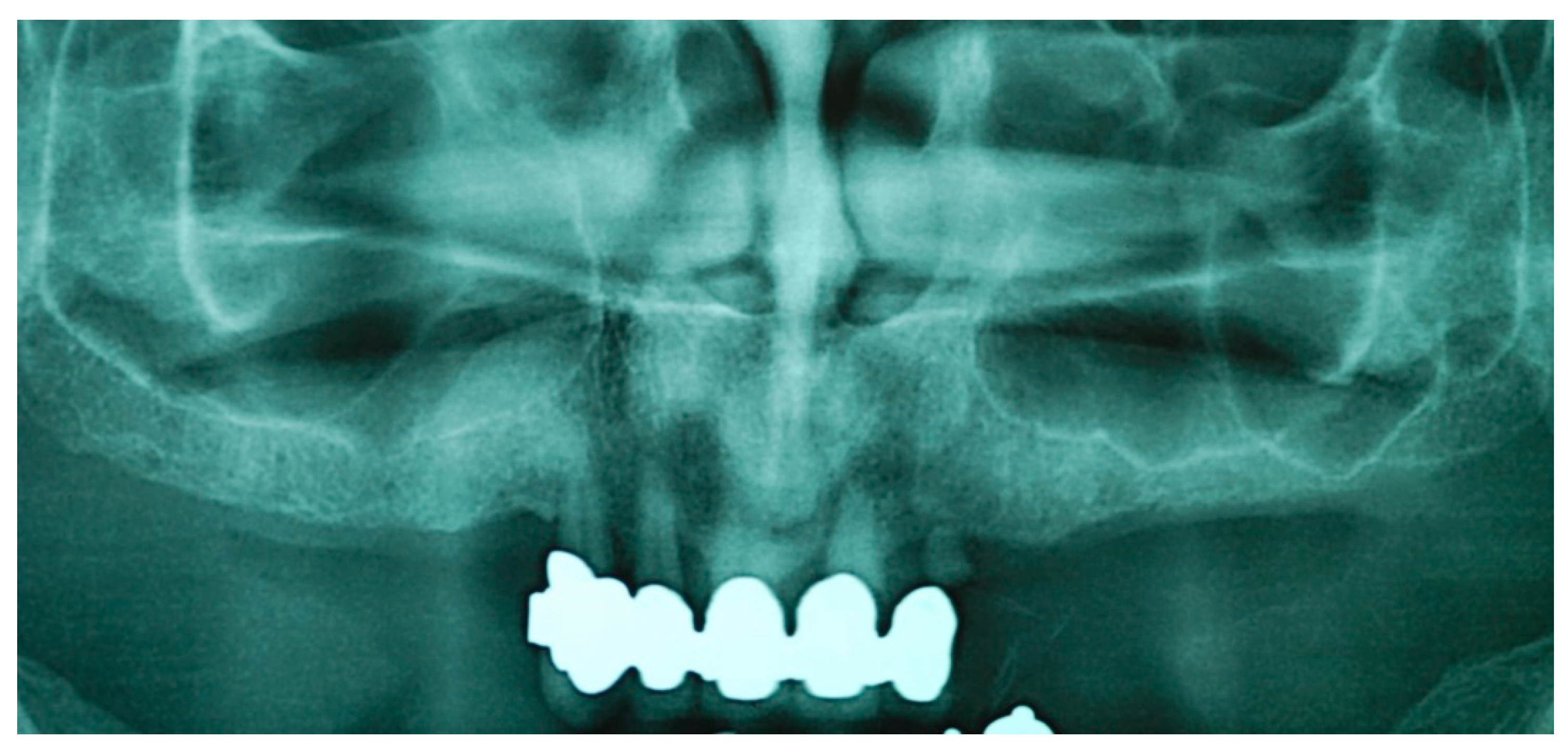
2.1. First Step: Complete Fixed Rehabilitation
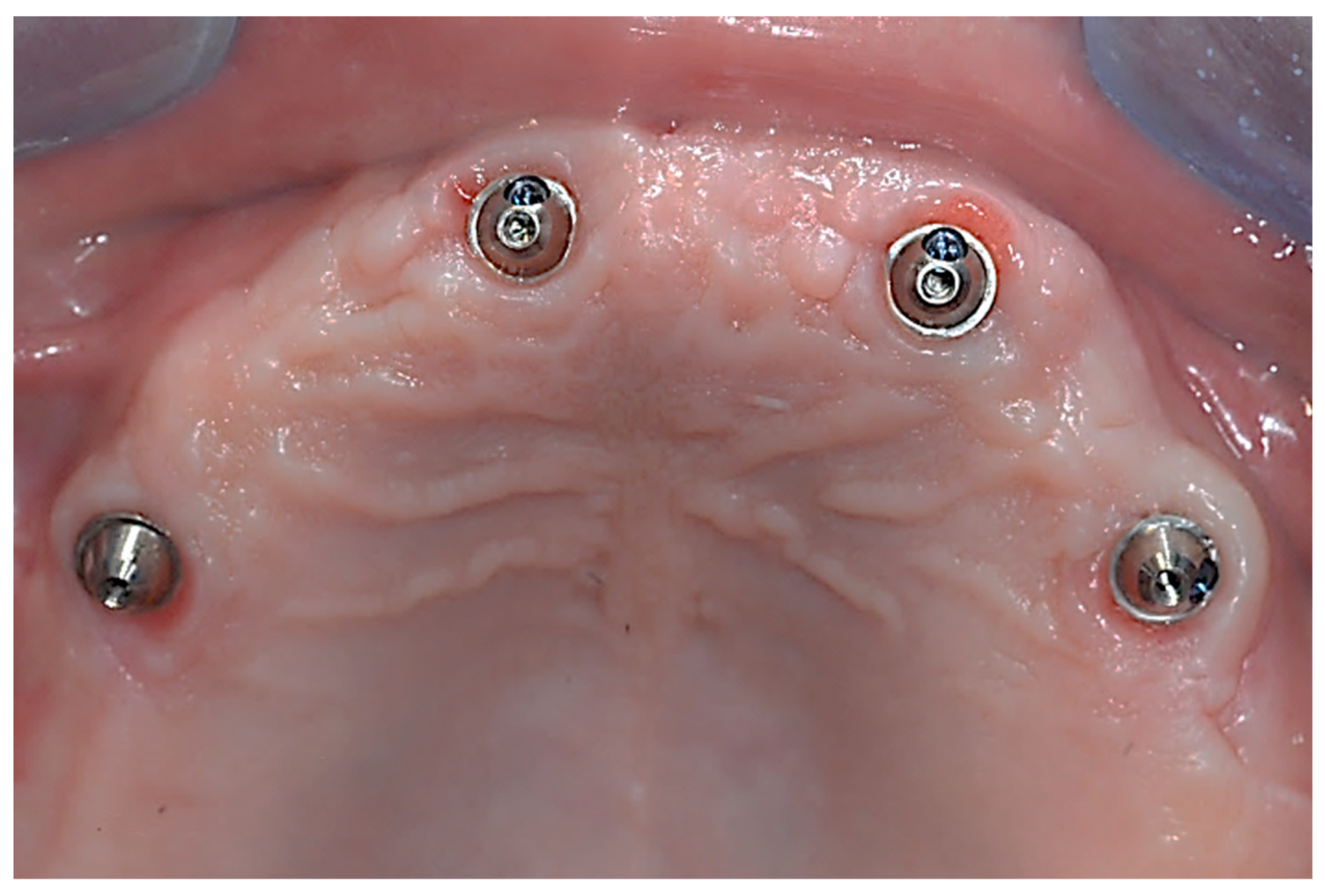
