
Urinary Tract Infections in Patients Hospitalized in a Gastroenterology Department—Study from a Tertiary Regional Hospital in South-East Poland


Abstract
:1. Introduction
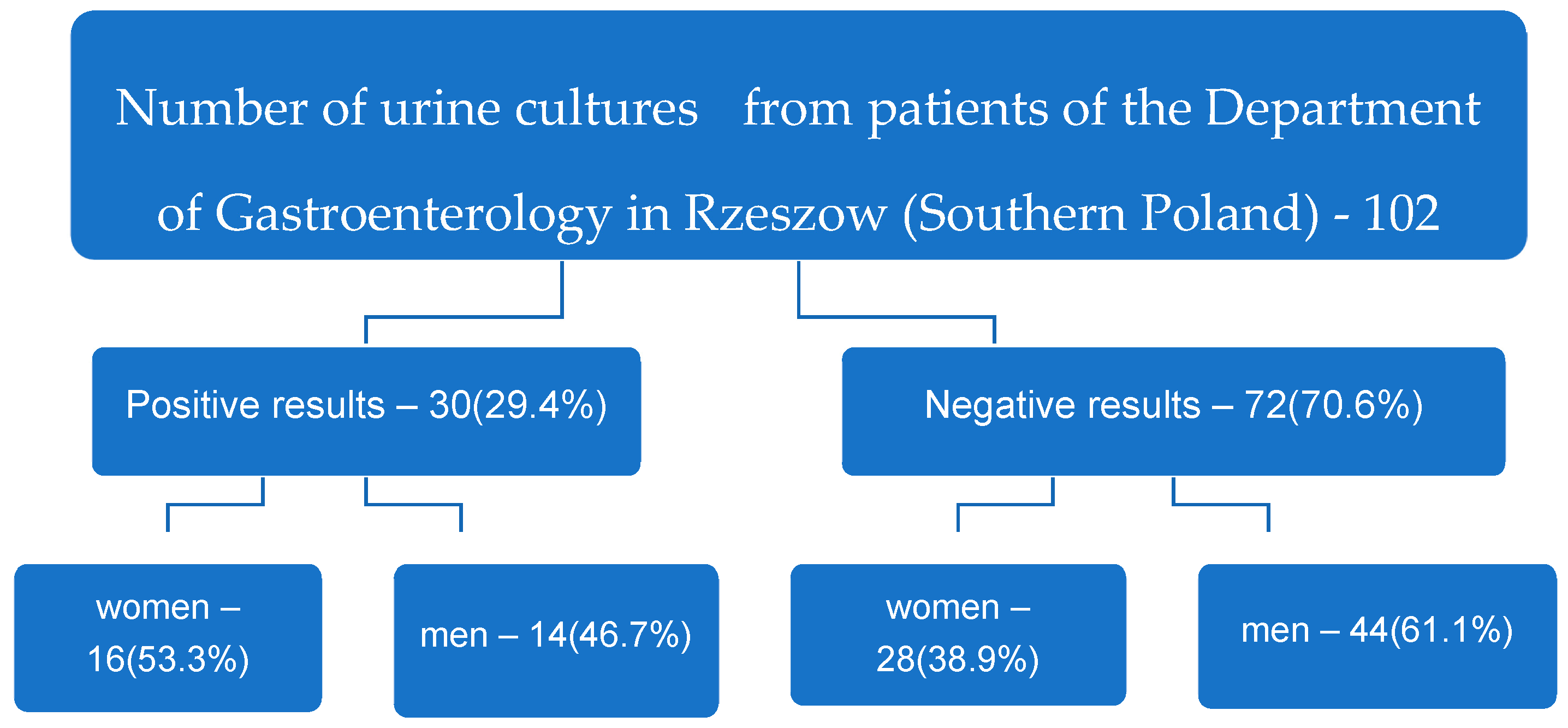
2. Results
3. Discussion
4. Materials and Methods
Ethics Statement
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zilberberg, M.D.; Shorr, A.F. Secular trends in gram-negative resistance among urinary tract infection hospitalizations in the United States, 2000–2009. Infect Control Hosp. Epidemiol. 2013, 34, 940–946. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, C.; Das-Mondal, M.; Gupta, D.; Sarkar, A.K.; Kar-Purkayastha, S.; Konar, A. Infection in cirrhosis: A prospective study. Ann. Hepatol. 2019, 18, 862–868. [Google Scholar] [CrossRef]
- Cohn, E.B.; Schaeffer, A.J. Urinary Tract Infections in Adults. Sci. World J. 2004, 4, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Hughes, T.; Juliebø-Jones, P.; Saada, L.; Saeed, K.; Somani, B.K. Recurrent urinary tract infections in adults: A practical guide. Br. J. Hosp. Med. 2021, 82, 1–11. [Google Scholar] [CrossRef]
- Ofek, I.; Beachey, E.H. General concepts and principles of bacterial adherence in animals and man, receptors and recognition. In Bacterial Adherence; Beachey, E.H., Ed.; Chapman and Hall: London, UK, 1980; pp. 3–29. [Google Scholar]
- Bonkat, G.; Cai, T.; Veeratterapillay, R.; Bruyère, F.; Bartoletti, R.; Pilatz, A.; Köves, B.; Geerlings, S.E.; Pradere, B.; Pickard, R.; et al. Management of Urosepsis in 2018. Eur. Urol. Focus 2019, 5, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Mazzariol, A.; Bazaj, A.; Cornaglia, G. Multi-drug-resistant Gram-negative bacteria causing urinary tract infections: A review. J. Chemother. 2017, 29, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Tandogdu, Z.; Wagenlehner, F.M. Global epidemiology of urinary tract infections. Curr. Opin. Infect. Dis. 2016, 29, 73–79. [Google Scholar] [CrossRef]
- Czajkowski, K.; Broś-Konopielko, M.; Teliga-Czajkowska, J. Urinary tract infection in women. Menopause Rev. 2021, 20, 40–47. [Google Scholar] [CrossRef]
