
Decellularized Porcine Pericardium Enhances Autologous Vascularized Matrix as a Prosthesis for Left Ventricular Full-Wall Myocardial Reconstruction

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Decellularization of Pericardium
2.2. Animal Experiment
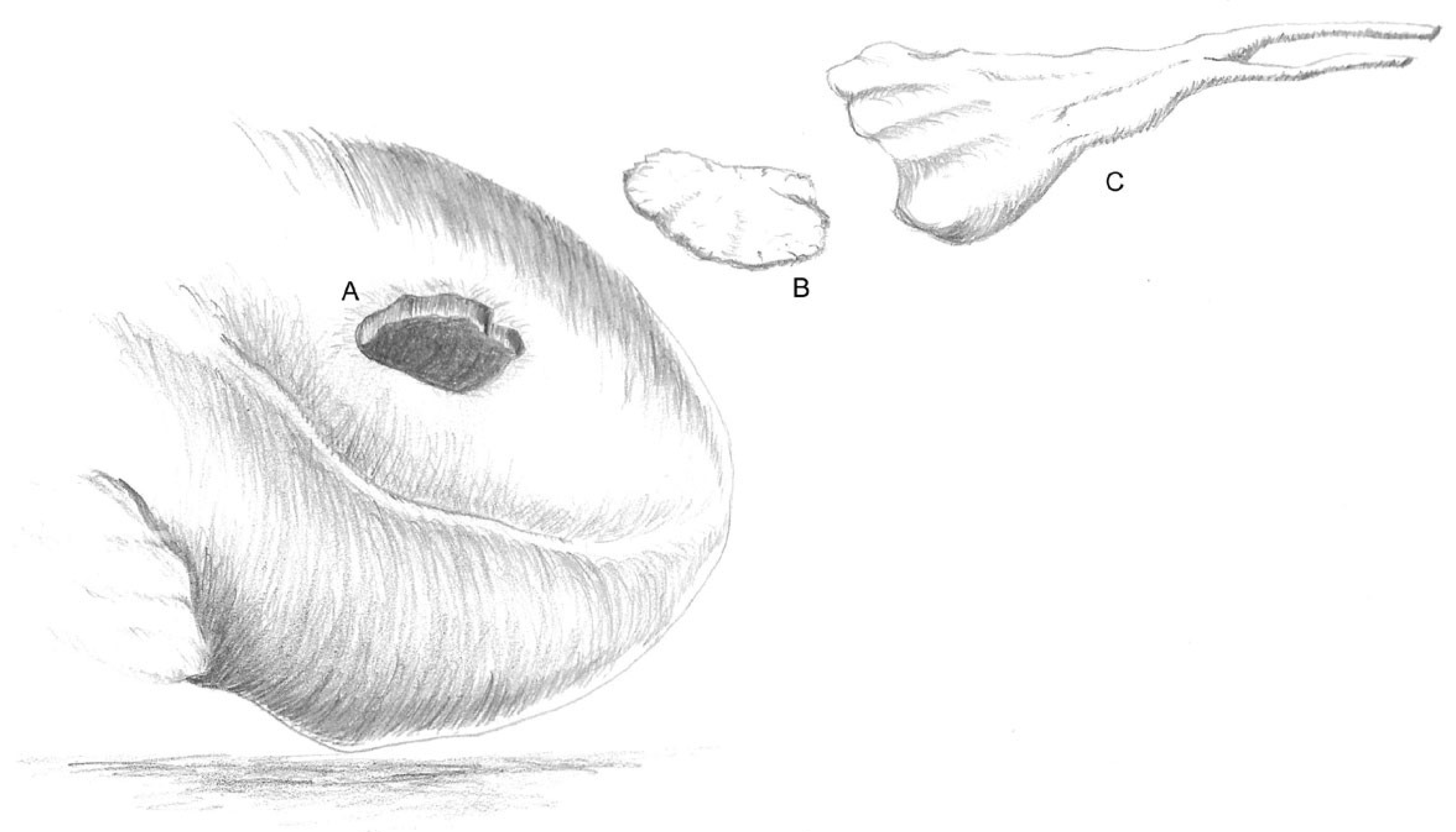
2.3. Implantation
2.4. Cardiac Magnetic Resonance Imaging (MRI)
2.5. Explantation
2.6. Preparation for Histological Examination
2.6.1. Light Microscopy of the Decellularized Pericardium
2.6.2. Scanning Electron Microscopy of the Decellularized Pericardium
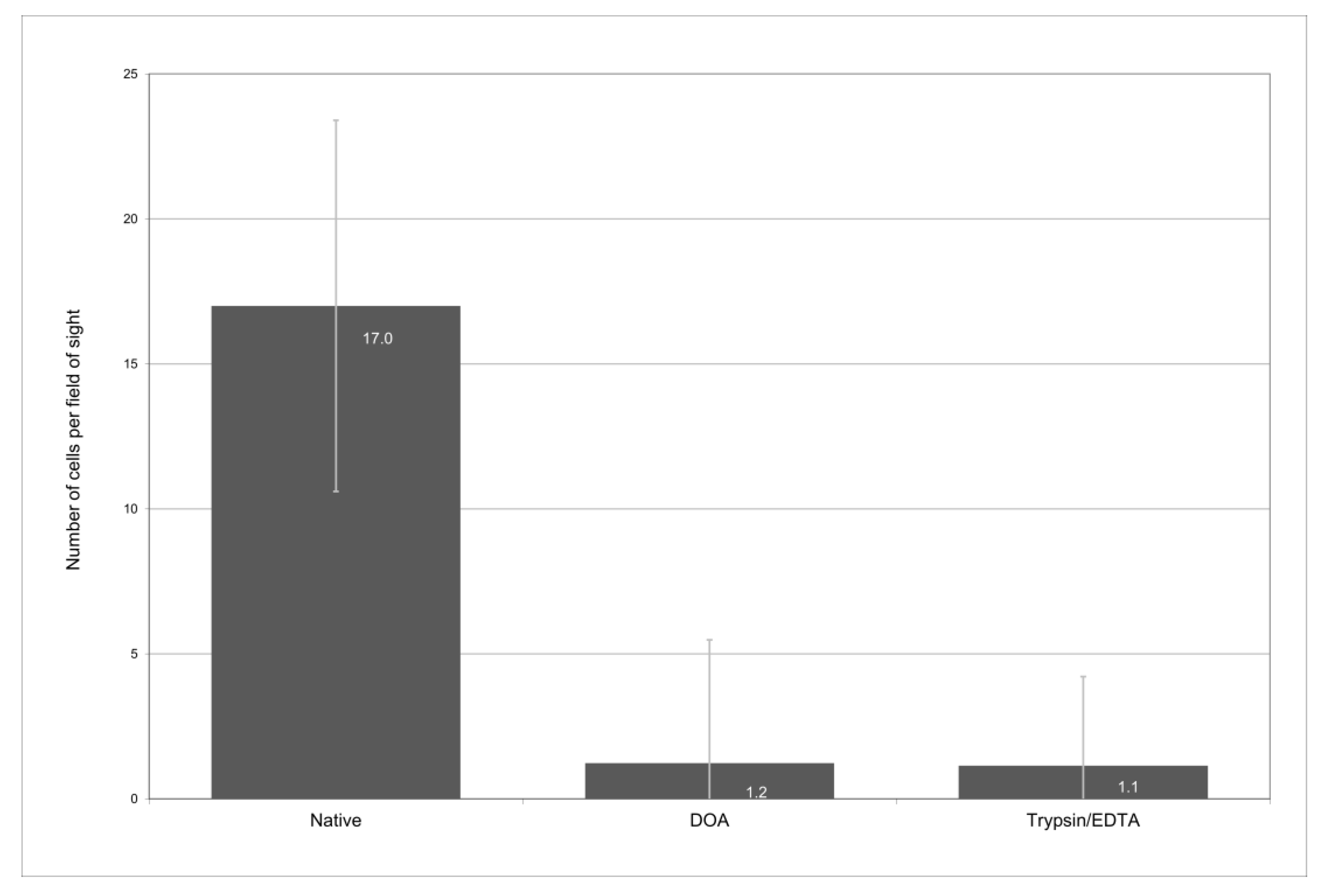
2.6.3. Biometric Assessment of the Cell Density and Collagen Architecture of the Decellularized Pericardium
2.6.4. Overview of the Staining and Immunohistochemistry of the Explants
2.7. Statistical Analysis
3. Results
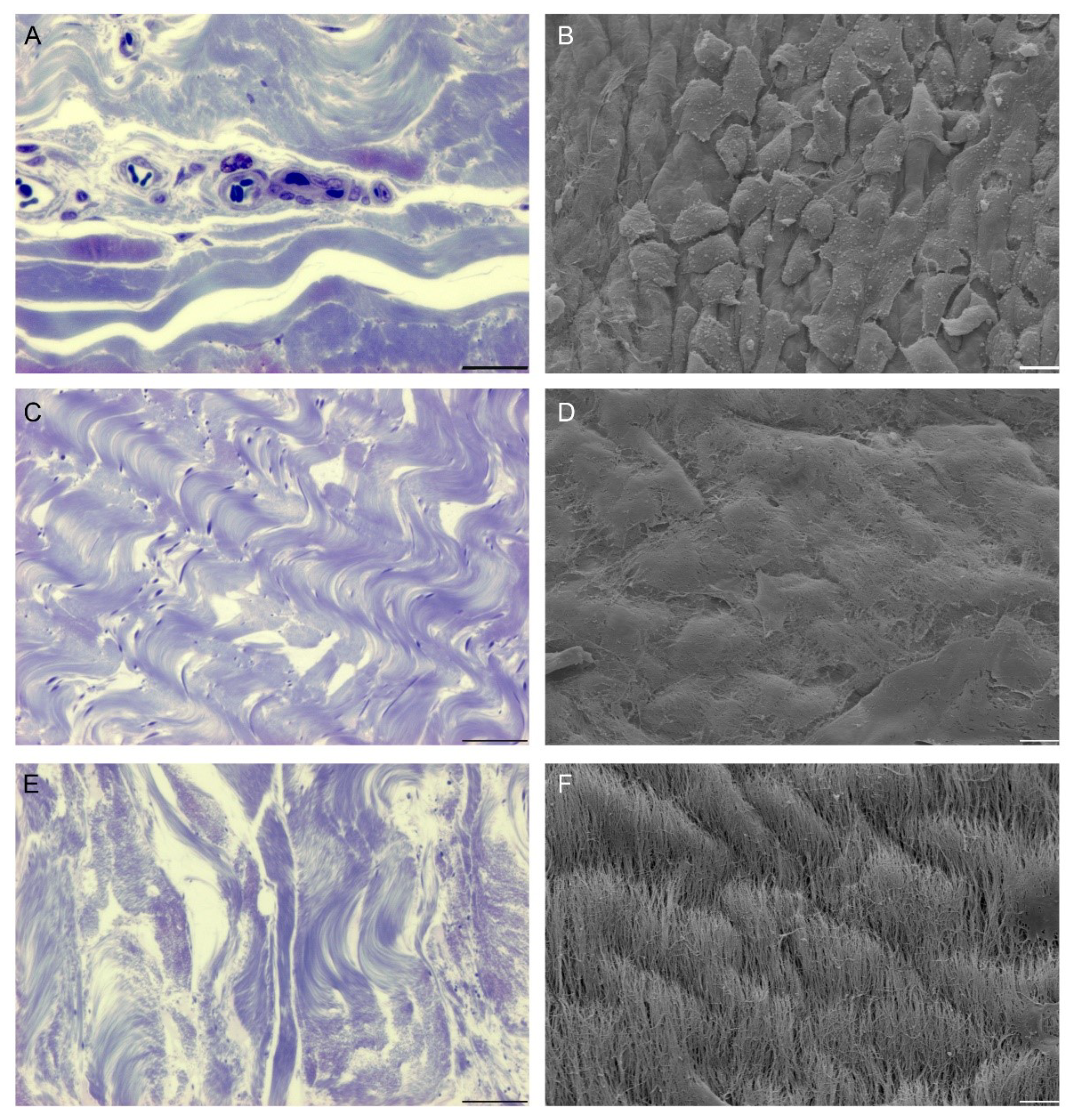
3.1. Decellularization of Pericardium
3.1.1. Native Pericardium
3.1.2. Pericardium following Decellularization Procedures
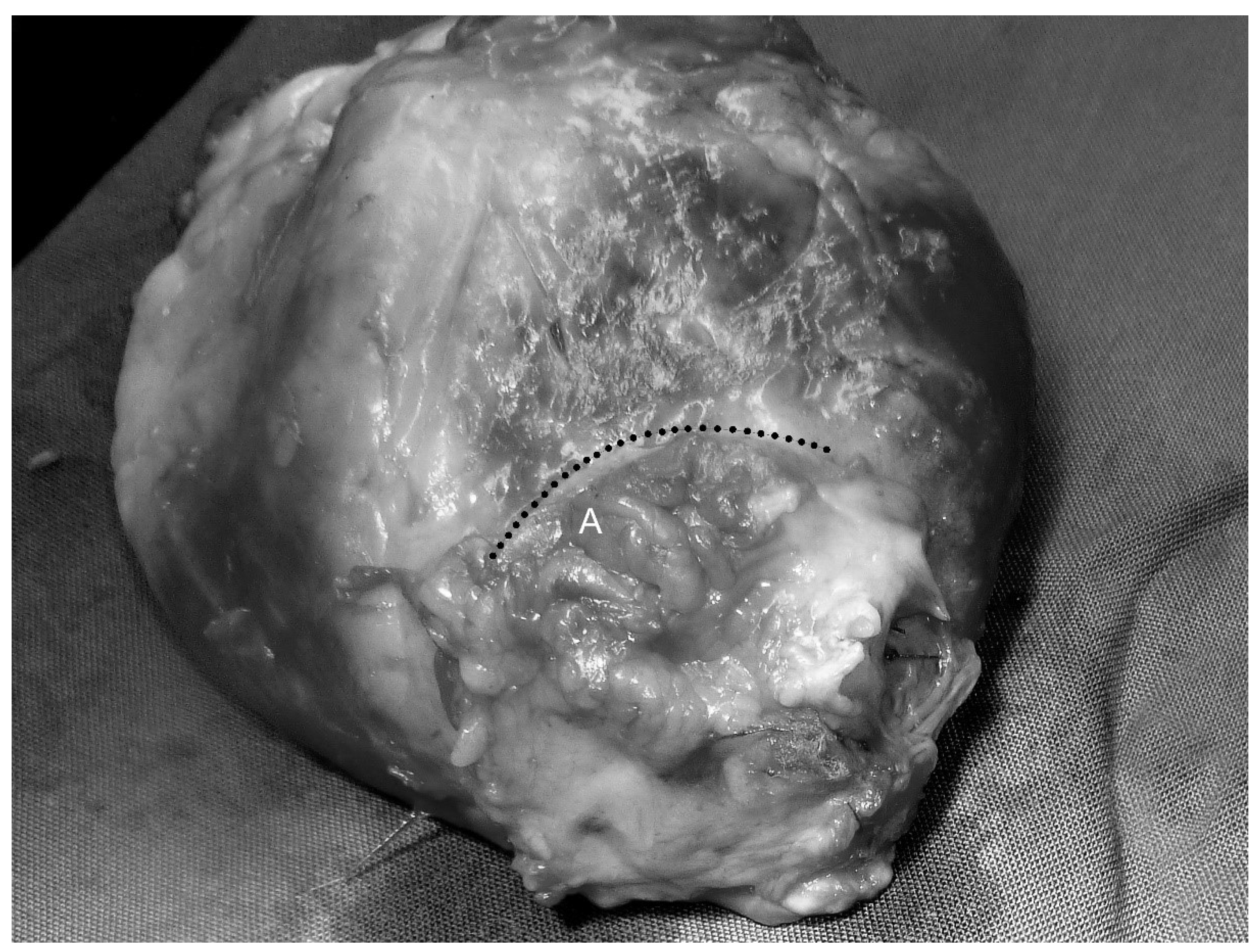
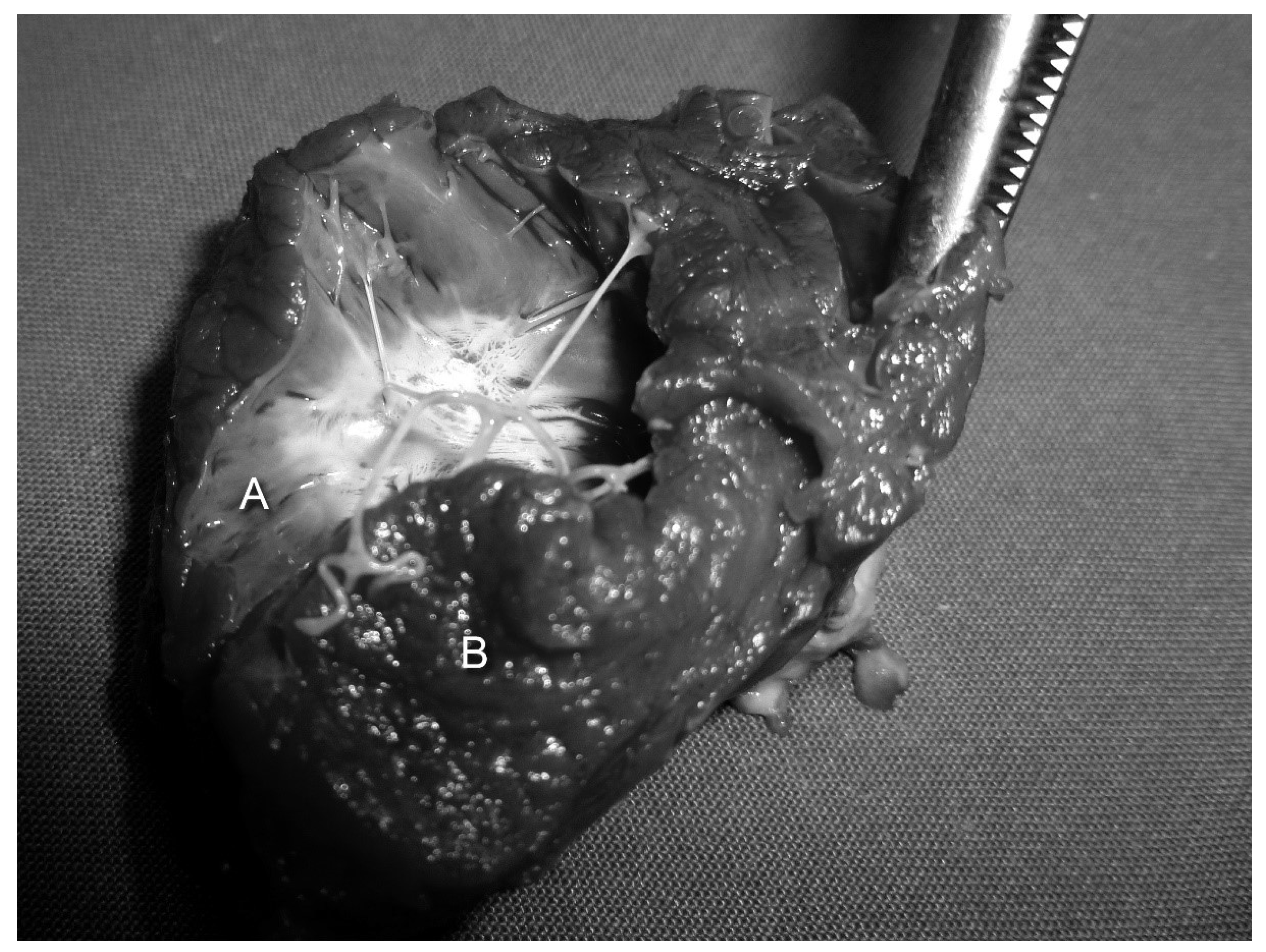
3.2. Clinical Results and Macroscopic Findings
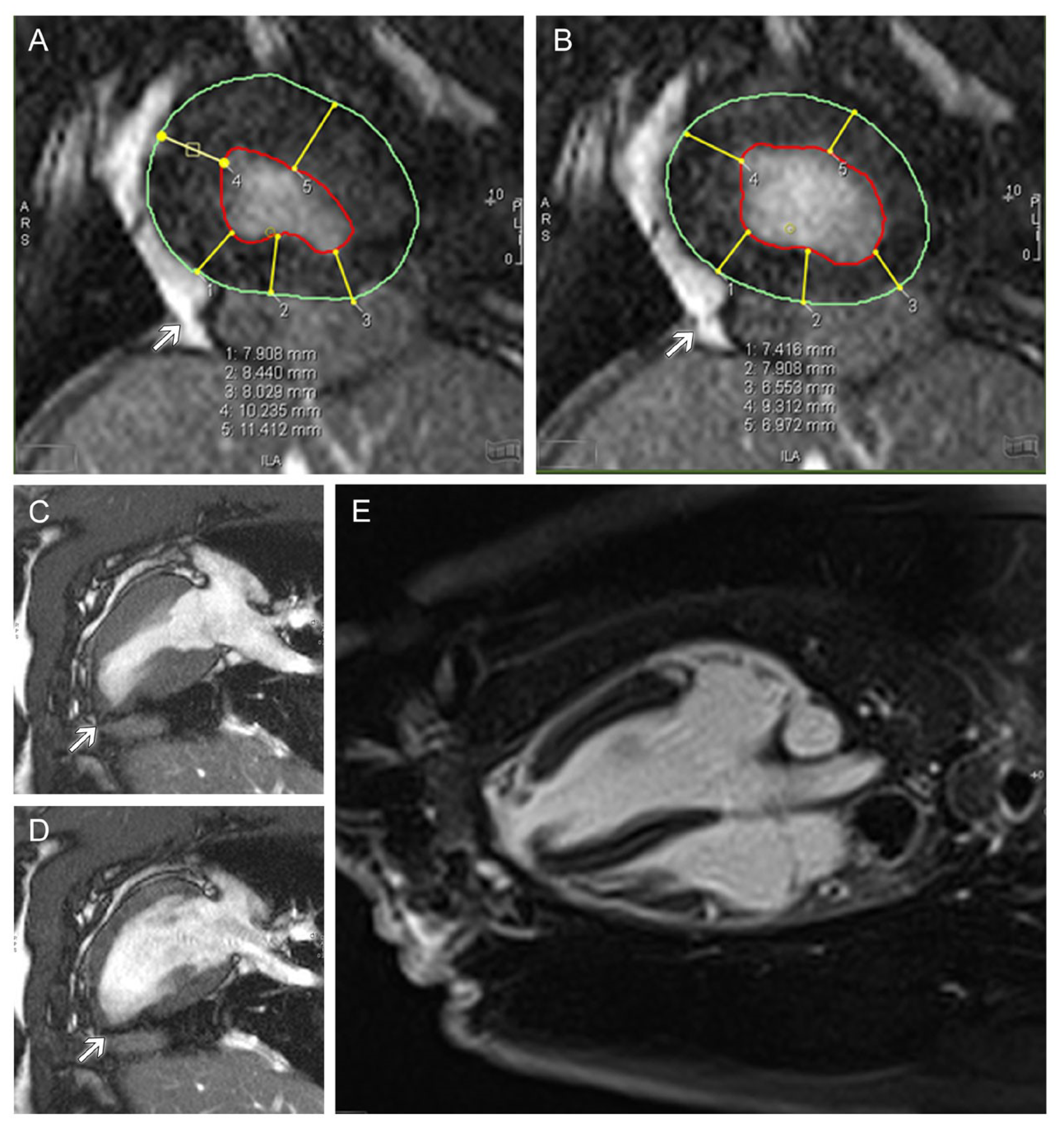
3.3. MRI
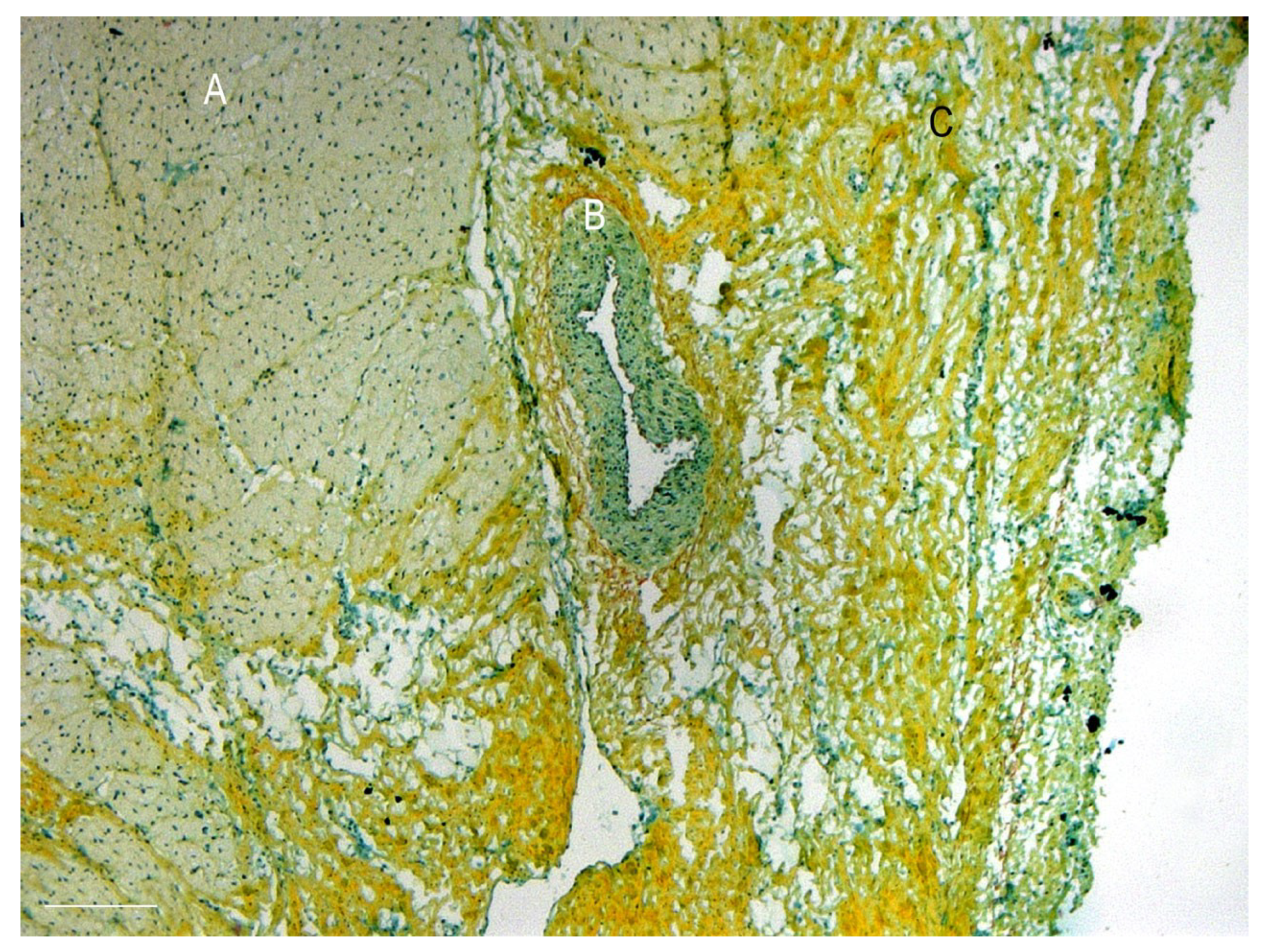
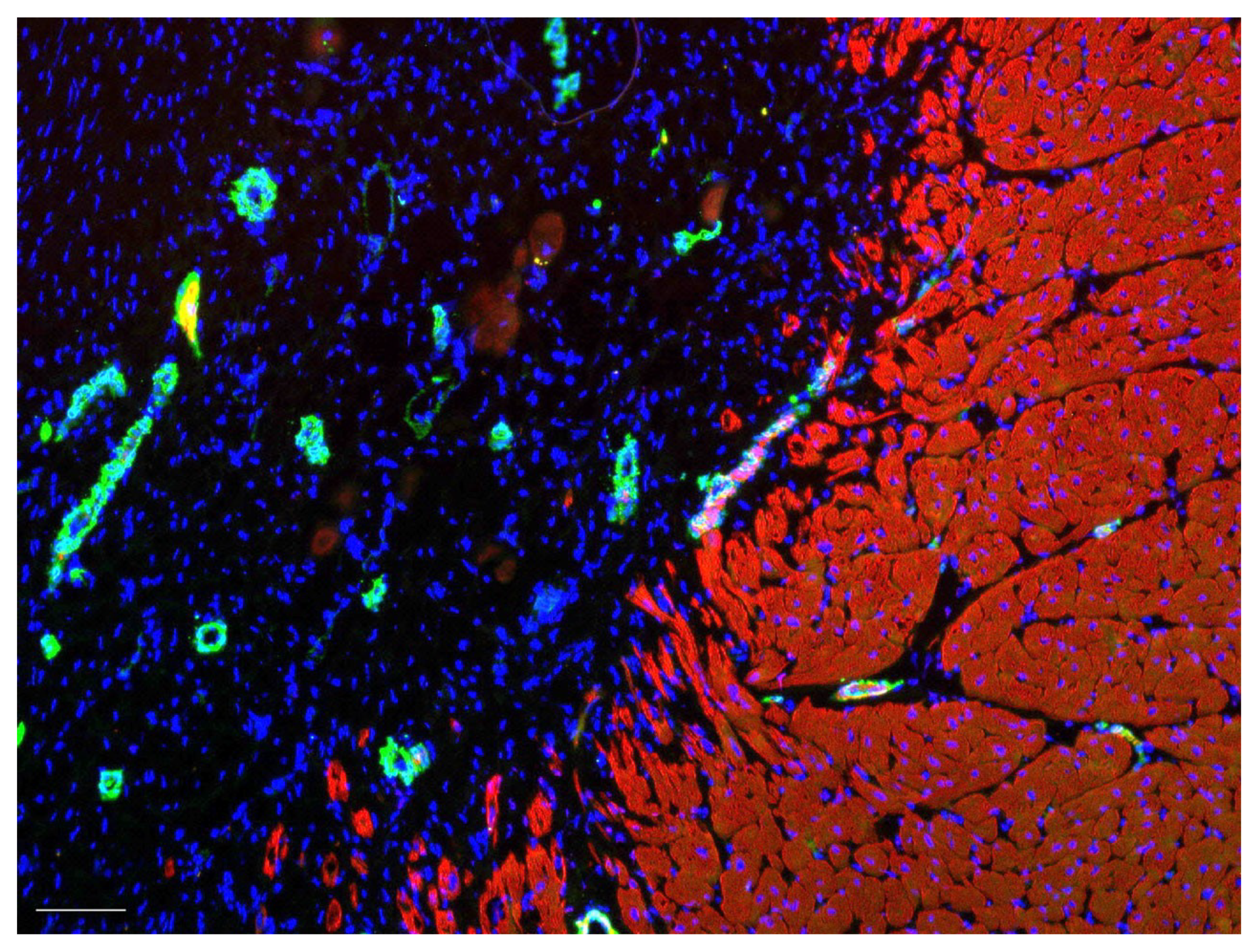
3.4. Histology and Immunohistochemistry of the Explanted Grafts and Myocardium
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Groenewegen, A.; Rutten, F.H.; Mosterd, A.; Hoes, A.W. Epidemiology of heart failure. Eur. J. Heart Fail. 2020, 22, 1342–1356. [Google Scholar] [CrossRef] [PubMed]