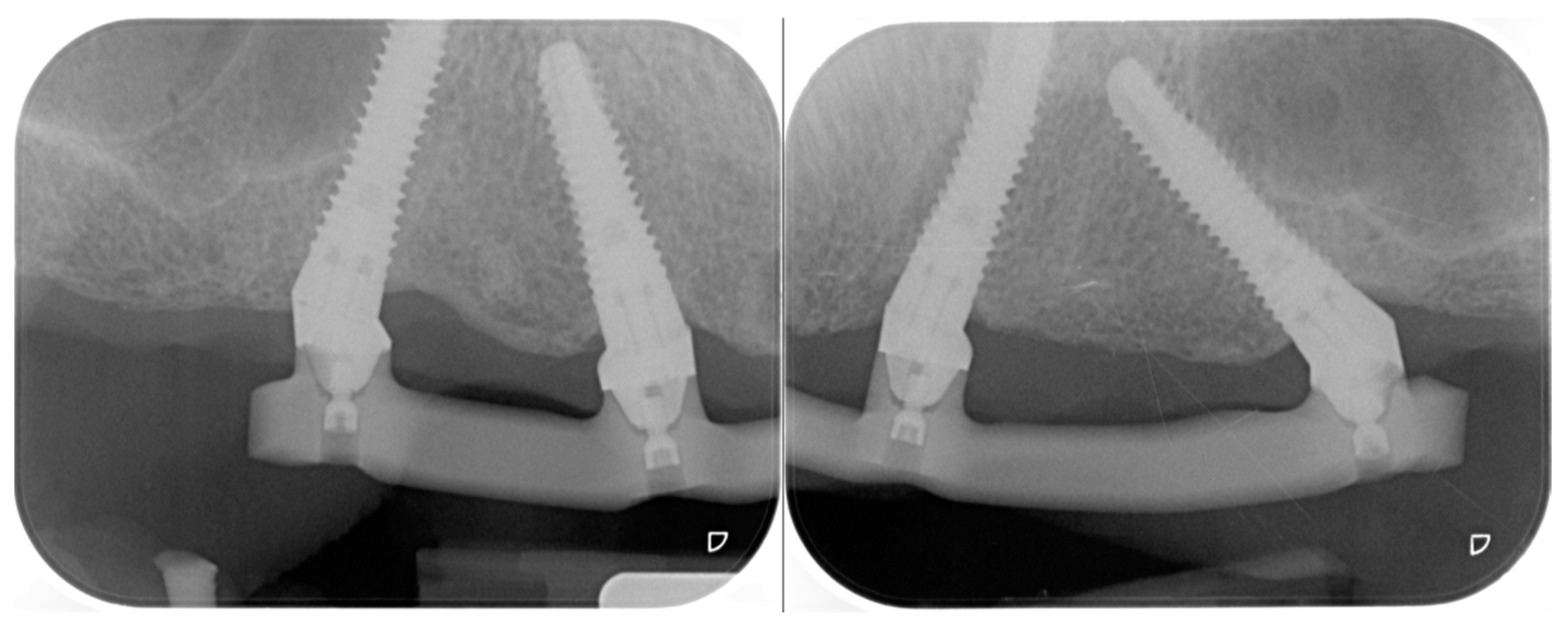
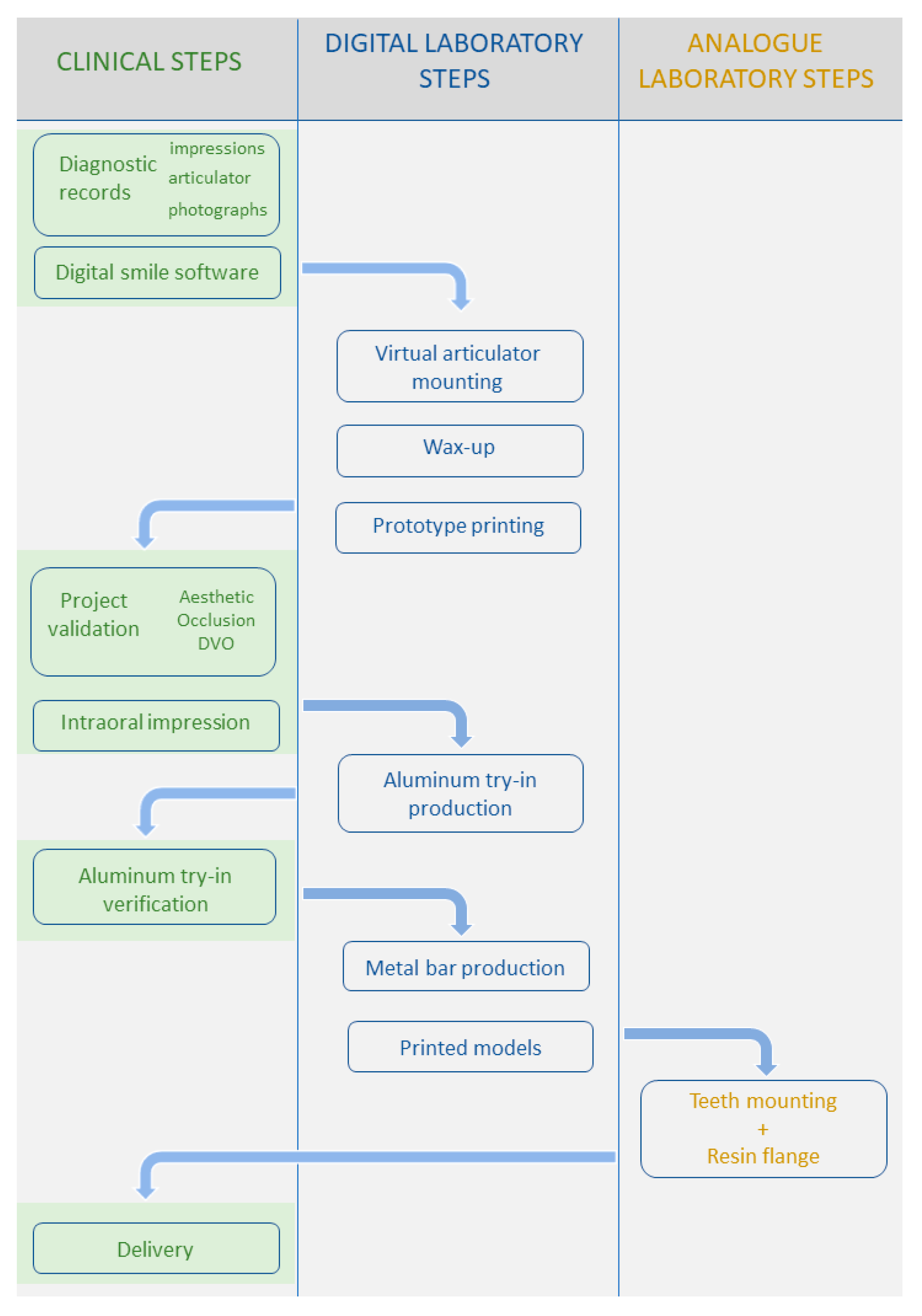
2.2. Second Step: From FDP to Implant-Supported Overdenture
