
Testing the Use of Advanced Upper Limb Prostheses: Towards Quantifying the Movement Quality with Inertial-Magnetic Measurement Units
 ,
,
Abstract
:1. Introduction
2. Design of the Test Procedure—Methods
2.1. Participants
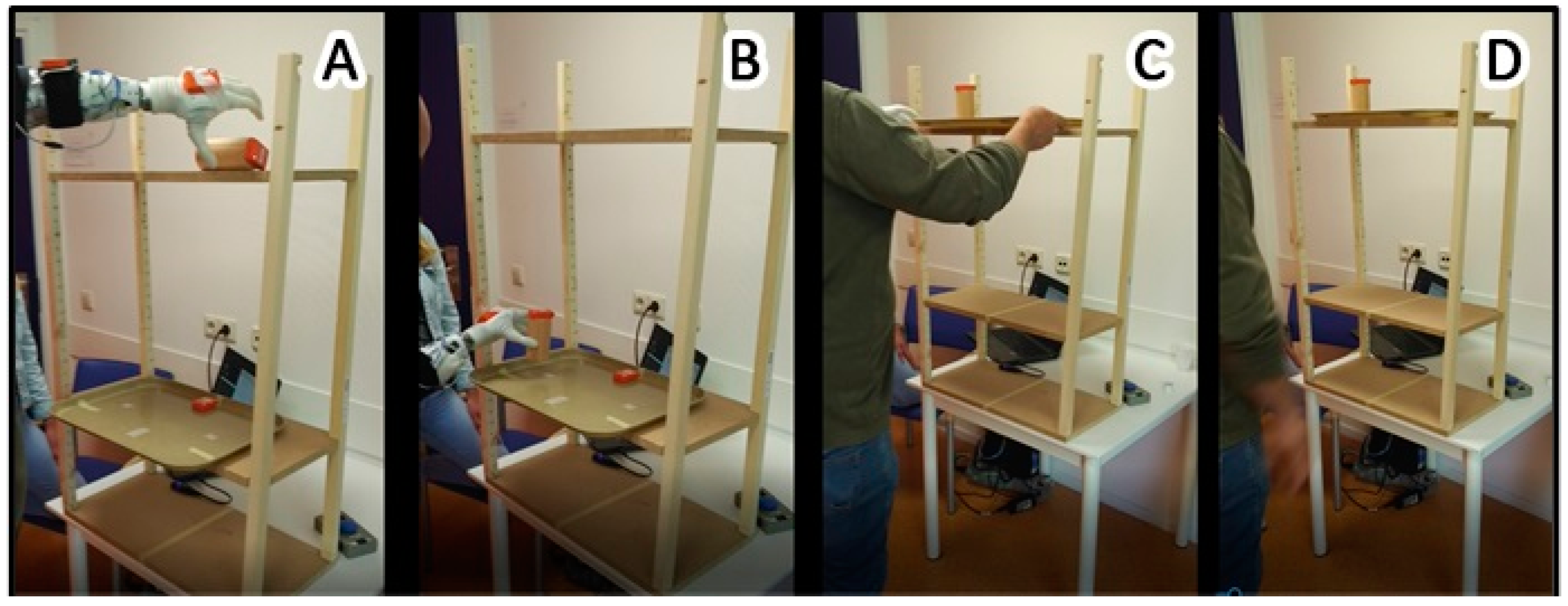
2.2. Description of the Task
2.3. Data Recording and Analysis
2.3.1. Placement of IMMUs
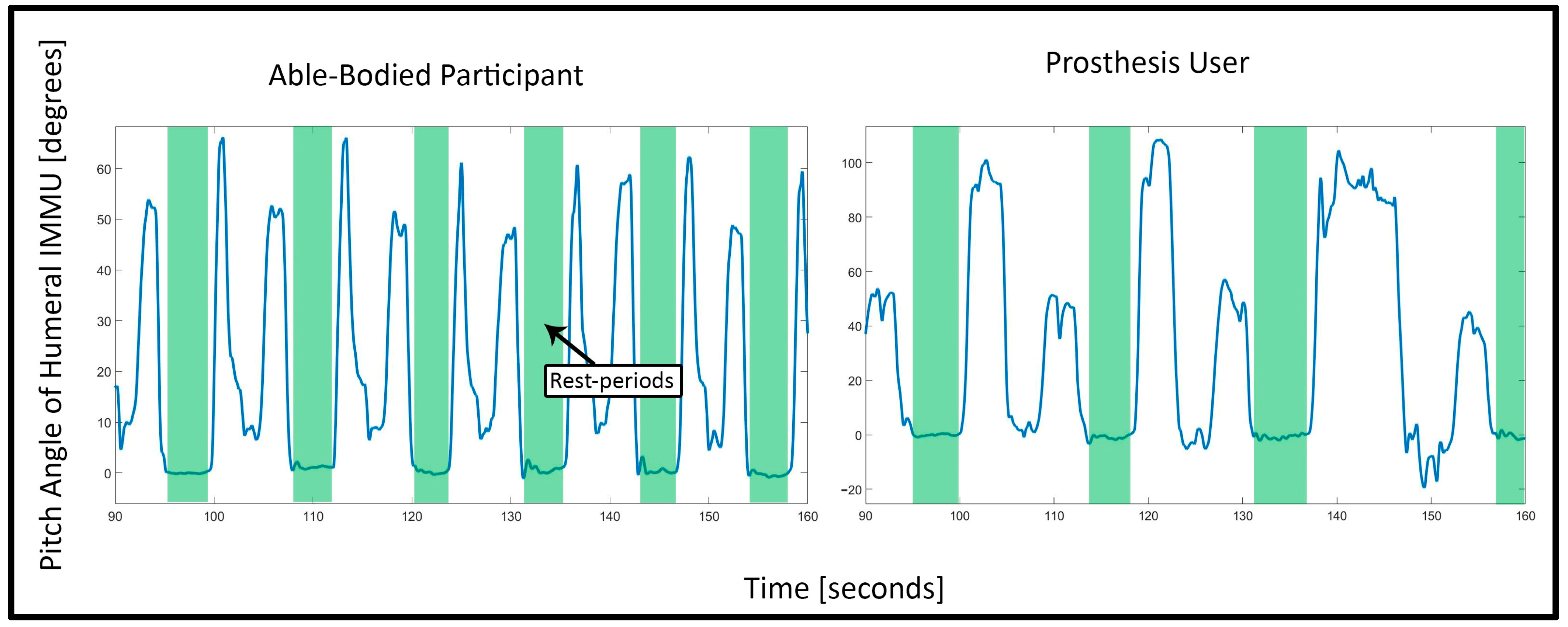
2.3.2. Determination of Onset and Ending of One Repetition
2.3.3. Calculation of 3D Orientation and Range of Motion
2.3.4. Smoothness
2.3.5. Stability of Coordination
2.3.6. Statistical Analysis
3. Results
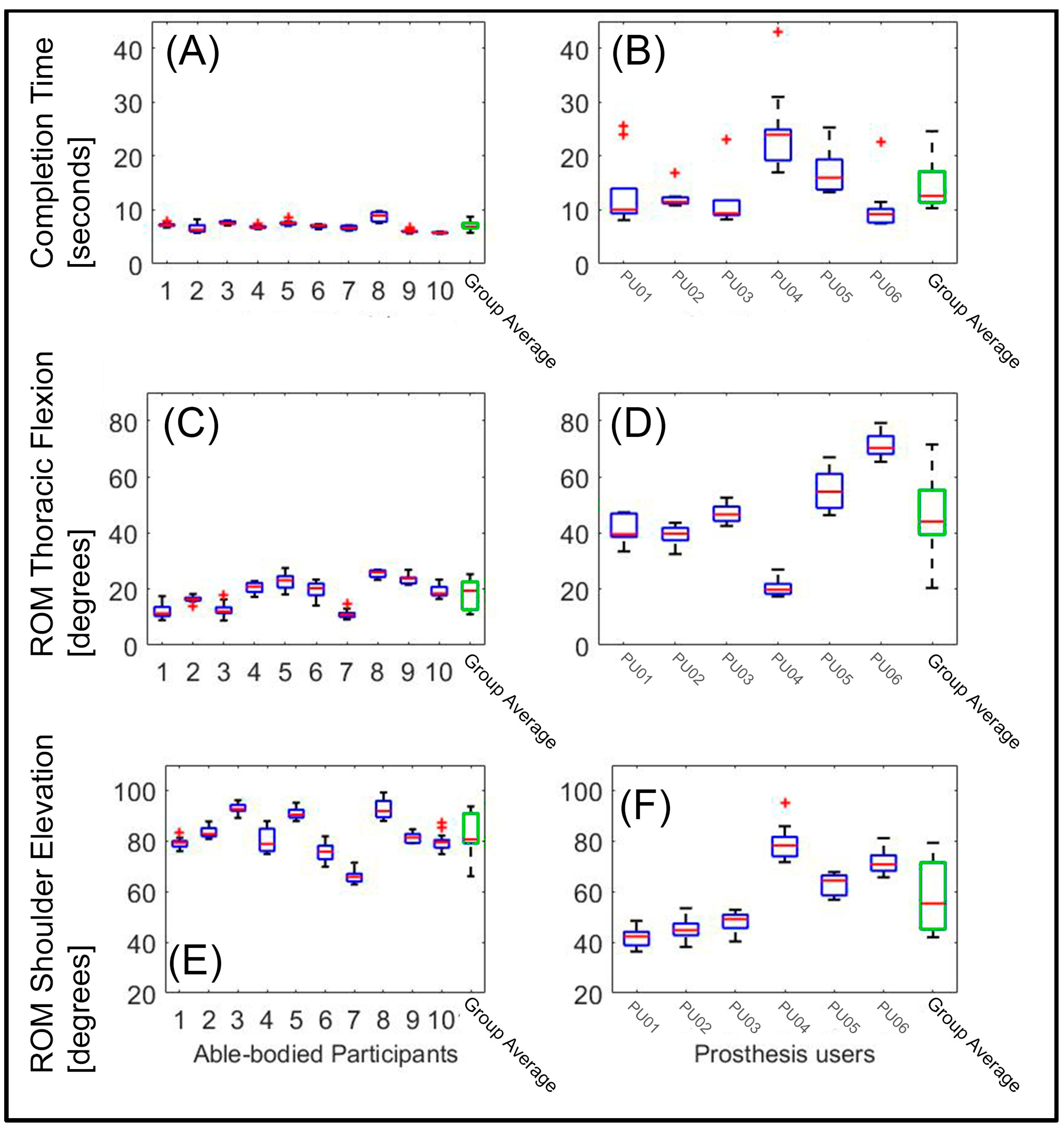
3.1. Average Time to Completion
3.2. Range of Motion (ROM) in Body Angles: Thoracic Flexion (Anterior/Posterior) and Humeral Elevation
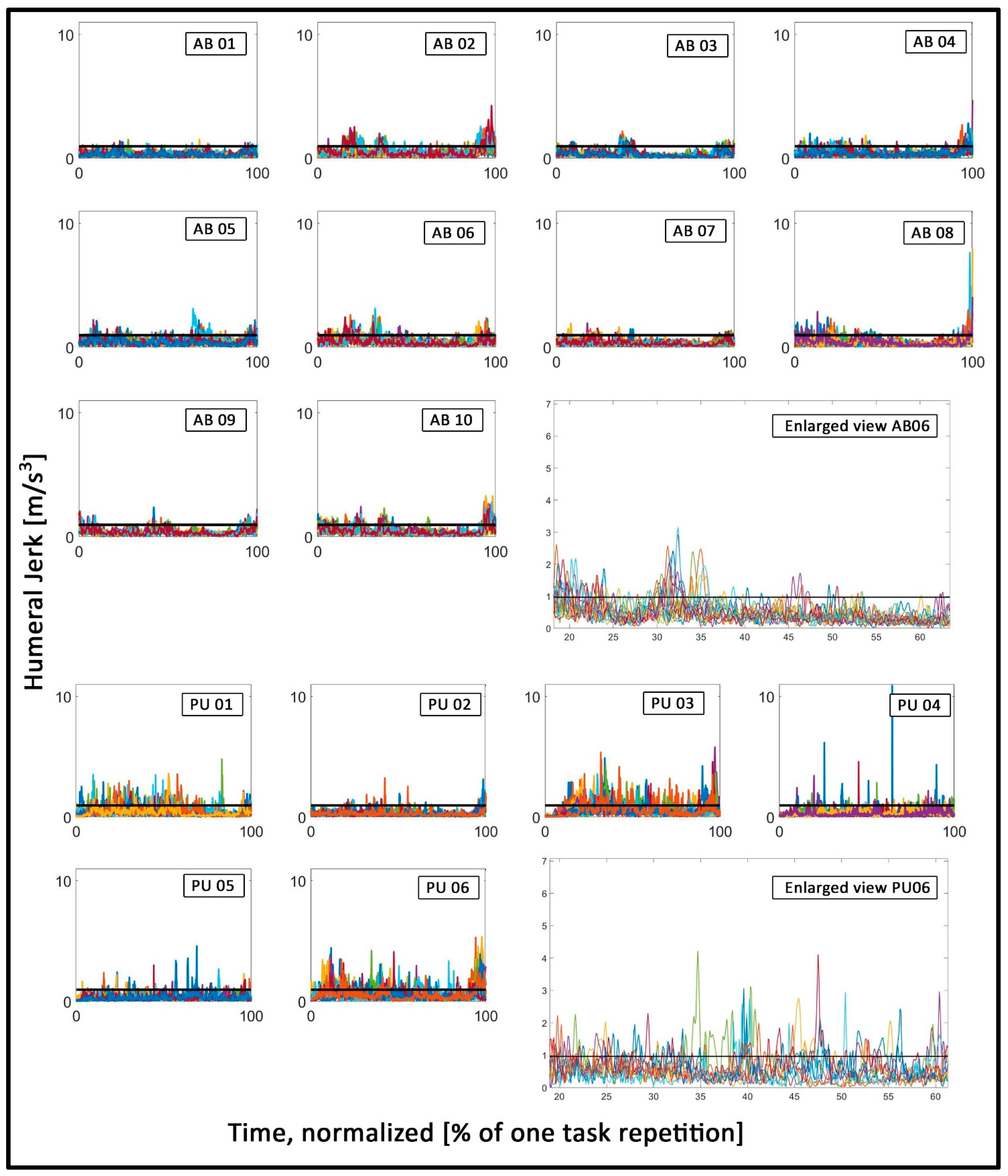
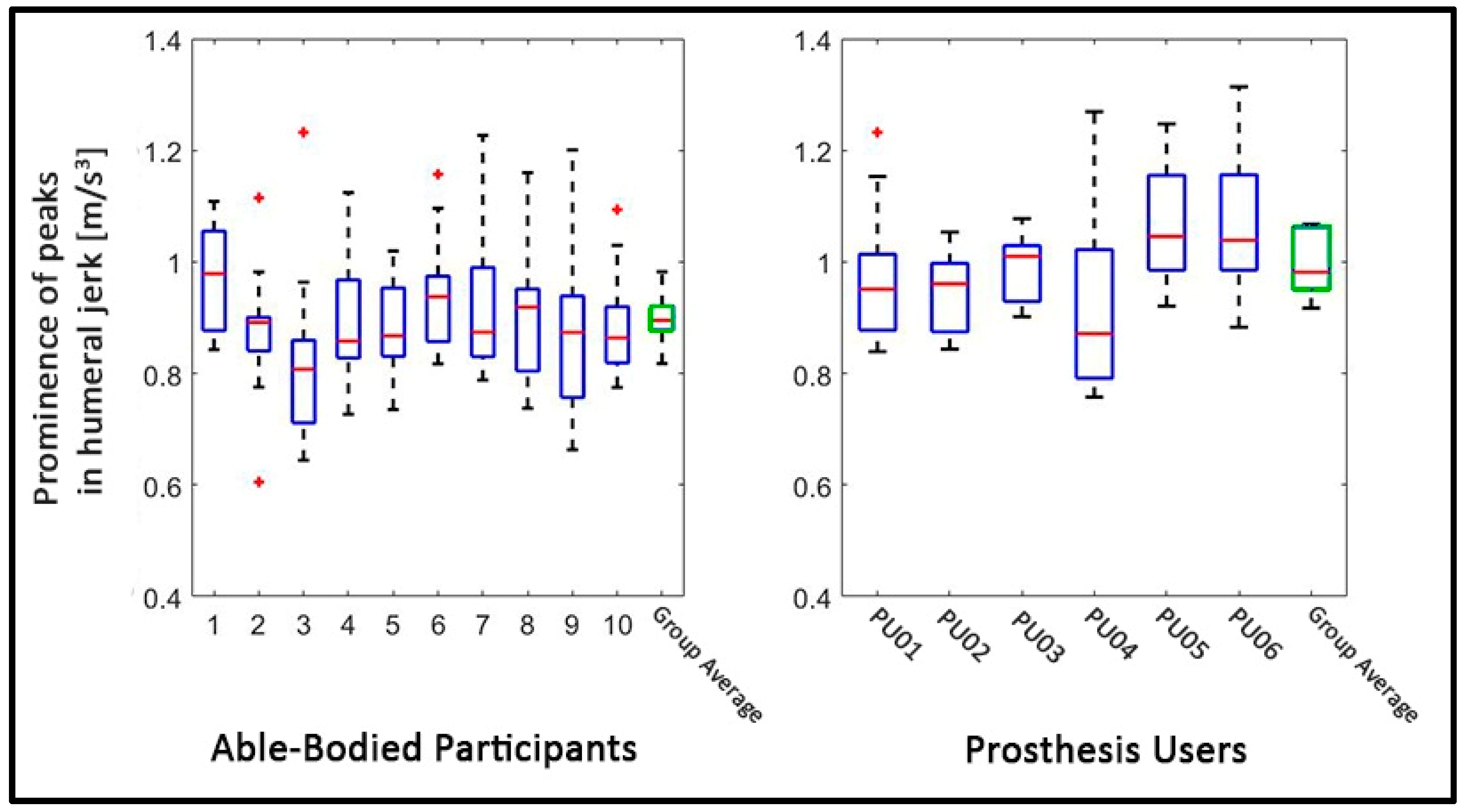
3.3. Smoothness of Motion: Prominence of Peaks in Humeral Jerk
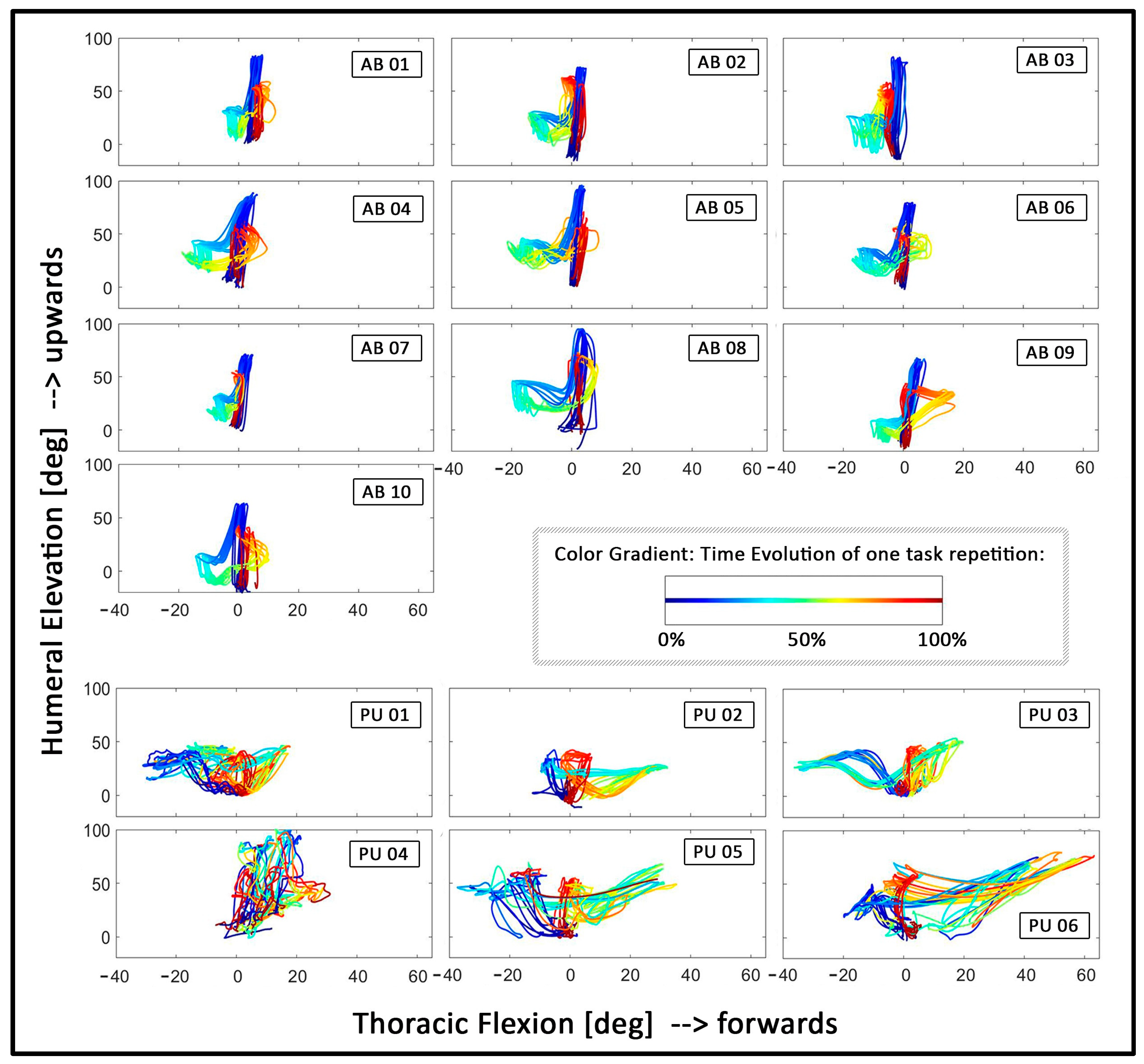
3.4. Coordination: Relative Motion between Thoracic Flexion and Humeral Elevation
4. Discussion
4.1. Challenges in the Design of a New Assessment of Upper Limb Prosthetics
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACMC | Assessment of capacity for myoelectric control |
| ADL | Activity of daily living |
| AM-ULA | Activities Measure for Upper Limb Amputees |
| ARAT | The Action Research Arm Test |
| BBT | Box and Block Test |
| BAM-ULA | Brief Activity Measure for Upper Limb Amputees |
| CRT | Clothespin Relocation Test |
| ICF | International Classification of Functioning Disability and Health |
| IMMUs | Inertial–magnetic measurement units |
| ISB | International Society of Biomechanics |
| J-T HFT | Jebsen–Taylor Hand Function Test |
| ROM | Range of motion |
| SHAP | The Southampton Hand Assessment Procedure |
| T-MAP | timed measure of activity performance for persons with upper limb amputation |
| UNB | University of New Brunswick Test of Prosthetic Function |
References
- Atzori, M.; Muller, H. Control Capabilities of Myoelectric Robotic Prostheses by Hand Amputees: A Scientific Research and Market Overview. Front. Syst. Neurosci. 2015, 9, 162. Available online: http://www.ncbi.nlm.nih.gov/pubmed/26648850%5Cnhttp://www.ncbi.nlm.nih.gov/pmc/articles/PMC4663252/pdf/fnsys-09-00162.pdf (accessed on 5 February 2021). [CrossRef] [PubMed]