- Dor, V.; Saab, M.; Coste, P.; Kornaszewska, M.; Montiglio, F. Left ventricular aneurysm: A new surgical approach. Thorac. Cardiovasc. Surg. 1989, 37, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Buckberg, G.D. Form versus disease: Optimizing geometry during ventricular restoration. Eur.J.Cardiothorac. Surg. 2006, 29 (Suppl. 1), S238–S244. [Google Scholar] [CrossRef]
- David, T.E. The use of pericardium in acquired heart disease: A review article. J. Heart Valve Dis. 1998, 7, 13–18. [Google Scholar]
- David, T.E.; Feindel, C.M.; Ropchan, G.V. Reconstruction of the left ventricle with autologous pericardium. J. Thorac. Cardiovasc. Surg. 1987, 94, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Schilling, T.; Cebotari, S.; Tudorache, I.; Haverich, A. [Tissue engineering of vascularized myocardial prosthetic tissue. Biological and solid matrices]. Chirurg 2011, 82, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Tudorache, I.; Kostin, S.; Meyer, T.; Teebken, O.; Bara, C.; Hilfiker, A.; Haverich, A.; Cebotari, S. Viable vascularized autologous patch for transmural myocardial reconstruction. Eur. J. Cardiothorac. Surg. 2009, 36, 306–311. [Google Scholar] [CrossRef]
- Ruel, M.A.; Sellke, F.W.; Bianchi, C.; Khan, T.A.; Faro, R.; Zhang, J.P.; Cohn, W.E. Endogenous myocardial angiogenesis and revascularization using a gastric submucosal patch. Ann. Thorac. Surg. 2003, 75, 1443–1449. [Google Scholar] [CrossRef]
