

Same-Day Digital Dentistry Restorative Workflow for Single Immediate Provisionalization of Narrow-Diameter Implants: An Exploratory Prospective Study
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
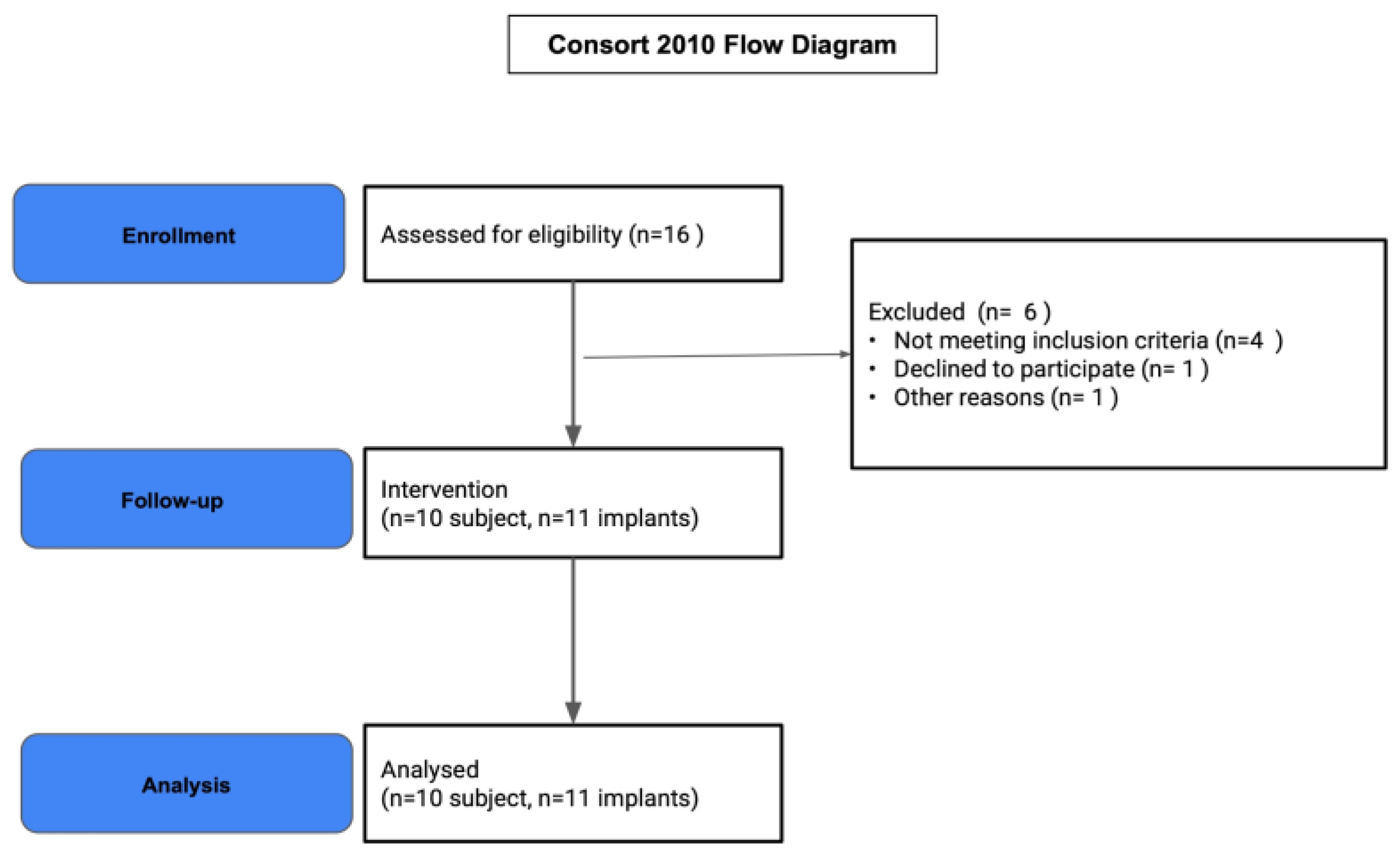
2.1. Study Population
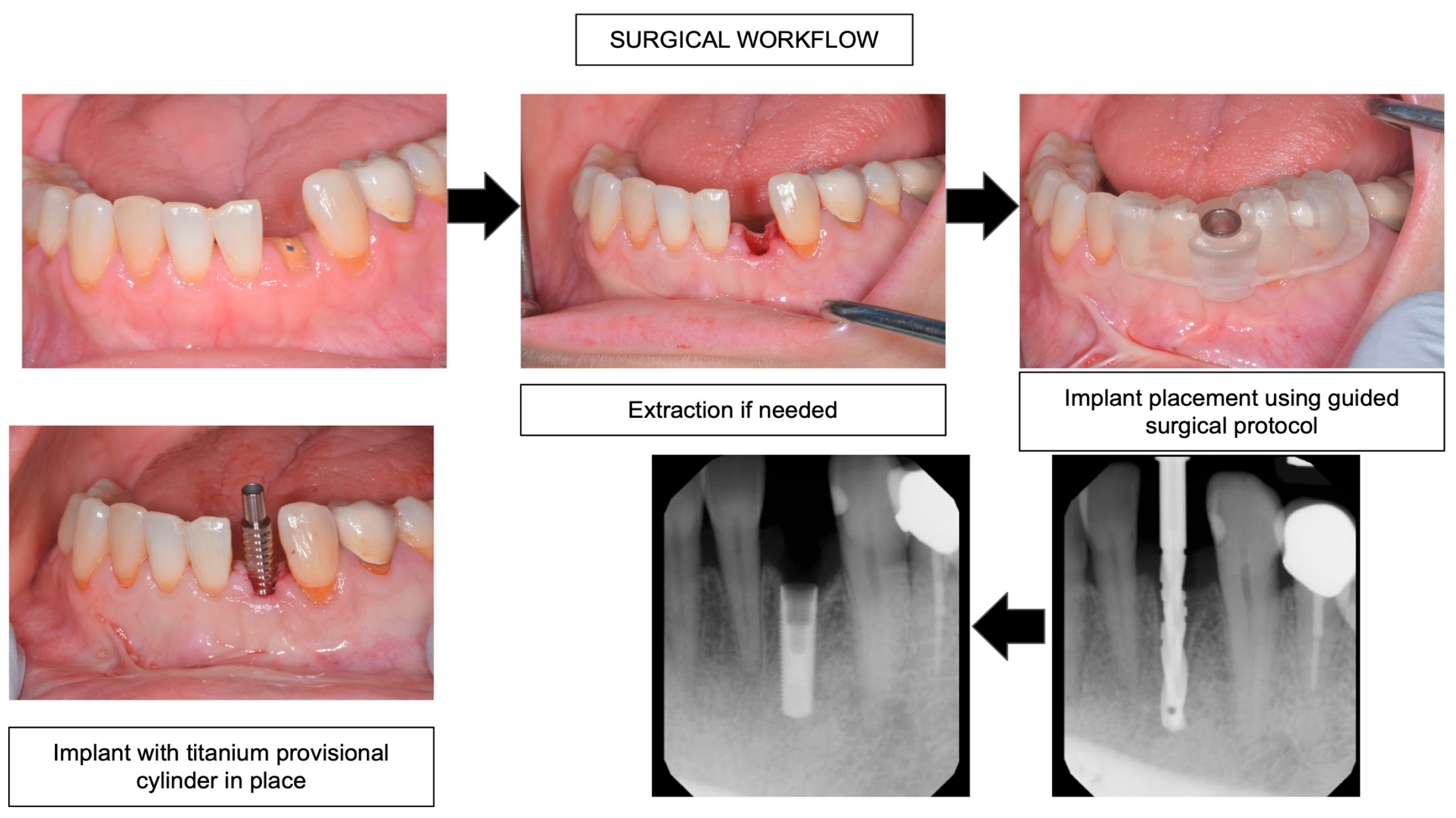
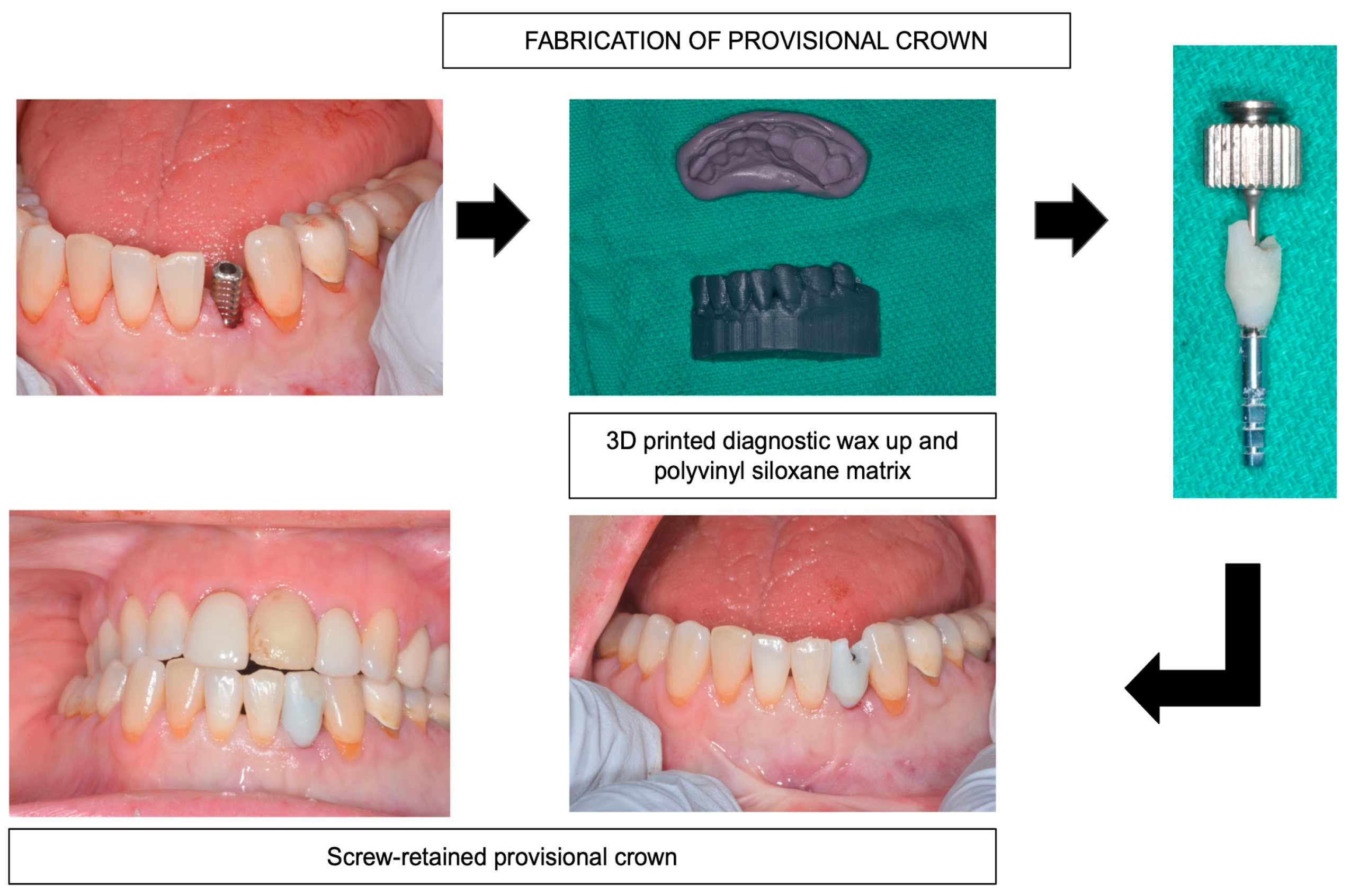
2.2. Clinical Protocol
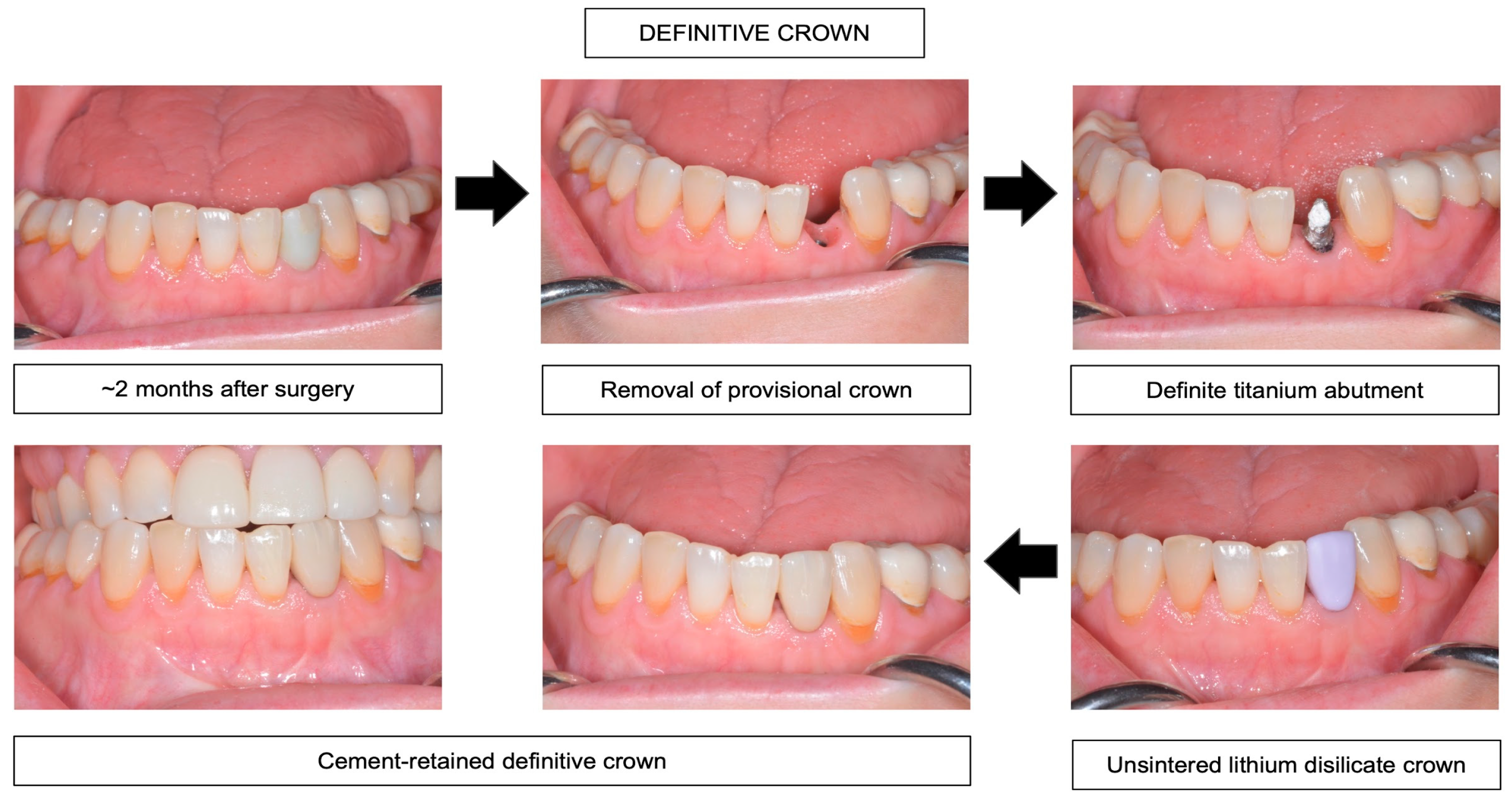
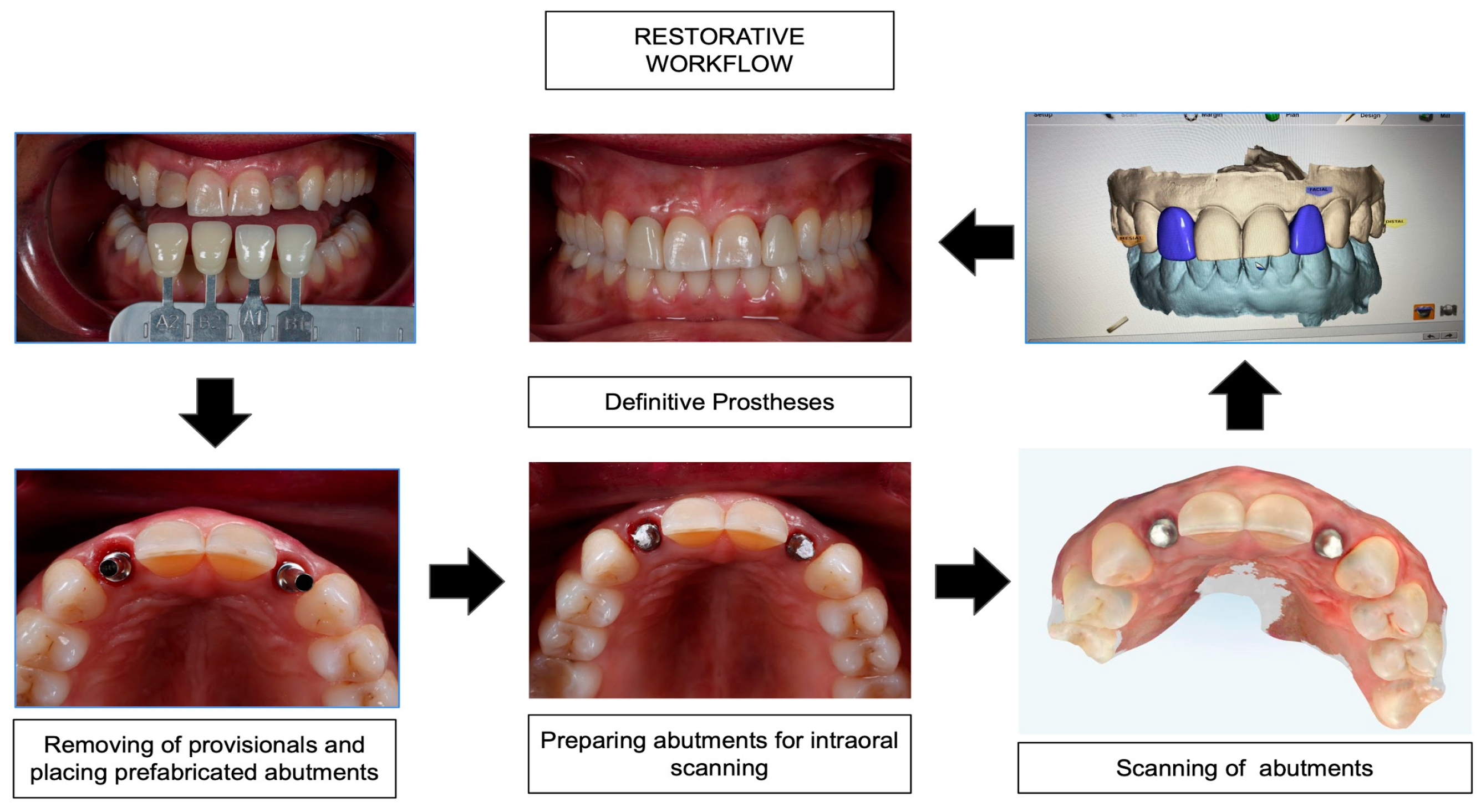
2.3. Same-Day Digital Dentistry Fabrication of Definitive Prosthesis
2.4. Clinical Evaluation of Peri-Implant Soft Tissue Health
2.5. Radiographic Evaluation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schiegnitz, E.; Al-Nawas, B. Narrow-Diameter Implants: A Systematic Review and Meta-Analysis. Clin. Oral Implants Res. 2018, 29 (Suppl. 16), 21–40. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.O.; Schiegnitz, E.; Al-Nawas, B. Systematic Review on Success of Narrow-Diameter Dental Implants. Int. J. Oral Maxillofac. Implants 2014, 29, 43–54. [Google Scholar] [CrossRef]
- Zhang, X.M.; Liu, B.L.; Qian, S.J.; Shi, J.Y.; Zhang, X.; Lai, H.C. Clinical evaluation of narrow-diameter implants versus standard-diameter implants with lateral bone augmentation in posterior jaws: Three-year results of a randomized controlled trial. Clin. Oral Implants Res. 2022, 33, 1245–1253. [Google Scholar] [CrossRef] [PubMed]
- Alrabiah, M. Comparison of Survival Rate and Crestal Bone Loss of Narrow Diameter Dental Implants versus Regular Dental Implants: A Systematic Review and Meta-Analysis. J. Investig. Clin. Dent. 2019, 10, e12367. [Google Scholar] [CrossRef] [PubMed]
