
Full-Digital Customized Meshes in Guided Bone Regeneration Procedures: A Scoping Review

 , ,
, ,  ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
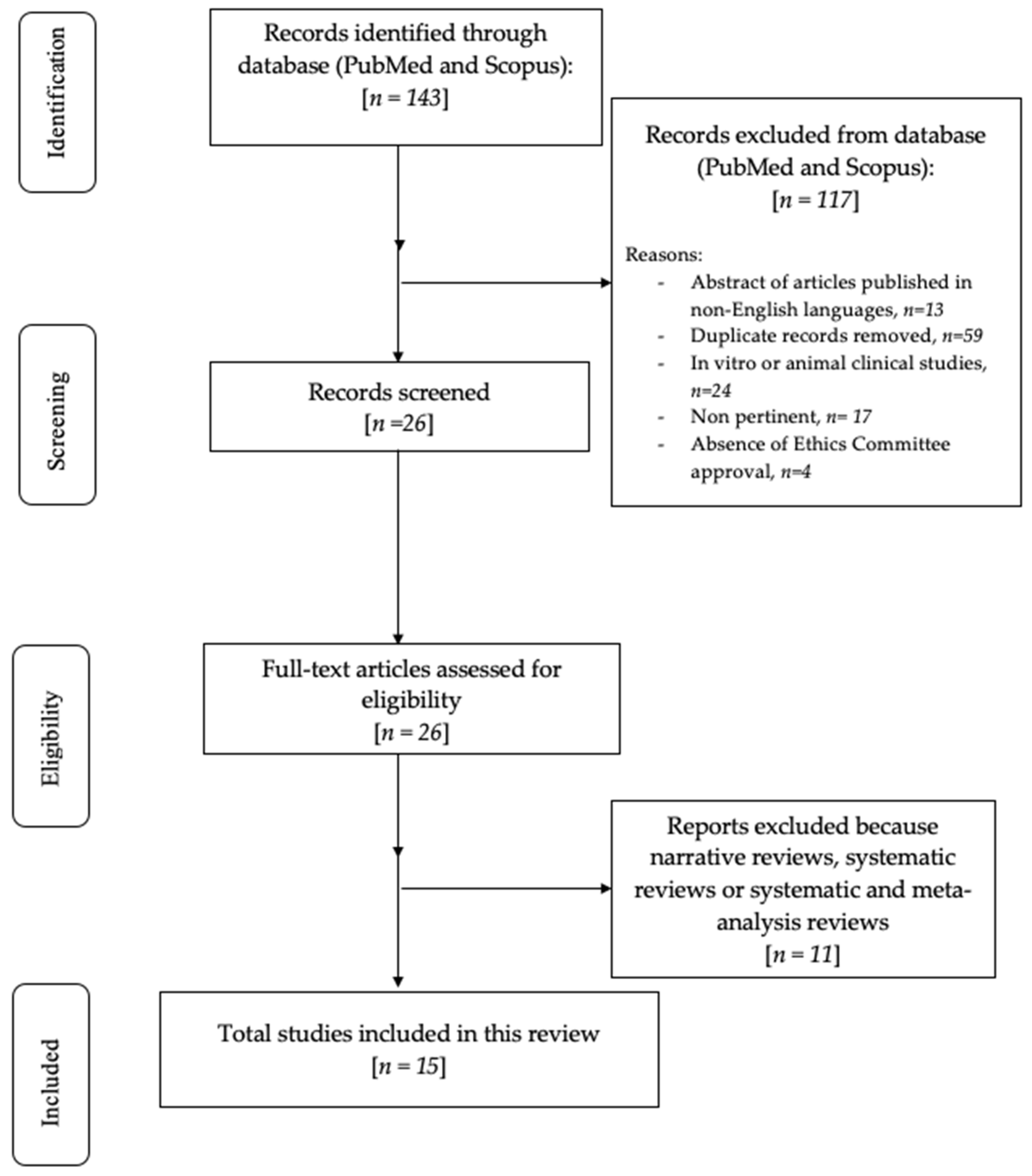
2. Materials and Methods
2.1. Focused Questions
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Research
2.5. Quality Assessment of Included Studies
3. Results
Risk of Bias
4. Discussion
4.1. Bone Defect Dimension
4.2. Aesthetic Aspects
4.3. Biological Considerations
4.4. Clinical Success and Complications
4.5. Early and Late Complication Management
4.6. New Materials
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Protocol Registration
References
- Hansson, S.; Halldin, A. Alveolar ridge resorption after tooth extraction: A consequence of a fundamental principle of bone physiology. J. Dent. Biomech. 2012, 3, 1758736012456543. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2012, 23, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided bone regeneration: Materials and biological mechanisms revisited. Eur. J. Oral Sci. 2017, 125, 315–337. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.M.; Halbritter, S.; Harnisch, H.; Weber, H.P.; Buser, D. A retrospective analysis of patients referred for implant placement to a specialty clinic: Indications, surgical procedures, and early failures. Int. J. Oral Maxillofac. Implant. 2008, 23, 1109–1116. [Google Scholar]
- Retzepi, M.; Donos, N. Guided Bone Regeneration: Biological principle and therapeutic applications. Clin. Oral Implant. Res. 2010, 21, 567–576. [Google Scholar] [CrossRef]
- Ortega-Oller, I.; Padial-Molina, M.; Galindo-Moreno, P.; O’Valle, F.; Jódar-Reyes, A.B.; Peula-García, J.M. Bone Regeneration from PLGA Micro-Nanoparticles. Biomed. Res. Int. 2015, 2015, 415289. [Google Scholar] [CrossRef]
- Padial-Molina, M.; O’Valle, F.; Lanis, A.; Mesa, F.; Dohan Ehrenfest, D.M.; Wang, H.L.; Galindo-Moreno, P. Clinical Application of Mesenchymal Stem Cells and Novel Supportive Therapies for Oral Bone Regeneration. Biomed. Res. Int. 2015, 2015, 341327. [Google Scholar] [CrossRef]
- Gallo, S.; Pascadopoli, M.; Pellegrini, M.; Pulicari, F.; Manfredini, M.; Zampetti, P.; Spadari, F.; Maiorana, C.; Scribante, A. Latest Findings of the Regenerative Materials Application in Periodontal and Peri-Implant Surgery: A Scoping Review. Bioengineering 2022, 9, 594. [Google Scholar] [CrossRef]
- Kormas, I.; Pedercini, A.; Alassy, H.; Wolff, L.F. The Use of Biocompatible Membranes in Oral Surgery: The Past, Present & Future Directions. A Narrative Review. Membranes 2022, 12, 841. [Google Scholar]
- Polo-Corrales, L.; Latorre-Esteves, M.; Ramirez-Vick, J.E. Scaffold design for bone regeneration. J. Nanosci. Nanotechnol. 2014, 14, 15–56. [Google Scholar] [CrossRef]
- Jung, G.; Jeon, J.; Hwang, K.; Park, C. Preliminary evaluation of a three-dimensional, customized, and preformed titanium mesh in peri-implant alveolar bone regeneration. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Badhey, A.; Kadakia, S.; Mourad, M.; Inman, J.; Ducic, Y. Calvarial Reconstruction. Semin. Plast. Surg. 2017, 31, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, I.; Kumar, T.; Kher, U.; Stanitsas, P.D.; Hinrichs, J.E.; Kotsakis, G.A. Clinical results of implant placement in resorbed ridges using simultaneous guided bone regeneration: A multicenter case series. Clin. Oral Investig. 2015, 19, 553–559. [Google Scholar] [CrossRef]
- Poli, P.P.; Beretta, M.; Cicciu, M.; Maiorana, C. Alveolar ridge augmentation with titanium mesh. A retrospective clinical study. Open Dent. J. 2014, 8, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Li, S.Y.; Terheyden, H.; Cao, S.S.; Che, Y.J.; Geng, Y.M. Particulate Coral Hydroxyapatite Sheltered by Titanium Mesh for Localized Alveolar Rehabilitation After Onlay Graft Failure: A Case Report. J. Oral Implantol. 2018, 44, 147–152. [Google Scholar] [CrossRef]
