
The Success and Complications of Complete-Arch Implant-Supported Fixed Monolithic Zirconia Restorations: A Systematic Review

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Source of Information and Research Strategy
2.2. Eligibility Criteria
2.3. Screening and Data Extraction
2.4. Quality Assessment/Risk of Bias
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Mechanical/Structural Complications
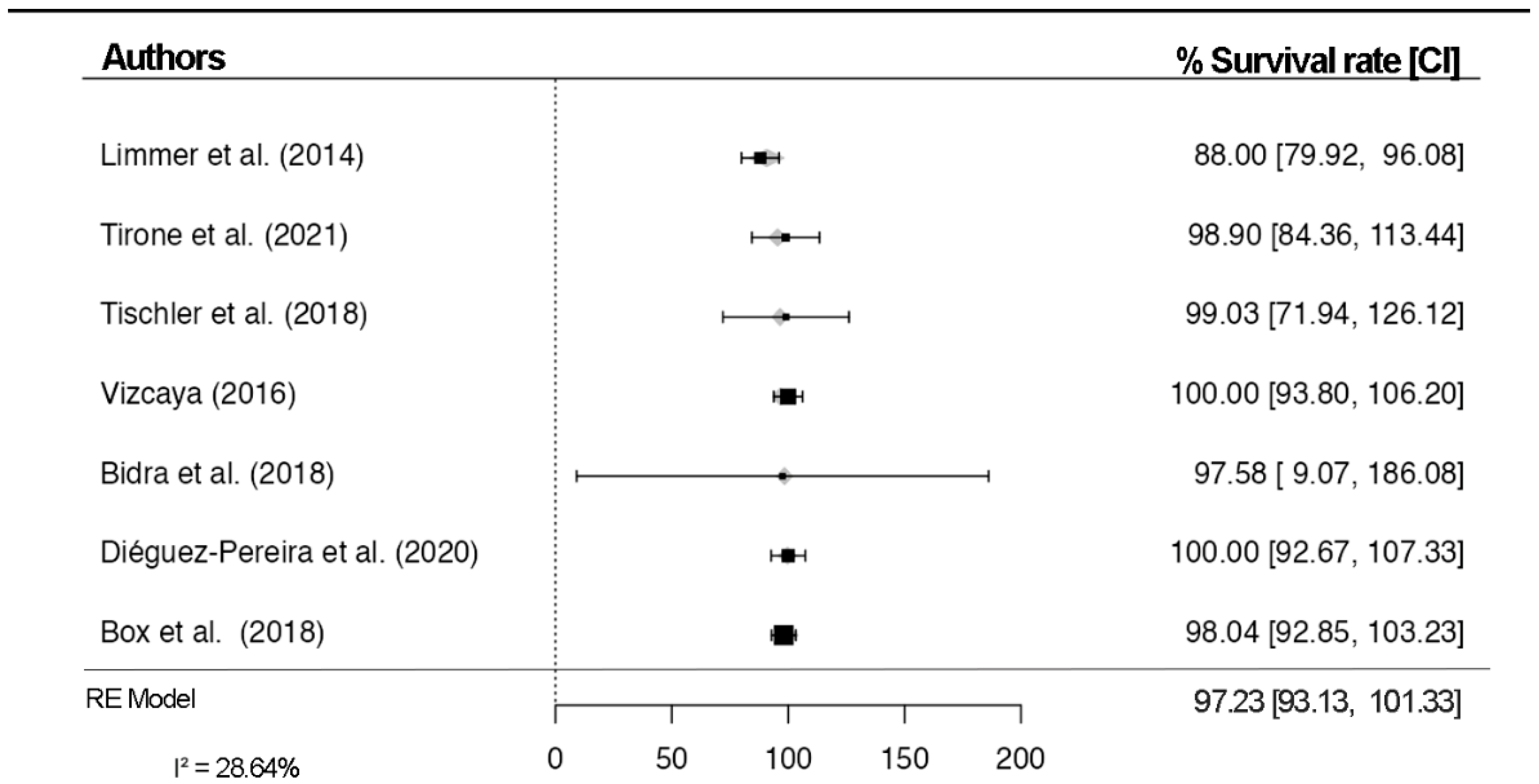
4.2. Survival Rate
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bidra, A.S.; Rungruanganunt, P.; Gauthier, M. Clinical outcomes of full arch fixed implant-supported zirconia prostheses: A systematic review. Eur. J. Oral. Implantol. 2017, 10 (Suppl. 1), 35–45. [Google Scholar] [PubMed]
- Carames, J.; Marques, D.; Malta Barbosa, J.; Moreira, A.; Crispim, P.; Chen, A. Full-arch implant-supported rehabilitations: A prospective study comparing porcelain-veneered zirconia frameworks to monolithic zirconia. Clin. Oral. Implant. Res. 2019, 30, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Barbin, T.; Silva, L.D.R.; Veloso, D.V.; Borges, G.A.; Presotto, A.G.C.; Barao, V.A.R.; Groppo, F.C.; Mesquita, M.F. Biomechanical behavior of CAD/CAM cobalt-chromium and zirconia full-arch fixed prostheses. J. Adv. Prosthodont. 2020, 12, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Dieguez-Pereira, M.; Chavarri-Prado, D.; Estrada-Martinez, A.; Perez-Pevida, E.; Brizuela-Velasco, A. Monolithic and Minimally Veneered Zirconia Complications as Implant-Supported Restorative Material: A Retrospective Clinical Study up to 5 Years. Biomed. Res. Int. 2020, 2020, 8821068. [Google Scholar] [CrossRef]
- Gonzalez-Gonzalez, I.; Dellanos-Lanchares, H.; Brizuela-Velasco, A.; Alvarez-Riesgo, J.-A.; Llorente-Pendas, S.; Herrero-Climent, M.; Alvarez-Arenal, A. Complications of Fixed Full-Arch Implant-Supported Metal-Ceramic Prostheses. Int. J. Environ. Res. Public Health 2020, 17, 4250. [Google Scholar] [CrossRef]
- Nazari, V.; Ghodsi, S.; Alikhasi, M.; Sahebi, M.; Shamshiri, A.R. Fracture Strength of Three-Unit Implant Supported Fixed Partial Dentures with Excessive Crown Height Fabricated from Different Materials. J. Dent. 2016, 13, 400–406. [Google Scholar]
- Cevik, P.; Schimmel, M.; Yilmaz, B. New generation CAD-CAM materials for implant-supported definitive frameworks fabricated by using subtractive technologies. Biomed. Res. Int. 2022, 2022, 3074182. [Google Scholar] [CrossRef]
- Alarcón-Sánchez, M.A.; Heboyan, A.; Fernandes, G.V.O.; Castro-Alarcón, N.; Romero-Castro, N.S. Potential Impact of Prosthetic Biomaterials on the Periodontium: A Comprehensive Review. Molecules 2023, 28, 1075. [Google Scholar] [CrossRef]