- Ukashi, O.; Barash, Y.; Klang, E.; Zilberman, T.; Ungar, B.; Kopylov, U.; Ben-Horin, S.; Veisman, I. Adverse Clinical Outcomes among Inflammatory Bowel Disease Patients Treated for Urinary Tract Infection. J. Clin. Med. 2022, 11, 1359. [Google Scholar] [CrossRef]
- Kim, Y.N.; Jung, Y. Renal and Urinary Manifestations of Inflammatory Bowel Disease. Korean J. Gastroenterol. 2019, 73, 260–268. [Google Scholar] [CrossRef]
- Herbert, J.; Teeter, E.; Burstiner, L.S.; Doka, R.; Royer, A.; Owings, A.H.; Liu, J.; Glover, S.C.; Hosseini-Carroll, P. Urinary manifestations in African American and Caucasian infammatory bowel disease patients: A retrospective cohort study. BMC Urology. 2022, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, B.; Fasugba, O.; Beckingham, W.; Bennett, N.; Gardner, A. A point prevalence study of healthcare associated urinary tract infections in Australian acute and aged care facilities. Infect. Dis. Health 2016, 21, 26–31. [Google Scholar] [CrossRef]
- Dzierżanowska, D. Zakażenia układu moczowo-płciowego. In Antybiotykoterapia Praktyczna, 6th ed.; Alfa-Medica Press: Bielsko Biała, Poland, 2018; pp. 633–664. [Google Scholar]
- Escherich, T. Die darmbakterien des neugeborenen und säuglings. Fortschr. Med. 1885, 3, 515–522, 547–554. [Google Scholar]
- Pappelbaum, K.; Kasprzak, J.; Czaczyk, K. Występowanie werotoksycznych Escherichia coli w żywności, ze szczególnym uwzględnieniem serotypu O104:H4. Żywność. Nauka. Technologia. Jakość. 2015, 5, 33–48. [Google Scholar]
- Mazur, E.; Chmiel, M.J. Piaskownice jako potencjalne źródło zagrożenia lekoopornymi szczepami Escherichia coli oraz Staphylococcus aureus. Postępy Mikrobiol.-Adv. Microbiol. 2021, 60, 77–89. [Google Scholar] [CrossRef]
- Kim, K.S. Human meningitis-associated Escherichia coli. EcoSal Plus 2016, 7, 1–20. [Google Scholar] [CrossRef]
- Maslikowska, J.A.; Walker, S.A.N.; Elligsen, M.; Palmay, L.; Daneman, N.; Simor, A. Impact of infection with extended-spectrum β-lactamase-producing Escherichia coli or Klebsiella species on outcome and hospitalization costs. J. Hosp. Infect. 2016, 92, 33–41. [Google Scholar] [CrossRef]
