
Effects on Sleep Quality of Physical Exercise Programs in Older Adults: A Systematic Review and Meta-Analysis
 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Criteria for Considering Studies in This Review
2.3. Search Strategies and Data Resources
2.4. Reviewing Procedure and Data Extraction
2.5. Methodological Quality Assessment
2.6. Data Synthesis and Analysis
3. Results
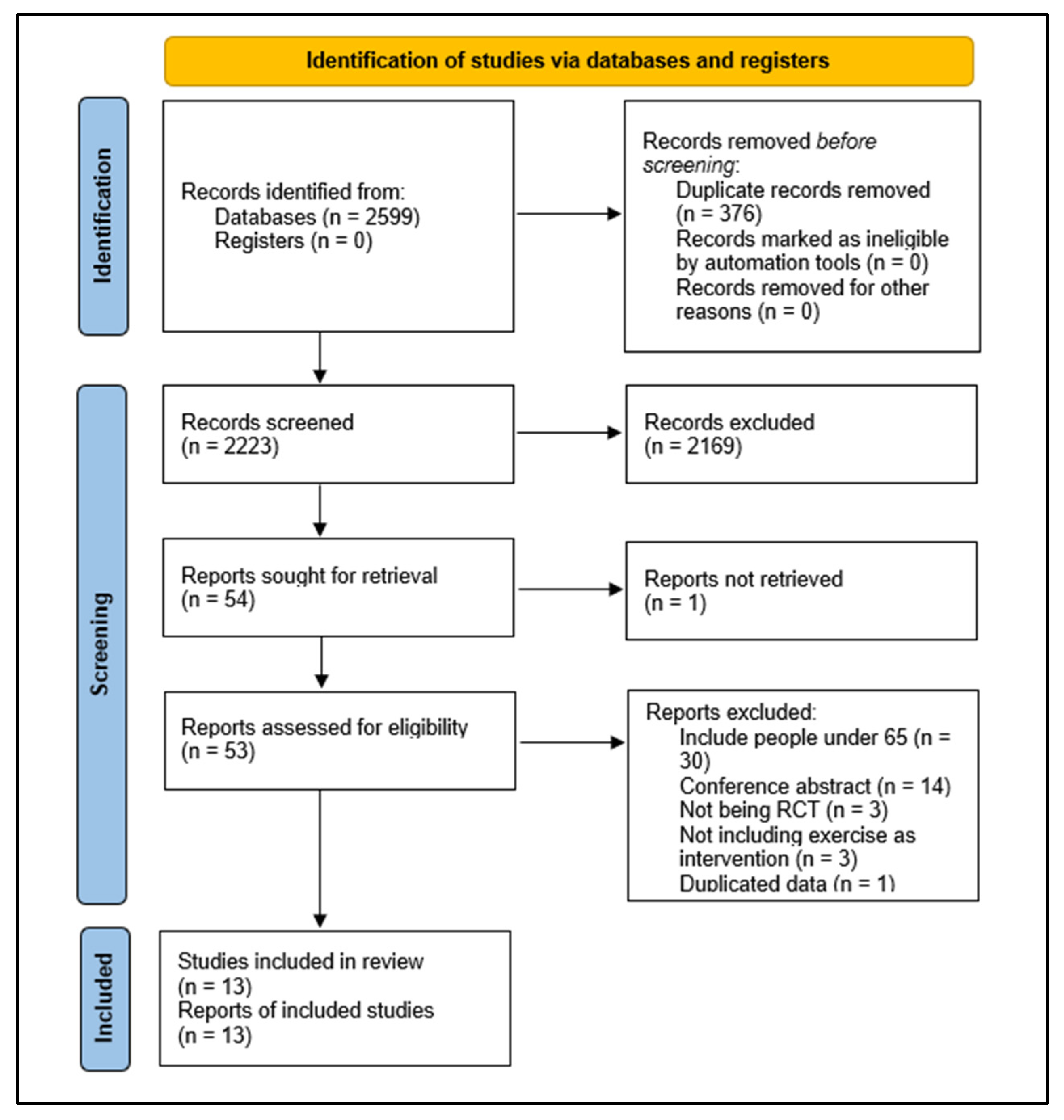