- Hudgins, B.; Parker, P.; Scott, R.N. A New Strategy for Multifunction Myoelectric Control. IEEE Trans. Biomed. Eng. 1993, 40, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Belter, J.T.; Segil, J.L.; Dollar, A.M.; Weir, R.F. Mechanical Design and Performance Specifications of Anthropomorphic Prosthetic Hands: A Review. J. Rehabil. Res. Dev. 2013, 50, 599–618. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24013909 (accessed on 5 February 2021). [CrossRef] [PubMed]
- Scheme, E.; Englehart, K. Electromyogram Pattern Recognition for Control of Powered Upper-Limb Prostheses: State of the Art and Challenges for Clinical Use. J. Rehabil. Res. Dev. 2011, 48, 643–660. Available online: http://www.rehab.research.va.gov/jour/11/486/pdf/scheme486.pdf (accessed on 5 February 2021). [CrossRef]
- Vujaklija, I.; Roche, A.D.; Hasenoehrl, T.; Sturma, A.; Amsuess, S.; Farina, D.; Aszmann, O.C. Translating research on myoelectric control into clinics-are the performance assessment methods adequate? Front Neurorobot. 2017, 11, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farina, D.; Aszmann, O. Bionic limbs: Clinical reality and academic promises. Sci. Transl. Med. 2014, 6, 257. [Google Scholar] [CrossRef]
- Hill, W.; Kyberd, P.; Norling Hermansson, L.; Hubbard, S.; Stavdahl, Ø.; Swanson, S. Upper Limb Prosthetic Outcome Measures (ULPOM): A Working Group and Their Findings. JPO J. Prosthet. Orthot. 2009, 21, P69–P82. [Google Scholar] [CrossRef]
- Light, C.M.; Chappell, P.H.; Kyberd, P.J. Establishing a standardized clinical assessment tool of pathologic and prosthetic hand function: Normative data, reliability, and validity. Arch. Phys. Med. Rehabil. 2002, 83, 776–783. [Google Scholar] [CrossRef] [Green Version]
- Burgerhof, J.G.M.; Vasluian, E.; Dijkstra, P.U.; Bongers, R.M.; van der Sluis, C.K. The Southampton Hand Assessment Procedure revisited: A transparent linear scoring system, applied to data of experienced prosthetic users. J. Hand. Ther. 2017, 30, 49–57. [Google Scholar] [CrossRef]
- Hussaini, A.; Kyberd, P. Refined clothespin relocation test and assessment of motion. Prosthet. Orthot. Int. 2017, 41, 294–302. [Google Scholar] [CrossRef]