- Badylak, S.F.; Kochupura, P.V.; Cohen, I.S.; Doronin, S.V.; Saltman, A.E.; Gilbert, T.W.; Kelly, D.J.; Ignotz, R.A.; Gaudette, G.R. The use of extracellular matrix as an inductive scaffold for the partial replacement of functional myocardium. Cell Transplant. 2006, 15, S29–S40. [Google Scholar] [CrossRef]
- Wei, H.J.; Chen, S.C.; Chang, Y.; Hwang, S.M.; Lin, W.W.; Lai, P.H.; Chiang, H.H.K.; Hsu, L.F.; Yang, H.H.; Sung, H.W. Porous acellular bovine pericardia seeded with mesenchymal stem cells as a patch to repair a myocardial defect in a syngeneic rat model. Biomaterials 2006, 27, 5409–5419. [Google Scholar] [CrossRef]
- Hubbell, J.A. Matrix Effects. In Principles of Tissue Engineering; Langer, R., Vacanti, J.P., Eds.; Academic Press: San Diego, London, 2000; pp. 237–250. [Google Scholar]
- Meredith, J.E., Jr.; Fazeli, B.; Schwartz, M.A. The extracellular matrix as a cell survival factor. Mol Biol Cell 1993, 4, 953–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cebotari, S.; Mertsching, H.; Kallenbach, K.; Kostin, S.; Repin, O.; Batrinac, A.; Kleczka, C.; Ciubotaru, A.; Haverich, A. Construction of autologous human heart valves based on an acellular allograft matrix. Circulation 2002, 106, I63–I68. [Google Scholar] [CrossRef] [PubMed]
- Cebotari, S.; Tudorache, I.; Jaekel, T.; Hilfiker, A.; Dorfman, S.; Ternes, W.; Haverich, A.; Lichtenberg, A. Detergent decellularization of heart valves for tissue engineering: Toxicological effects of residual detergents