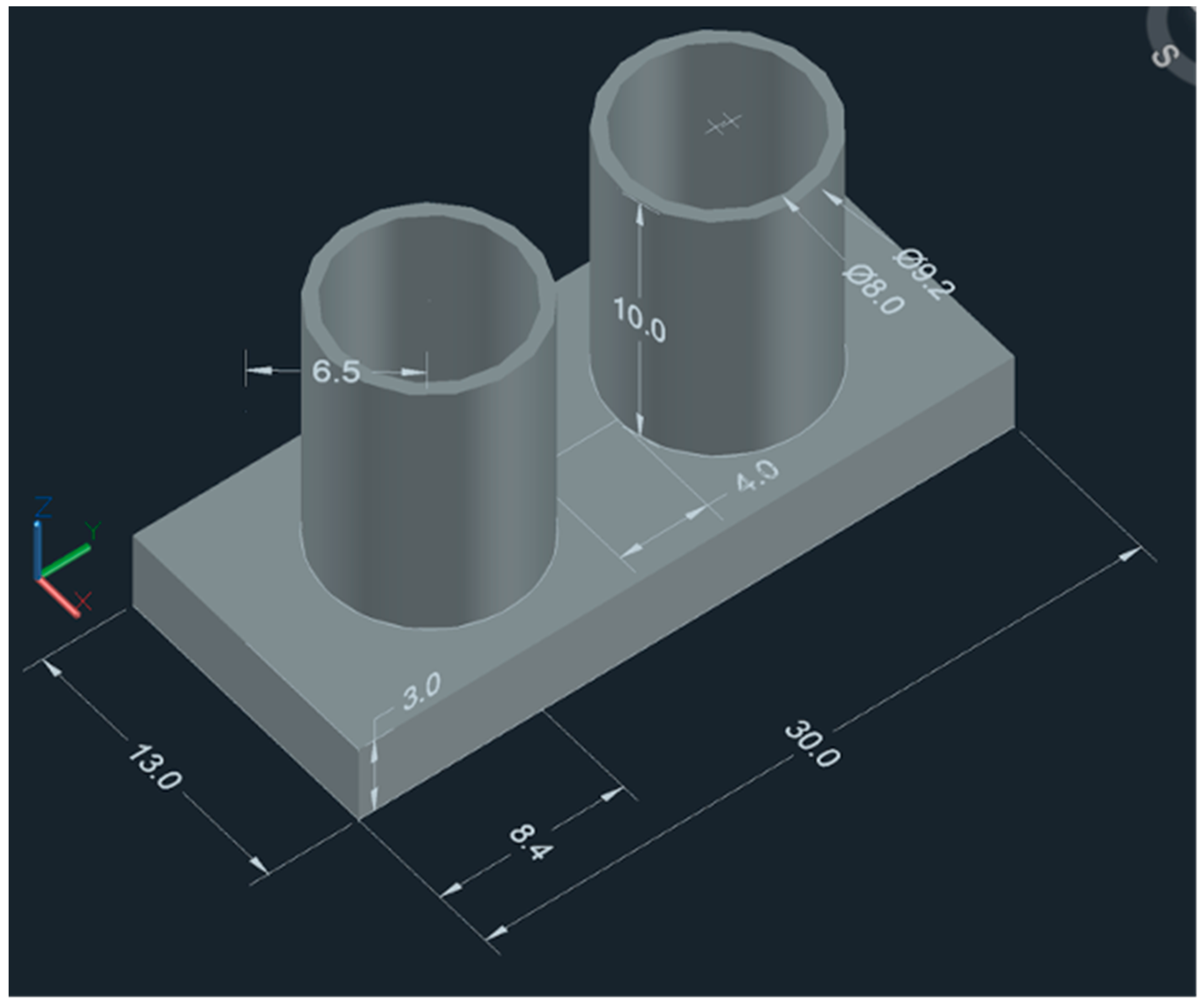
Figure 1.
Scheme of the CAD design (dimensions in mm).
Figure 1.
Scheme of the CAD design (dimensions in mm).
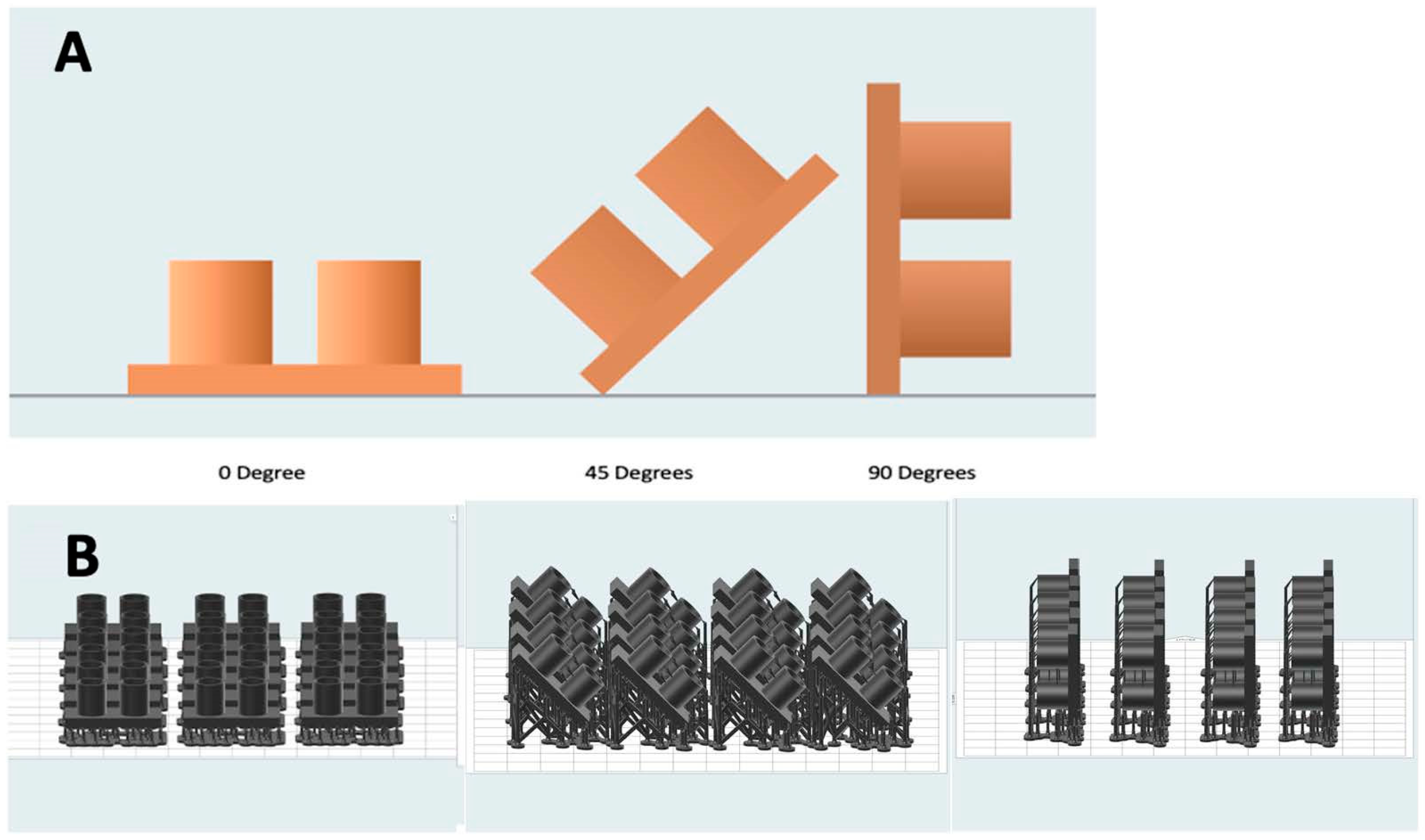
Figure 2.
(A) Printing orientations of the surgical guides selected for this experiment. (B) Surgical guides with their supports respective to the build platform.
Figure 2.
(A) Printing orientations of the surgical guides selected for this experiment. (B) Surgical guides with their supports respective to the build platform.