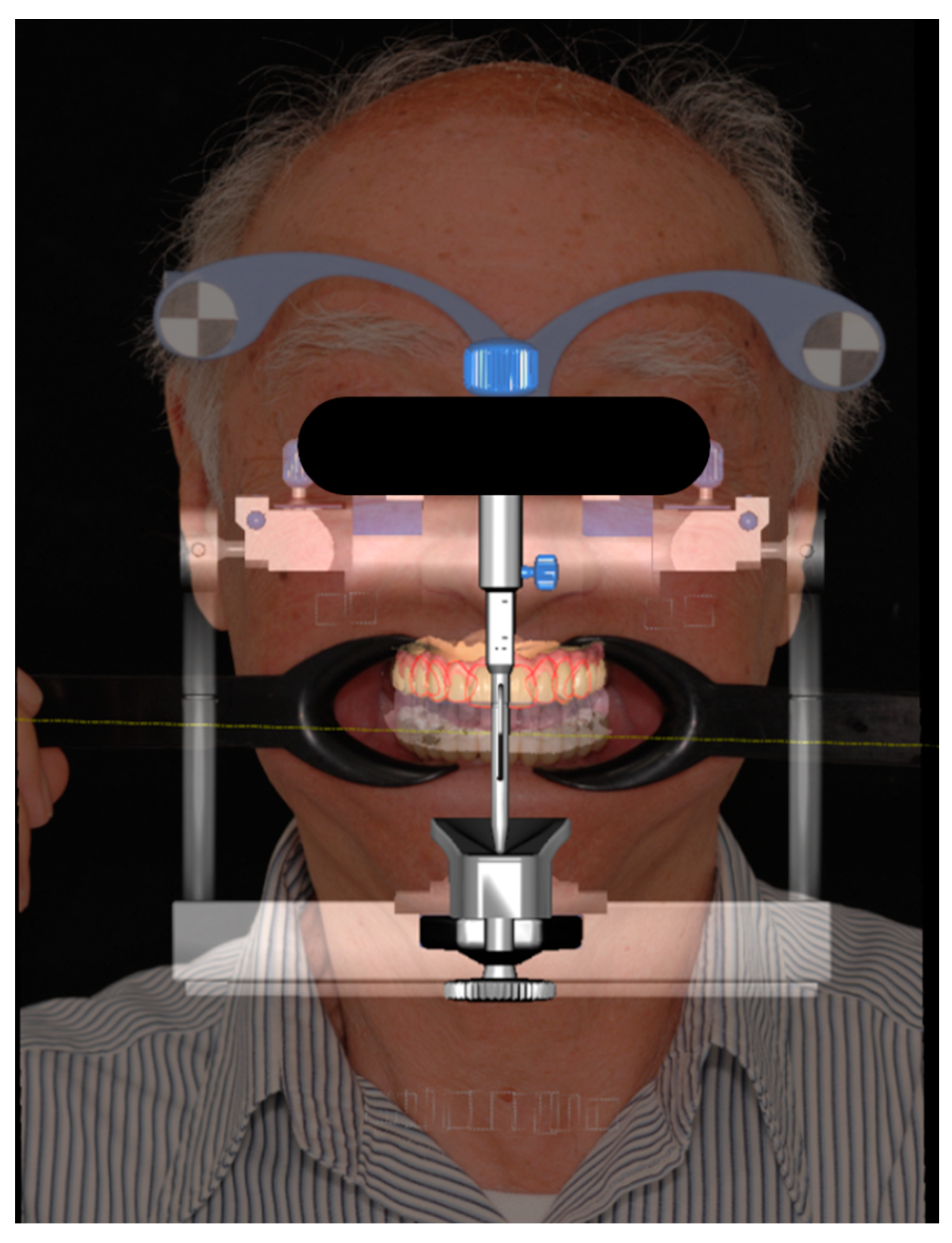
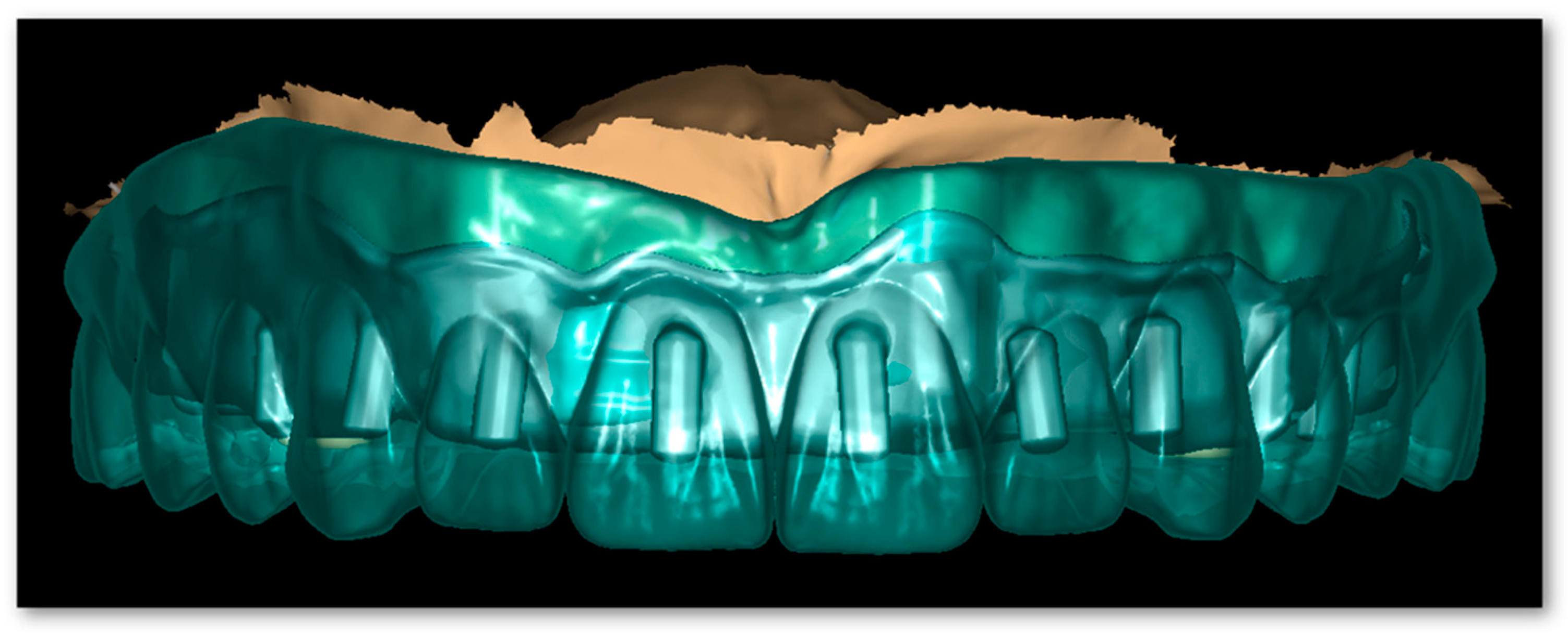
- Intra-oral impressions: an intra-oral scanner (IOS) (Trios3 v1.4.7.5, 3Shape; Copenhagen, Denmark) was used to produce a full-arch digital model of the patient’s upper and lower arches [19];
- Virtual articulation of the model was performed through a digital facebow (Jaw registration JMA, Zebris Medical GmbH; Isny, Germany) [23].