- Korsak, D.; Popowska, M. Oporność bakterii na antybiotyki. In Antybiotyki w Dobie Narastającej Lekooporności; Markiewicz, Z., Korsak, D., Popowska, M., Eds.; Wydawnictwo Naukowe PWN: Warsaw, Poland, 2021; pp. 187–337. [Google Scholar]
- Bush, K.; Bradford, P.A. β-Lactams and β-Lactamase Inhibitors: An Overview. Cold Spring Harb. Perspect. Med. 2016, 6, a025247. [Google Scholar] [CrossRef]
- Dzierżanowska-Fangrat, K. Zakażenia układu moczowo-płciowego. In Przewodnik Antybiotykoterapii, 26th ed.; Alfa-Medica Press: Bielsko Biała, Poland, 2021; pp. 60–79. [Google Scholar]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Multistate point-prevalence survey of healthcare-associated infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef]
- Bushman, W.; Le, B.V. Nawracające zakażenia dróg moczowych po menopauzie. Ginekologia po Dyplomie. 2017, 1, 47–49. [Google Scholar]
- Bajaj, J.S.; O’Leary, J.G.; Reddy, K.R.; Wong, F.; Olson, J.C.; Subramanian, R.M.; Brown, G.; Noble, N.A.; Thacker, L.R.; Kamath, P.S. Second Infections Independently increase mortality in hospitalized patients with cirrhosis: The North American Consortium for the study of end stage liver disease (NACSELD) experience. Hepatology 2012, 56, 2328–2335. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.; Acevedo, J.; Castro, M.; Garcia, O.; de Lope, C.R.; Roca, D.; Pavesi, M.; Sola, E.; Moreira, L.; Silva, A.; et al. Prevalence and risk factors of infections by multiresistant bacteria in cirrhosis: A prospective study. Hepatology 2012, 55, 1551–1561. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.; Harris, P.N.; Williamson, D.A.; Liss, M.A.; Doi, S.A.R.; Roberts, M.J. The effectiveness of targeted relative to empiric prophylaxis on infectious complications after transrectal ultrasound-guided prostate biopsy: A meta-analysis. World J. Urol. 2018, 36, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- EAU Guidelines; Edn. presented at the EAU Annual Congress Amsterdam, the Netherlands; EAU Guidelines Office: Arnhem, The Netherlands, 2022; ISBN 978-94-92671-16-5. p. 9. Available online: http://uroweb.org/guidelines/compilations-of-all-guidelines/ (accessed on 20 March 2023).