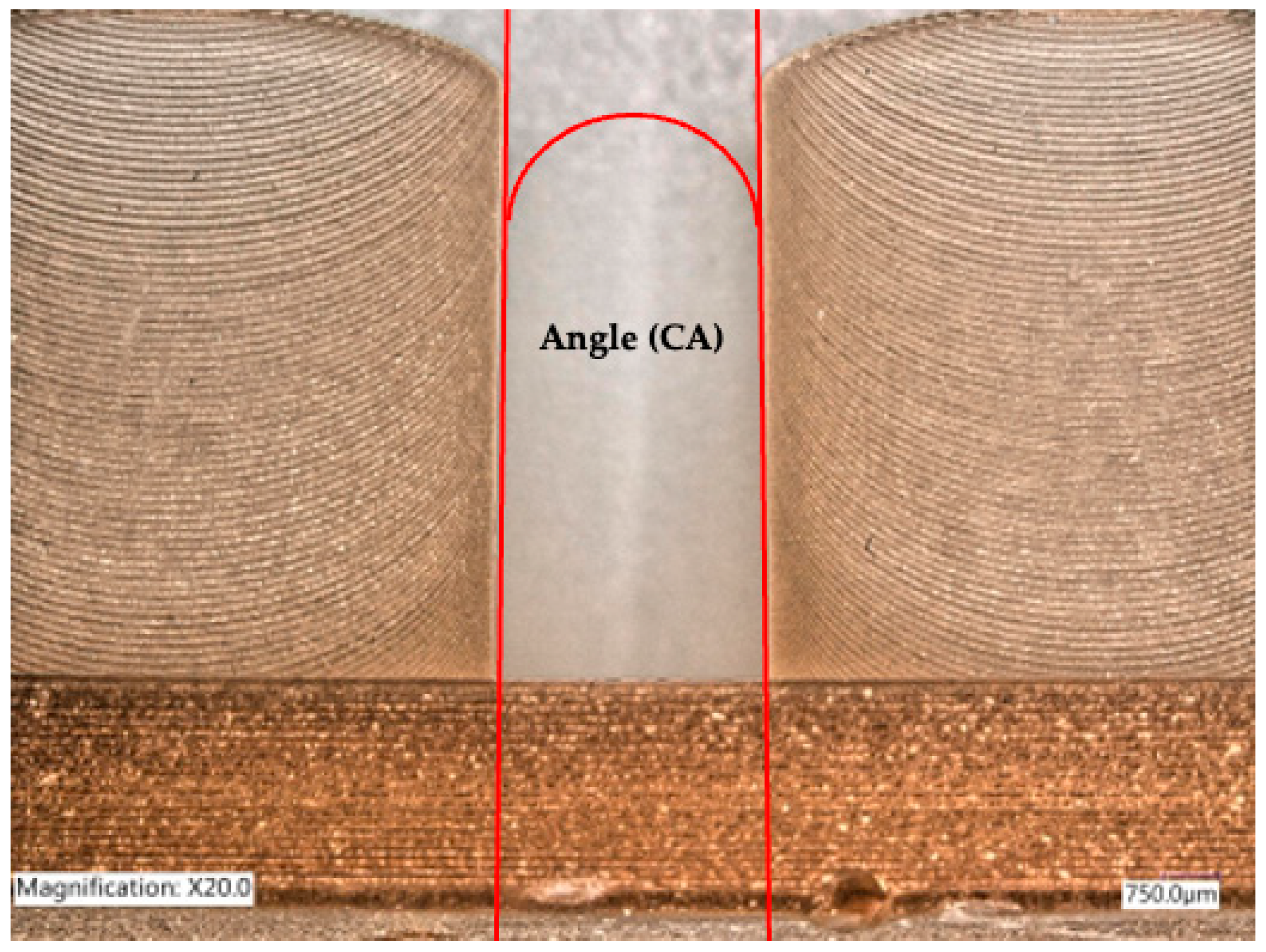
Figure 3.
Angle between adjacent cylinders.
Figure 3.
Angle between adjacent cylinders.
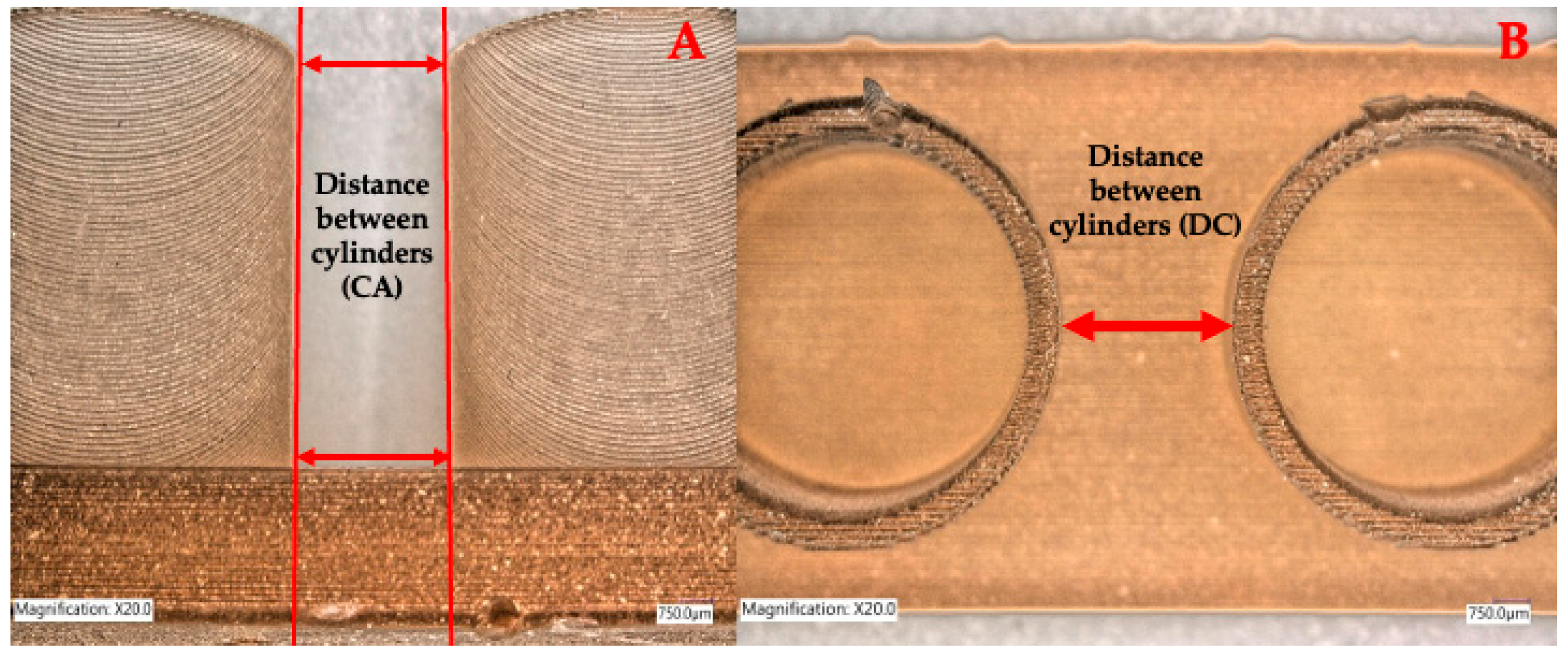
Figure 4.
Distance between cylinders. (A) represents a lateral view of the distance between the cylinders’ walls at the top and at the base. (B) represents a top view at the top of the cylinders.
Figure 4.
Distance between cylinders. (A) represents a lateral view of the distance between the cylinders’ walls at the top and at the base. (B) represents a top view at the top of the cylinders.
