
The Success Rate of the Adhesive Partial Fixed Prosthesis after Five Years: A Systematic Review


 and
and
Abstract
:1. Introduction
2. Materials and Methods
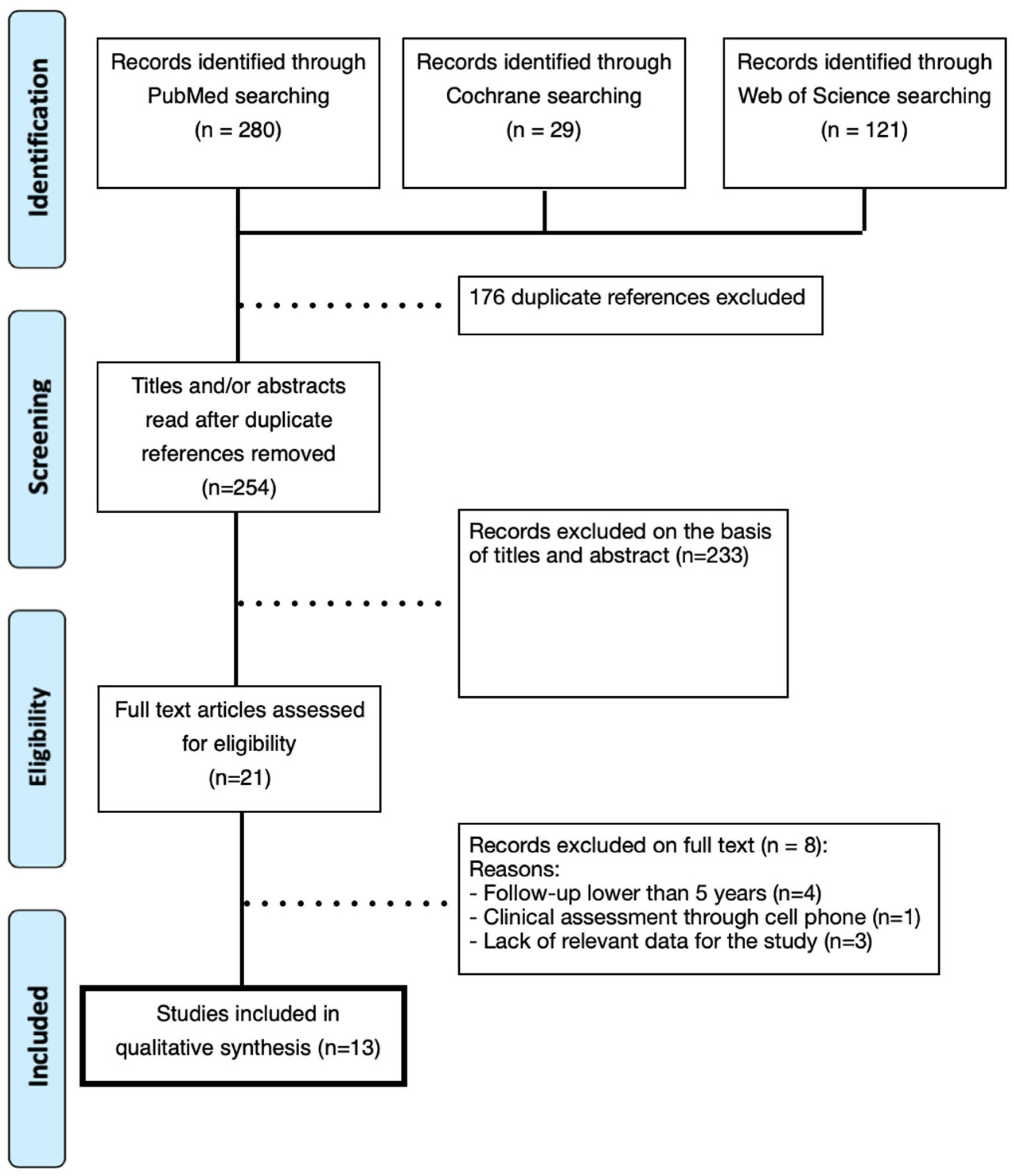
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Quality Assessment/Risk of Bias
2.5. Statistical Analysis
3. Results
3.1. Biological and Mechanical Complications
3.2. Success/Survival Rate and Risk of Bias/Quality Assessment
3.3. Statistical Analysis
4. Discussion
4.1. Success/Survival or Retention Rates
4.2. Failure rate and RBFPD Design
4.3. Tooth/Teeth Preparation
4.4. Retention and Retainers
4.5. Limitations and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ferro, K.J.; Morgano, S.M.; Driscoll, C.F.; Freilich, M.A.; Guckes, A.D.; Knoernschild, K.L.; McGarry, T.J. The Glossary of Prosthodontic Terms: Ninth Edition. J. Prosthet. Dent. 2017, 117, e1-105. [Google Scholar]
- Pjetursson, B.E.; Tan, W.C.; Tan, K.; Brägger, U.; Zwahlen, M.; Lang, N.P. A systematic review of the survival and complication rates of resin-bonded bridges after an observation period of at least 5 years. Clin. Oral Implant. Res. 2008, 19, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Rochette, A.L. Attachment of a splint to enamel of lower anterior teeth. J. Prosthet. Dent. 1973, 30, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Williams, V.D.; Drennon, D.G.; Silverstone, L.M. The effect of retainer design on the retention of filled resin in acid-etched fixed partial dentures. J. Prosthet. Dent. 1982, 48, 417. [Google Scholar] [CrossRef] [PubMed]
- Livaditis, G.J.; Thompson, V.P. Etched castings: An improved retentive mechanism for resin-bonded retainers. J. Prosthet. Dent. 1982, 47, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Thompson, V.P.; Del Castillo, E.; Livaditis, G.J. Resin-bonded retainers. Part I: Resin bond to electrolytically etched nonprecious alloys. J. Prosthet. Dent. 1983, 50, 771–779. [Google Scholar] [CrossRef]
- Thompson, V.P.; Livaditis, G.J. Etched casting acid etch composite bonded posterior bridges. Pediatr. Dent. 1982, 4, 38–43. [Google Scholar]
- Shimizu, H.; Kawaguchi, T.; Takahashi, Y. The current status of the design of resin-bonded fixed partial dentures, splints and overcastings. Jpn. Dent. Sci. Rev. 2014, 50, 23–28. [Google Scholar] [CrossRef] [Green Version]
- van Heumen, C.C.; Kreulen, C.M.; Creugers, N.H. Clinical studies of fiber-reinforced resin-bonded fixed partial dentures: A systematic review. Eur. J. Oral Sci. 2009, 117, 1–6. [Google Scholar] [CrossRef]
- Meijndert, L.; Raghoebar, G.M.; Meijer, H.J.A.; Vissink, A. Clinical and radiographic characteristics of single-tooth replacements preceded by local ridge augmentation: A prospective randomized clinical trial. Clin. Oral Implant. Res. 2008, 19, 1295–1303. [Google Scholar] [CrossRef]