on human endothelial cells. Artif Organs 2010, 34, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Heine, J.; Schmiedl, A.; Cebotari, S.; Karck, M.; Mertsching, H.; Haverich, A.; Kallenbach, K. Tissue engineering human small-caliber autologous vessels using a xenogenous decellularized connective tissue matrix approach: Preclinical comparative biomechanical studies. Artif. Organs 2011, 35, 930–940. [Google Scholar] [CrossRef]
- Lichtenberg, A.; Tudorache, I.; Cebotari, S.; Ringes-Lichtenberg, S.; Sturz, G.; Hoeffler, K.; Hurscheler, C.; Brandes, G.; Hilfiker, A.; Haverich, A. In vitro re-endothelialization of detergent decellularized heart valves under simulated physiological dynamic conditions. Biomaterials 2006, 27, 4221–4229. [Google Scholar] [CrossRef]
- Velivassis, M. Vergleichende Morphologische Analyse von Bovinem und Porcinem Perikard nach Dezellularisierung mit Natrium-Desoxycholat und Trypsin. Medizinische Hochschule Hannover: Hannover, Germany, 2006. [Google Scholar]
- Calafiore, A.M.; Iaco, A.L.; Abukoudair, W.; Penco, M.; Di, M.M. Left ventricular surgical remodeling after the STICH trial. Thorac. Cardiovasc. Surg. 2011, 59, 195–200. [Google Scholar] [CrossRef]
- Esmaeili, H.; Patino-Guerrero, A.; Hasany, M.; Ansari, M.O.; Memic, A.; Dolatshahi-Pirouz, A.; Nikkhah, M. Electroconductive biomaterials for cardiac tissue engineering. Acta Biomater. 2022, 139, 118–140. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, L.; Li, T.; Liu, S.; Guo, B.; Huang, W.; Wu, Y. 3D bioprinting in cardiac tissue engineering. Theranostics 2021, 11, 7948–7969. [Google Scholar] [CrossRef]