- Worni, A.; Hicklin, S.P.; Mericske-Stern, R.; Enkling, N. Performance and Marginal Bone Level Alteration around Immediately Loaded Narrow-Diameter Implants. A Prospective Clinical Study: Results after 1 Year. Quintessence Int. 2018, 49, 267–276. [Google Scholar]
- Geckili, O.; Mumcu, E.; Bilhan, H. Radiographic Evaluation of Narrow-Diameter Implants after 5 Years of Clinical Function: A Retrospective Study. J. Oral Implantol. 2013, 39, 273–279. [Google Scholar] [CrossRef]
- Sierra-Sánchez, J.-L.; Martínez-González, A.; García-Sala Bonmatí, F.; Mañes-Ferrer, J.-F.; Brotons-Oliver, A. Narrow-Diameter Implants: Are They a Predictable Treatment Option? A Literature Review. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e74–e81. [Google Scholar] [CrossRef]
- Cruz, R.S.; Lemos, C.A.A.; de Batista, V.E.S.; Yogui, F.C.; Oliveira, H.F.F.; Verri, F.R. Narrow-Diameter Implants versus Regular-Diameter Implants for Rehabilitation of the Anterior Region: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Surg. 2021, 50, 674–682. [Google Scholar] [CrossRef]
- Parize, H.; Bohner, L.; Gama, L.; Porporatti, A.; Mezzomo, L.; Martin, W.; Gonçalves, T. Narrow-Diameter Implants in the Anterior Region: A Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2019, 34, 1347–1358. [Google Scholar] [CrossRef]
- Davarpanah, M.; Martinez, H.; Tecucianu, J.F.; Celletti, R.; Lazzara, R. Small-diameter implants: Indications and contraindications. J. Esthet. Restor. Dent. 2000, 12, 186–194. [Google Scholar] [CrossRef]
