
The Frequency and Characteristics of Severe Liver-Related Adverse Events in Patients with Chronic Liver Diseases after Vaccination against Severe Acute Respiratory Syndrome Coronavirus 2: A Retrospective Study

 ,
,
Abstract
:1. Introduction
2. Results
2.1. High Vaccination Rate in Patients with Chronic Liver Diseases in Our Hospital
2.2. Liver Cirrhosis and Autoimmune Diseases as Risk Factors for Severe LrAEs after Vaccination
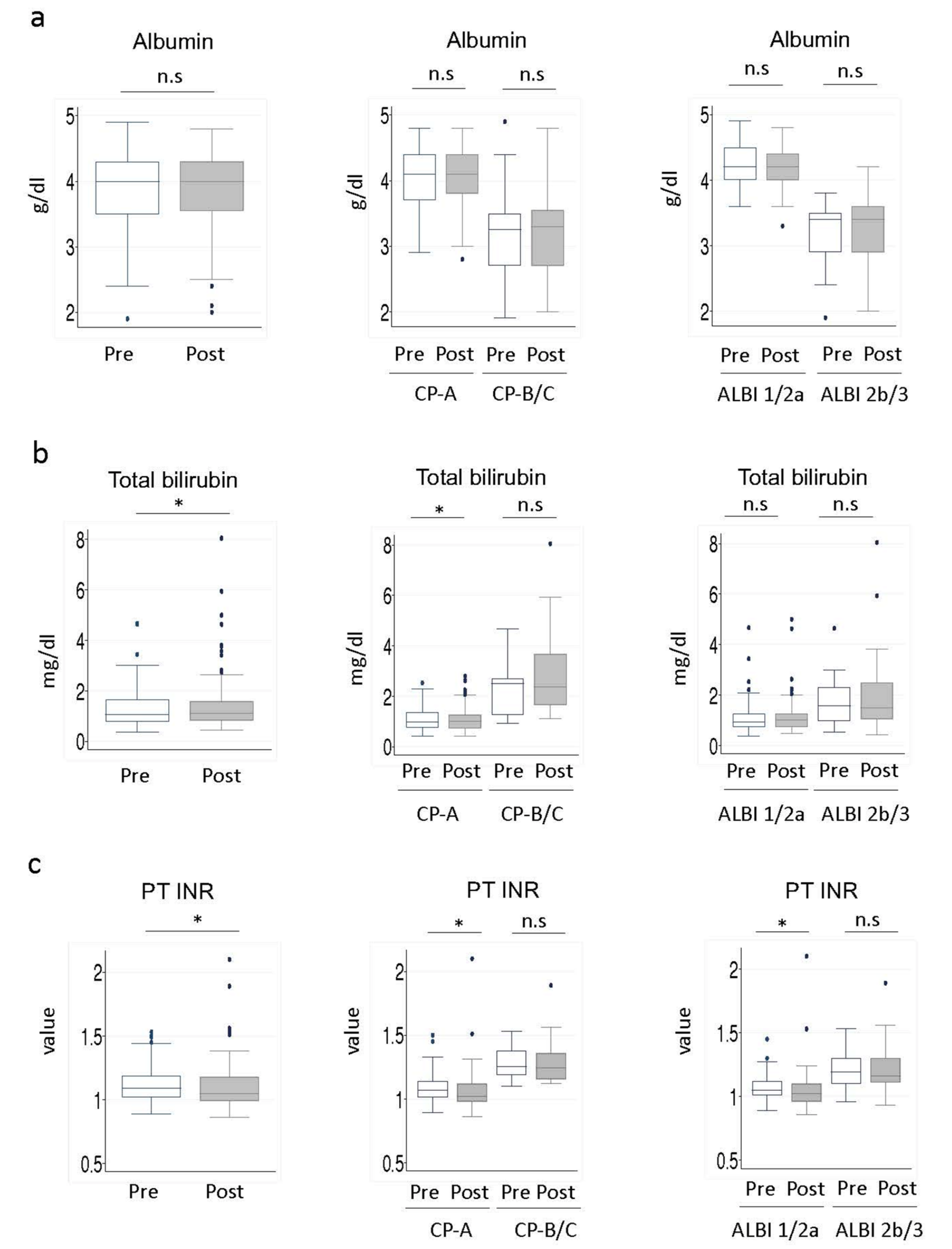
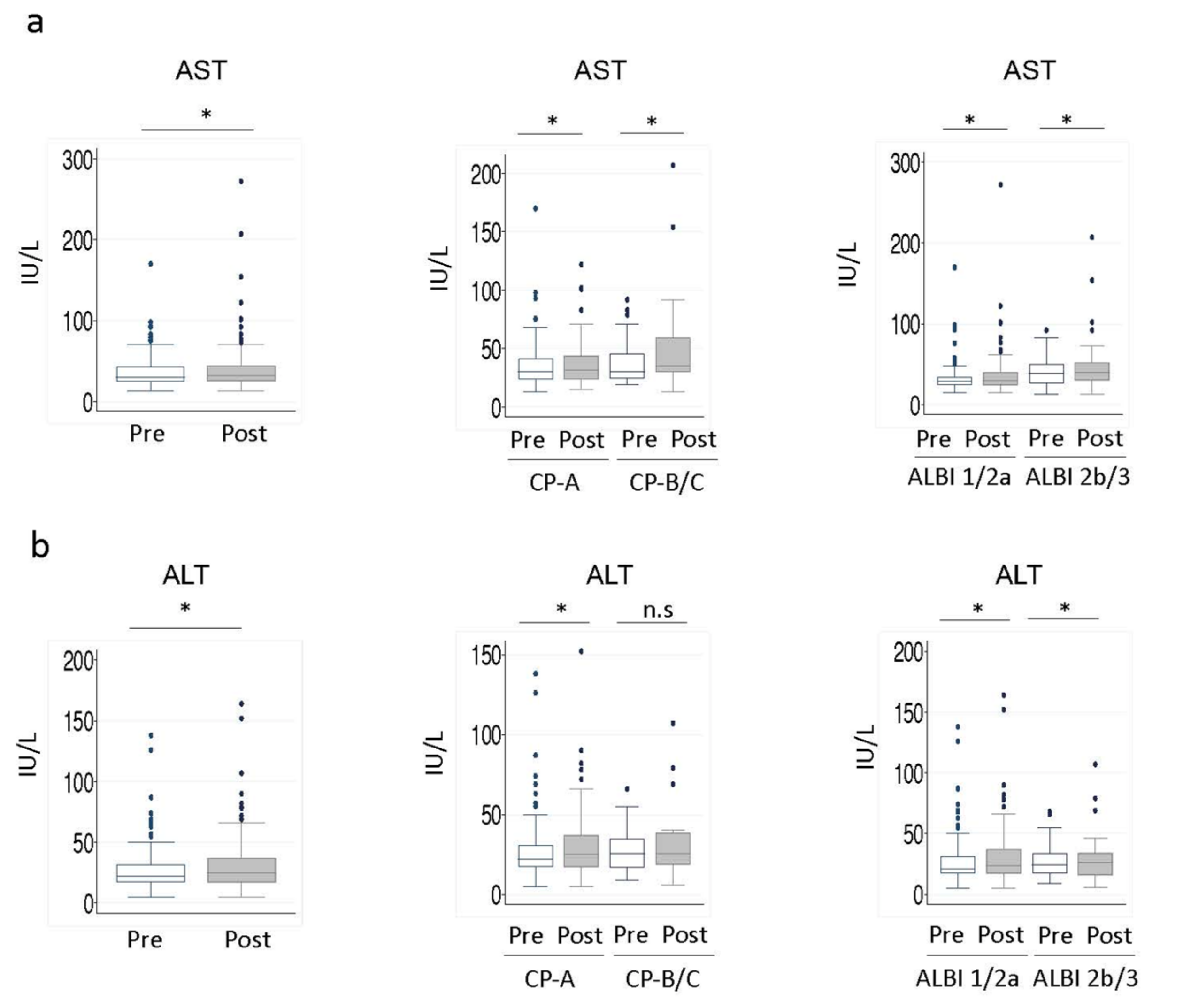
2.3. Association between Vaccination and the Liver Function Reserve in Patients with Liver Cirrhosis
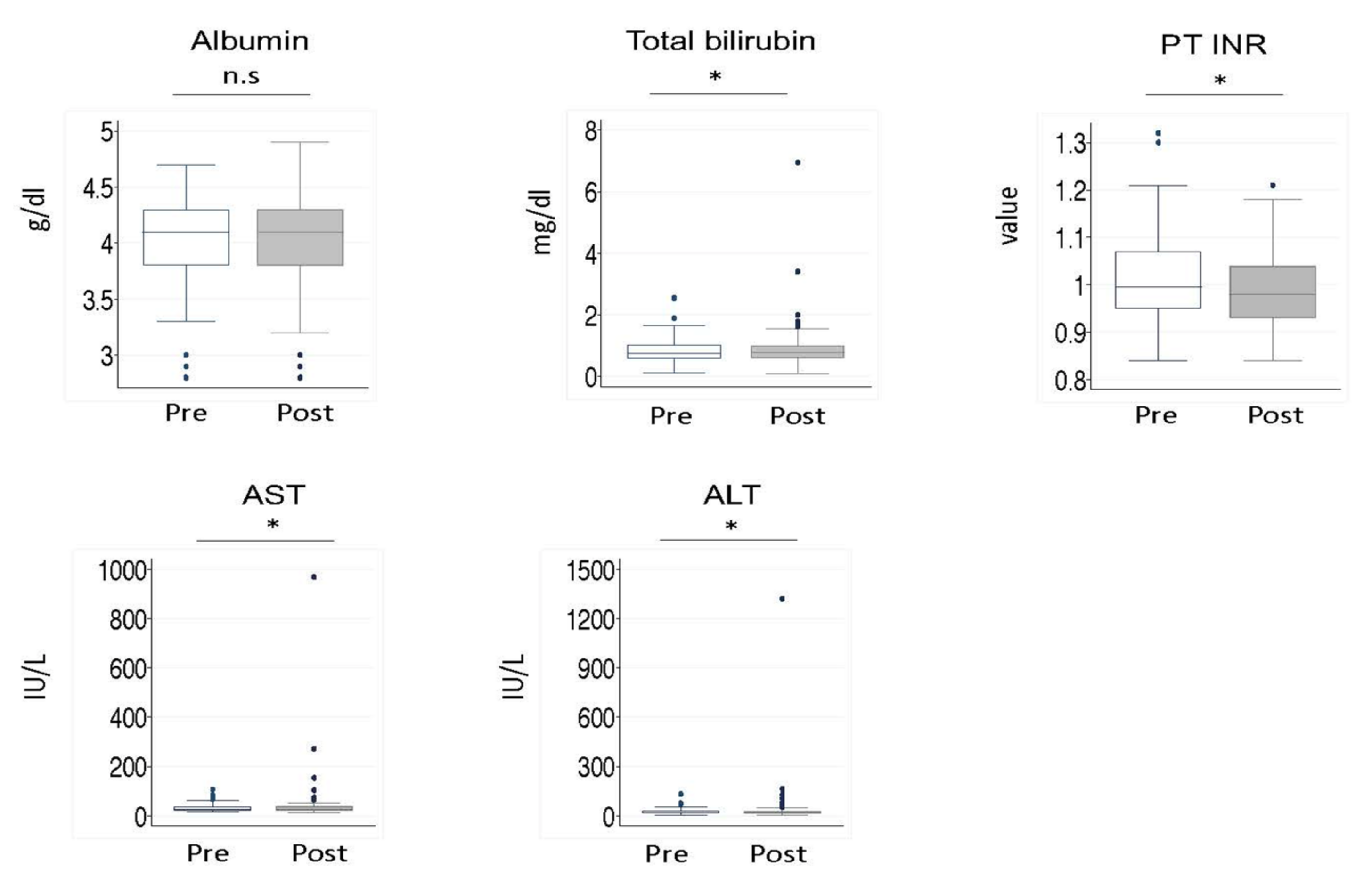
2.4. Vaccination Effects on the Liver Function Tests in Patients with Autoimmune Diseases
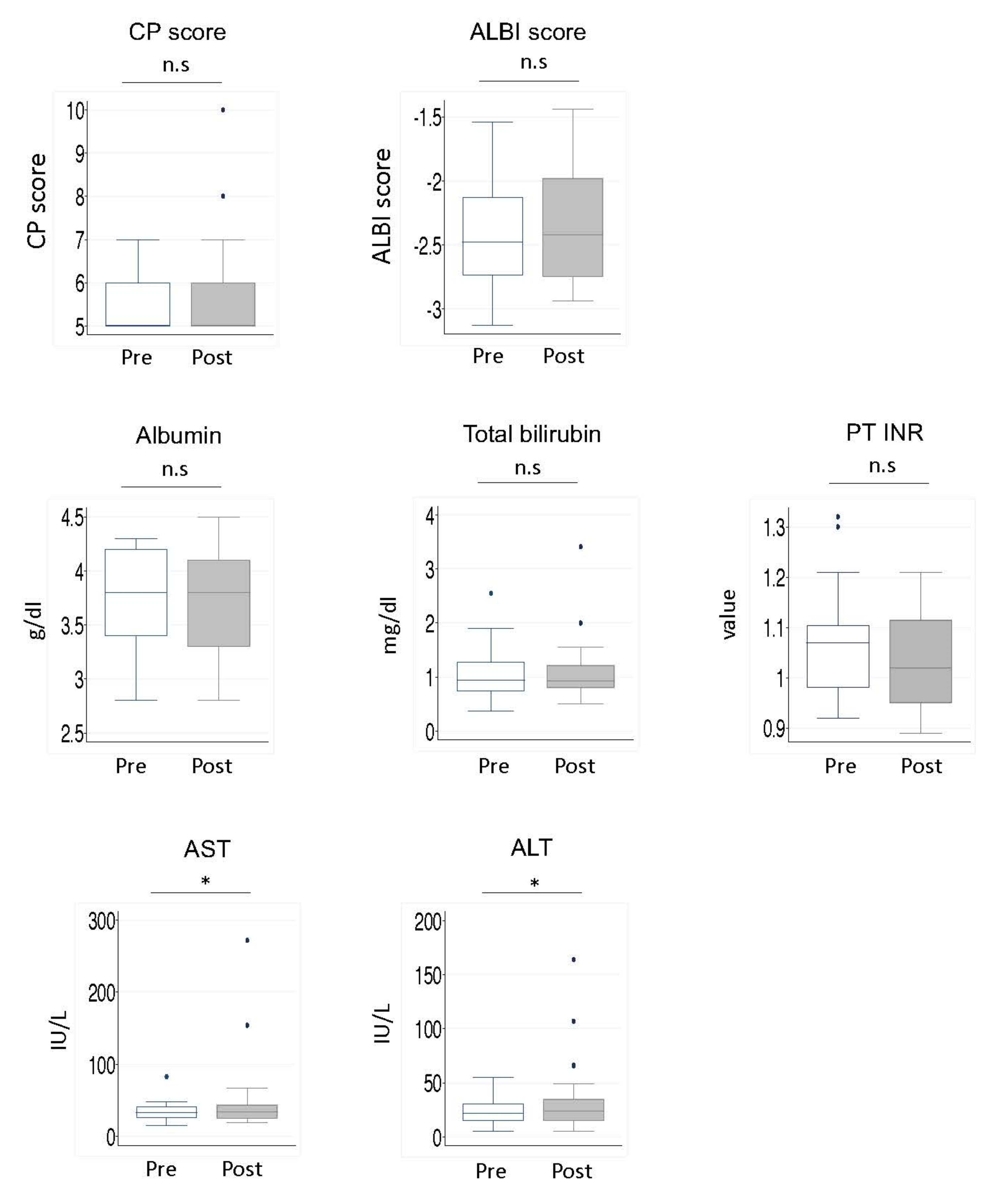
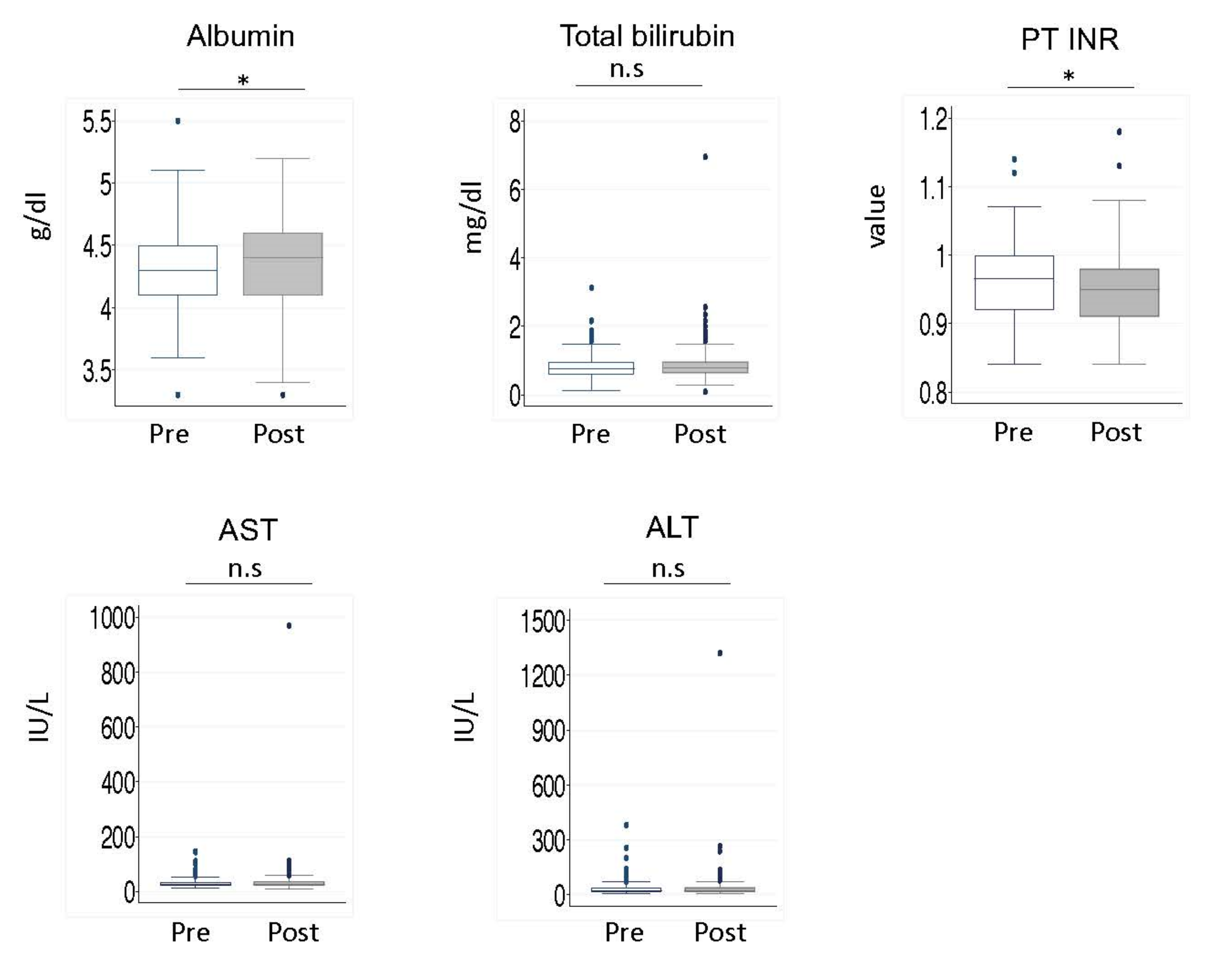
2.5. Vaccination Effects on Liver Function Tests in Noncirrhotic Patients
3. Discussion
4. Materials and Methods
4.1. Design
4.2. Patients
5. Statistical Analyses
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.-J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef]