- Kyberd, P.; Hussaini, A.; Maillet, G. Characterisation of the Clothespin Relocation Test as a functional assessment tool. J. Rehabil. Assist. Technol. Eng. 2018, 5, 2055668317750810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussaini, A.; Hill, W.; Kyberd, P. Clinical evaluation of the refined clothespin relocation test: A pilot study. Prosthet. Orthot. Int. 2019, 43, 485–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carroll, D. A quantitative test of upper extremity function. J. Chronic Dis. 1965, 18, 479–491. [Google Scholar] [CrossRef] [Green Version]
- Lyle, R.C. A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int. J. Rehabil. Res. 1981, 4, 483–492. [Google Scholar] [CrossRef] [PubMed]
- van der Lee, J.H.; Roorda, L.D.; Beckerman, H.; Lankhorst, G.J.; Bouter, L.M. Improving the Action Research Arm test: A unidimensional hierarchical scale. Clin. Rehabil. 2002, 16, 646–653. [Google Scholar] [CrossRef] [Green Version]
- Yozbatiran, N.; Der-Yeghiaian, L.; Cramer, S.C. A standardized approach to performing the action research arm test. Neurorehabil. Neural. Repair 2008, 22, 78–90. [Google Scholar] [CrossRef] [Green Version]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult norms for the Box and Block Test of manual dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Resnik, L.; Adams, L.; Borgia, M.; Delikat, J.; Disla, R.; Ebner, C.; Walters, L.S. Development and evaluation of the activities measure for upper limb amputees. Arch. Phys. Med Rehabil. 2013, 94, 488–494. [Google Scholar] [CrossRef]
- Resnik, L.; Borgia, M.; Acluche, F. Brief activity performance measure for upper limb amputees: BAM-ULA. Prosthet. Orthot. Int. 2018, 42, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Hermansson, L.M.; Fisher, A.G.; Bernspang, B.; Eliasson, A.-C. Assessment of capacity for myoelectric control: A new Rasch-built measure of prosthetic hand control. J. Rehabil. Med. 2005, 37, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Hermansson, L.M.; Bodin, L.; Eliasson, A.-C. Intra- and inter-rater reliability of the assessment of capacity for myoelectric control. J. Rehabil. Med. 2006, 38, 118–123. [Google Scholar] [CrossRef] [Green Version]