- Wang, Z.; Lee, S.J.; Cheng, H.J.; Yoo, J.J.; Atala, A. 3D bioprinted functional and contractile cardiac tissue constructs. Acta Biomater. 2018, 70, 48–56. [Google Scholar] [CrossRef]
- McCready, R.A.; Kiell, C.S.; Chugh, A.R.; Rapp, B.M.; Webb, T.H.; Barksdale, A.; Parikshak, M.; Gerdisch, M.W. Long-term Results With CorMatrix Extracellular Matrix Patches After Carotid Endarterectomy. J. Surg. Res. 2021, 262, 21–26. [Google Scholar] [CrossRef]
- Zivkovic, I.; Mihajlovic, V.; Zdravkovic, D.; Krstic, D.; Krasic, S.; Lesanovic, J.; Peric, M.; Milacic, P. Surgical Reconstruction of a Left Ventricular Aneurysm Using an Extracellular Matrix Patch. Braz. J. Cardiovasc. Surg. 2022, 37, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Neethling, W.M.; Cooper, S.; Van Den Heever, J.J.; Hough, J.; Hodge, A.J. Evaluation of kangaroo pericardium as an alternative substitute for reconstructive cardiac surgery. J.Cardiovasc. Surg. 2002, 43, 301–306. [Google Scholar]
- Fentie, I.H.; Allen, D.J.; Schenck, M.H.; Didio, L.J. Comparative electron microscopic study of bovine, porcine and human parietal pericardium, as materials for cardiac valve bioprostheses. J. Submicrosc. Cytol. 1986, 18, 53–65. [Google Scholar] [PubMed]