- Desai, S.R.; Koulgikar, K.D.; Alqhtani, N.R.; Alqahtani, A.R.; Alqahtani, A.S.; Alenazi, A.; Heboyan, A.; Fernandes, G.V.O.; Mustafa, M. Three-Dimensional FEA Analysis of the Stress Distribution on Titanium and Graphene Frameworks Supported by 3 or 6-Implant Models. Biomimetics 2023, 8, 15. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Scarano, A.; Cortellari, G.C.; Fernandes, G.V.O.; Mesquita, A.M.M.; Bianchini, M.A. Marginal Bone Level and Biomechanical Behavior of Titanium-Indexed Abutment Base of Conical Connection Used for Single Ceramic Crowns on Morse-Taper Implant: A Clinical Retrospective Study. J. Funct. Biomater. 2023, 14, 128. [Google Scholar] [CrossRef]
- Tischler, M.; Patch, C.; Bidra, A.S. Rehabilitation of edentulous jaws with zirconia complete-arch fixed implant-supported prostheses: An up to 4-year retrospective clinical study. J. Prosthet. Dent. 2018, 120, 204–209. [Google Scholar] [CrossRef]
- Ferro, K.J.; Morgano, S.M.; Driscoll, C.F.; Freilich, M.A.; Guckes, A.D.; Knoernschild, K.L.; McGarry, T.J. The Glossary of Prosthodontic Terms: Ninth Edition. J. Prosthet. Dent. 2017, 117, e1–e105. [Google Scholar]
- Apratim, A.; Eachempati, P.; Krishnappa Salian, K.K.; Singh, V.; Chhabra, S.; Shah, S. Zirconia in dental implantology: A review. J. Int. Soc. Prev. Community Dent. 2015, 5, 147–156. [Google Scholar] [CrossRef]
- Borges, H.; Correia, A.R.M.; Castilho, R.M.; Fernandes, G.V.O. Zirconia Implants and Marginal Bone Loss: A Systematic Review and Meta-Analysis of Clinical Studies. Int. J. Oral. Maxillofac. Implants. 2020, 35, 707–720. [Google Scholar] [CrossRef]
- Bona, A.D.; Pecho, O.E.; Alessandretti, R. Zirconia as a Dental Biomaterial. Materials 2015, 8, 4978–4991. [Google Scholar] [CrossRef]
- Bidra, A.S.; Tischler, M.; Patch, C. Survival of 2039 complete arch fixed implant-supported zirconia prostheses: A retrospective study. J. Prosthet. Dent. 2018, 119, 220–224. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Bordin, T.B.; Natto, Z.S.; El-Rafie, K.; Pagni, S.E.; Chochlidakis, K.; Ercoli, C.; Weber, H.-P. Complications and survival rates of 55 metal-ceramic implant-supported fixed complete-arch prostheses: A cohort study with mean 5- year follow-up. J. Prosthet. Dent. 2019, 122, 441–449. [Google Scholar] [CrossRef]
- Esquivel-Upshaw, J.; Kim, M.; Hsu, S.; Abdulhameed, N.; Jenkins, R.; Neal, D.; Ren, F.; Clark, A. Randomized clinical study of wear of enamel antagonists against polished monolithic zirconia crowns. J. Dent. 2018, 68, 19–27. [Google Scholar] [CrossRef]
- Stober, T.; Bermejo, J.L.; Rammelsberg, P.; Schmitter, M. Enamel wear caused by monolithic zirconia crowns after 6 months of clinical use. J. Oral. Rehabil. 2014, 41, 314–322. [Google Scholar] [CrossRef]