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Participants
3.4. Characteristics of Training
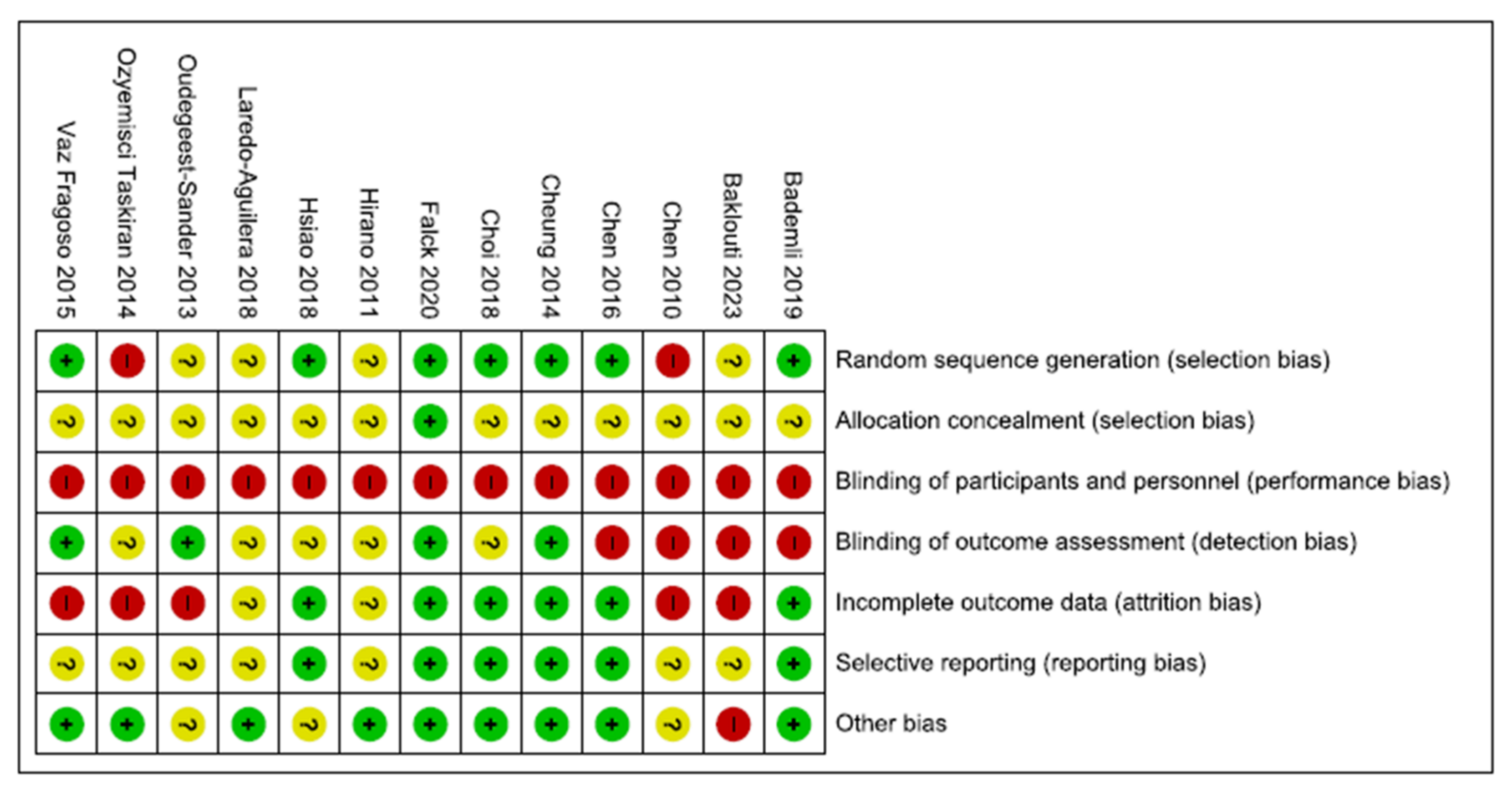
3.5. Methodological Quality Assessment
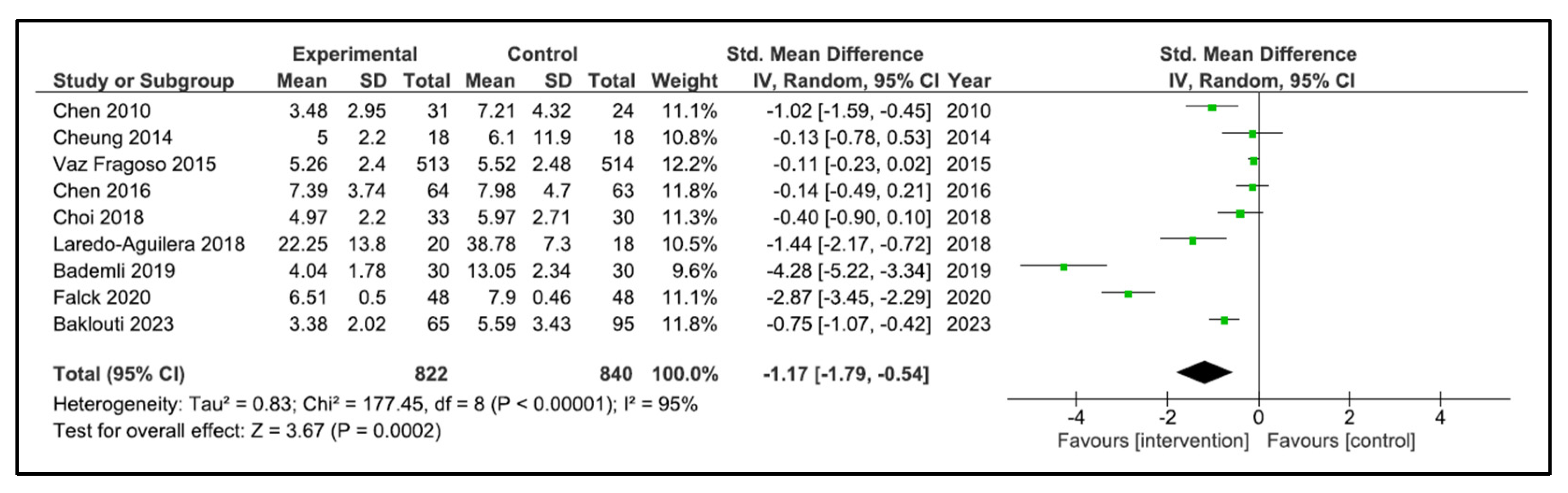