- Garcia Paez, J.M.; Carrera, A.; Herrero, E.J.; Millan, I.; Rocha, A.; Cordon, A.; Sainz, N.; Mendez, J.; Castillo-Olivares, J.L. Influence of the selection of the suture material on the mechanical behavior of a biomaterial to be employed in the construction of implants. Part 2: Porcine pericardium. J. Biomater. Appl. 2001, 16, 68–90. [Google Scholar] [CrossRef] [PubMed]
- Crapo, P.M.; Gilbert, T.W.; Badylak, S.F. An overview of tissue and whole organ decellularization processes. Biomaterials 2011, 32, 3233–3243. [Google Scholar] [CrossRef]
- Dohmen, P.M.; da Costa, F.; Lopes, S.V.; Vilani, R.; Bloch, O.; Konertz, W. Successful implantation of a decellularized equine pericardial patch into the systemic circulation. Med. Sci. Monit. Basic Res. 2014, 20, 1–8. [Google Scholar] [CrossRef]
- Cebotari, S.; Lichtenberg, A.; Tudorache, I.; Hilfiker, A.; Mertsching, H.; Leyh, R.; Breymann, T.; Kallenbach, K.; Maniuc, L.; Batrinac, A.; et al. Clinical application of tissue engineered human heart valves using autologous progenitor cells. Circulation 2006, 114, I132–I137. [Google Scholar] [CrossRef]
- Schilling, T.; Meyer, T.; Brandes, G.; Hartung, D.; Tudorache, I.; Nolte, I.; Wacker, F.; Hilfiker, A.; Hoeffler, K.; Haverich, A.; et al. Left Ventricular Wall Reconstruction with Autologous Vascularized Gastric Graft in a Porcine Pilot Model. Eur. Surg. Res. 2022. [Google Scholar] [CrossRef]
- Huang, W.; Zhang, D.S.; Millard, R.W.; Wang, T.; Zhao, T.M.; Fan, G.C.; Ashraf, A.; Xu, M.F.; Ashraf, M.; Wang, Y.G. Gene manipulated peritoneal cell patch repairs infarcted myocardium. J. Mol. Cell. Cardiol. 2010, 48, 702–712. [Google Scholar] [CrossRef]