- Creugers, N.H.; De Kanter, R.J.; Verzijden, C.W.; Van’t Hof, M.A. Risk factors and multiple failures in posterior resin-bonded bridges in a 5-year multi-practice clinical trial. J. Dent. 1998, 26, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Behr, M.; Leibrock, A.; Stich, W.; Rammelsberg, P.; Rosentritt, M.; Handel, G. Adhesive-fixed partial dentures in anterior and posterior areas. Results of an on-going prospective study begun in 1985. Clin. Oral Investig. 1998, 2, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Livaditis, G.J. Cast metal resin-bonded retainers for posterior teeth. J. Am. Dent. Assoc. 1980, 101, 926–929. [Google Scholar] [CrossRef]
- Rosenstiel, S.F.; Land, M.F.; Fujimoto, J. Section 1 Planning and Preparation. In Contemporary Fixed Prosthodontics; Mosby, Inc.: St. Louis, MO, USA, 2002; pp. 65–74. [Google Scholar]
- Lin, C.-L.; Hsu, K.-W.; Wu, C.-H. Multi-factorial Retainer Design Analysis of Posterior Resin-Bonded Fixed Partial Dentures: A Finite Element Study. J. Dent. 2005, 33, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Tanoue, N. Longevity of Resin-Bonded Fixed Partial Dental Prostheses Made with Metal Alloys. Clin. Oral Investig. 2016, 20, 1329–1336. [Google Scholar] [CrossRef] [Green Version]
- Acharya, P.H.; Patel, V.V.; Duseja, S.S.; Chauhan, V.R. Comparative Evaluation of Peri-Implant Stress Distribution in Implant Protected Occlusion and Cuspally Loaded Occlusion on a 3 Unit Implant Supported Fixed Partial Denture: A 3D Finite Element Analysis Study. J. Adv. Prosthodont. 2021, 13, 79–88. [Google Scholar] [CrossRef]
- Alraheam, I.A.; Ngoc, C.N.; Wiesen, C.A.; Donovan, T.E. Five-year success rate of resin-bonded fixed partial dentures: A systematic review. J. Esthet. Restor. Dent. 2019, 31, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Kravitz, N.D. The Maryland bridge retainer: A modification of a Maryland bridge. Am. J. Orthod. Dentofacial. Orthop. 2020, 157, 128–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Donato, H.; Donato, M. Stages for undertaking a systematic review. Acta Med. Port. 2019, 32, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Hooper, P.; Jutai, J.W.; Strong, G.; Russell-Minda, E. Age-related macular degeneration and low-vision rehabilitation: A systematic review. Can. J. Ophthalmol. 2008, 43, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Aggstaller, H.; Beuer, F.; Edelhoff, D.; Rammelsberg, P.; Gernet, W. Long-term clinical performance of resin-bonded fixed partial dentures with retentive preparation geometry in anterior and posterior areas. J. Adhes. Dent. 2008, 10, 301–306. [Google Scholar] [PubMed]
- Botelho, M.G.; Ma, X.M.; Cheung, G.J.K.; Law, R.K.S.; Tai, M.T.C.; Lam, W.Y.H. Long-term clinical evaluation of 211 two-unit cantilevered resin-bonded fixed partial dentures. J. Dent. 2014, 42, 778–784. [Google Scholar] [CrossRef]