- Sailer, I.; Balmer, M.; Husler, J.; Hammerle, C.H.F.; Kanel, S.; Thoma, D.S. 10- year randomized trial (RCT) of zirconia-ceramic and metal-ceramic fixed dental prostheses. J. Dent. 2018, 76, 32–39. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Tan, K.; Lang, N.P.; Bragger, U.; Egger, M.; Zwahlen, M. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. Clin. Oral. Implant. Res. 2004, 15, 625–642. [Google Scholar] [CrossRef]
- Tirone, F.; Salzano, S.; Rolando, E.; Pozzatti, L.; Rodi, D. Framework Fracture of Zirconia Supported Full Arch Implant Rehabilitation: A Retrospective Evaluation of Cantilever Length and Distal Cross-Sectional Connection Area in 140 Patients Over an Up-To-7 Year Follow-Up Period. J. Prosthodont. 2022, 31, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Franco, A.; Vidigal, M.T.C.; de Oliveira, M.N.; de Nascimento, C.T.; da Silva, R.F.; Paranhos, L.R. Evidence-based mapping of third molar techniques for age estimation applied to Brazilian adolescents—A systematic review. Res. Soc. Dev. 2020, 9, e9339109395. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 6th ed.; Cochrane: London, UK, 2019. [Google Scholar]
- Box, V.H.; Sukotjo, C.; Knoernschild, K.L.; Campbell, S.D.; Afshari, F.S. Patient-Reported and Clinical Outcomes of Implant-Supported Fixed Complete Dental Prostheses: A Comparison of Metal-Acrylic, Milled Zirconia, and Retrievable Crown Prostheses. J. Oral. Implantol. 2018, 44, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Limmer, B.; Sanders, A.E.; Reside, G.; Cooper, L.F. Complications and patient-centered outcomes with an implant-supported monolithic zirconia fixed dental prosthesis: 1 year results. J. Prosthodont. 2014, 23, 267–275. [Google Scholar] [CrossRef]
- Rojas Vizcaya, F. Retrospective 2- to 7-Year Follow-Up Study of 20 Double Full-Arch Implant-Supported Monolithic Zirconia Fixed Prostheses: Measurements and Recommendations for Optimal Design. J. Prosthodont. 2018, 27, 501–508. [Google Scholar] [CrossRef]
- Ferreira, P.W.; Nogueira, P.J.; Nobre, M.A.A.; Guedes, C.M.; Salvado, F. Impact of Mechanical Complications on Success of Dental Implant Treatments: A Case-Control Study. Eur. J. Dent. 2022, 16, 179–187. [Google Scholar] [CrossRef]
- Ettl, T.; Junold, N.; Zeman, F.; Hautmann, M.; Hahnel, S.; Kolbeck, C.; Müller, S.; Klingelhöffer, C.; Reichert, T.E.; Meier, J.K. Implant survival or implant success? Evaluation of implant-based prosthetic rehabilitation in head and neck cancer patients-a prospective observational study. Clin. Oral. Investig. 2020, 24, 3039–3047. [Google Scholar] [CrossRef]
- Chang, J.S.; Ji, W.; Choi, C.H.; Kim, S. Catastrophic failure of a monolithic zirconia prosthesis. J. Prosthet. Dent. 2015, 113, 86–90. [Google Scholar] [CrossRef]
- Durkan, R.; Oyar, P.; Deste, G. Effects of Cantilever Length and Implant Inclination on the Stress Distribution of Mandibular Prosthetic Restorations Constructed from Monolithic Zirconia Ceramic. Int. J. Oral. Maxillofac. Implant. 2020, 35, 121–129. [Google Scholar] [CrossRef]