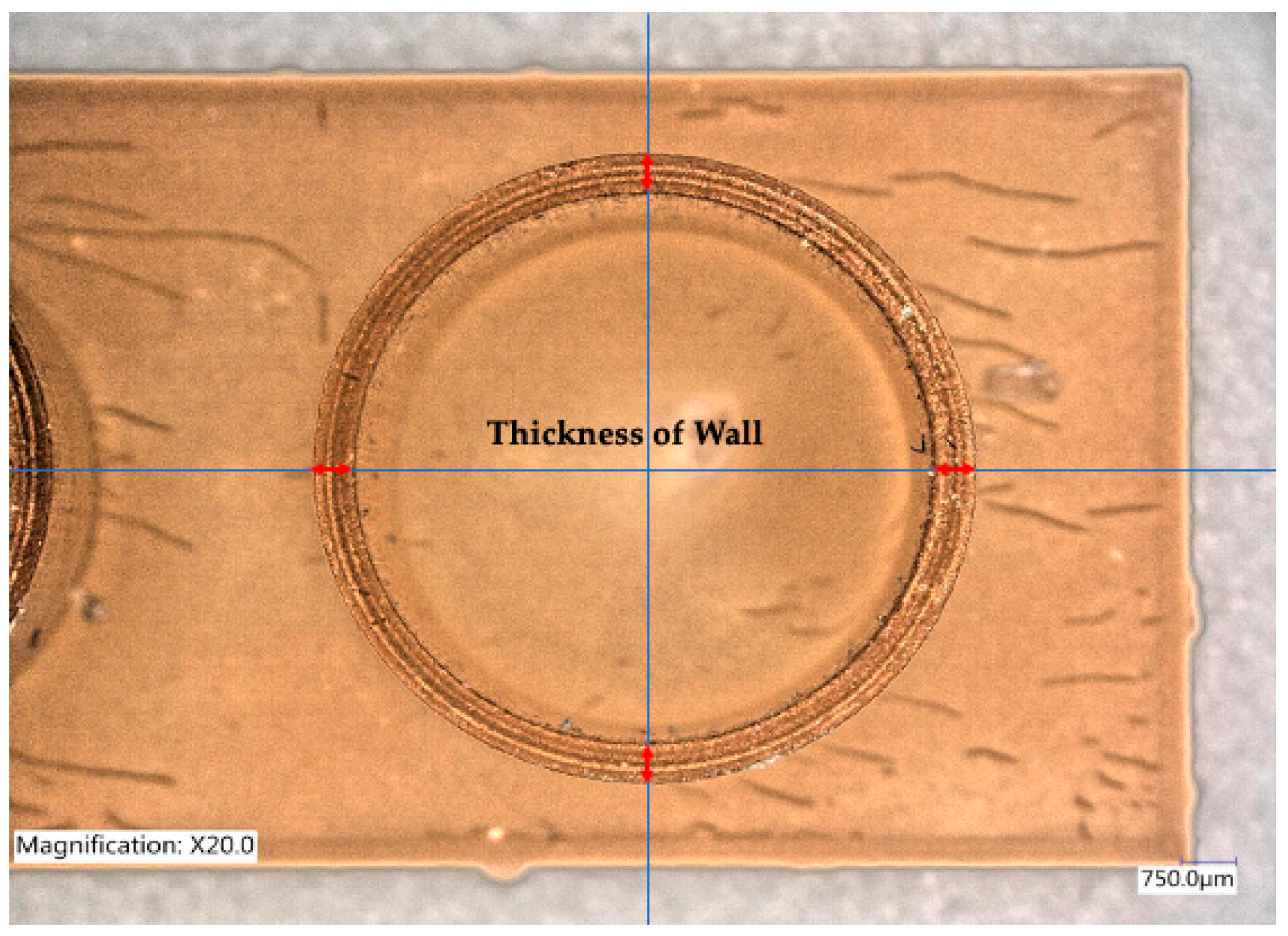
Figure 5.
Thickness of the cylinders’ walls measured at four equidistant points.
Figure 5.
Thickness of the cylinders’ walls measured at four equidistant points.
Figure 6.
Regions identified at the reference model for cloud comparisons with the STL files of the 3D-printed samples.
Figure 6.
Regions identified at the reference model for cloud comparisons with the STL files of the 3D-printed samples.
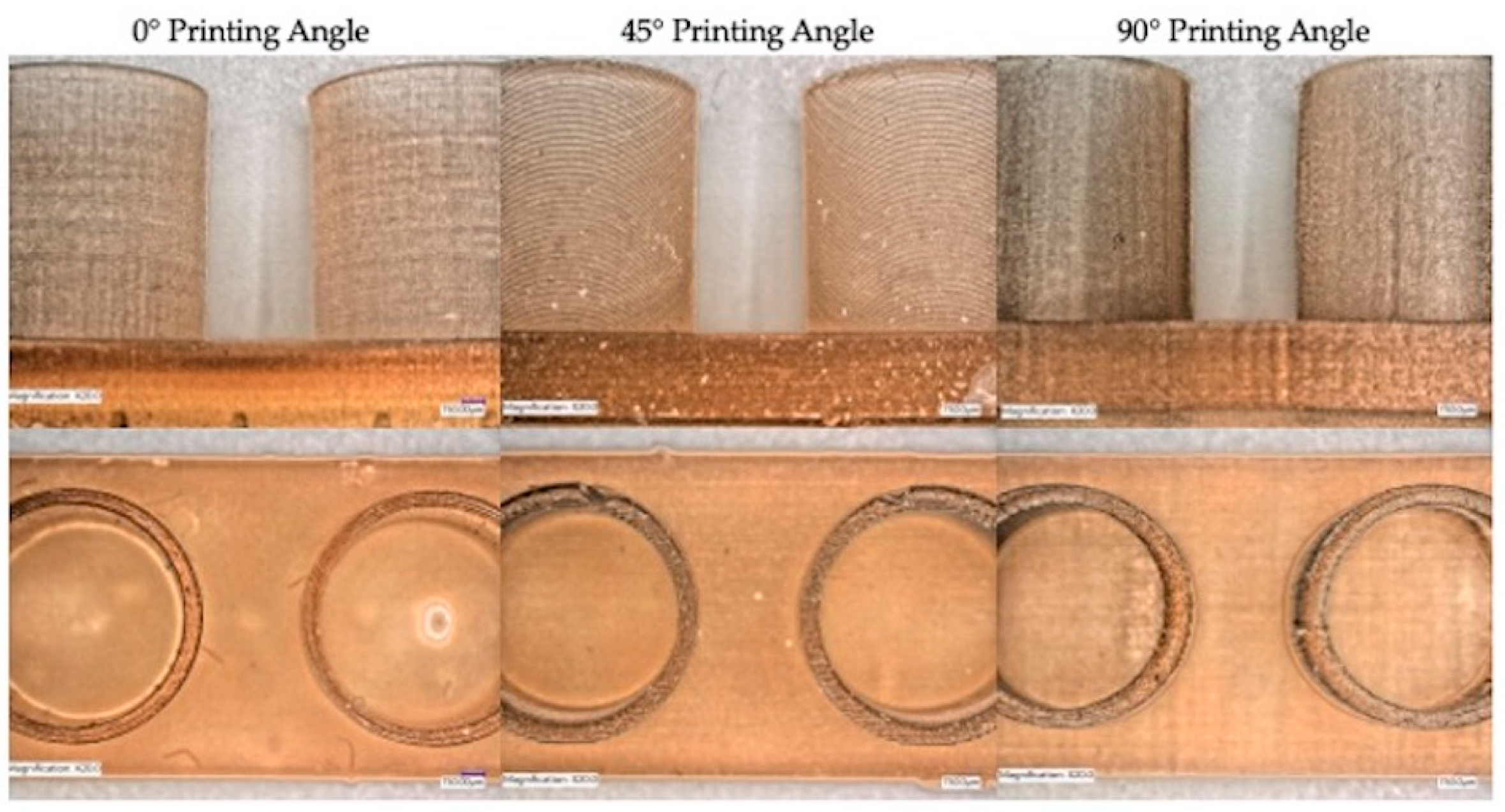
Figure 7.
Representative photos of samples printed with different printing orientations showing discrepancies in distances and angle between cylinders in all the groups.
Figure 7.
Representative photos of samples printed with different printing orientations showing discrepancies in distances and angle between cylinders in all the groups.