- Strus, M. Zakażenia narządów płciowych i układu moczowego. In Mikrobiologia Lekarska; Heczko, P.B., Wróblewska, M., Pietrzyk, A., Eds.; PZWL (National Institute of Medical Publications): Warsaw, Poland, 2022; pp. 715–718. [Google Scholar]
- Jung, J.; Kim, S.Y.; Park, Y.J.; Lee, J.; Suk, H.S.; Ha, S.I.; Shin, J.S.; Park, K.G.; Kim, Y. Comparison of the ASTA MicroIDSys and VITEK MS matrix-assisted laser desorption/ionization time-of-flight mass spectrometry systems for identification of clinical bacteria and yeasts. J. Infect Chemother. 2020, 26, 1328–1333. [Google Scholar] [CrossRef]
- Luo, Y.; Siu, K.H.; Yeung, A.S.F.; Chen, J.H.K.; Ho, P.L.; Leung, K.W.; Tsang, J.L.Y.; Cheng, V.C.C.; Guo, L.; Yang, J.; et al. Performance of the VITEK MS matrix-assisted laser desorption ionization-time of flight mass spectrometry system for rapid bacterial identification in two diagnostic centres in China. J. Med. Microbiol. 2015, 64, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Kovaleva, J. Infectious complications in gastrointestinal endoscopy and their prevention. Best. Pr. Res. Clin. Gastroenterol. 2016, 30, 689–704. [Google Scholar] [CrossRef]
- Sanguinetti, M.; Posteraro, B. Identification of Molds by Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry. J. Clin. Mikrobiol. 2017, 55, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Knabl, L.; Huber, S.; Lass-Flörl, C.; Fuchs, S. Comparison of novel approaches for expedited pathogen identification and antimicrobial susceptibility testing against routine blood culture diagnostics. Lett. Appl. Microbiol. 2021, 73, 2–8. [Google Scholar] [CrossRef]


{kind=link}
| The Microorganisms Identified n | E. coli 8 | E. coli, ESBL 2 | E. faecalis 5 | E. faecium 4 | K. pneumoniae, ESBL 3 | P. mirabilis 3 | P. aeruginosa 1 | S. epidermidis, MRCNS 1 | S. capitis, MRCNS 1 | C. albicans 1 | C. tropicalis 1 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| The Number of Sensitive Microorganisms, n (Percentages) | ||||||||||||
| AK | 8 (100%) | 1 (50%) | 3 (100%) | 3 (100%) | 1 (100%) | 1 (100%) | ||||||
| AMC | 4 (50%) | 2 (100%) | 2 (66.6%) | |||||||||
| ATM | 1 (100%) | |||||||||||
| CAZ | 8 (100%) | 3 (100%) | 1 (100%) | |||||||||
| CTX | 8 (100%) | 1 (33.3%) | 3 (100%) | |||||||||
| CXM | 8 (100%) | 1 (33.3%) | 2 (66.6%) | |||||||||
| CIP | 6 (75%) | 1 (33.3%) | 3 (100%) | |||||||||
| CT | 8 (100%) | 2 (66.6%) | ||||||||||
| FEP | 8 (100%) | 1 (33.3%) | 3 (100%) | 1 (100%) | ||||||||
| GM | 7 (87.5%) | 1 (50%) | 1 (33.3%) | 3 (100%) | 1 (100%) | |||||||
| IPM | 8 (100%) | 2 (100%) | 5 (100%) | 3 (100%) | 3 (100%) | 1 (100%) | ||||||
| MEM | 8 (100%) | 2 (100%) | 3 (100%) | 3 (100%) | 1 (100%) | |||||||
| TZP | 8 (100%) | 2 (100%) | 3 (100%) | 1 (100%) | ||||||||
| TGC | 8 (100%) | 2 (100%) | 5 (100%) | 4 (100%) | 1 (100%) | 1 (100%) | ||||||
| TM | 8 (100%) | 1 (50%) | 3 (100%) | 1 (100%) | ||||||||
| TIM | 1 (33.3%) | 1 (100%) | ||||||||||
| SXT | 7 (87.5%) | 1 (50%) | 2 (66.6%) | 2 (66.6%) | 1 (100%) | |||||||
| AM | 5 (100%) | |||||||||||
| LEV | 1 (20%) | |||||||||||
| LZD | 5 (100%) | 4 (100%) | 1 (100%) | 1 (100%) | ||||||||