- Maiorana, C.; Manfredini, M.; Beretta, M.; Signorino, F.; Bovio, A.; Poli, P.P. Clinical and Radiographic Evaluation of Simultaneous Alveolar Ridge Augmentation by Means of Preformed Titanium Meshes at Dehiscence-Type Peri-Implant Defects: A Prospective Pilot Study. Materials 2020, 13, 2389. [Google Scholar] [CrossRef]
- Louis, P.J.; Gutta, R.; Said-Al-Naief, N.; Bartolucci, A.A. Reconstruction of the maxilla and mandible with particulate bone graft and titanium mesh for implant placement. J. Oral Maxillofac. Surg. 2008, 66, 235–245. [Google Scholar] [CrossRef]
- Corinaldesi, G.; Pieri, F.; Sapigni, L.; Marchetti, C. Evaluation of survival and success rates of dental implants placed at the time of or after alveolar ridge augmentation with an autogenous mandibular bone graft and titanium mesh: A 3- to 8-year retrospective study. Int. J. Oral Maxillofac. Implant. 2009, 24, 1119–1128. [Google Scholar]
- Maiorana, C.; Santoro, F.; Rabagliati, M.; Salina, S. Evaluation of the use of iliac cancellous bone and anorganic bovine bone in the reconstruction of the atrophic maxilla with titanium mesh: A clinical and histologic investigation. Int. J. Oral Maxillofac. Implant. 2001, 16, 427–432. [Google Scholar]
- Roccuzzo, M.; Ramieri, G.; Bunino, M.; Berrone, S. Autogenous bone graft alone or associated with titanium mesh for vertical alveolar ridge augmentation: A controlled clinical trial. Clin. Oral Implant. Res. 2007, 18, 286–294. [Google Scholar] [CrossRef]
- Poli, P.P.; Beretta, M.; Maiorana, C.; Souza, F.Á.; Bovio, A.; Manfredini, M. Therapeutic Strategies in the Management of Nonresorbable Membrane and Titanium Mesh Exposures Following Alveolar Bone Augmentation: A Systematic Scoping Review. Int. J. Oral Maxillofac. Implant. 2022, 37, 250–269. [Google Scholar] [CrossRef] [PubMed]
- Benic, G.I.; Hämmerle, C.H. Horizontal bone augmentation by means of guided bone regeneration. Periodontol. 2000 2014, 66, 13–40. [Google Scholar] [CrossRef] [PubMed]
- Okubo, T.; Tsukimura, N.; Taniyama, T.; Ishijima, M.; Nakhaei, K.; Rezaei, N.M.; Hirota, M.; Park, W.; Akita, D.; Tateno, A.; et al. Ultraviolet treatment restores bioactivity of titanium mesh plate degraded by contact with medical gloves. J. Oral Sci. 2018, 60, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, A.; Hildebrandt, H.; Schmohl, J.U.; Kämmerer, P.W. Evaluation of risk parameters in bone regeneration using a customized titanium mesh: Results of a clinical study. Implant. Dent. 2019, 28, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Al-Ardah, A.J.; Alqahtani, N.; AlHelal, A.; Goodacre, B.J.; Swamidass, R.; Garbacea, A.; Lozada, J. Using Virtual Ridge Augmentation and 3-Dimensional Printing to Fabricate a Titanium Mesh Positioning Device: A Novel Technique Letter. J. Oral Implantol. 2018, 44, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, A.; Seiler, M. Minimizing risk of customized titanium mesh exposures—A retrospective analysis. BMC Oral Health 2020, 20, 36. [Google Scholar] [CrossRef]
- Inoue, K.; Nakajima, Y.; Omori, M.; Suwa, Y.; Kato-Kogoe, N.; Yamamoto, K.; Kitagaki, H.; Mori, S.; Nakano, H.; Ueno, T. Reconstruction of the Alveolar Bone Using Bone Augmentation With Selective Laser Melting Titanium Mesh Sheet: A Report of 2 Cases. Implant. Dent. 2018, 27, 602–607. [Google Scholar] [CrossRef]
- Ciocca, L.; Fantini, M.; De Crescenzio, F.; Corinaldesi, G.; Scotti, R. Direct metal laser sintering (DMLS) of a customized titanium mesh for prosthetically guided bone regeneration of atrophic maxillary arches. Med. Biol. Eng. Comput. 2011, 49, 1347–1352. [Google Scholar] [CrossRef]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis. 2020. Available online: https://synthesismanual.jbi.global (accessed on 24 April 2023).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Nhlbi, N.I.H. Study Quality Assessment Tool. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 24 April 2023).