- Schinas, G.; Polyzou, E.; Mitropetrou, F.; Pazionis, A.; Gogos, C.; Triantos, C.; Akinosoglou, K. COVID-19 Vaccination in Patients with Chronic Liver Disease. Viruses 2022, 14, 2778. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, Q.; Ai, J.; Liu, D.; Liu, C.; Xiang, H.; Gu, Y.; Guo, Y.; Lv, J.; Huang, Y.; et al. Safety and immunogenicity of SARS-CoV-2 vaccines in Chinese patients with cirrhosis: A prospective multicenter study. Hepatol. Int. 2022, 16, 691–701. [Google Scholar] [CrossRef]
- Ai, J.; Wang, J.; Liu, D.; Xiang, H.; Guo, Y.; Lv, J.; Zhang, Q.; Li, J.; Zhang, X.; Li, Q.; et al. Safety and Immunogenicity of SARS-CoV-2 Vaccines in Patients With Chronic Liver Diseases (CHESS-NMCID 2101): A Multicenter Study. Clin. Gastroenterol. Hepatol. 2022, 20, 1516–1524.e2. [Google Scholar] [CrossRef] [PubMed]
- Fix, O.K.; Blumberg, E.A.; Chang, K.-M.; Chu, J.; Chung, R.T.; Goacher, E.K.; Hameed, B.; Kaul, D.R.; Kulik, L.M.; Kwok, R.M.; et al. American Association for the Study of Liver Diseases Expert Panel Consensus Statement: Vaccines to Prevent Coronavirus Disease 2019 Infection in Patients with Liver Disease. Hepatology 2021, 74, 1049–1064. [Google Scholar] [CrossRef] [PubMed]