- Garnett, M.J.; Wassell, R.W.; Jepson, N.J.; Nohl, F.S. Survival of resin-bonded bridgework provided for post-orthodontic hypodontia patients with missing maxillary lateral incisors. Br. Dent. J. 2006, 201, 527–534. [Google Scholar] [CrossRef]
- Kern, M. Clinical long-term survival of two-retainer and single-retainer all-ceramic resin-bonded fixed partial dentures. Quintessence Int. 2005, 36, 141–147. [Google Scholar]
- Kern, M. Fifteen-year survival of anterior all-ceramic cantilever resin-bonded fixed dental prostheses. J. Dent. 2017, 56, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Kern, M.; Passia, N.; Sasse, M.; Yazigi, C. Ten-year outcome of zirconia ceramic cantilever resin-bonded fixed dental prostheses and the influence of the reasons for missing incisors. J. Dent. 2017, 65, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Bonani, T.; Brodbeck, U.; Hämmerle, C.H.F. Retrospective clinical study of single-retainer cantilever anterior and posterior glass-ceramic resin-bonded fixed dental prostheses at a mean follow-up of 6 years. Int. J. Prosthodont. 2013, 26, 443–450. [Google Scholar] [CrossRef] [Green Version]
- Sasse, M.; Kern, M. CAD/CAM single retainer zirconia-ceramic resin-bonded fixed dental prostheses: Clinical outcome after 5 years. Int. J. Comput. Dent. 2013, 16, 109–118. [Google Scholar]
- Sasse, M.; Kern, M. Survival of anterior cantilevered all-ceramic resin-bonded fixed dental prostheses made from zirconia ceramic. J. Dent. 2014, 42, 660–663. [Google Scholar] [CrossRef] [PubMed]
- Younes, F.; Raes, F.; Van Berghe, L.; De Bruyn, H. A retrospective cohort study of metal-cast resin-bonded fixed dental prostheses after at least 16 years. Eur. J. Oral Implantol. 2013, 6, 61–70. [Google Scholar]
- Miettinen, M.; Millar, B.J. A review of the success and failure characteristics of resin-bonded bridges. Br. Dent. J. 2013, 215, E3. [Google Scholar] [CrossRef] [Green Version]
- Sailer, I.; Hämmerle, C.H. Zirconia ceramic single-retainer resin-bonded fixed dental prostheses (RBFDPs) after 4 years of clinical service: A retrospective clinical and volumetric study. Int. J. Periodontics Restorative Dent. 2014, 34, 333–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galiatsatos, A.A.; Bergou, D. Clinical evaluation of anterior all-ceramic resin-bonded fixed dental prostheses. Quintessence Int. 2014, 45, 9–14. [Google Scholar] [PubMed]
- El Mesbahi, N.; Hamza, M.; Bennani, A. Resin-bonded fixed partial dentures with metal framework a report of 49 cases followed for 2 years. Int. J. Info. Res. Rev. 2018, 5, 5782–5786. [Google Scholar]
- Rosentritt, M.; Ries, S.; Kolbeck, C.; Westphal, M.; Richter, E.-J.; Handel, G. Fracture characteristics of anterior resin-bonded zirconia-fixed partial dentures. Clin. Oral Investig. 2009, 13, 453–457. [Google Scholar] [CrossRef]
- Botelho, M.G.; Chan, A.W.; Leung, N.C.; Lam, W.Y.H. Long-term evaluation of cantilevered versus fixed-fixed resin-bonded fixed partial dentures for missing maxillary incisors. J. Dent. 2016, 45, 59–66. [Google Scholar] [CrossRef] [Green Version]