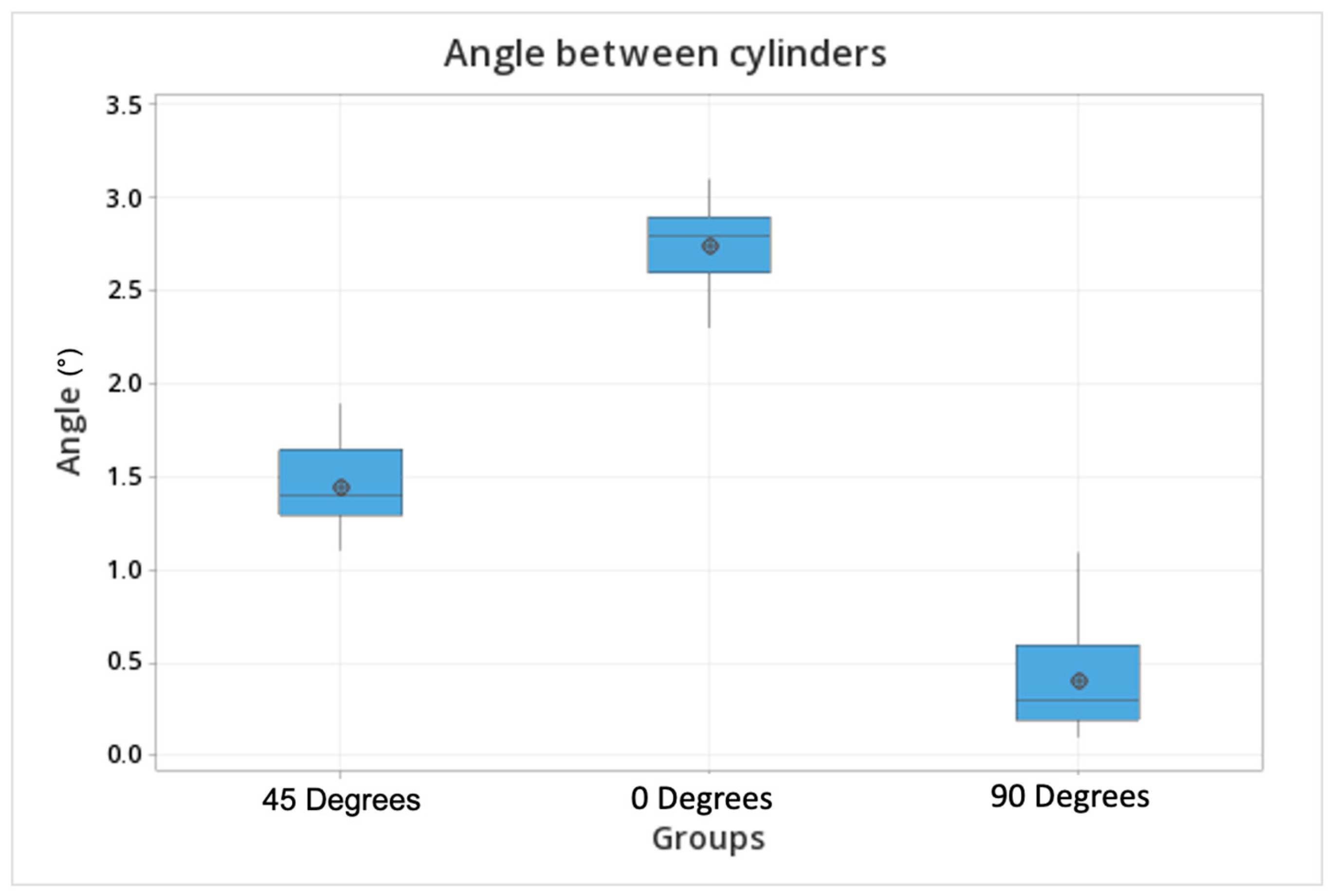
Figure 8.
Box plot comparisons of the angle formed between cylinders printed at different angulations (45, 0, 90 degrees). The dots represent the mean values, the upper and lower lines are the upper and lower values within each group.
Figure 8.
Box plot comparisons of the angle formed between cylinders printed at different angulations (45, 0, 90 degrees). The dots represent the mean values, the upper and lower lines are the upper and lower values within each group.
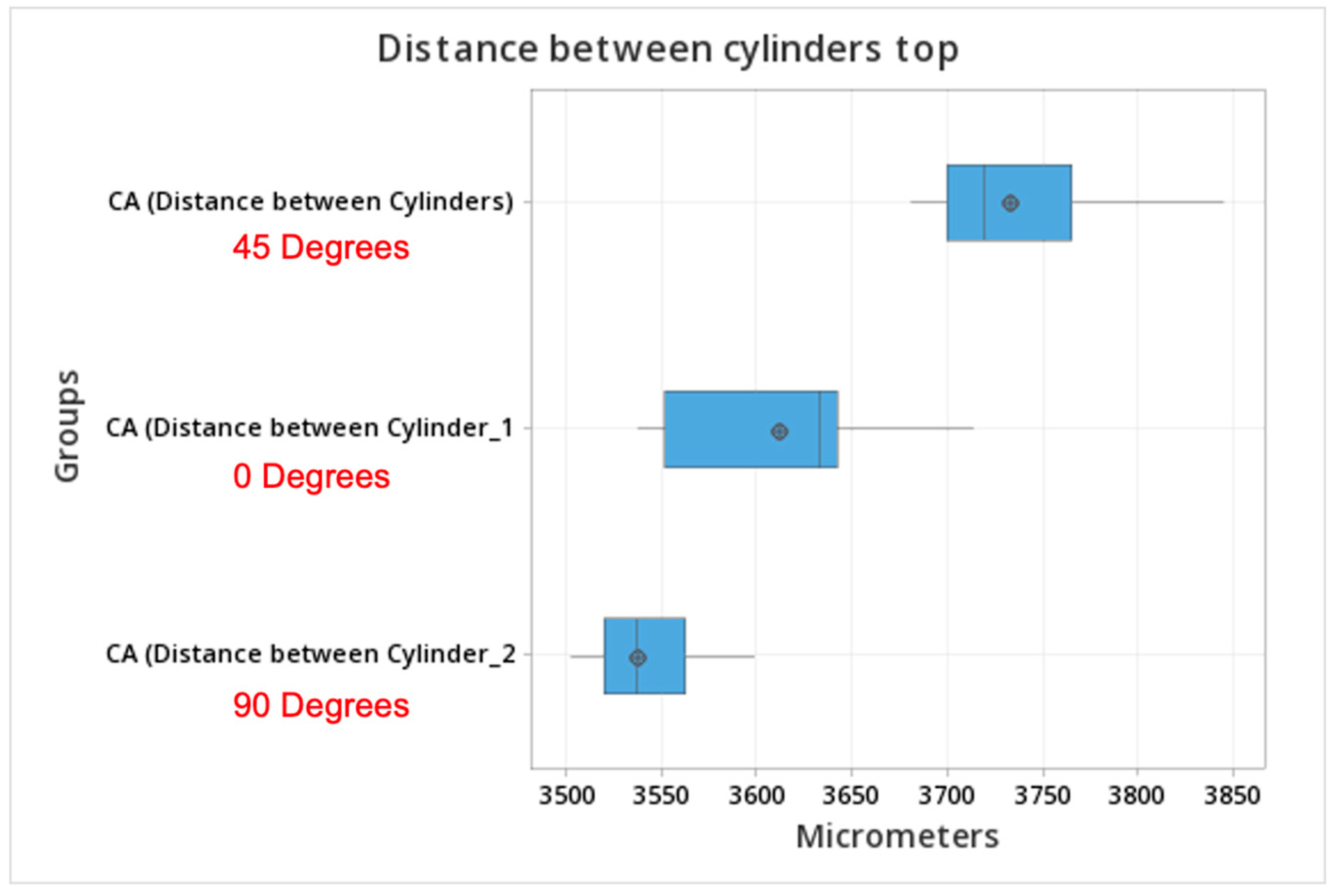
Figure 9.
Box plot of the distance between the top of the cylinders printed with different orientations.
Figure 9.
Box plot of the distance between the top of the cylinders printed with different orientations.