- Cornberg, M.; Buti, M.; Eberhardt, C.S.; Grossi, P.A.; Shouval, D. EASL position paper on the use of COVID-19 vaccines in patients with chronic liver diseases, hepatobiliary cancer and liver transplant recipients. J. Hepatol. 2021, 74, 944–951. [Google Scholar] [CrossRef] [PubMed]
- John, B.V.; Deng, Y.; Scheinberg, A.; Mahmud, N.; Taddei, T.H.; Kaplan, D.; Labrada, M.; Baracco, G.; Dahman, B. Association of BNT162b2 mRNA and mRNA-1273 Vaccines With COVID-19 Infection and Hospitalization Among Patients With Cirrhosis. JAMA Intern. Med. 2021, 181, 1306–1314. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Zhang, C.; Zhao, S.; Sheng, Z.; Xiang, X.; Li, R.; Qian, Z.; Wang, Y.; Bin Chen, B.; Li, Z.; et al. COVID-19 vaccines in patients with decompensated cirrhosis: A retrospective cohort on safety data and risk factors associated with unvaccinated status. Infect. Dis. Poverty 2022, 11, 56. [Google Scholar] [CrossRef] [PubMed]
- Shroff, H.; Satapathy, S.K.; Crawford, J.M.; Todd, N.J.; VanWagner, L.B. Liver injury following SARS-CoV-2 vaccination: A multicenter case series. J. Hepatol. 