- Xie, Y.; Li, S.; Zhang, T.; Wang, C.; Cai, X. Titanium mesh for bone augmentation in oral implantology: Current application and progress. Int. J. Oral Sci. 2020, 12, 37. [Google Scholar] [CrossRef]
- Tolstunov, L.; Hamrick, J.F.E.; Broumand, V.; Shilo, D.; Rachmiel, A. Bone Augmentation Techniques for Horizontal and Vertical Alveolar Ridge Deficiency in Oral Implantology. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 163–191. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Su, Y.; Wang, J.; Wang, X.; Liu, Q.; Wang, J. Effect of Exposure Rates With Customized Versus Conventional Titanium Mesh on Guided Bone Regeneration: Systematic Review and Meta-Analysis. J. Oral Implantol. 2022, 48, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Herford, A.S.; Lowe, I.; Jung, P. Titanium Mesh Grafting Combined with Recombinant Human Bone Morphogenetic Protein 2 for Alveolar Reconstruction. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Casap, N.; Rushinek, H.; Jensen, O.T. Vertical Alveolar Augmentation Using BMP-2/ACS/Allograft with Printed Titanium Shells to Establish an Early Vascular Scaffold. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 473–487. [Google Scholar] [CrossRef]
- Trento, G.S.; Carvalho, P.H.A.; Macedo, D.V.; Gabrielli, M.A.C.; Monnazzi, M.S.; Pereira-Filho, V.A. Titanium mesh associated with rhBMP-2 in alveolar ridge reconstruction. Int. J. Oral Maxillofac. Surg. 2019, 48, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Lim, G.; Lin, G.H.; Monje, A.; Chan, H.L.; Wang, H.L. Wound Healing Complications Following Guided Bone Regeneration for Ridge Augmentation: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Ricci, L.; Perrotti, V.; Ravera, L.; Scarano, A.; Piattelli, A.; Iezzi, G. Rehabilitation of deficient alveolar ridges using titanium grids before and simultaneously with implant placement: A systematic review. J. Periodontol. 2013, 84, 1234–1242. [Google Scholar] [CrossRef]
- Rasia-dal Polo, M.; Poli, P.P.; Rancitelli, D.; Beretta, M.; Maiorana, C. Alveolar ridge reconstruction with titanium meshes: A systematic review of the literature. Med. Oral Patol. Oral Cir. Bucal. 2014, 19, e639–e646. [Google Scholar] [CrossRef]
- Briguglio, F.; Falcomatà, D.; Marconcini, S.; Fiorillo, L.; Briguglio, R.; Farronato, D. The Use of Titanium Mesh in Guided Bone Regeneration: A Systematic Review. Int. J. Dent. 2019, 2019, 9065423. [Google Scholar] [CrossRef]
- Carini, F.; Longoni, S.; Amosso, E.; Paleari, J.; Carini, S.; Porcaro, G. Bone augmentation with TiMesh. autologous bone versus autologous bone and bone substitutes. A systematic review. Ann. Stomatol. 2014, 5, 27–36. [Google Scholar]
- Cucchi, A.; Vignudelli, E.; Franceschi, D.; Randellini, E.; Lizio, G.; Fiorino, A.; Corinaldesi, G. Vertical and horizontal ridge augmentation using customized CAD/CAM titanium mesh with versus without resorbable membranes. A randomized clinical trial. Clin. Oral Implant. Res. 2021, 32, 1411–1424. [Google Scholar] [CrossRef] [PubMed]
- Mounir, M.; Shalash, M.; Mounir, S.; Nassar, Y.; El Khatib, O. Assessment of three-dimensional bone augmentation of severely atrophied maxillary alveolar ridges using prebent titanium mesh vs customized poly-ether-ether-ketone (PEEK) mesh: A randomized clinical trial. Clin. Implant Dent. Relat. Res. 2019, 21, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Cucchi, A.; Bettini, S.; Corinaldesi, G. A novel technique for digitalisation and customisation of reinforced polytetrafluoroethylene meshes: Preliminary results of a clinical trial. Int. J. Oral Implantol. 2022, 15, 129–146. [Google Scholar]