- Alshahrani, F.A.; Yilmaz, B.; Seidt, J.D.; McGlumphy, E.A.; Brantley, W.A. A load-to-fracture and strain analysis of monolithic zirconia cantilevered frameworks. J. Prosthet. Dent. 2017, 118, 752–758. [Google Scholar] [CrossRef]
- Sailer, I.; Muhlemann, S.; Zwahlen, M.; Hammerle, C.H.; Schneider, D. Cemented and screw-retained implant reconstructions: A systematic review of the survival and complication rates. Clin. Oral. Implant. Res. 2012, 23 (Suppl. 6), 163–201. [Google Scholar] [CrossRef]
- Wright, S.P.; Hayden, J.; Lynd, J.A.; Walker-Finch, K.; Willett, J.; Ucer, C.; Speechley, S.D. Factors affecting the complexity of dental implant restoration—What is the current evidence and guidance? Br. Dent. J. 2016, 221, 615–622. [Google Scholar] [CrossRef]
- Gaddale, R.; Mishra, S.K.; Chowdhary, R. Complications of screw- and cement-retained implant-supported full-arch restorations: A systematic review and meta-analysis. Int. J. Oral. Implantol. 2020, 13, 11–40. [Google Scholar]
- Oda, Y.; Mori, G.; Sasaki, H.; Furuya, Y.; Ito, T.; Iijima, T.; Sekine, H.; Yajima, Y. Dimensional changes of buccal bone in the edentulous maxilla with telescopic-retained implant-supported fixed dental prostheses. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef]
- Waltimo, A.; Kononen, M. A novel bite force recorder and maximal isometric bite force values for healthy young adults. Scand J. Dent. Res. 1993, 101, 171–175. [Google Scholar] [CrossRef]
- Cosme, D.C.; Baldisserotto, S.M.; Andrade, C.S.; Shinkai, R.S. Bruxism and voluntary maximal bite force in young dentate adults. Int. J. Prosthodont. 2005, 18, 328–332. [Google Scholar]
- Umesh, S.; Padma, S.; Asokan, S.; Srinivas, T. Fiber Bragg Grating based bite force measurement. J. Biomech. 2016, 49, 2877–2881. [Google Scholar] [CrossRef]
- Gonzalez, J.; Triplett, R.G. Complications and Clinical Considerations of the Implant-Retained Zirconia Complete-Arch Prosthesis with Various Opposing Dentitions. Int. J. Oral. Maxillofac. Implant. 2017, 32, 864–869. [Google Scholar] [CrossRef]
- Calderon, U.; Hicklin, S.; Mojon, P.; Fehmer, V.; Nesic, D.; Mekki, M.; Sailer, I. Influence of the Titanium Base Abutment Design on Monolithic Zirconia Multiple-Unit Implant Fixed Dental Prostheses: A Laboratory Study. Int. J. Oral. Maxillofac. Implant. 2022, 37, 19–29. [Google Scholar] [CrossRef]
- Carames, J.; Tovar Suinaga, L.; Yu, Y.C.; Perez, A.; Kang, M. Clinical Advantages and Limitations of Monolithic Zirconia Restorations Full Arch Implant Supported Reconstruction: Case Series. Int. J. Dent. 2015, 2015, 392496. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Oh, S.H.; Kim, J.H.; Ju, S.W.; Seo, D.G.; Jun, S.H.; Ahn, J.S.; Ryu, J.J. Wear evaluation of the human enamel opposing different Y-TZP dental ceramics and other porcelains. J. Dent. 2012, 40, 979–988. [Google Scholar] [CrossRef] [PubMed]