- Tan, M.Y.; Zhi, W.; Wei, R.Q.; Huang, Y.C.; Zhou, K.P.; Tan, B.; Deng, L.; Luo, J.C.; Li, X.Q.; Xie, H.Q.; et al. Repair of infarcted myocardium using mesenchymal stem cell seeded small intestinal submucosa in rabbits. Biomaterials 2009, 30, 3234–3240. [Google Scholar] [CrossRef]
- Taheri, S.A.; Yeh, J.; Batt, R.E.; Fang, Y.; Ashraf, H.; Heffner, R.; Nemes, B.; Naughton, J. Uterine myometrium as a cell patch as an alternative graft for transplantation to infarcted cardiac myocardium: A preliminary study. Int. J. Artif. Organs 2008, 31, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Taheri, S.A.; Ashraf, H.; Merhige, M.; Miletich, R.S.; Satchidanand, S.; Malik, C.; Naughton, J.; Zhao, Q. Myoangiogenesis after cell patch cardiomyoplasty and omentopexy in a patient with ischemic cardiomyopathy. Tex. Heart Inst. J. 2005, 32, 598–601. [Google Scholar] [PubMed]
- Kusaba, E.; Schraut, W.; Sawatani, S.; Jaron, D.; Freed, P.; Kantrowitz, A. A diaphragmatic graft for augmenting left ventricular function: A feasibility study. Trans. Am. Soc. Artif. Intern. Organs 1973, 19, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Beck, C.S. The development of a new blood supply to the heart by operation. Ann.Surg. 1935, 102, 801–813. [Google Scholar] [CrossRef]
- Broughton, K.M.; Sussman, M.A. Cardiac tissue engineering therapeutic products to enhance myocardial contractility. J. Muscle Res. Cell Motil. 2020, 41, 363–373. [Google Scholar] [CrossRef]