- Ghazal, S.; Huynh-Ba, G.; Aghaloo, T.; Dibart, S.; Froum, S.; O’Neal, R.; Cochran, D. Randomized Controlled Multicenter Clinical Study Evaluating Crestal Bone Level Change of Narrow-Diameter Versus Standard-Diameter Ti-Zr Implants for Single Tooth Replacement in Anterior and Premolar Region. Int. J. Oral Maxillofac. Implant. 2019, 34, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Roccuzzo, A.; Imber, J.; Lempert, J.; Hosseini, M.; Jensen, S.S. Narrow Diameter Implants to Replace Congenital Missing Maxillary Lateral Incisors: A 1-year Prospective, Controlled, Clinical Study. Clin. Oral Implant. Res. 2022, 33, 844–857. [Google Scholar] [CrossRef] [PubMed]
- Marcello-Machado, R.M.; Faot, F.; Schuster, A.J.; Nascimento, G.G.; Del Bel Cury, A.A. Mini-Implants and Narrow Diameter Implants as Mandibular Overdenture Retainers: A Systematic Review and Meta-Analysis of Clinical and Radiographic Outcomes. J. Oral Rehabil. 2018, 45, 161–183. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Piattelli, A.; Carinci, F. Clinical Outcome of Narrow Diameter Implants: A Retrospective Study of 510 Implants. J. Periodontol. 2008, 79, 49–54. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Piattelli, A. Immediate versus One-Stage Restoration of Small-Diameter Implants for a Single Missing Maxillary Lateral Incisor: A 3-Year Randomized Clinical Trial. J. Periodontol. 2009, 80, 1393–1398. [Google Scholar] [CrossRef]
- Oyama, K.; Kan, J.Y.K.; Rungcharassaeng, K.; Lozada, J. Immediate Provisionalization of 3.0-Mm-Diameter Implants Replacing Single Missing Maxillary and Mandibular Incisors: 1-Year Prospective Study. Int. J. Oral Maxillofac. Implants 2012, 27, 173–180. [Google Scholar]