- Rammelsberg, P.; Meyer, A.; Lorenzo-Bermejo, J.; Kappel, S.; Zenthofer, A. Long-term chipping and failure rates of implant-supported and combined tooth-implant-supported metal-ceramic and ceramic fixed dental prostheses: A cohort study. J. Prosthet. Dent. 2021, 126, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Schwindling, F.S.; Waldecker, M.; Rammelsberg, P.; Rues, S.; Bomicke, W. Tooth substance removal for ceramic single crown materials-an in vitro comparison. Clin. Oral. Investig. 2019, 23, 3359–3366. [Google Scholar] [CrossRef]
- Sripetchdanond, J.; Leevailoj, C. Wear of human enamel opposing monolithic zirconia, glass ceramic, and composite resin: An in vitro study. J. Prosthet. Dent. 2014, 112, 1141–1150. [Google Scholar] [CrossRef]
- Jung, Y.S.; Lee, J.W.; Choi, Y.J.; Ahn, J.S.; Shin, S.W.; Huh, J.B. A study on the in-vitro wear of the natural tooth structure by opposing zirconia or dental porcelain. J. Adv. Prosthodont. 2010, 2, 111–115. [Google Scholar] [CrossRef]
- Barootchi, S.; Askar, H.; Ravida, A.; Gargallo-Albiol, J.; Travan, S.; Wang, H.L. Long-term Clinical Outcomes and Cost-Effectiveness of Full-Arch Implant-Supported Zirconia-Based and Metal-Acrylic Fixed Dental Prostheses: A Retrospective Analysis. Int. J. Oral. Maxillofac. Implant. 2020, 35, 395–405. [Google Scholar] [CrossRef]
- Carames, J.M.M.; da Mata, A.D.S.P.; da Silva Marques, D.N.; de Oliveira Francisco, H.C. Ceramic-Veneered Zirconia Frameworks in Full-Arch Implant Rehabilitations: A 6-Month to 5-Year Retrospective Cohort Study. Int. J. Oral. Maxillofac. Implant. 2016, 31, 1407–1414. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| MESH Terms (PubMed) | MESH Search (PubMed) |
|---|---|
|
|
| “Natural language” terms (PubMed) | Free text search (PubMed) |
| P: edentulous I: complete-arch implant-supported monolithic zirconia fixed dental prostheses, complete-arch implant-supported fixed dental prostheses C: metal-ceramic implant-supported fixed dental prostheses O: “technical complications” | complete-arch implant-supported monolithic zirconia fixed dental prostheses “complete-arch” [All Fields] AND “implant-supported” [All Fields] AND (“monolith” [All Fields] OR “monolithic” [All Fields] OR “monolithically” [All Fields] OR “monolithics” [All Fields] OR “monoliths” [All Fields]) AND (“zirconia s” [All Fields] OR “zirconias” [All Fields] OR “zirconium oxide” [Supplementary Concept] OR “zirconium oxide” [All Fields] OR “zirconia” [All Fields]) AND (“fixatives” [Pharmacological Action] OR “fixatives” [MeSH Terms] OR “fixatives” [All Fields] OR “fixative” [All Fields] OR “fixed” [All Fields] OR “fixes” [All Fields] OR “fixing” [All Fields] OR “fixings” [All Fields]) AND (“dental prosthesis”[MeSH Terms] OR (“dental” [All Fields] AND “prosthesis” [All Fields]) OR “dental prosthesis” [All Fields] OR (“dental” [All Fields] AND “prostheses” [All Fields]) OR “dental prostheses” [All Fields]) complete-arch implant-supported fixed dental prostheses “complete-arch” [All Fields] AND “implant-supported” [All Fields] AND (“fixatives” [Pharmacological Action] OR “fixatives” [MeSH Terms] OR “fixatives” [All Fields] OR “fixative” [All Fields] OR “fixed” [All Fields] OR “fixes” [All Fields] OR “fixing” [All Fields] OR “fixings” [All Fields]) AND (“dental prosthesis” [MeSH Terms] OR (“dental” [All Fields] AND “prosthesis” [All Fields]) OR “dental prosthesis” [All Fields] OR (“dental” [All Fields] AND “prostheses” [All Fields]) OR “dental prostheses” [All Fields]) |
| Web of Science search | |
| complete arch implant-supported monolithic zirconia fixed dental prostheses | |
| full arch implant-supported monolithic zirconia fixed dental prostheses | |
| TS = (implant-supported fixed dental prostheses) AND TS = (monolithic zirconia) | |
| Author | Title | Study Design | Patients (n) | Prostheses (n) | Average Age |
|---|---|---|---|---|---|
| Bidra et al. (2018) [16] | Survival of 2039 complete arch fixed implant-supported zirconia prostheses: a retrospective study | retrospective study | N/A | 2039 | N/A |
| Tischler et al. (2018) [5] | Rehabilitation of edentulous jaws with zirconia complete-arch fixed implant-supported prostheses: an up to 4-year retrospective clinical study | retrospective study | 128 | 191 | N/A |
| Box et al. (2018) [25] | Patient-reported and clinical outcomes of implant-supported fixed complete dental prostheses: a comparison of metal-acrylic, milled zirconia, and retrievable crown prostheses | retrospective study | 5 | 7 | 63.0 |
| Dieguez-Pereira et al. (2020) [14] | Monolithic and minimally veneered zirconia complications as implant-supported restorative material: a retrospective clinical study up to 5 years | retrospective study | N/A | 14 | 56.3 |
| Tirone et al. (2022) [22] | Framework fracture of zirconia supported full arch implant rehabilitation: a retrospective evaluation of cantilever length and distal cross-sectional connection area in 140 patients over an up-to 7-year follow-up period | retrospective study | 41 | 55 | 63.0 |
| Rojas Vizcaya (2018) [27] | Retrospective 2-to 7-year follow-up study of 20 double full-arch implant-supported monolithic zirconia fixed prostheses: measurements and recommendations for the optimal design | retrospective study | 10 | 20 | 60.0 |
| Limmer et al. (2014) [26] | Complications and patient-centered outcomes with implant-supported monolithic zirconia fixed dental prosthesis: 1-year results | retrospective study | 17 | 17 | 57.9 |
| Author | Prosthesis Site | Trademark of Zirconia | Retention | No. of Implants/Arch | Follow-Up (Months) | Survival Rate | Complications |