- Jebsen, R.H.; Taylor, N.; Trieschmann, R.B.; Trotter, M.J.; Howard, L.A. An objective and standardized test of hand function. Arch. Phys. Med. Rehabil. 1969, 50, 311–319. [Google Scholar] [PubMed]
- Sanderson, E.R.; Scott, R.N. UNB Test of Prosthetics Function: A Test for Unilateral Upper Extremity Amputees, Ages 2–13; Institute of Biomedical Engineering, University of New Brunswick: Fredericton, NB, Canada, 1985. [Google Scholar]
- Resnik, L.; Borgia, M.; Acluche, F. Timed activity performance in persons with upper limb amputation: A preliminary study. J. Hand Ther. 2017, 30, 468–476. [Google Scholar] [CrossRef] [PubMed]
- WHO. The International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2001; Volume 18, p. 237. [Google Scholar]
- Carey, S.L.; Jason Highsmith, M.; Maitland, M.E.; Dubey, R.V. Compensatory movements of transradial prosthesis users during common tasks. Clin. Biomech. 2008, 23, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Carey, S.L.; Dubey, R.V.; Bauer, G.S.; Highsmith, M.J. Kinematic comparison of myoelectric and body powered prostheses while performing common activities. Prosthet. Orthot. Int. 2009, 33, 179–186. [Google Scholar] [CrossRef]
- Hebert, J.S.; Lewicke, J. Case report of modified Box and Blocks test with motion capture to measure prosthetic function. J. Rehabil. Res. Dev. 2012, 49, 1163–1174. [Google Scholar] [CrossRef]
- Major, M.J.; Stine, R.L.; Heckathorne, C.W.; Fatone, S.; Gard, S.A. Comparison of range-of-motion and variability in upper body movements between transradial prosthesis users and able-bodied controls when executing goal-oriented tasks. J. Neuroeng. Rehabil. 2014, 11, 132. [Google Scholar] [CrossRef] [Green Version]
- Hebert, J.S.; Boser, Q.A.; Valevicius, A.M.; Tanikawa, H.; Lavoie, E.B.; Vette, A.H.; Pilarski, P.M.; Chapman, C.S. Quantitative Eye Gaze and Movement Differences in Visuomotor Adaptations to Varying Task Demands Among Upper-Extremity Prosthesis Users. JAMA Netw. Open 2019, 2, e1911197. [Google Scholar] [CrossRef] [Green Version]
- Valevicius, A.M.; Boser, Q.A.; Chapman, C.S.; Pilarski, P.M.; Vette, A.H.; Hebert, J.S. Compensatory strategies of body-powered prosthesis users reveal primary reliance on trunk motion and relation to skill level. Clin. Biomech. 2019, 21, 74–78. [Google Scholar] [CrossRef]