2022, 76, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Izagirre, A.; Arzallus, T.; Garmendia, M.; Torrente, S.; Castiella, A.; Zapata, E.M. Autoimmune hepatitis following COVID-19 vaccination. J. Autoimmun. 2022, 132, 102874. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Zhang, T.; Xu, Y.; Lu, X.; Sang, X. Autoimmune hepatitis after COVID-19 vaccination. Front. Immunol. 2022, 13, 1035073. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Xu, Z.; Wang, P.; Li, X.; Shuai, Z.; Ye, D.; Pan, H. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology 2022, 165, 386–401. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Akira, S. Toll-like Receptors and Their Crosstalk with Other Innate Receptors in Infection and Immunity. Immunity 2011, 34, 637–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segal, Y.; Shoenfeld, Y. Vaccine-induced autoimmunity: The role of molecular mimicry and immune crossreaction. Cell. Mol. Immunol. 2018, 15, 586–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shulman, R.M.; Weinberg, D.S.; Ross, E.A.; Ruth, K.; Rall, G.F.; Olszanski, A.J.; Helstrom, J.; Hall, M.J.; Judd, J.; Chen, D.Y.; et al. Adverse Events Reported by Patients With Cancer After Administration of a 2-Dose mRNA COVID-19 Vaccine. J. Natl. Compr. Cancer Netw. 2022, 20, 160–166. [Google Scholar] [CrossRef] [PubMed]