- Lizio, G.; Pellegrino, G.; Corinaldesi, G.; Ferri, A.; Marchetti, C.; Felice, P. Guided bone regeneration using titanium mesh to augment 3-dimensional alveolar defects prior to implant placement. A pilot study. Clin. Oral Implant. Res. 2022, 33, 607–621. [Google Scholar] [CrossRef]
- Dellavia, C.; Canciani, E.; Pellegrini, G.; Tommasato, G.; Graziano, D.; Chiapasco, M. Histological assessment of mandibular bone tissue after guided bone regeneration with customized computer-aided design/computer-assisted manufacture titanium mesh in humans: A cohort study. Clin. Implant Dent. Relat. Res. 2021, 23, 600–611. [Google Scholar] [CrossRef]
- Ciocca, L.; Lizio, G.; Baldissara, P.; Sambuco, A.; Scotti, R.; Corinaldesi, G. Prosthetically CAD-CAM-Guided Bone Augmentation of Atrophic Jaws Using Customized Titanium Mesh: Preliminary Results of an Open Prospective Study. J. Oral Implantol. 2018, 44, 131–137. [Google Scholar] [CrossRef]
- Chiapasco, M.; Casentini, P.; Tommasato, G.; Dellavia, C.; Del Fabbro, M. Customized CAD/CAM titanium meshes for the guided bone regeneration of severe alveolar ridge defects: Preliminary results of a retrospective clinical study in humans. Clin. Oral Implant. Res. 2021, 32, 498–510. [Google Scholar] [CrossRef]
- Navarro Cuéllar, C.; Tousidonis Rial, M.; Antúnez-Conde, R.; Ochandiano Caicoya, S.; Navarro Cuéllar, I.; Arenas de Frutos, G.; Sada Urmeneta, Á.; García-Hidalgo Alonso, M.I.; Navarro Vila, C.; Salmerón Escobar, J.I. Virtual Surgical Planning, Stereolitographic Models and CAD/CAM Titanium Mesh for Three-Dimensional Reconstruction of Fibula Flap with Iliac Crest Graft and Dental Implants. J. Clin. Med. 2021, 10, 1922. [Google Scholar] [CrossRef]
- Yang, W.; Chen, D.; Wang, C.; Apicella, D.; Apicella, A.; Huang, Y.; Li, L.; Zheng, L.; Ji, P.; Wang, L.; et al. The effect of bone defect size on the 3D accuracy of alveolar bone augmentation performed with additively manufactured patient-specific titanium mesh. BMC Oral Health 2022, 22, 557. [Google Scholar] [CrossRef]
- Ghanaati, S.; Al-Maawi, S.; Conrad, T.; Lorenz, J.; Rössler, R.; Sader, R. Biomaterial-based bone regeneration and soft tissue management of the individualized 3D-titanium mesh: An alternative concept to autologous transplantation and flap mobilization. J. Craniomaxillofac. Surg. 2019, 47, 1633–1644. [Google Scholar] [CrossRef]
- Boogaard, M.J.; Santoro, F.; Romanos, G.E. Mesh Ridge Augmentation Using CAD/CAM Technology for Design and Printing: Two Case Reports. Compend. Contin. Educ. Dent. 2022, 43, 654–663. [Google Scholar] [PubMed]
- Nickenig, H.J.; Riekert, M.; Zirk, M.; Lentzen, M.P.; Zöller, J.E.; Kreppel, M. 3D-based buccal augmentation for ideal prosthetic implant alignment-an optimized method and report on 7 cases with pronounced buccal concavities. Clin. Oral Investig. 2022, 26, 3999–4010. [Google Scholar] [CrossRef] [PubMed]
- De Santis, D.; Luciano, U.; Donadello, D.; Faccioni, P.; Zarantonello, M.; Alberti, C.; Verlato, G.; Gelpi, F. Custom Bone Regeneration (CBR): An Alternative Method of Bone Augmentation-A Case Series Study. J. Clin. Med. 2022, 11, 4739. [Google Scholar] [CrossRef] [PubMed]
- Gelețu, G.L.; Burlacu, A.; Murariu, A.; Andrian, S.; Golovcencu, L.; Baciu, E.R.; Maftei, G.; Onica, N. Customized 3D-Printed Titanium Mesh Developed for an Aesthetic Zone to Regenerate a Complex Bone Defect Resulting after a Deficient Odontectomy: A Case Report. Medicina 2022, 58, 1192. [Google Scholar] [CrossRef]
- Tallarico, M.; Park, C.J.; Lumbau, A.I.; Annucci, M.; Baldoni, E.; Koshovari, A.; Meloni, S.M. Customized 3D-Printed Titanium Mesh Developed to Regenerate a Complex Bone Defect in the Aesthetic Zone: A Case Report Approached with a Fully Digital Workflow. Materials 2020, 13, 3874. [Google Scholar] [CrossRef]