- Bouwsema, H.; der Sluis CK van Bongers, R.M. Movement characteristics of upper extremity prostheses during basic goal-directed tasks. Clin. Biomech. 2010, 25, 523–529. [Google Scholar] [CrossRef] [Green Version]
- Bouwsema, H.; Kyberd, P.J.; Hill, W.; van der Sluis, C.K.; Bongers, R.M. Determining Skill Level in Myoelectric Prosthesis Use with Multiple Outcome Measures. J. Rehabil. Res. Dev. 2012, 49, 1331. Available online: http://www.rehab.research.va.gov/jour/2012/499/pdf/bouwsema499.pdf (accessed on 8 May 2022). [CrossRef] [PubMed] [Green Version]
- Thies, S.B.; Kenney, L.P.; Sobuh, M.; Galpin, A.; Kyberd, P.; Stine, R.; Major, M.J. Skill assessment in upper limb myoelectric prosthesis users: Validation of a clinically feasible method for characterising upper limb temporal and amplitude variability during the performance of functional tasks. Med. Eng. Phys. 2017, 47, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Valevicius, A.M.; Jun, P.Y.; Hebert, J.S.; Vette, A.H. Use of Optical Motion Capture for the Analysis of Normative Upper Body Kinematics during Functional Upper Limb Tasks: A Systematic Review. J. Electromyogr. Kinesiol. 2018, 40, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.E.; Davidson, J.H. Save that arm: A study of problems in the remaining arm of unilateral upper limb amputees. Prosthet. Orthot. Int. 1999, 2355–2358. [Google Scholar] [CrossRef] [Green Version]
- Hanley, M.A.; Ehde, D.M.; Jensen, M.; Czerniecki, J.; Smith, D.G.; Robinson, L.R. Chronic Pain Associated with Upper-Limb Loss and VA Puget Sound HealthCare System. Am. J. Phys. Med. Rehabil. 2009, 88, 742–779. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3079279/pdf/nihms264457.pdf (accessed on 5 February 2021). [CrossRef] [Green Version]
- Østlie, K.; Franklin, R.J.; Skjeldal, O.H.; Skrondal, A.; Magnus, P. Musculoskeletal Pain and Overuse Syndromes in Adult Acquired Major Upper-Limb Amputees. Arch. Phys. Med. Rehabil. 2011, 92, 1967–1973.e1. [Google Scholar] [CrossRef] [PubMed]
- Johansen, H.; Østlie, K.; Andersen, L.Ø.; Rand-Hendriksen, S. Adults with congenital limb deficiency in Norway: Demographic and clinical features, pain and the use of health care and welfare services. A cross-sectional study. Disabil. Rehabil. 2015, 37, 2076–2082. [Google Scholar] [CrossRef]