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kontis, V.; Bennett, J.E.; Mathers, C.D.; Li, G.; Foreman, K.; Ezzati, M. Future Life Expectancy in 35 Industrialised Countries: Projections with a Bayesian Model Ensemble. Lancet 2017, 389, 1323–1335. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.C.; Drefahl, S.; Ahlbom, A.; Lambe, M.; Modig, K. Trends in Life Expectancy: Did the Gap between the Healthy and the Ill Widen or Close? BMC Med. 2020, 18, 41. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Severe Tooth Loss: A Systematic Review and Meta-Analysis. J. Dent. Res. 2014, 93, 20S–28S. [Google Scholar] [CrossRef] [PubMed]
- Romandini, M.; Baima, G.; Antonoglou, G.; Bueno, J.; Figuero, E.; Sanz, M. Periodontitis, Edentulism, and Risk of Mortality: A Systematic Review with Meta-Analyses. J. Dent. Res. 2021, 100, 37–49. [Google Scholar] [CrossRef]
- Ettinger, R.L.; Beck, J.D. Geriatric Dental Curriculum and the Needs of the Elderly. Spec. Care Dent. 1984, 4, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Reissmann, D.R.; Dard, M.; Lamprecht, R.; Struppek, J.; Heydecke, G. Oral Health-Related Quality of Life in Subjects with Implant-Supported Prostheses: A Systematic Review. J. Dent. 2017, 65, 22–40. [Google Scholar] [CrossRef]
- Zembic, A.; Wismeijer, D. Patient-Reported Outcomes of Maxillary Implant-Supported Overdentures Compared with Conventional Dentures. Clin. Oral Implant. Res. 2014, 25, 441–450. [Google Scholar] [CrossRef]
- Yao, C.J.; Cao, C.; Bornstein, M.M.; Mattheos, N. Patient-reported Outcome Measures of Edentulous Patients Restored with Implant-supported Removable and Fixed Prostheses: A Systematic Review. Clin. Oral Implant. Res. 2018, 29, 241–254. [Google Scholar] [CrossRef]
- Curtis, D.A.; Lin, G.H.; Rajendran, Y.; Gessese, T.; Suryadevara, J.; Kapila, Y.L. Treatment Planning Considerations in the Older Adult with Periodontal Disease. Periodontol 2000 2021, 87, 157–165. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-Implant Diseases and Conditions: Consensus Report of Workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef]
- Monje, A.; Aranda, L.; Diaz, K.T.; Alarcón, M.A.; Bagramian, R.A.; Wang, H.L.; Catena, A. Impact of Maintenance Therapy for the Prevention of Peri-Implant Diseases. J. Dent. Res. 2016, 95, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Blanco, C.; Liñares, A.; Dopico, J.; Pico, A.; Sobrino, T.; Leira, Y.; Blanco, J. Peri-Implantitis, Systemic Inflammation, and Dyslipidemia: A Cross-Sectional Biochemical Study. J. Periodontal Implant. Sci. 2021, 51, 342. [Google Scholar] [CrossRef] [PubMed]
- Catapano, S.; Ortensi, L.; Mobilio, N.; Grande, F. The New Elderly Patient: A Necessary Upgrade. Prosthesis 2021, 3, 99–104. [Google Scholar] [CrossRef]
- Doyle, D.J.; Hendrix, J.M.; Garmon, E.H. American Society of Anesthesiologists Classification; StatPearls Publishing: Tampa, FL, USA, 2023. [Google Scholar]
- Miller, E.L. Systems for Classifying Partially Dentulous Arches. J. Prosthet. Dent. 1970, 24, 25–40. [Google Scholar] [CrossRef] [PubMed]
- Catapano, S.; Ferrari, M.; Mobilio, N.; Montanari, M.; Corsalini, M.; Grande, F. Comparative Analysis of the Stability of Prosthetic Screws under Cyclic Loading in Implant Prosthodontics: An in Vitro Study. Appl. Sci. 2021, 11, 622. [Google Scholar] [CrossRef]