- Shi, Y.; Liu, J.; Du, M.; Zhang, S.; Liu, Y.; Yang, H.; Shi, R.; Guo, Y.; Song, F.; Zhao, Y.; et al. Customized Barrier Membrane (Titanium Alloy, Poly Ether-Ether Ketone and Unsintered Hydroxyapatite/Poly-l-Lactide) for Guided Bone Regeneration. Front. Bioeng. Biotechnol. 2022, 10, 916967. [Google Scholar] [CrossRef]
- Matsuo, A.; Chiba, H.; Takahashi, H.; Toyoda, J.; Abukawa, H. Clinical Application of a Custom-Made Bioresorbable Raw Particulate Hydroxyapatite/Poly-L-Lactide Mesh Tray for Mandibular Reconstruction. Odontology 2010, 98, 85–88. [Google Scholar] [CrossRef]
- El Morsy, O.A.; Barakat, A.; Mekhemer, S.; Mounir, M. Assessment of 3-dimensional Bone Augmentation of Severely Atrophied Maxillary Alveolar Ridges Using Patient-specific Poly Ether-ether Ketone (PEEK) Sheets. Clin. Implant Dent. Relat. Res. 2020, 22, 148–155. [Google Scholar] [CrossRef]
- Kadkhodazadeh, M.; Amid, R.; Moscowchi, A. Management of extensive peri-implant defects with titanium meshes. Oral Maxillofac. Surg. 2021, 25, 561–568. [Google Scholar] [CrossRef]
- Windisch, P.; Orban, K.; Salvi, G.E.; Sculean, A.; Molnar, B. Vertical-guided bone regeneration with a titanium-reinforced d-PTFE membrane utilizing a novel split-thickness flap design: A prospective case series. Clin. Oral Investig. 2021, 25, 2969–2980. [Google Scholar] [CrossRef]
- Cuellar, C.N.; Gil, M.C.; Delgado, J.P.; Martínez, B.G.; Sanz, J.A.; de Atalaya, J.L.; Ochandiano, S.; Vila, C.N. Reconstrucción oromandibular con colgajo libre de peroné e implantes osteointegrados. Acta Otorrinolaringol. Esp. 2003, 54, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Iino, M.; Fukuda, M.; Nagai, H.; Hamada, Y.; Yamada, H.; Nakaoka, K.; Mori, Y.; Chikazu, D.; Saijo, H.; Seto, I.; et al. Evaluation of 15 mandibular reconstructions with Dumbach titan mesh-system and particulate cancellous bone and marrow harvested from bilateral posterior ilia. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Farronato, D.; Pasini, P.M.; Orsina, A.A.; Manfredini, M.; Azzi, L.; Farronato, M. Correlation between Buccal Bone Thickness at Implant Placement in Healed Sites and Buccal Soft Tissue Maturation Pattern: A Prospective Three-Year Study. Materials 2020, 13, 511. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco, M.; Casentini, P. Horizontal bone-augmentation procedures in implant dentistry: Prosthetically guided regeneration. Periodontol. 2000 2018, 77, 213–240. [Google Scholar] [CrossRef]
- Lorenz, J.; Al-Maawi, S.; Sader, R.; Ghanaati, S. Individualized Titanium Mesh Combined With Platelet-Rich Fibrin and Deproteinized Bovine Bone: A New Approach for Challenging Augmentation. J. Oral Implantol. 2018, 44, 345–351. [Google Scholar] [CrossRef]
- Lizio, G.; Corinaldesi, G.; Marchetti, C. Alveolar ridge reconstruction with titanium mesh: A three-dimensional evaluation of factors affecting bone augmentation. Int. J. Oral Maxillofac. Implant. 2014, 29, 1354–1363. [Google Scholar] [CrossRef]
- Canullo, L.; Laino, L.; Longo, F.; Filetici, P.; D’Onofrio, I.; Troiano, G. Does chlorhexidine prevent complications in extractive, periodontal, and implant surgery? A systematic review and meta-analysis with trial sequential analysis. Int. J. Oral Maxillofac. Implant. 2020, 35, 1149–1158. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Ramieri, G.; Spada, M.C.; Bianchi, S.D.; Berrone, S. Vertical alveolar ridge augmentation by means of a titanium mesh and autogenous bone grafts. Clin. Oral Implant. Res. 2004, 15, 73–81. [Google Scholar] [CrossRef]
- Al-Ardah, A.J.; AlHelal, A.; Proussaefs, P.; AlBader, B.; Al Humaidan, A.A.; Lozada, J. Managing titanium mesh exposure with partial removal of the exposed site: A case series study. J. Oral Implantol. 2017, 43, 482–490. [Google Scholar] [CrossRef]