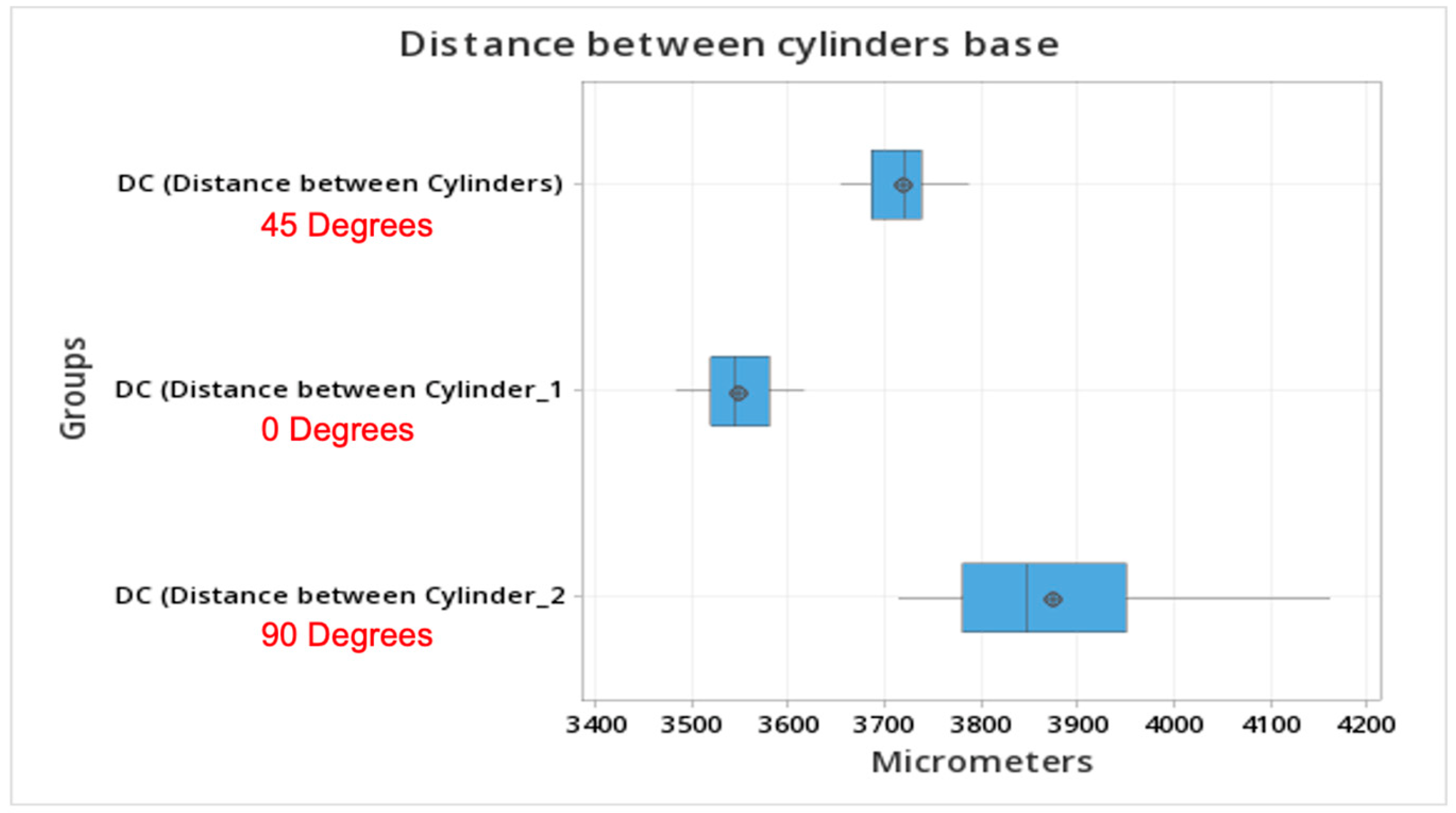
Figure 10.
Distance at the base of cylinders printed with different orientations. Printing at a 90-degree angle resulted in values closer to the reference model. Meanwhile, orientations of 45 or 0 degrees resulted in shorter distances at the cylinders’ bases.
Figure 10.
Distance at the base of cylinders printed with different orientations. Printing at a 90-degree angle resulted in values closer to the reference model. Meanwhile, orientations of 45 or 0 degrees resulted in shorter distances at the cylinders’ bases.
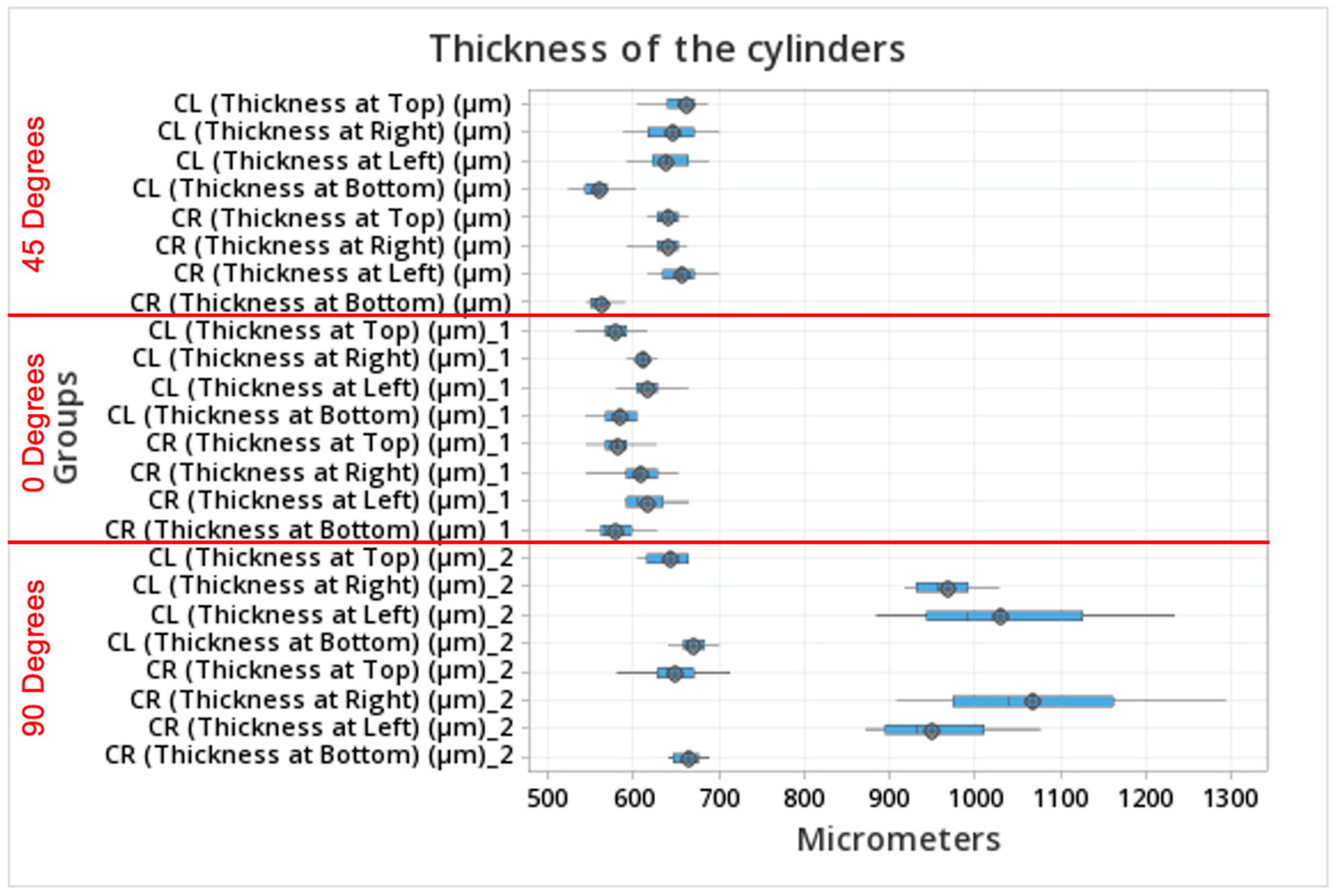
Figure 11.
Box plot comparisons of the thickness of the cylinder walls at different angulations (45, 0, 90 degrees) measured from a coronal view.
Figure 11.
Box plot comparisons of the thickness of the cylinder walls at different angulations (45, 0, 90 degrees) measured from a coronal view.