- John, B.V.; Ferreira, R.D.; Doshi, A.; Kaplan, D.E.; Taddei, T.H.; Spector, S.A.; Paulus, E.; Deng, Y.; Bastaich, D.; Dahman, B. Third dose of COVID-19 mRNA vaccine appears to overcome vaccine hyporesponsiveness in patients with cirrhosis. J. Hepatol. 2022, 77, 1349–1358. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n) | Vaccine, n (%) | Japan | Tochigi | |
|---|---|---|---|---|
| 431 | 416 (96.5%) | 81.0% | 82.7% | |
| Age 20–29 | 9 | 9 (100%) | 80.5% | 84.2% |
| Age 30–39 | 18 | 18 (100%) | 79.8% | 81.8% |
| Age 40–49 | 40 | 38 (95%) | 82.5% | 85.0% |
| Age 50–59 | 89 | 87 (97.8%) | 92.5% | 93.9% |
| Age 60–69 | 109 | 100 (91.7%) | 89.1% | 88.7% |
| Age 70–79 | 130 | 128 (98.4%) | 94.5% | 97.3% |
| Age 80- | 36 | 36 (100%) | 99.3% | 98.6% |
| Total | |
|---|---|
| n | 345 |
| Age | 66 (22–90) |
| Liver cirrhosis | 125 (36.2%) |
| Hepatocellular carcinoma | 65 (18.8%) |
| Autoimmune diseases * | 92 (26.7%) |
| Pfizer/Moderna/unknown | 283/34/28 |
| Hepatitis B virus | 65 (18.8%) |