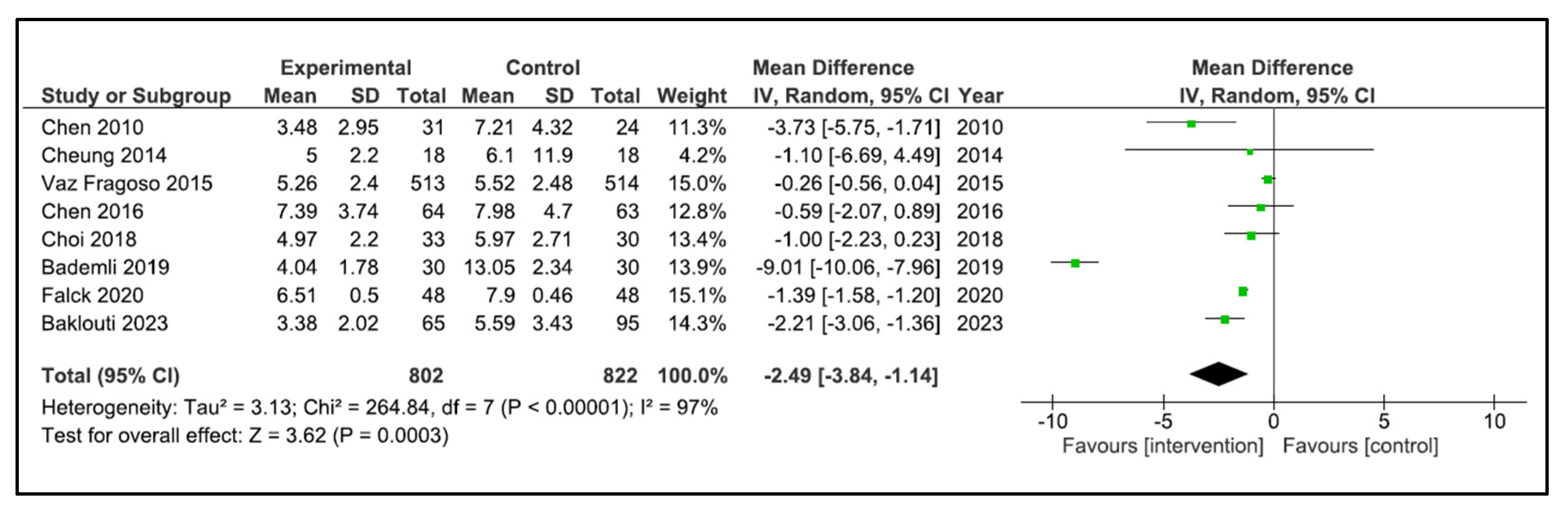
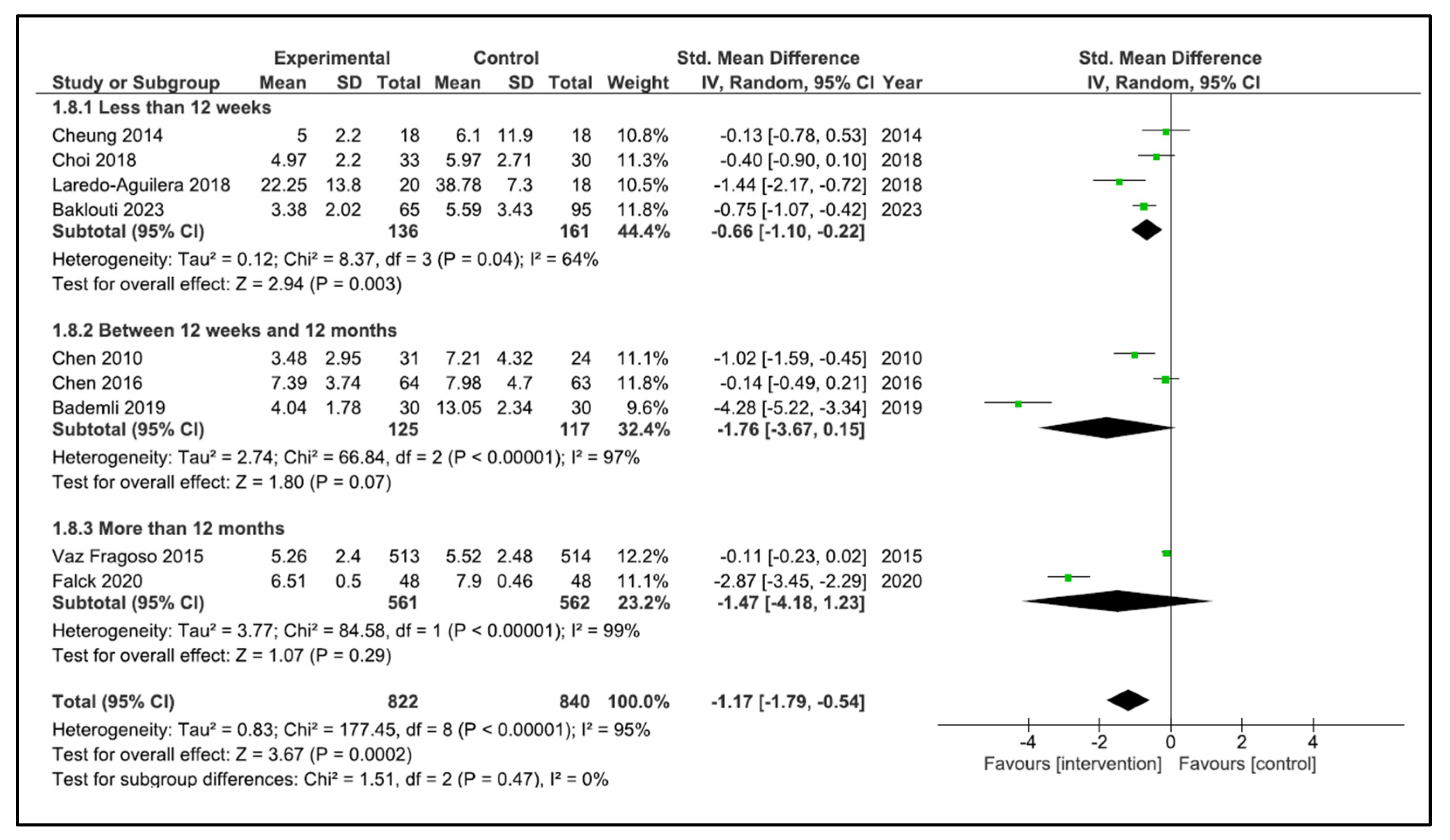
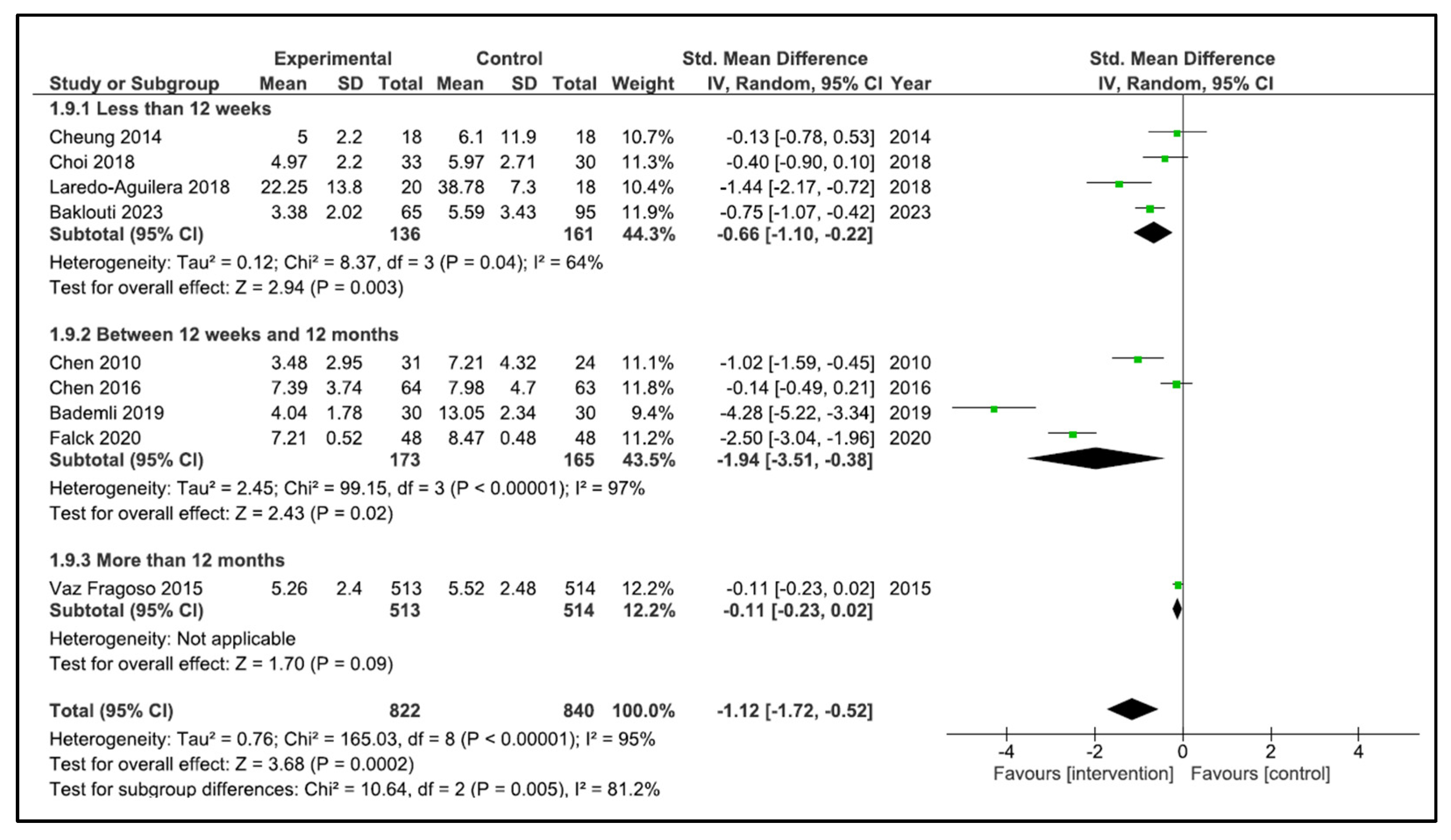
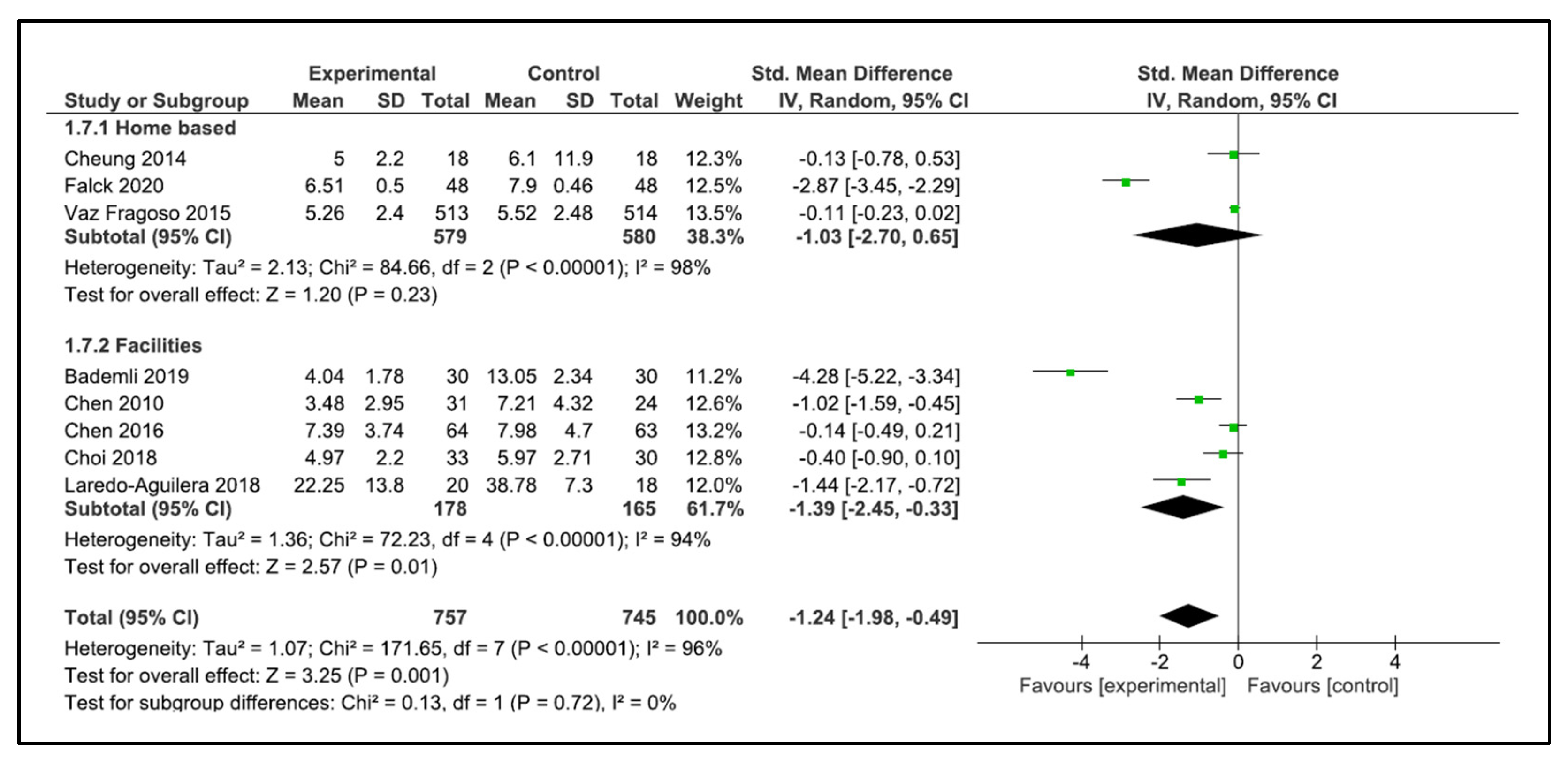
3.6. Main Findings
4. Discussion
4.1. Effects on Sleep Quality
4.2. Sleep Quality Assessment
4.3. Exercise Programs
4.4. Clinical Implications
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The World Bank. United Nations Population Division. World Population Prospects: 2022 Revision. Available online: https://data.worldbank.org/indicator/SP.POP.65UP.TO.ZS (accessed on 15 January 2023).
- World Health Organization. Ageing and Health. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 2 May 2022).