- Biscaro, L.; Becattelli, A.; Poggio, P.M.; Soattin, M.; Rossini, F. The One-Model Technique: A New Method for Immediate Loading with Fixed Prostheses in Edentulous or Potentially Edentulous Jaws. Int. J. Periodontics Restor. Dent. 2009, 29, 307–313. [Google Scholar]
- Monje, A.; Wang, H.-L.; Nart, J. Association of Preventive Maintenance Therapy Compliance and Peri-Implant Diseases: A Cross-Sectional Study. J. Periodontol. 2017, 88, 1030–1041. [Google Scholar] [CrossRef]
- Celeghin, G.; Franceschetti, G.; Mobilio, N.; Fasiol, A.; Catapano, S.; Corsalini, M.; Grande, F. Complete-Arch Accuracy of Four Intraoral Scanners: An in Vitro Study. Healthcare 2021, 9, 246. [Google Scholar] [CrossRef]
- Ortensi, L.; Ortensi, M.; Minghelli, A.; Grande, F. Implant-Supported Prosthetic Therapy of an Edentulous Patient: Clinical and Technical Aspects. Prosthesis 2020, 2, 140–152. [Google Scholar] [CrossRef]
- Ortensi, L.; Vitali, T.; Bonfiglioli, R.; Grande, F. New Tricks in the Preparation Design for Prosthetic Ceramic Laminate Veeners. Prosthesis 2019, 1, 29–40. [Google Scholar] [CrossRef]
- Ortensi, L.; Fisichella, M.L.; Ortensi, M.; Grande, F.; Pellegrino, G.; Ferri, A.; La Rosa, G.R.; Pedullà, E. A Comparison of Accuracy between Three Different Facial Detection Systems for Prosthodontic Esthetic Preview: A Single-Blinded in Vitro Study. Minerva Dent. Oral Sci. 2021, 71, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Petre, A.; Drafta, S.; Stefanescu, C.; Oancea, L. Virtual Facebow Technique Using Standardized Background Images. J. Prosthet. Dent. 2019, 121, 724–728. [Google Scholar] [CrossRef] [PubMed]
- Ortensi, L.; Sigari, G.; La Rosa, G.R.M.; Ferri, A.; Grande, F.; Pedullà, E. Digital Planning of Composite Customized Veneers Using Digital Smile Design: Evaluation of Its Accuracy and Manufacturing. Clin. Exp. Dent. Res. 2022, 8, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Paratelli, A.; Vania, S.; Gómez-Polo, C.; Ortega, R.; Revilla-León, M.; Gómez-Polo, M. Techniques to Improve the Accuracy of Complete-Arch Implant Intraoral Digital Scans: A Systematic Review. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef]
- Albayrak, B.; Sukotjo, C.; Wee, A.G.; Korkmaz, İ.H.; Bayındır, F. Three-Dimensional Accuracy of Conventional Versus Digital Complete Arch Implant Impressions. J. Prosthodont. 2021, 30, 163–170. [Google Scholar] [CrossRef]
- Tallarico, M.; Lumbau, A.I.; Scrascia, R.; Demelas, G.; Sanseverino, F.; Amarena, R.; Meloni, S.M. Feasibility of Using a Prosthetic-Based Impression Template to Improve the Trueness and Precision of a Complete Arch Digital Impression on Four and Six Implants: An in Vitro Study. Materials 2020, 13, 3543. [Google Scholar] [CrossRef]
- Venezia, P.; Torsello, F.; D’Amato, S.; Cavalcanti, R. Digital Cross-Mounting: A New Opportunity in Prosthetic Dentistry. Quintessence Int. 2017, 48, 701–709. [Google Scholar] [CrossRef]
- United Nations. World Population, Ageing; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; Abyu, G.Y.; Alsharif, U.; et al. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- Bakker, M.H.; Vissink, A.; Spoorenberg, S.L.W.; Jager-Wittenaar, H.; Wynia, K.; Visser, A. Are Edentulousness, Oral Health Problems and Poor Health-Related Quality of Life Associated with Malnutrition in Community-Dwelling Elderly (Aged 75 Years and over)? A Cross-Sectional Study. Nutrients 2018, 10, 1965. [Google Scholar] [CrossRef]
- Lantto, A.; Lundqvist, R.; Wårdh, I. Quality of Life Related to Tooth Loss and Prosthetic Replacements among Persons with Dependency and Functional Limitations. Acta Odontol. Scand. 2020, 78, 173–180. [Google Scholar] [CrossRef]