- Bencharit, S.; Clark, W.A.; Stoner, L.O.; Chiang, G.; Sulaiman, T.A. Recent Advancements in CAD/CAM Same-Day Dentistry in Practice and Education. Preprints 2021. 2021110490. [Google Scholar]
- Blatz, M.B.; Conejo, J. The Current State of Chairside Digital Dentistry and Materials. Dent. Clin. N. Am. 2019, 63, 175–197. [Google Scholar] [CrossRef]
- Pelekanos, S. The Single Implant-Crown Complex in the Aesthetic Zone: Abutment Selection and the Treatment Sequencing. In Implant Aesthetics; Karateew, E., Ed.; Springer: Cham, Switzerland, 2017; pp. 301–336. [Google Scholar]
- Lambert, F.E.; Lecloux, G.; Grenade, C.; Bouhy, A.; Lamy, M.; Rompen, E.H. Less Invasive Surgical Procedures Using Narrow-Diameter Implants: A Prospective Study in 20 Consecutive Patients. J. Oral Implantol. 2015, 41, 693–699. [Google Scholar] [CrossRef]
- Froum, S.; Shi, Y.; Fisselier, F.; Cho, S.-C. Long-Term Retrospective Evaluation of Success of Narrow-Diameter Implants in Esthetic Areas: A Consecutive Case Series with 3 to 14 Years Follow-Up. Int. J. Periodontics Restor. Dent. 2017, 37, 629–637. [Google Scholar] [CrossRef]
- Block, M.S.; Mercante, D.E.; Lirette, D.; Mohamed, W.; Ryser, M.; Castellon, P. Prospective Evaluation of Immediate and Delayed Provisional Single Tooth Restorations. J. Oral Maxillofac. Surg. 2009, 67, 89–107. [Google Scholar] [CrossRef]
- Hagiwara, Y. Does Platform Switching Really Prevent Crestal Bone Loss around Implants? Jpn. Dent. Sci. Rev. 2010, 46, 122–131. [Google Scholar] [CrossRef]
- De Kok, I.J.; Chang, S.S.; Moriarty, J.D.; Cooper, L.F. A Retrospective Analysis of Peri-Implant Tissue Responses at Immediate Load/provisionalized Microthreaded Implants. Int. J. Oral Maxillofac. Implants 2006, 21, 405–412. [Google Scholar]