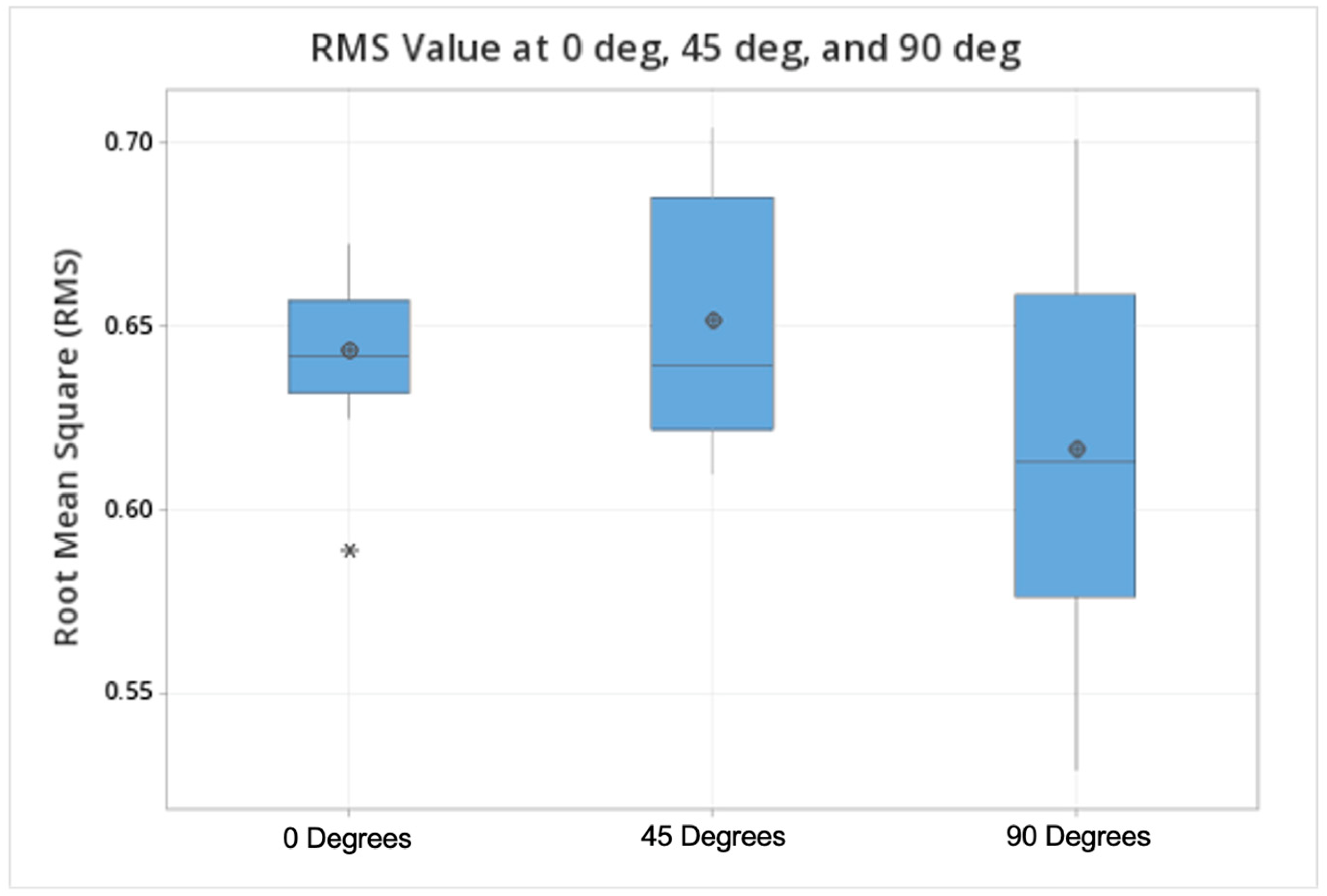
Figure 12.
Box plot comparisons of the RMSE values at all orientations (0, 45, 90 degrees).
Figure 12.
Box plot comparisons of the RMSE values at all orientations (0, 45, 90 degrees).
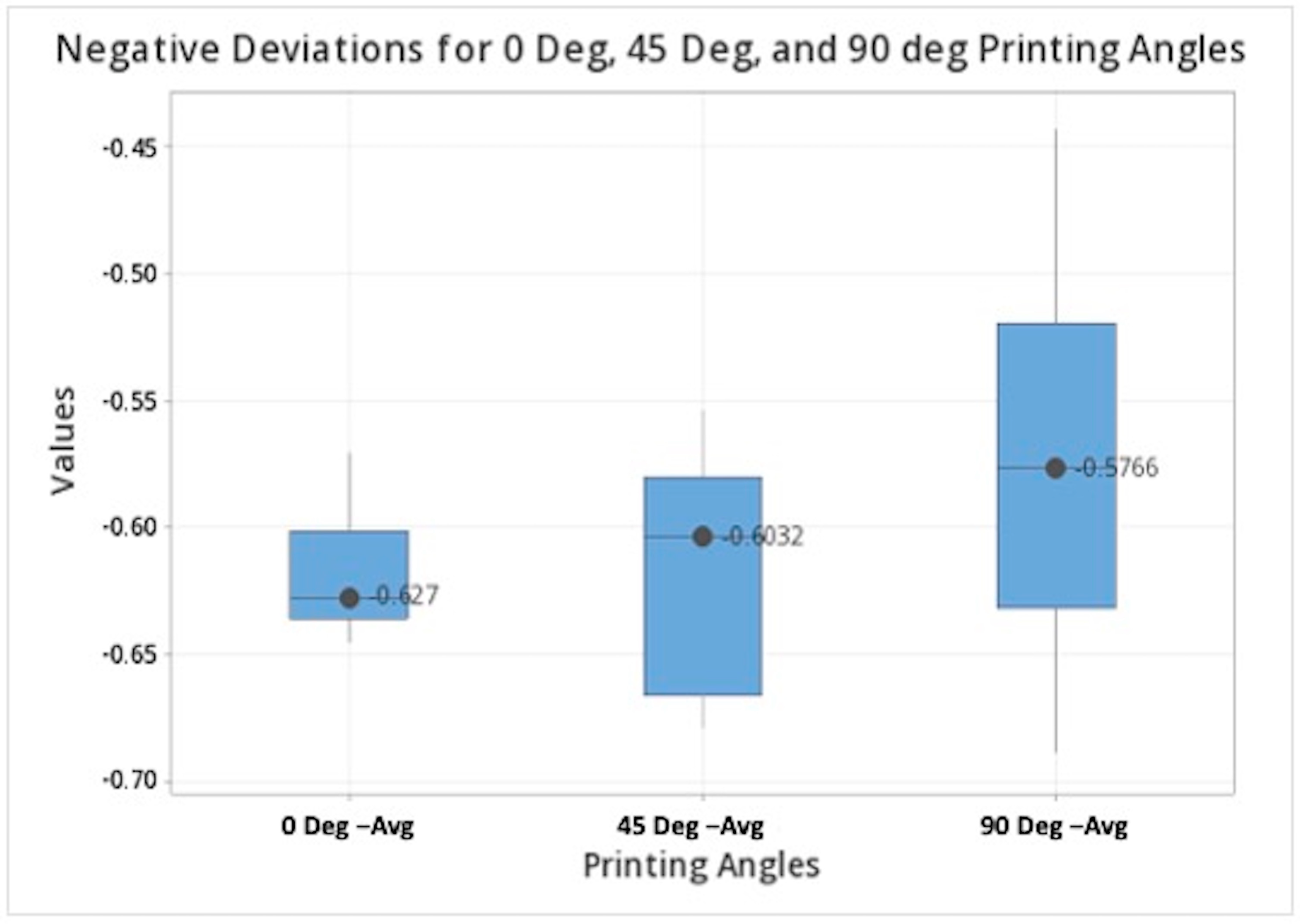
Figure 13.
Box plot comparisons of the negative deviation values at all orientations (0, 45, 90 degrees).
Figure 13.
Box plot comparisons of the negative deviation values at all orientations (0, 45, 90 degrees).