- Postema, S.G.; Bongers, R.M.; Brouwers, M.A.; Burger, H.; Norling-Hermansson, L.M.; Reneman, M.F.; Dijkstra, P.U.; van der Sluis, C.K. Musculoskeletal Complaints in Transverse Upper Limb Reduction Deficiency and Amputation in the Netherlands: Prevalence, Predictors, and Effect on Health. Arch. Phys. Med. Rehabil. 2016, 97, 1137–1145. [Google Scholar] [CrossRef]
- Wright, F.V.; Rosenbaum, P.L.; Goldsmith, C.H.; Law, M.; Fehlings, D.L. How do changes in body functions and structures, activity, and participation relate in children with cerebral palsy? Dev. Med. Child. Neurol. 2008, 50, 283–289. [Google Scholar] [CrossRef]
- Wright, V. Prosthetic outcome measures for use with upper limb amputees: A systematic review of the peer-reviewed literature, 1970–2009. J. Prosthet. Orthot. 2009, 21, 64–68. [Google Scholar] [CrossRef]
- Spiers, A.J.; Resnik, L.; Dollar, A.M. Analyzing at-home prosthesis use in unilateral upper-limb amputees to inform treatment & device design. In IEEE International Conference on Rehabilitation Robotics; IEEE: Piscataway, NY, USA, 2017; pp. 1273–1280. [Google Scholar]
- Franzke, A.W.; Kristoffersen, M.B.; Bongers, R.; Murgia, A.; Pobatschnig, B.; Unglaube, F.; Van Der Sluis, C.K. Users’ and therapists’ perceptions of myoelectric multi-function upper limb prostheses with conventional and pattern recognition control. PLoS ONE 2019, 14, e0220899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidovic, M.M.C.; Hwang, H.J.; Amsuss, S.; Hahne, J.M.; Farina, D.; Muller, K.R. Improving the robustness of myoelectric pattern recognition for upper limb prostheses by covariate shift adaptation. IEEE Trans. Neural. Syst. Rehabil. Eng. 2016, 24, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Dosen, S.; Muller, K.R.; Farina, D. Myoelectric control of artificial limbsis there a need to change focus? [In the Spotlight]. IEEE Signal Process. Mag. 2012, 29, 148–152. [Google Scholar]
- Cohen, M. Brain Mapping, Handedness Questionnaire 2008 [cited 2005 Jul 20]. Available online: http://www.brainmapping.org/shared/Edinburgh.php (accessed on 5 February 2021).