- van Heumen, C.C.; van Dijken, J.W.; Tanner, J.; Pikaar, R.; Lassila, L.V.; Creugers, N.H.; Vallittu, P.K.; Kreulen, C.M. Five-year survival of 3-unit fiber-reinforced composite fixed partial dentures in the anterior area. Dent. Mater. 2009, 25, 820–827. [Google Scholar] [CrossRef]
- Thoma, D.S.; Sailer, I.; Ioannidis, A.; Zwahlen, M.; Makarov, N.; Pjetursson, B.E. A systematic review of the survival and complication rates of resin-bonded fixed dental prostheses after a mean observation period of at least 5 years. Clin. Oral Implant. Res. 2017, 28, 1421–1432. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Brägger, U.; Lang, N.P.; Zwahlen, M. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin. Oral Implant. Res. 2007, 18, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Fanmgthh, C., Jr. Periodontia Clínica, 9th ed.; Guanabara Koogan: Rio de Janeiro, Brazil, 2004. [Google Scholar]
- Proffit, W.F. Tratamento Combinado Ortodôntico e Cirúrgico. In Ortodontia Contemporânea; Profitt, W.R., Fields, J.R., Eds.; Guanabara-Koogan: Rio de Janeiro, Brazil, 1995; pp. 555–590. [Google Scholar]
- Kern, M.; Sasse, M. Ten-year survival of anterior all-ceramic resin-bonded fixed dental prostheses. J. Adhes. Dent. 2011, 13, 407–410. [Google Scholar] [PubMed]
- Wei, Y.R.; Wang, X.D.; Zhang, Q.; Li, X.X.; Blatz, M.B.; Jian, Y.T.; Zhao, K. Clinical performance of anterior resin-bonded fixed dental prostheses with different framework designs: A systematic review and meta-analysis. J. Dent. 2016, 47, 1–7. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Özcan, M.; Scherrer, S.S.; Bühler, J.M.; Weiger, R.; Krastl, G. Resin-bonded restorations: A strategy for managing anterior tooth loss in adolescence. J. Prosthet. Dent. 2015, 113, 270–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Author/Year | Adhesive Partial Fixed Prostheses (n) | Bridges (n) | Retainers (n) | Preparation of Abutment Teeth | Material of the Framework | Cement | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total | Max | Mand | Ant | Post | ||||||
| Aggstaller et al., 2008 [24] | 84 | NR | NR | NR | NR | <3 | <3 | Yes | Metal-Ceramic | Resin cement (Microfill pontic™ or Variolink™) |
| Behr et al., 1998 [12] | 120 | 38 | 19 | 40 | 17 | 1 | 2 | Preparation with retention and without retention | Metal-Ceramic | Resin cement (Microfill-pontic™ and Variolink™) |
| Botelho et al., 2014 [25] | 211 | 136 | 75 | 111 | 100 | 1 | 1 | Yes | Metal-Ceramic | Resin cement (Panavia EX™ or Panavia 21™) |
| Garnett et al., 2006 [26] | 73 | NR | NR | NR | NR | 1 | <2 | Yes/No | Metal-Ceramic | Resin cement (Panavia EX™ or Panavia 21™) |
| Kern, 2005 [27] | 37 | 24 | 13 | 37 | 0 | 1 | 2 | Yes | Alumina-Ceramic | Resin cement (Panavia TC™ (Kuraray®)) |