- Her, S.; Kang, T.; Fien, M.J. Titanium mesh as an alternative to a membrane for ridge augmentation. J. Oral Maxillofac. Surg. 2012, 70, 803–810. [Google Scholar] [CrossRef]
- Suresh, V.; Anolik, R.; Powers, D. The Utility of Polyether-Ether-Ketone Implants Adjacent to Sinus Cavities after Craniofacial Trauma. J. Oral Maxillofac. Surg. 2018, 76, 2361–2369. [Google Scholar] [CrossRef]
- Honigmann, P.; Sharma, N.; Okolo, B.; Popp, U.; Msallem, B.; Thieringer, F.M. Patient-Specific Surgical Implants Made of 3D Printed PEEK: Material, Technology, and Scope of Surgical Application. Biomed. Res. Int. 2018, 2018, 4520636. [Google Scholar] [CrossRef]
- Salem, D.; Reher, P.; Evans, J.L.; Mansour, M.H. Exploring digital technologies used in the design and manufacture of craniofacial implant surgical guides: A scoping review. J. Prosthet. Dent. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Thakur, J.; Parlani, S.; Shivakumar, S.; Jajoo, K. Accuracy of marginal fit of an implant-supported framework fabricated by 3D printing versus subtractive manufacturing technique: A systematic review and meta-analysis. J. Prosthet. Dent. 2023, 129, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Gallo, S.; Pascadopoli, M.; Pellegrini, M.; Pulicari, F.; Manfredini, M.; Zampetti, P.; Spadari, F.; Maiorana, C.; Scribante, A. CAD/CAM Abutments versus Stock Abutments: An Update Review. Prosthesis 2022, 4, 468–479. [Google Scholar] [CrossRef]
- Cabello-Domínguez, G.; Pérez-López, J.; Veiga-López, B.; González, D.; Revilla-León, M. Maxillary zirconia and mandibular composite resin-lithium disilicate-modified PEEK fixed implant-supported restorations for a completely edentulous patient with an atrophic maxilla and mandible: A clinical report. J. Prosthet. Dent. 2020, 124, 403–410. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Random Sequence Generation | Allocation Concealment | Blinding | Incomplete Outcome Data | Selective Reporting | |
|---|---|---|---|---|---|
| Cucchi et al., 2021 [43] |  |  | | | |
| Mounir et al., 2019 [44] | | | | | |
| Cucchi et al., 2022 [45] | | | | | |
| Lizio et al., 2022 [46] | | | | | |
| Dellavia et al., 2021 [47] | | | | | |
| Ciocca et al., 2018 [48] | | | | | |
| Chiapasco 2021 [49] | | | | | |
| Navarro Cuellar 2021 [50] | | | | | |
| Yang et al., 2022 [51] | | | | | |
| Ghanaati et al., 2019 [52] | | | | | |
| Boogaard et al., 2019 [53] | | | | | |
| Nickenig et al., 2022 [54] | | | | | |
| De Santis et al., 2022 [55] | | | | | |
| Geletu et al., 2022 [56] | | | | | |
| Tallarico et al., 2020 [57] | | | | | |
| References (Authors, Year of Publication, and Study Design) | N° of Patients and % Women | Mean Age (Years), Mean (SD or Range) | Inclusion and Exclusion Criteria | Clinical Outcome |
|---|---|---|---|---|
| Cucchi et al., 2021 [43]: randomized controlled clinical trial | Group 1: 15 W: 53.3% Group 2: 15 W: 46.7% | N.R. | Inclusion criteria: partial edentulism of upper maxilla or mandible with vertical and horizontal bone resorption of the alveolar ridge requiring three-dimensional bone regeneration for prosthetically guided implant placement and capacity to understand and accept the written conditions of the study. Exclusion criteria: insufficient oral hygiene; smoking habit of >10 cigarettes/day; abuse of alcohol or drugs; pregnancy, acute local or systemic infections; uncontrolled diabetes or other metabolic diseases; severe hepatic or renal dysfunction; autoimmune disorders; patients who underwent radiotherapy in the last 5 years and patients undergoing immunosuppressive therapy or immunocompromised patients. | Complex bone defects |