- Liu, Y.; Wang, J. Influences of Microgap and Micromotion of Implant–abutment Interface on Marginal Bone Loss around Implant Neck. Arch. Oral Biol. 2017, 83, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Pisoni, L.; Ordesi, P.; Siervo, P.; Bianchi, A.E.; Persia, M.; Siervo, S. Flapless Versus Traditional Dental Implant Surgery: Long-Term Evaluation of Crestal Bone Resorption. J. Oral Maxillofac. Surg. 2016, 74, 1354–1359. [Google Scholar] [CrossRef]
- Mishra, P.; Tandan, A.; Shivakumar, G.C.; Choudhary, K.; Shivakumar, S.; Sharma, N.; Saxena, A. Evaluation of Crestal Bone Loss in Flap vs Flapless Implant Placement Technique: An In Vivo Comparative Study. J. Contemp. Dent. Pract. 2022, 23, 56–60. [Google Scholar]
- Vohra, F.; Al-Kheraif, A.A.; Almas, K.; Javed, F. Comparison of crestal bone loss around dental implants placed in healed sites using flapped and flapless techniques: A systematic review. J. Periodontol. 2015, 86, 185–191. [Google Scholar] [CrossRef]
- Al-Juboori, M.J.; Bin Abdulrahaman, S.; Jassan, A. Comparison of Flapless and Conventional Flap and the Effect on Crestal Bone Resorption during a 12-Week Healing Period. Dent. Implantol. Update 2012, 23, 9–16. [Google Scholar]
- Tamimi, F.; Hirayama, H. Digital Restorative Dentistry: A Guide to Materials, Equipment, and Clinical Procedures; Springer: Berlin/Heidelberg, Germany, 2019; ISBN 9783030159740. [Google Scholar]
- Baroudi, K.; Ibraheem, S.N. Assessment of Chair-Side Computer-Aided Design and Computer-Aided Manufacturing Restorations: A Review of the Literature. J. Int. Oral. Health 2015, 7, 96–104. [Google Scholar]