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Metzger, A.J.; Dromerick, A.W.; Holley, R.J.; Lum, P.S. Characterization of Compensatory Trunk Movements during Prosthetic Upper Limb Reaching Tasks. Arch. Phys. Med. Rehabil 2012, 93, 2029–2034. [Google Scholar] [CrossRef]
- van der Laan, T.M.J.; Postema, S.G.; Reneman, M.F.; Bongers, R.M.; van der Sluis, C.K. Development and Reliability of the Rating of Compensatory Movements in Upper Limb Prosthesis Wearers during Work-Related Tasks. J. Hand Ther. 2019, 32, 368–374. [Google Scholar] [CrossRef]
- Wu, G.; van der Helm, F.; Veeger, D.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Robertson, D.G.E.; Caldwell, G.E.; Hamill, J.; Kamen, G.; Whittlesey, S.N. Research Methods in Biomechanics; Human Kinetics: Champaign, IL, USA, 2014. [Google Scholar]
- Biddiss, E.; Chau, T.T. Upper limb prosthesis use and abandonment: A survey of the last 25 years. Prosthet. Orthot. Int. 2007, 31, 236–257. [Google Scholar] [CrossRef]
- Østlie, K.; Lesjø, I.M.; Franklin, R.J.; Garfelt, B.; Skjeldal, O.H.; Magnus, P. Prosthesis rejection in acquired major upper-limb amputees: A population-based survey. Disabil. Rehabil. Assist Technol. 2012, 7, 294–303. [Google Scholar] [CrossRef]
- Hill, W.; Stavdahl, Ø.; Hermansson, L.N.; Kyberd, P.; Swanson, S.; Hubbard, S. Functional outcomes in the WHO-ICF model: Establishment of the upper limb prosthetic outcome measures group. J. Prosthet. Orthot. 2009, 21, 115–119. [Google Scholar] [CrossRef]
- Hussaini, A.; Zinck, A.; Kyberd, P. Categorization of compensatory motions in transradial myoelectric prosthesis users. Prosthet. Orthot. Int. 2017, 41, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Michaelsen, S.M.; Jacobs, S.; Roby-Brami, A.; Levin, M.F. Compensation for distal impairments of grasping in adults with hemiparesis. Exp. Brain Res. 2004, 157, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Valevicius, A.M.; Boser, Q.A.; Lavoie, E.B.; Chapman, C.S.; Pilarski, P.M.; Hebert, J.S.; Vette, A.H. Characterization of Normative Angular Joint Kinematics during Two Functional Upper Limb Tasks. Gait Posture 2019, 69, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Flash, T.; Hogan, N. The Coordination of Arm Movements: An Experimentally Confirmed Mathematical Model. J. Neurosci. 1985, 5, 1688–1703. Available online: http://www.ncbi.nlm.nih.gov/pubmed/4020415 (accessed on 5 February 2021). [CrossRef] [PubMed]
- Krebs, H.I.; Hogan, N.; Aisen, M.L.; Volpe, B.T. Robot-aided neurorehabilitation. IEEE Trans. Rehabil. Eng. 1998, 6, 75–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sejnowski, T.J. Neurobiology. In Making Smooth Moves; Nature: York, UK, 1998; Volume 394, pp. 725–726. [Google Scholar]
- Refai, M.I.M.; Saes, M.; Scheltinga, B.L.; van Kordelaar, J.; Bussmann, J.B.J.; Veltink, P.H.; Buurke, J.H.; Meskers, C.G.M.; van Wegen, E.E.H.; Kwakkel, G.; et al. Smoothness Metrics for Reaching Performance after Stroke. Part 1: Which One to Choose? J. Neuroeng. Rehabil. 2021, 18, 1–16. [Google Scholar] [CrossRef]
- Bayle, N.; Lempereur, M.; Hutin, E.; Motavasseli, D.; Remy-Neris, O.; Gracies, J.-M.; Cornec, G. Comparison of Various Smoothness Metrics for Upper Limb Movements in Middle-Aged Healthy Subjects. Sensors 2023, 23, 1158. [Google Scholar] [CrossRef]
- Chadwell, A.; Kenney, L.; Thies, S.; Head, J.; Galpin, A.; Baker, R. Addressing unpredictability may be the key to improving performance with current clinically prescribed myoelectric prostheses. Sci. Rep. 2021, 11, 3300. [Google Scholar] [CrossRef]
- Touillet, A.; Gouzien, A.; Badin, M.; Herbe, P.; Martinet, N.; Jarrassé, N.; Roby-Brami, A. Kinematic analysis of impairments and compensatory motor behavior during prosthetic grasping in below-elbow amputees. PLoS ONE 2022, 17, e0277917. [Google Scholar] [CrossRef]
- Bloomer, C.; Kontson, K.L. Comparison of DEKA Arm and Body-Powered Upper Limb Prosthesis Joint Kinematics. Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100057. [Google Scholar] [CrossRef]
- Kontson, K.L.; Wang, S.; Barovsky, S.; Bloomer, C.; Wozniczka, L.; Civillico, E.F. Assessing Kinematic Variability during Performance of Jebsen-Taylor Hand Function Test. J. Hand Ther. 2020, 33, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Kontson, K.; Marcus, I.; Myklebust, B.; Civillico, E. Targeted box and blocks test: Normative data and comparison to standard tests. PLoS ONE 2017, 12, e0177965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chadwell, A.; Kenney, L.; Granat, M.; Thies, S.; Head, J.S.; Galpin, A. Visualisation of Upper Limb Activity Using Spirals: A New Approach to the Assessment of Daily Prosthesis Usage. Prosthet. Orthot. Int. 2017, 42, 37–44. Available online: http://journals.sagepub.com/doi/10.1177/0309364617706751 (accessed on 5 February 2021). [CrossRef] [PubMed] [Green Version]