|---|---|---|---|---|---|---|---|
| Bidra et al. (2018) [16] | N/A | Zirconia Prettau®zircon tooth | Screw-retained | N/A | 60 | 1 year (2039 prostheses): 99.85% 5 years (69 prostheses): 99.3% |
|
| Tischler et al. (2018) [5] | 102 maxilla 89 mandible (65 double arches) | Zirconia Prettau®zircon tooth | Screw-retained | 6—maxilla 5—mandible | 48 | Implant—98.8% Zirconia—99.4% Treatment—98.9% |
|
| Box et al. (2018) [25] | 5 maxilla 2 mandible (2 double arches) | N/A | Screw-retained | Between 4 and 6 | 70 | 98.04% |
|
| Dieguez-Pereira et al. (2020) [14] | N/A | Zahn Dental Labs | Screw-retained | N/A | 68 | 100% |
|
| Tirone et al. (2021) [22] | Double arches | Amann Girrbach® | Screw-retained | All-on-4 and All-on-6 | 41.6 | 98.9% |
|
| Rojas Vizcaya (2016) [27] | 10 double arches | Zirconia Prettau®zircon tooth | Screw-retained | 8—maxilla 4 to 6—mandible | 48.6 | 100% |
|
| Limmer et al. (2014) [26] | 17 mandibles | Zirconia Prettau®zircon tooth | Screw-retained | 4—mandible | 12 | 88% |
|
| Author | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total | % |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bidra et al. (2018) [16] | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 8 | 72.72 |
| Tischler et al. (2018) [5] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 10 | 90.91 |
| Box et al. (2018) [25] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 9 | 81.82 |
| Dieguez-Pereira et al. (2020) [14] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 9 | 81.82 |
| Tirone et al. (2021) [22] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 100 |
| Rojas Vizcaya (2016) [27] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 100 |
| Limmer et al. (2014) [26] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vozzo, L.M.; Azevedo, L.; Fernandes, J.C.H.; Fonseca, P.; Araújo, F.; Teixeira, W.; Fernandes, G.V.O.; Correia, A. The Success and Complications of Complete-Arch Implant-Supported Fixed Monolithic Zirconia Restorations: A Systematic Review. Prosthesis 2023, 5, 425-436. https://doi.org/10.3390/prosthesis5020029
Vozzo LM, Azevedo L, Fernandes JCH, Fonseca P, Araújo F, Teixeira W, Fernandes GVO, Correia A. The Success and Complications of Complete-Arch Implant-Supported Fixed Monolithic Zirconia Restorations: A Systematic Review. Prosthesis. 2023; 5(2):425-436. https://doi.org/10.3390/prosthesis5020029
Chicago/Turabian StyleVozzo, Ludovico Maria, Luís Azevedo, Juliana Campos Hasse Fernandes, Patrícia Fonseca, Filipe Araújo, Wendel Teixeira, Gustavo Vicentis Oliveira Fernandes, and André Correia. 2023. "The Success and Complications of Complete-Arch Implant-Supported Fixed Monolithic Zirconia Restorations: A Systematic Review" Prosthesis 5, no. 2: 425-436. https://doi.org/10.3390/prosthesis5020029