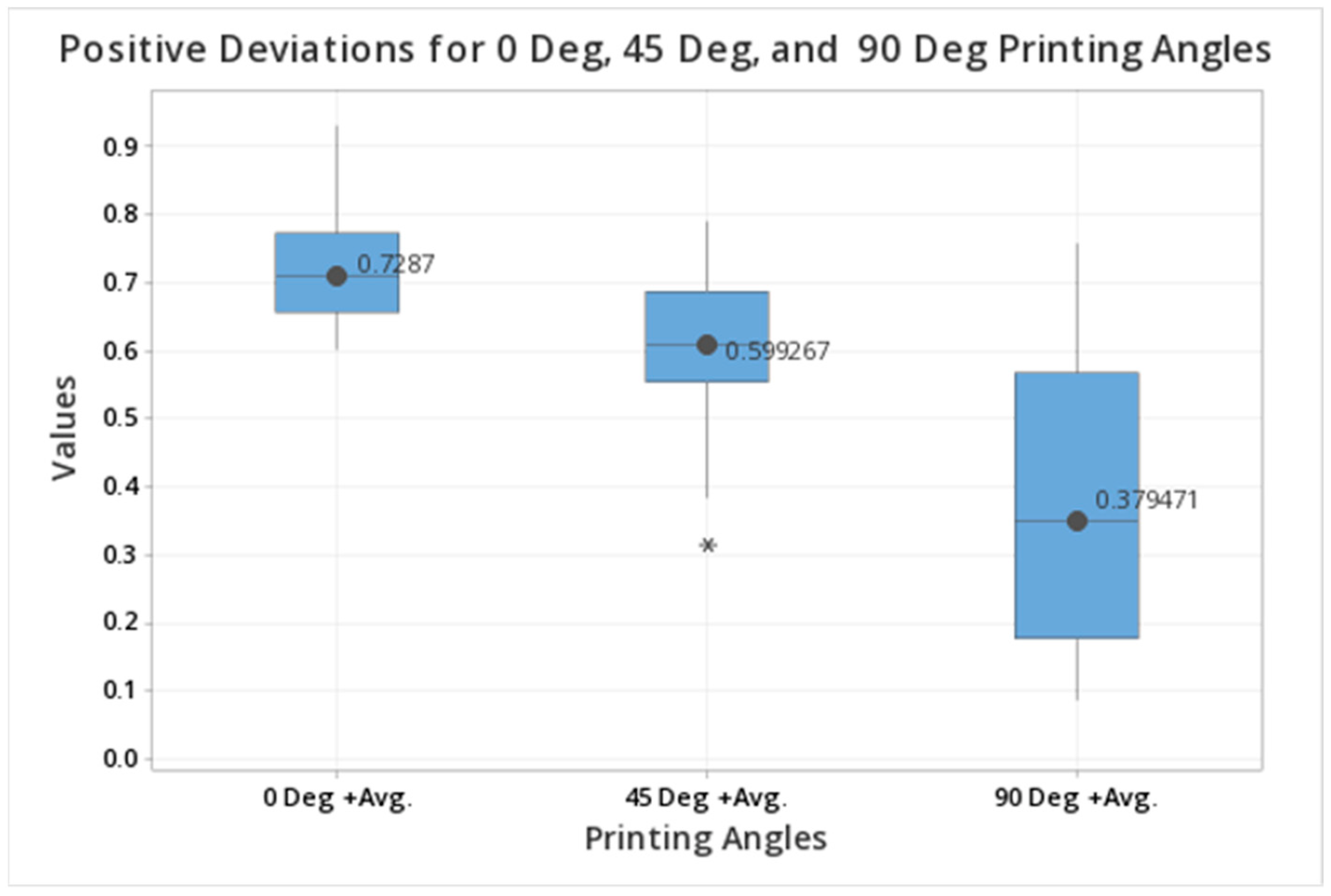
Figure 14.
Box plot comparisons of the positive deviation values at all orientations (0, 45, 90 degrees).
Figure 14.
Box plot comparisons of the positive deviation values at all orientations (0, 45, 90 degrees).
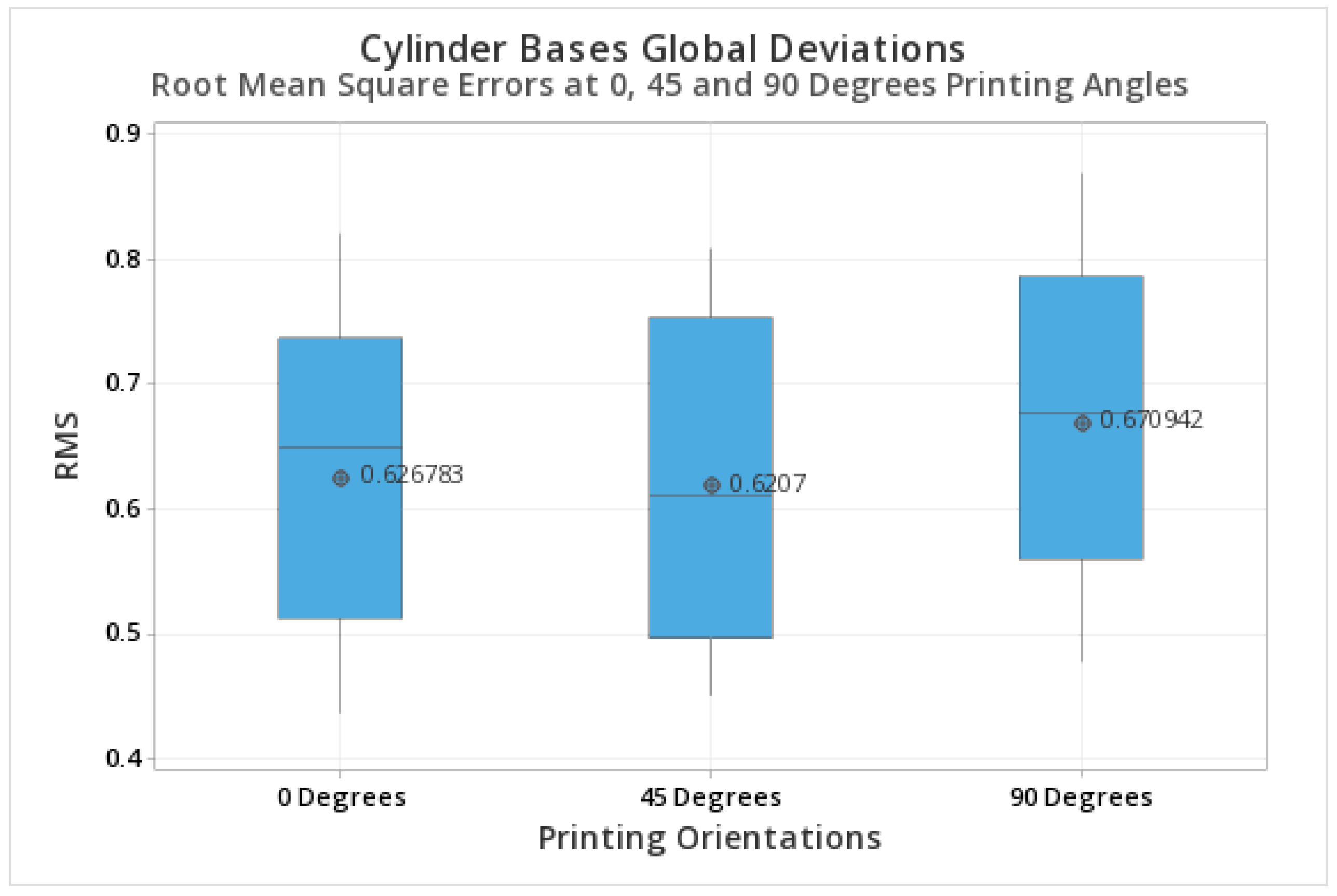
Figure 15.
Box plot comparisons of the RMSE at the base of the cylinders at 0, 45, 90 degrees.
Figure 15.
Box plot comparisons of the RMSE at the base of the cylinders at 0, 45, 90 degrees.
Table 1.
Descriptive statistics of the angle between cylinders printed with different orientations. Values near 0 represent parallel cylinders.
Table 1.
Descriptive statistics of the angle between cylinders printed with different orientations. Values near 0 represent parallel cylinders.
| Angle | N | Mean | SD | 95% CI |
|---|
| CA 45 Degrees | 21 | 1.4571 | 0.2378 | (1.3591, 1.5552) |
| CA 0 Degrees | 21 | 2.7429 | 0.1886 | (2.6448, 2.8409) |
| CA 90 Degrees | 21 | 0.4143 | 0.2435 | (0.3162, 0.5124) |
Table 2.
Statistical comparison of the angle formed between cylinders printed with different orientations. Tukey test.
Table 2.