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE guidelines 2.0: Updated guidelines for reporting animal research. BMJ Open Sci. 2020, 4, e100115. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Characterization | Collagen | Decellularization |
|---|---|---|---|
| Native |
|
| n.a. |
| DOA |
|
|
|
| Trypsin/EDTA |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, T.; Cebotari, S.; Brandes, G.; Hartung, D.; Wacker, F.; Theis, M.; Kaufeld, T.; Tudorache, I.; Nolte, I.; Haverich, A.; et al. Decellularized Porcine Pericardium Enhances Autologous Vascularized Matrix as a Prosthesis for Left Ventricular Full-Wall Myocardial Reconstruction. Prosthesis 2023, 5, 113-129. https://doi.org/10.3390/prosthesis5010010
Meyer T, Cebotari S, Brandes G, Hartung D, Wacker F, Theis M, Kaufeld T, Tudorache I, Nolte I, Haverich A, et al. Decellularized Porcine Pericardium Enhances Autologous Vascularized Matrix as a Prosthesis for Left Ventricular Full-Wall Myocardial Reconstruction. Prosthesis. 2023; 5(1):113-129. https://doi.org/10.3390/prosthesis5010010
Chicago/Turabian StyleMeyer, Tanja, Serghei Cebotari, Gudrun Brandes, Dagmar Hartung, Frank Wacker, Monika Theis, Tim Kaufeld, Igor Tudorache, Ingo Nolte, Axel Haverich, and et al. 2023. "Decellularized Porcine Pericardium Enhances Autologous Vascularized Matrix as a Prosthesis for Left Ventricular Full-Wall Myocardial Reconstruction" Prosthesis 5, no. 1: 113-129. https://doi.org/10.3390/prosthesis5010010