| Hepatitis C virus | 69 (20.0%) |
| Autoimmune hepatitis | 38 (11.0%) |
| Primary biliary cholangitis | 31 (9.0%) |
| Nonalcoholic fatty liver disease | 81 (23.5%) |
| Alcohol | 33 (9.6%) |
| Others | 20 (5.8%) |
| Unknown | 8 (2.3%) |
| No | Age | Sex | Liver Disease | Cirrhosis | HCC | AID | CP Score | ALBI | Provider | sAE | LrAE | Detail of LrAEs |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 70′ | F | HBV | Yes | No | 6 | 2b | Pfizer | No | Grade 3 | CP score 9, limiting self-care ADL due to ascites | |
| 2 | 40′ | M | HCV | Yes | Yes | 7 | 2b | Moderna | Yes | Grade 3 | Total bilirubin 1.23 → 8.05 | |
| 3 | 70′ | F | AIH | Yes | No | N/A | 1 | Pfizer | Yes | Grade 3 | ALT 20 → 164 | |
| 4 | 70′ | M | NAFLD | Yes | No | RA | 6 | 2b | Pfizer | Yes | Grade 3 | CP score 8, limiting self-care ADL due to ascites |
| 5 | 50′ | M | Alcohol | Yes | No | Basedow | 7 | 2b | Pfizer | Yes | Grade 3 | CP score 10, limiting self-care ADL due to ascites |
| 6 | 50′ | F | AIH | No | No | 5 | 1 | Pfizer | Yes | Grade 4 | ALT 33 → 1321 |
| Parameters | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p Value | |