| Kern, 2017 [28] | 22 | 16 | 6 | 22 | 0 | 1 | 1 | Yes | Zirconia-Ceramic | Resin cement (Panavia 21™) |
| Kern et al., 2017 [29] | 108 | 82 | 33 | 115 | 0 | 1 | 1 | Yes | Zirconia-Ceramic | Resin cement (Panavia 21™ and Multilink Automix™) |
| Sailer et al., 2013 [30] | 14 | 8 | 6 | 9 | 5 | 1 | 1 | Yes | Lithium disilicate | Resin cement (Tetric Flow™, Tetric Ceram™, Rely-X™, Panavia F™, HFO™, and Variolink™) |
| Sasse and Kern, 2013 [31] | 30 | 19 | 11 | 30 | 0 | 1 | 1 | Yes | Zirconia-Ceramic | Resin cement (Panavia 21™ and Multilink Automix™) |
| Sasse and Kern, 2014 [32] | 42 | 26 | 16 | 42 | 0 | 1 | 1 | Yes | Zirconia-Ceramic | Resin cement (Panavia™) |
| Younes et al., 2013 [33] | 42 | 29 | 13 | 24 | 18 | 1 | 2 | Yes | Metal-Ceramic | Resin cement (Panavia™ or Panavia EX™) |
| Author/Year | Follow-Up Median (Years) | Biological/Mechanical Complications (n) | Estimated Failure Rate (%/Year) | Total Exposure Time of RBFPDS (Years) | Estimated Success Rate ≥5 Years (T MAX) | Estimated Survival Rate ≥5 Years (T MAX) |
|---|---|---|---|---|---|---|
| Aggstaller et al., 2008 [24] | 6.3 | 12 | 12/529.2 = 2.27 | 84 × 6.3 = 529.2 | NR | 77% |
| Behr et al., 1998 [12] | 11 | 7 | 7/1320 = 0.53 | 120 × 11 = 1320 | NR | 62% |
| Botelho et al., 2014 [25] | 9.4 | 46 | 46/1983.4 = 2.32 | 211 × 9.4 = 1983.4 | 84.4% | 90% |
| Garnett et al., 2006 [26] | 11 | 31 | 31/803 = 3.86 | 73 × 11 = 803 | NR | 75% |
| Kern, 2005 [27] | 5.3 | 10 | 10/196.1 = 5.10 | 37 × 5.3 = 196.1 | NR | 83.1% |
| Kern, 2017 [28] | 15.7 | 4 | 4/345.4 = 1.16 | 22 × 15.7 = 345.4 | NR | 90.9% |
| Kern et al., 2017 [29] | 7.7 | 13 | 13/831.6 = 1.56 | 108 × 7.7 = 831.6 | 93.1% | NR |
| Sailer et al., 2013 [30] | 6 | 2 | 2/84 = 2.38 | 14 × 6 = 84 | NR | 100% |
| Sasse and Kern, 2013 [31] | 5.4 | 4 | 4/162 = 2.47 | 30 × 5.4 = 162 | NR | 93.3% |
| Sasse and Kern, 2014 [32] | 5.2 | 3 | 3/218.4 = 1.37 | 42 × 5.2 = 218.4 | 93% | NR |
| Younes et al., 2013 [33] | 7 | 10 | 10/294 = 3.4 | 42 × 7 = 294 | NR | 83% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, M.C.; Azevedo, L.; Fonseca, P.; Viana, P.C.; Araújo, F.; Villarinho, E.; Fernandes, G.V.O.; Correia, A. The Success Rate of the Adhesive Partial Fixed Prosthesis after Five Years: A Systematic Review. Prosthesis 2023, 5, 282-294. https://doi.org/10.3390/prosthesis5010021
Santos MC, Azevedo L, Fonseca P, Viana PC, Araújo F, Villarinho E, Fernandes GVO, Correia A. The Success Rate of the Adhesive Partial Fixed Prosthesis after Five Years: A Systematic Review. Prosthesis. 2023; 5(1):282-294. https://doi.org/10.3390/prosthesis5010021
Chicago/Turabian StyleSantos, Maria Catarina, Luis Azevedo, Patrícia Fonseca, Pedro Couto Viana, Filipe Araújo, Eduardo Villarinho, Gustavo Vicentis Oliveira Fernandes, and André Correia. 2023. "The Success Rate of the Adhesive Partial Fixed Prosthesis after Five Years: A Systematic Review" Prosthesis 5, no. 1: 282-294. https://doi.org/10.3390/prosthesis5010021