Statistical comparison of the angle formed between cylinders printed with different orientations. Tukey test.
| Difference of Levels | Difference
of Means | SE of
Difference | 95% CI | T-Value | Adjusted
p-Value |
|---|
| CA (Angle) 0 Degrees–CA (Angle) 45 Degrees | 1.2857 | 0.0693 | (1.1190, 1.4524) | 18.54 | 0.001 |
| CA (Angle) 90 Degrees–CA (Angle) 45 Degrees | −1.0429 | 0.0693 | (−1.2095, −0.876) | −15.04 | 0.001 |
| CA (Angle) 90 Degrees–CA (Angle) 0 Degrees | −2.3286 | 0.0693 | (−2.4953, −2.161) | −33.58 | 0.001 |
Table 3.
Descriptive statistics of the distance between cylinders at the top.
Table 3.
Descriptive statistics of the distance between cylinders at the top.
| Factor | N | Mean | SD | 95% CI |
|---|
| CA DC 45 Degrees | 21 | 3733.05 | 40.82 | (3714.20, 3751.90) |
| CA DC 0 Degrees | 21 | 3611.3 | 49.6 | (3592.5, 3630.2) |
| CA DC 90 Degrees | 21 | 3537.53 | 38.25 | (3518.69, 3556.38) |
Table 4.
Group comparisons of the distances at the top of the cylinders. Tukey test.
Table 4.
Group comparisons of the distances at the top of the cylinders. Tukey test.
| Difference of Levels | Difference
of Means | SE of
Difference | 95% CI | T-Value | Adjusted
p-Value |
|---|
| CA DC 0 Degrees–CA DC 45 Degrees | −121.7 | 13.3 | (−153.8, −89.7) | −9.13 | 0.001 |
| CA DC 90 Degrees–CA DC 45 Degrees | −195.5 | 13.3 | (−227.6, −163.5) | −14.67 | 0.001 |
| CA DC 90 Degrees–CA DC 0 Degrees | −73.8 | 13.3 | (−105.8, −41.8) | −5.54 | 0.001 |
Table 5.
Descriptive statistics of the distance between cylinders at the base.
Table 5.
Descriptive statistics of the distance between cylinders at the base.
| Factor | N | Mean | SD | 95% CI |
|---|
| DC 45 Degrees | 21 | 3718.27 | 36.22 | (3687.33, 3749.21) |
| DC 0 Degrees | 21 | 3548.36 | 39.39 | (3517.42, 3579.30) |
| DC 90 Degrees | 21 | 3873.2 | 110.5 | (3842.3, 3904.2) |
Table 6.
Group comparisons of the distance between cylinders at the base. Tukey test.
Table 6.
Group comparisons of the distance between cylinders at the base. Tukey test.
| Difference of Levels | Difference
of Means | SE of
Difference | 95% CI | T-Value | Adjusted
p-Value |
|---|
| CA DC 0 Degrees–CA DC 45 Degrees | −121.7 | 13.3 | (−153.8, −89.7) | −9.13 | 0.001 |
| CA DC 90 Degrees–CA DC 45 Degrees | −195.5 | 13.3 | (−227.6, −163.5) | −14.67 | 0.001 |
| CA DC 90 Degrees–CA DC 0 Degrees | −73.8 | 13.3 | (−105.8, −41.8) | −5.54 | 0.001 |
Table 7.
Descriptive statistics of the RMSE values at all orientations (0, 45, 90 degrees).
Table 7.
Descriptive statistics of the RMSE values at all orientations (0, 45, 90 degrees).
| Sample | N | Mean | SD | SE Mean |
|---|
| 0 Degrees | 21 | 0.64334 | 0.01873 | 0.00409 |
| 45 Degrees | 21 | 0.65199 | 0.03332 | 0.00727 |
| 90 Degrees | 21 | 0.6168 | 0.0511 | 0.0112 |
Table 8.
T-Value and p-Value comparisons of RMSE at all orientations.
Table 8.
T-Value and p-Value comparisons of RMSE at all orientations.
| Samples | T-Value | p-Value |
|---|
| 0 Degrees vs. 45 Degrees | −0.88 | 0.392 |
| 0 Degrees vs. 90 Degrees | 2.67 | 0.015 |
| 45 Degrees vs. 90 Degrees | 2.48 | 0.022 |
Table 9.
Descriptive statistics of the negative deviation values at all orientations (0, 45, 90 degrees).
Table 9.
Descriptive statistics of the negative deviation values at all orientations (0, 45, 90 degrees).
| Variable | N | Mean | SE Mean | StDev | Minimum | Q1 | Median | Q3 | Maximum |
|---|
| 0 Degrees–Avg. | 21 | −0.61731 | 0.00475 | 0.02179 | −0.64520 | −0.63535 | −0.62700 | −0.60090 | −0.57010 |
| 45 Degrees–Avg. | 21 | −0.61815 | 0.00964 | 0.04417 | −0.67830 | −0.66545 | −0.60320 | −0.57950 | −0.55360 |
| 90 Degrees–Avg. | 21 | −0.5747 | 0.0145 | 0.0665 | −0.6885 | −0.6315 | −0.5766 | −0.5191 | −0.4427 |
Table 10.
T-Value and p-Value comparisons of the negative deviation values at all orientations.
Table 10.
T-Value and p-Value comparisons of the negative deviation values at all orientations.
| Samples | T-Value | p-Value |
|---|
| 0 Degrees vs. 45 Degrees | 0.07 | 0.947 |
| 0 Degrees vs. 90 Degrees | −3.05 | 0.006 |
| 45 Degrees vs. 90 Degrees | −2.26 | 0.035 |
Table 11.
Descriptive statistics of the positive deviation values at all orientations (0, 45, 90 degrees).
Table 11.
Descriptive statistics of the positive deviation values at all orientations (0, 45, 90 degrees).
| Variable | N | Mean | SE Mean | StDev | Minimum | Q1 | Median | Q3 | Maximum |
|---|
| 0 Degrees+ Avg. | 21 | 0.7287 | 0.0193 | 0.0885 | 0.6026 | 0.6573 | 0.7095 | 0.7737 | 0.9329 |
| 45 Degrees+ Avg. | 21 | 0.5993 | 0.0248 | 0.1135 | 0.3171 | 0.5551 | 0.6086 | 0.6877 | 0.7900 |
| 90 Degrees+ Avg. | 21 | 0.3795 | 0.0475 | 0.2176 | 0.0873 | 0.1788 | 0.3495 | 0.5685 | 0.7585 |
Table 12.
T-Value and p-Value comparisons of the positive deviation values at all orientations.
Table 12.
T-Value and p-Value comparisons of the positive deviation values at all orientations.
| Samples | T-Value | p-Value |
|---|
| 0 Degrees vs. 45 Degrees | 4.17 | 0.001 |
| 0 Degrees vs. 90 Degrees | 6.53 | 0.001 |
| 45 Degrees vs. 90 Degrees | 5.12 | 0.001 |
Table 13.
Descriptive statistics of the RMSE values at all orientations at the bases (0, 45, 90 degrees).
Table 13.
Descriptive statistics of the RMSE values at all orientations at the bases (0, 45, 90 degrees).
| Factor | N | Mean | StDev | 95% CI |
|---|
| 0 Degrees | 21 | 0.6079 | 0.1278 | (0.5417, 0.6742) |
| 45 Degrees | 21 | 0.6090 | 0.1203 | (0.5428, 0.6753) |
| 90 Degrees | 21 | 0.6475 | 0.1194 | (0.5812, 0.7137) |
Table 14.
ANOVA analysis for the RMSE at the base of the cylinders.
Table 14.
ANOVA analysis for the RMSE at the base of the cylinders.
| Analysis of Variance |
|---|
| Source | DF | Adj SS | Adj MS | F-Value | p-Value |
|---|
| Factor | 2 | 0.01419 | 0.007097 | 0.47 | 0.627 |
| Error | 39 | 0.58552 | 0.015013 | | |
| Total | 41 | 0.59972 | | | |
Table 15.
Tukey comparisons for the RMSE at the base of the cylinders for all the printing orientations.
Table 15.
Tukey comparisons for the RMSE at the base of the cylinders for all the printing orientations.
| Factor | N | p-Value |
|---|
| 90 Degrees | 21 | 0.6475 |
| 45 Degrees | 21 | 0.6090 |
| 0 Degrees | 21 | 0.6079 |



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}