- Turkyilmaz, I.; Wilkins, G.N.; Varvara, G. Tooth Preparation, Digital Design and Milling Process Considerations for CAD/CAM Crowns: Understanding the Transition from Analog to Digital Workflow. J. Dent. Sci. 2021, 16, 1312–1314. [Google Scholar] [CrossRef]
- Schepke, U.; Meijer, H.J.A.; Kerdijk, W.; Cune, M.S. Digital versus Analog Complete-Arch Impressions for Single-Unit Premolar Implant Crowns: Operating Time and Patient Preference. J. Prosthet. Dent. 2015, 114, 403–406.e1. [Google Scholar] [CrossRef] [PubMed]
- Sivaramakrishnan, G.; Alsobaiei, M.; Sridharan, K. Patient Preference and Operating Time for Digital versus Conventional Impressions: A Network Meta-analysis. Aust. Dent. J. 2020, 65, 58–69. [Google Scholar] [CrossRef]
- De Oliveira, N.R.C.; de Oliveira, N.R.C.; Pigozzo, M.N.; Sesma, N.; Laganá, D.C. Clinical Efficiency and Patient Preference of Digital and Conventional Workflow for Single Implant Crowns Using Immediate and Regular Digital Impression: A Meta-analysis. Clin. Oral Implant. Res. 2020, 31, 669–686. [Google Scholar] [CrossRef]
- Joda, T.; Brägger, U. Patient-Centered Outcomes Comparing Digital and Conventional Implant Impression Procedures: A Randomized Crossover Trial. Clin. Oral Implants Res. 2016, 27, e185–e189. [Google Scholar] [CrossRef]
- Joda, T.; Lenherr, P.; Dedem, P.; Kovaltschuk, I.; Bragger, U.; Zitzmann, N.U. Time Efficiency, Difficulty, and Operator’s Preference Comparing Digital and Conventional Implant Impressions: A Randomized Controlled Trial. Clin. Oral Implant. Res. 2017, 28, 1318–1323. [Google Scholar] [CrossRef]