| Hepatitis B virus | 0.714 (0.084–6.031) | 0.757 | - | - |
| Hepatitis C virus | 0.662 (0.784–5.589) | 0.705 | - | - |
| Nonalcoholic fatty liver disease | 0.538 (0.064–4.531) | 0.568 | - | - |
| Alcohol | 1.593 (0.186–13.66) | 0.671 | - | - |
| Unknown | 7.881 (0.834–74.43) | 0.072 | - | - |
| Autoimmune disease | 7.441 (1.418–39.06) | 0.018 | 21.14 (1.846–242.0) | 0.014 |
| Age ≧ 65 | 0.666 (0.147–3.022) | 0.599 | - | - |
| Gender | 0.674 (0.149–3.058) | 0.609 | - | - |
| Liver cirrhosis | 11.04 (1.314–92.80) | 0.027 | 16.23 (1.304–202.1) | 0.030 |
| Hepatocellular carcinoma | 0.714 (0.084–6.031) | 0.757 | - | - |
| Provider of vaccine | 1.321 (0.156–11.18) | 0.798 | - | - |
| Symptomatic AEs | 3.218 (0.383–27.05) | 0.282 | - | - |
| ≥Grade 3 LrAEs | p Value | |
|---|---|---|
| CP Class A (n = 91) | 2 (2.2%) | 0.09 |
| CP Class B/C (n = 20) | 2 (10.0%) | |
| ALBI Grade 1/2a (n = 82) | 1 (1.2%) | 0.026 |
| ALBI Grade 2b/3 (n = 42) | 4 (9.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bat-Erdene, O.; Miura, K.; Maeda, H.; Watanabe, S.; Tsukui, M.; Takaoka, Y.; Nomoto, H.; Goka, R.; Morimoto, N.; Yamamoto, H. The Frequency and Characteristics