| Mounir et al., 2019 [44]: randomized controlled clinical trial | Group 1: 8 W: 25% Group 2: 8 W: 50% | Group 1: 38 Group 2: 39 | Inclusion criteria: patients who had a partial or completely edentulous maxillary alveolar ridge with apparent 3D defect following teeth loss. The ridge had to exhibit severe vertical and horizontal (3D) alveolar ridge deficiency with alveolar ridge height less than 6 mm from the alveolar crest to the basal bone and a ridge width of less than 2 mm or a clinically apparent increase in inter-arch space relative to the adjacent natural teeth. Exclusion criteria: N.R. | Complex bone defects |
| Cucchi et al., 2022 [45]: preliminary clinical trial | 10 W: 50% | 54 | Inclusion criteria: age > 18 years;partial edentulism of the maxilla or mandible; VBD requiring 3D bone augmentation for prosthetically guided implant placement; informed consent for experimental treatment and processing of personal data. Exclusion criteria: poor oral hygiene; untreated periodontal disease; smoking > 10 cigarettes per day; abuse of alcohol or drugs; pregnancy; presence of odontostomatological and/or systemic infections; metabolic, liver, kidney, or autoimmune disease; radiotherapy in the head and neck region in the last 5 years; patients undergoing immunosuppressive therapy and/or immunocompromised patients. | Optimal bone regeneration: 90% |
| Lizio et al., 2022 [46]: retrospective clinical study | 17 W: 70.6% | 55.9 ± 13.7 | Inclusion criteria: the absence of any systemic or local contraindication to surgical treatment: acute or chronic infections in the head and neck; smoking > 10 cigarettes per day; uncontrolled diabetes; a history of radiation therapy in the head or neck region; current anti-tumor chemotherapy; liver, blood, or kidney disease; immunosuppression; everyday corticosteroid use; pregnancy; inflammatory and autoimmune disease of the oral cavity; and poor oral hygiene and motivation. The specific conditions for intervention were the presence of maxillary or mandibular complex defects (with horizontal and vertical deficits in the same site), which was considered inadequate for the placement of at least two standard fixtures (≥6 mm long and ≥3.3 wide). | Optimal bone regeneration: 88% |
| Dellavia et al., 2021 [47]: retrospective cohort study | 20 W: 75% | 43–81 | Inclusion criteria: age > 18 years, general good health conditions, adequate compliance both in terms of home oral hygiene maneuvers and in the ability to show up at the controls and to have completely understanding informed consent. Furthermore, in the posterior mandibular edentulous sites, they presented severe bone atrophy incompatible with placement of even short (≤6 mm) or narrow (<3 mm) implants in an appropriate and prosthetically guided position. Exclusion criteria: systemic diseases and conditions conflicting with GBR and implant placement: severe kidney and/or liver disease, congenital or acquired immunodeficiency, ongoing antiblastic chemotherapy at the time of first examination, sequelae of radiotherapy in the head and neck area, smoking > 10 cigarettes per day, alcohol abuse, non-compensated diabetes, bisphosphonate chemotherapy in progress and pregnant women, patients with diseases of oral mucosa (lichen planus, FMPS, and FMBS > 20%, active periodontal disease) | Regeneration of vital, well-structured, and vascularized alveolar bone |
| Ciocca et al., 2018 [48]: preliminary prospective study | 9 W: 66.7% | 50 (25–68) | Inclusion criteria: N.R. Exclusion criteria: N.R. | High post-operative morbidity related to mesh exposure |