- Williams, H.E.; Chapman, C.S.; Pilarski, P.M.; Vette, A.H.; Hebert, J.S. Myoelectric Prosthesis Users and Non-Disabled Individuals Wearing a Simulated Prosthesis Exhibit Similar Compensatory Movement Strategies. J. Neuroeng. Rehabil. 2021, 18, 1–15. [Google Scholar] [CrossRef]
- Thies, S.B.; A Tresadern, P.; Kenney, L.P.; Smith, J.; Howard, D.; Goulermas, J.Y.; Smith, C.; Rigby, J. Movement variability in stroke patients and controls performing two upper limb functional tasks: A new assessment methodology. J. Neuroeng. Rehabil. 2009, 6, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Latash, M.L.; Anson, J.G. What are “normal movements” in atypical populations? Behav. Brain Sci. 1996, 19, 55. [Google Scholar] [CrossRef]
- Wang, S.L.; Bloomer, C.; Civillico, G.; Kontson, K. Application of Machine Learning to the Identification of Joint Degrees of Freedom Involved in Abnormal Movement during Upper Limb Prosthesis Use. PLoS ONE 2021, 16, e0246795. [Google Scholar] [CrossRef]
- Emmerik REA van Miller, R.H.; Hamill, J. Dynamical Systems Analysis of Coordination. In Research Methods in Biomechanics, 2nd ed; Robertson, D.G.E., Caldwell, G.E., Hamill, J., Kamen, G., Whittlesey, S.N., Eds.; Human Kinetics: Champaign, IL, USA, 2014; pp. 291–316. Available online: https://www.humankineticslibrary.com/encyclopedia-chapter?docid=b-9781492595809&tocid=b-9781492595809-chapter13 (accessed on 8 May 2022).
- Donker, S.F.; Beek, P.J. Interlimb coordination in prosthetic walking: Effects of asymmetry and walking velocity. Acta Psychol. 2002, 110, 265–288. [Google Scholar] [CrossRef]
- Krasovsky, T.; Baniña, M.C.; Hacmon, R.; Feldman, A.G.; Lamontagne, A.; Levin, M.F. Stability of gait and interlimb coordination in older adults. J. Neurophysiol. 2012, 107, 2560–2569. [Google Scholar] [CrossRef] [Green Version]
- Armitano, C.N.; Morrison, S.; Russell, D.M. Coordination stability between the legs is reduced after anterior cruciate ligament reconstruction. Clin. Biomech. 2018, 58, 28–33. [Google Scholar] [CrossRef]
- Yamagata, M.; Tateuchi, H.; Shimizu, I.; Saeki, J.; Ichihashi, N. The Relation between Limb Segment Coordination during Walking and Fall History in Community-Dwelling Older Adults. J. Biomech. 2019, 93, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Khoramshahi, M.; Roby-Brami, A.; Parry, R.; Jarrassé, N. Identification of inverse kinematic parameters in redundant systems: Towards quantification of inter-joint coordination in the human upper extremity. PLoS ONE 2022, 17, e0278228. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Age | Sex | Affected Side | Level | Cause of Upper Limb Defect | Prosthesis Type | Use of Prosthesis [Total Years] | Wearing Time [Days/Week] | Wearing Time [Hours/Day] |
|---|---|---|---|---|---|---|---|---|---|
| PU01 | 52 | F | L | TR | PD | Myoelectric, 1 DOF | 23 | 7 | 14 |
| PU02 | 39 | F | L | TC | Congenital | Myoelectric, 1 DOF | Prosthesis was used during 8 weeks in 2004; then abandoned. | 0 | 0 |
| PU03 | 59 | M | L | TR | Congenital | Myoelectric, 1 DOF | 45 | 6 | 8 |
| PU04 | 48 | M | R | TR | Trauma | Michelangelo Hand with Axon Rotation | 14 | 7 | 8 |
| PU05 | 46 | M | L | TR | PD | iLimb quantum | 5 | 7 | 4 |
| PU06 | 57 | M | L | TR | Trauma | iLimb quantum with gesture control | 13 | 7 | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franzke, A.W.; Kristoffersen, M.B.; Farina, D.; van der Sluis, C.K.; Bongers, R.M.; Murgia, A. Testing the Use of Advanced Upper Limb Prostheses: Towards Quantifying the Movement Quality with Inertial-Magnetic Measurement Units. Prosthesis 2023, 5, 264-281. https://doi.org/10.3390/prosthesis5010020
Franzke AW, Kristoffersen MB, Farina D, van der Sluis CK, Bongers RM, Murgia A. Testing the Use of Advanced Upper Limb Prostheses: Towards Quantifying the Movement Quality with Inertial-Magnetic Measurement Units. Prosthesis. 2023; 5(1):264-281. https://doi.org/10.3390/prosthesis5010020
Chicago/Turabian StyleFranzke, Andreas W., Morten B. Kristoffersen, Dario Farina, Corry K. van der Sluis, Raoul M. Bongers, and Alessio Murgia. 2023. "Testing the Use of Advanced Upper Limb Prostheses: Towards Quantifying the Movement Quality with Inertial-Magnetic Measurement Units" Prosthesis 5, no. 1: 264-281. https://doi.org/10.3390/prosthesis5010020