of Severe Liver-Related Adverse Events in Patients with Chronic Liver Diseases after Vaccination against Severe Acute Respiratory Syndrome Coronavirus 2: A Retrospective Study. Gastrointest. Disord. 2023, 5, 15-27. https://doi.org/10.3390/gidisord5010002
Bat-Erdene O, Miura K, Maeda H, Watanabe S, Tsukui M, Takaoka Y, Nomoto H, Goka R, Morimoto N, Yamamoto H. The Frequency and Characteristics of Severe Liver-Related Adverse Events in Patients with Chronic Liver Diseases after Vaccination against Severe Acute Respiratory Syndrome Coronavirus 2: A Retrospective Study. Gastrointestinal Disorders. 2023; 5(1):15-27. https://doi.org/10.3390/gidisord5010002
Chicago/Turabian StyleBat-Erdene, Oyunjargal, Kouichi Miura, Hiroshi Maeda, Shunji Watanabe, Mamiko Tsukui, Yoshinari Takaoka, Hiroaki Nomoto, Rie Goka, Naoki Morimoto, and Hironori Yamamoto. 2023. "The Frequency and Characteristics of Severe Liver-Related Adverse Events in Patients with Chronic Liver Diseases after Vaccination against Severe Acute Respiratory Syndrome Coronavirus 2: A Retrospective Study" Gastrointestinal Disorders 5, no. 1: 15-27. https://doi.org/10.3390/gidisord5010002