| F | 5 (100%) | |||||||||||
| S | ||||||||||||
| TEC | 5 (100%) | 1 (100%) | 1 (100%) | |||||||||
| VA | 5 (100%) | 4 (100%) | 1 (100%) | 1 (100%) | ||||||||
| CM | 1 (100%) | 1 (100%) | ||||||||||
| E | 1 (100%) | 1 (100%) | ||||||||||
| OX | ||||||||||||
| TE | 1 (100%) | 1 (100%) | ||||||||||
| PIP | 1 (100%) | |||||||||||
| AmB | 1 (100%) | 1 (100%) | ||||||||||
| CAS | 1 (100%) | 1 (100%) | ||||||||||
| FLU | 1 (100%) | 1 (100%) | ||||||||||
| AFY | 1 (100%) | |||||||||||
| MYC | 1 (100%) | 1 (100%) | ||||||||||
| VO | 1 (100%) | 1 (100%) | ||||||||||
| Characteristics of the Patients | Positive Urine Culture Results (n = 30) | Negative Urine Culture Results (n = 72) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Women (n = 16) | Men (n = 14) | Women (n = 28) | Men (n = 44) | |||||||||
| Age of patients, years | 33–101 | 27–93 | 30–87 | 26–99 | ||||||||
| Age of patients—arithmetic mean, years (standard deviation) | 75.6 (17.17) | 61.7 (18.3) | 66.1 (18.7) | 63.2 (17.2) | ||||||||
| Duration of hospitalization, days | 2–35 | |||||||||||
| Duration of hospitalization—arithmetic mean, days (standard deviation) | 11.6 (7.1) | |||||||||||
| The diagnoses with which the patients reported to the hospital (concerns all 102 examined patients), n | IBD, 4 | Liver cirrhosis, 35 | Pancreatitis, 14 | Gastrointestinal bleeding, 18 | Diverticulosis of the large intestine, 2 | Other, 29 ** | ||||||
| Urine culture result/quantity (%) * | −/4 | +/0 | −/23 | +/12 (34.3) | −/13 | +/1 (7.1) | −/13 | +/5 (27.8) | −/0 | +/2 (100) | −/19 | +/10 (34.5) |
| Origin of the infection | community-acquired | hospital-acquired | ||||||||||
| n = 20 | n = 10 | |||||||||||
| Women—11 | Men—9 | Women—5 | Men—5 | |||||||||
| Diagnoses with which the patients reported to the hospital (applies to the 30 patients with positive urine cultures), n | Liver cirrhosis, 14 | Pancreatitis, 8 | Diverticulosis of the large intestine, 2 | Cholecystitis, 2 | Duodenitis, 2 | Duodenalulcer, 2 | ||||||
| Treatment effect | Improvement—21 | Death—9 | ||||||||||
| Patients with a positive urine culture and a urinary catheter, n | 26 | |||||||||||
| Women—13 | Men—13 | |||||||||||
| Taking samples for testing | All samples were taken during hospitalization. | |||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gruszecka, J.; Filip, R. Urinary Tract Infections in Patients Hospitalized in a Gastroenterology Department—Study from a Tertiary Regional Hospital in South-East Poland. Gastrointest. Disord. 2023, 5, 198-208. https://doi.org/10.3390/gidisord5020017
Gruszecka J, Filip R. Urinary Tract Infections in Patients Hospitalized in a Gastroenterology Department—Study from a Tertiary Regional Hospital in South-East Poland. Gastrointestinal Disorders. 2023; 5(2):198-208. https://doi.org/10.3390/gidisord5020017
Chicago/Turabian StyleGruszecka, Jolanta, and Rafał Filip. 2023. "Urinary Tract Infections in Patients Hospitalized in a Gastroenterology Department—Study from a Tertiary Regional Hospital in South-East Poland" Gastrointestinal Disorders 5, no. 2: 198-208. https://doi.org/10.3390/gidisord5020017