| Chiapasco 2021 [49]: retrospective clinical study | 41 W: 75.6% | 53.98 ± 14.32 (20–81) | Inclusion criteria: systemically healthy patients; a minimum age of 18 years; relevant or severe bone atrophy at the edentulous sites incompatible with placement of even short (≤6 mm) or narrow (<3 mm) implants in an appropriate and prosthetically guided position; adequate compliance of patients, both in terms of oral hygiene and respect the follow-up recalls; and ability to understand the proposed surgical treatment and to understand and sign the informed consent. Exclusion criteria: severe kidney and/or liver disease; congenital or acquired immunodeficiency; ongoing antiblastic chemotherapy at the time of first examination; sequelae of radiotherapy in the head and neck area; oral mucosa disease, such as lichen planus; FMPS and FMBS > 20%; non-compliant patients; tobacco (>10 cigarettes per day) or alcohol abuse; non compensated diabetes; active periodontal disease at the time of first examination (in these cases, patients underwent etiologic therapy and motivation in personal oral hygiene and were re-evaluated for surgical treatment); bisphosphonate chemotherapy in progress; and pregnant women. | Severe bone defects |
| Navarro Cuellar et al., 2021 [50]: retrospective clinical study | 8 W: 37.5% | N.R. | Inclusion criteria: Oncologic patients treated with segmental mandibulectomy and reconstructed with fibula flap; patients with traumatic injuries and mandibular segmental defects reconstructed with fibula flap; patients with three-dimensional discrepancy between the native mandible and the fibula flap; VSP, stereolitographic models, and CAD/CAM titanium mesh for 3D fibula reconstruction; and Cortico-cancellous iliac crest graft. Exclusion criteria: segmental mandibular defects reconstructed with double-barrel fibula flap and patients who previously underwent vertical distraction of the fibula flap. | Aesthetic and functional results |
| Yang et al., 2022 [51]: retrospective clinical study | Group 1: 10 Group 2: 10 W: 40% | 35.7 (21–56) | Inclusion criteria: adults (at least 18 years); with good physical health, willing to actively cooperate with the clinical study; had undergone implant placement 6~9 months after GBR therapy with patient-specific titanium mesh in the first period. Exclusion criteria: No regular follow-up information; without complete imaging data. | Effective for minor and major bone defects |
| Ghanaati et al., 2019 [52]: case series | 7 W: 71.4% | 41 | Inclusion criteria: N.R. Exclusion criteria: N.R. | Complex bone defects |
| Boogaard et al., 2019 [53]: case series | 2 W: 50% | 59.5 | Inclusion criteria: N.R. Exclusion criteria: N.R. | Complex bone defects |
| Nickenig et al., 2022 [54]: case series | 3 W: 66.7% | 23.6 | Inclusion criteria: N.R. Exclusion criteria: N.R. | Aesthetic results in severe bone defects |
| De Santis et al., 2022 [55]: case series | 9 W: 66.7% | 53.11 ± 6.79 43–65 |
| Severe or complex bone defects |
| Geletu et al., 2022 [56]: case report | 1 W: 100% | 27 | Inclusion criteria: N.R. Exclusion criteria: N.R. | Aesthetic maxillary defects |
| Tallarico et al., 2020 [57]: case report | 1 W: 100% | 19 | Inclusion criteria: N.R. Exclusion criteria: N.R. | Aesthetic maxillary defects |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scribante, A.; Ghizzoni, M.; Pellegrini, M.; Pulicari, F.; Manfredini, M.; Poli, P.P.; Maiorana, C.; Spadari, F. Full-Digital Customized Meshes in Guided Bone Regeneration Procedures: A Scoping Review. Prosthesis 2023, 5, 480-495. https://doi.org/10.3390/prosthesis5020033
Scribante A, Ghizzoni M, Pellegrini M, Pulicari F, Manfredini M, Poli PP, Maiorana C, Spadari F. Full-Digital Customized Meshes in Guided Bone Regeneration Procedures: A Scoping Review. Prosthesis. 2023; 5(2):480-495. https://doi.org/10.3390/prosthesis5020033
Chicago/Turabian StyleScribante, Andrea, Martina Ghizzoni, Matteo Pellegrini, Federica Pulicari, Mattia Manfredini, Pier Paolo Poli, Carlo Maiorana, and Francesco Spadari. 2023. "Full-Digital Customized Meshes in Guided Bone Regeneration Procedures: A Scoping Review" Prosthesis 5, no. 2: 480-495. https://doi.org/10.3390/prosthesis5020033