- Joda, T.; Zarone, F.; Ferrari, M. The Complete Digital Workflow in Fixed Prosthodontics: A Systematic Review. BMC Oral. Health 2017, 17, 124. [Google Scholar] [CrossRef]
- Joda, T.; Gintaute, A.; Brägger, U.; Ferrari, M.; Weber, K.; Zitzmann, N.U. Time-Efficiency and Cost-Analysis Comparing Three Digital Workflows for Treatment with Monolithic Zirconia Implant Fixed Dental Prostheses: A Double-Blinded RCT. J. Dent. 2021, 113, 103779. [Google Scholar] [CrossRef]
- Kunavisarut, C.; Jarangkul, W.; Pornprasertsuk-Damrongsri, S.; Joda, T. Patient-Reported Outcome Measures (PROMs) Comparing Digital and Conventional Workflows for Treatment with Posterior Single-Unit Implant Restorations: A Randomized Controlled Trial. J. Dent. 2022, 117, 103875. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Arzukanyan, A.V.; Spagnuolo, G.; Cicciù, M. Dental Restorative Digital Workflow: Digital Smile Design from Aesthetic to Function. Dent. J. 2019, 7, 30. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Variable | Values | n * | % |
|---|---|---|---|
| Gender | Male | 3 | 30 |
| Female | 7 | 70 | |
| Ethnicity | Caucasian | 6 | 60 |
| African American | 4 | 40 | |
| Implant placement site | Maxillary lateral incisor | 5 | 45.5 |
| Maxillary canine | 1 | 9.1 | |
| Maxillary premolar | 4 | 3.6 | |
| Mandibular lateral incisor | 1 | 9.1 | |
| Implant length | 8.0 mm | 1 | 9.1 |
| 10.0 mm | 2 | 18.2 | |
| 11.5 mm | 6 | 54.5 | |
| 13.0 mm | 2 | 18.2 |
| Time Period | Tooth Surface | Change (mm) |
|---|---|---|
| Between 3–6 months | mesial | 0.43 ± 0.5 |
| distal | −0.14 ± 1.07 | |
| buccal | 0 | |