- Patzelt, S.B.M.; Bahat, O.; Reynolds, M.A.; Strub, J.R. The All-on-Four Treatment Concept: A Systematic Review. Clin. Implant Dent. Relat. Res. 2014, 16, 836–855. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Brägger, U.; Lang, N.P.; Zwahlen, M. Comparison of Survival and Complication Rates of Tooth-Supported Fixed Dental Prostheses (FDPs) and Implant-Supported FDPs and Single Crowns (SCs). Clin. Oral Implants Res. 2007, 18 (Suppl. 3), 97–113. [Google Scholar] [CrossRef] [PubMed]
- Rojas Vizcaya, F. Retrospective 2- to 7-Year Follow-Up Study of 20 Double Full-Arch Implant-Supported Monolithic Zirconia Fixed Prostheses: Measurements and Recommendations for Optimal Design. J. Prosthodont. 2018, 27, 501–508. [Google Scholar] [CrossRef]
- Mumcu, E.; Dayan, S.C.; Genceli, E.; Geckili, O. Comparison of Four-Implant-Retained Overdentures and Implant-Supported Fixed Prostheses Using the All-on-4 Concept in the Maxilla in Terms of Patient Satisfaction, Quality of Life, and Marginal Bone Loss: A 2-Year Retrospective Study. Quintessence Int. 2020, 51, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Marinello, C.P. Treatment Outcomes of Fixed or Removable Implant-Supported Prostheses in the Edentulous Maxilla. Part I: Patients’ Assessments. J. Prosthet. Dent. 2000, 83, 424–433. [Google Scholar] [CrossRef]
- Homsi, G.; Karlsson, A.; Almotairy, N.; Trulsson, M.; Kumar, A.; Grigoriadis, A. Subjective and Objective Evaluation of Masticatory Function in Patients with Bimaxillary Implant-Supported Prostheses. J. Oral Rehabil. 2022, 50, 140–149. [Google Scholar] [CrossRef]
- ELsyad, M.A.; Tella, E.A.E.S.; Mohamed, S.S.; Mahrous, A.I. Within-Patient Evaluation of Chewing Efficiency and Maximum Bite Force of Conventional Dentures, Fixed Prostheses, and Milled Bar Overdentures Used for All-on-4 Implant Rehabilitation of Atrophied Mandibular Ridges: A Short-Term Randomized Trial. Clin. Implant. Dent. Relat. Res. 2022, 24, 522–531. [Google Scholar] [CrossRef]
- Feine, J.S.; Maskawi, K.; de Grandmont, P.; Donohue, W.B.; Tanguay, R.; Lund, J.P. Within-Subject Comparisons of Implant-Supported Mandibular Prostheses: Evaluation of Masticatory Function. J. Dent. Res. 1994, 73, 1646–1656. [Google Scholar] [CrossRef]
- Monaco, C.; Scheda, L.; Ciocca, L.; Zucchelli, G. The Prototype Concept in a Full Digital Implant Workflow. J. Am. Dent. Assoc. 2018, 149, 918–923. [Google Scholar] [CrossRef]
- Bishti, S.; Tuna, T.; Rittich, A.; Wolfart, S. Patient-Reported Outcome Measures (PROMs) of Implant-Supported Reconstructions Using Digital Workflows: A Systematic Review and Meta-Analysis. Clin. Oral Implant. Res. 2021, 32, 318–335. [Google Scholar] [CrossRef]















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortensi, L.; Vitali, T.; Mirra, R.; Ortensi, M.; Borromeo, C. Ageing-Oriented Prosthetic Treatment Plan: A Case Report. Prosthesis 2023, 5, 496-508. https://doi.org/10.3390/prosthesis5020034
Ortensi L, Vitali T, Mirra R, Ortensi M, Borromeo C. Ageing-Oriented Prosthetic Treatment Plan: A Case Report. Prosthesis. 2023; 5(2):496-508. https://doi.org/10.3390/prosthesis5020034
Chicago/Turabian StyleOrtensi, Luca, Tommaso Vitali, Raffaele Mirra, Marco Ortensi, and Carlo Borromeo. 2023. "Ageing-Oriented Prosthetic Treatment Plan: A Case Report" Prosthesis 5, no. 2: 496-508. https://doi.org/10.3390/prosthesis5020034