| lingual | 0.29 ± 0.95 | |
| Between 6 months and 1 year | mesial | 0.13 ± 0.99 |
| distal | 0.25 ± 0.71 | |
| buccal | −0.44 ± 1.05 | |
| lingual | 0.25 ± 0.89 | |
| Between 1 year and 2 years | mesial | 0.25 ± 0.50 |
| distal | 0.50 ± 0.58 | |
| buccal | −0.25 ± 0.5 | |
| lingual | 0 |
| Clinical Measures | GI | BOP | MGI * | PI * |
|---|---|---|---|---|
| 1 week | 0.67 ± 0.52 | 0.20 ± 0.40 | N/A | N/A |
| 3 weeks | 0.25 ± 0.44 | 0 | N/A | N/A |
| Prosthetic insertion | 0.10 ± 0.30 | 0 | 0.17 ± 0.41 | 0.17 ± 0.41 |
| 6 months | 0.14 ± 0.38 | 0 | 0.17 ± 0.41 | 0 |
| 12 months | 0.13 ± 0.35 | 0 | 0.29 ± 0.49 | 0 |
| 24 months | 0 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deeb, J.G.; Reddy, N.G.; Hopfensperger, L.J.; Harris, A.L.; Bencharit, S. Same-Day Digital Dentistry Restorative Workflow for Single Immediate Provisionalization of Narrow-Diameter Implants: An Exploratory Prospective Study. Prosthesis 2023, 5, 197-207. https://doi.org/10.3390/prosthesis5010015
Deeb JG, Reddy NG, Hopfensperger LJ, Harris AL, Bencharit S. Same-Day Digital Dentistry Restorative Workflow for Single Immediate Provisionalization of Narrow-Diameter Implants: An Exploratory Prospective Study. Prosthesis. 2023; 5(1):197-207. https://doi.org/10.3390/prosthesis5010015
Chicago/Turabian StyleDeeb, Janina Golob, Nitya G. Reddy, Liam J. Hopfensperger, April L. Harris, and Sompop Bencharit. 2023. "Same-Day Digital Dentistry Restorative Workflow for Single Immediate Provisionalization of Narrow-Diameter Implants: An Exploratory Prospective Study" Prosthesis 5, no. 1: 197-207. https://doi.org/10.3390/prosthesis5010015