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Mora, J.C.; Valencia, W.M. Exercise and Older Adults. Clin. Geriatr. Med. 2018, 34, 145–162. [Google Scholar] [CrossRef]
- Daskalopoulou, C.; Stubbs, B.; Kralj, C.; Koukounari, A.; Prince, M.; Prina, A.M. Physical activity and healthy ageing: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Res. Rev. 2017, 38, 6–17. [Google Scholar] [CrossRef] [Green Version]
- Gopinath, B.; Kifley, A.; Flood, V.M.; Mitchell, P. Physical Activity as a Determinant of Successful Aging over Ten Years. Sci. Rep. 2018, 8, 10522. [Google Scholar] [CrossRef] [Green Version]
- Speakman, J.R.; Westerterp, K.R. Associations between energy demands, physical activity, and body composition in adult humans between 18 and 96 y of age. Am. J. Clin. Nutr. 2010, 92, 826–834. [Google Scholar] [CrossRef] [Green Version]
- Sindi, S.; Pérez, L.M.; Vetrano, D.L.; Triolo, F.; Kåreholt, I.; Sjöberg, L.; Darin-Mattsson, A.; Kivipelto, M.; Inzitari, M.; Calderón-Larrañaga, A. Sleep disturbances and the speed of multimorbidity development in old age: Results from a longitudinal population-based study. BMC Med. 2020, 18, 382. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Picca, A.; Tosato, M.; Martone, A.M.; Angelo, E.D.; Serafini, E.; Bernabei, R.; Marzetti, E. Impact of habitual physical activity and type of exercise on physical performance across ages in community-living people. PLoS ONE 2018, 13, e0191820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaput, J.-P.; Dutil, C.; Featherstone, R.; Ross, R.; Giangregorio, L.; Saunders, T.J.; Janssen, I.; Poitras, V.J.; Kho, M.E.; Ross-White, A.; et al. Sleep timing, sleep consistency, and health in adults: A systematic review. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2020, 45, S232–S247. [Google Scholar] [CrossRef]
- Chen, K.-M.; Huang, H.-T.; Cheng, Y.-Y.; Li, C.-H.; Chang, Y.-H. Sleep quality and depression of nursing home older adults in wheelchairs after exercises. Nurs. Outlook 2015, 63, 357–365. [Google Scholar] [CrossRef]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.; Ancoli-Israel, S.; Britz, P.; Walsh, J. Sleep disturbances and chronic disease in older adults: Results of the 2003 National Sleep Foundation Sleep in America Survey. J. Psychosom. Res. 2004, 56, 497–502. [Google Scholar] [CrossRef]
- Bertisch, S.M.; Herzig, S.J.; Winkelman, J.W.; Buettner, C. National use of prescription medications for insomnia: NHANES 1999–2010. Sleep 2014, 37, 343–349. [Google Scholar] [CrossRef] [Green Version]
- Atkin, T.; Comai, S.; Gobbi, G. Drugs for Insomnia beyond Benzodiazepines: Pharmacology, Clinical Applications, and Discovery. Pharmacol. Rev. 2018, 70, 197–245. [Google Scholar] [CrossRef]
- Mokhar, A.; Tillenburg, N.; Dirmaier, J.; Kuhn, S.; Härter, M.; Verthein, U. Potentially inappropriate use of benzodiazepines and z-drugs in the older population-analysis of associations between long-term use and patient-related factors. PeerJ 2018, 6, e4614. [Google Scholar] [CrossRef]
- Amari, D.T.; Juday, T.; Frech, F.H.; Wang, W.; Wu, Z.; Atkins, N.; Wickwire, E.M. Falls, healthcare resources and costs in older adults with insomnia treated with zolpidem, trazodone, or benzodiazepines. BMC Geriatr. 2022, 22, 484. [Google Scholar] [CrossRef]
- By the 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef]
- Solis-Navarro, L.; Gismero, A.; Fernández-Jané, C.; Torres-Castro, R.; Solá-Madurell, M.; Bergé, C.; Pérez, L.M.; Ars, J.; Martín-Borràs, C.; Vilaró, J.; et al. Effectiveness of home-based exercise delivered by digital health in older adults: A systematic review and meta-analysis. Age Ageing 2022, 51, afac243. [Google Scholar] [CrossRef]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef]
- Fiuza-Luces, C.; Santos-Lozano, A.; Joyner, M.; Carrera-Bastos, P.; Picazo, O.; Zugaza, J.L.; Izquierdo, M.; Ruilope, L.M.; Lucia, A. Exercise benefits in cardiovascular disease: Beyond attenuation of traditional risk factors. Nat. Rev. Cardiol. 2018, 15, 731–743. [Google Scholar] [CrossRef]
- Torres-Castro, R.; Vilaró, J.; Martí, J.-D.; Garmendia, O.; Gimeno-Santos, E.; Romano-Andrioni, B.; Embid, C.; Montserrat, J.M. Effects of a Combined Community Exercise Program in Obstructive Sleep Apnea Syndrome: A Randomized Clinical Trial. J. Clin. Med. 2019, 8, 361. [Google Scholar] [CrossRef] [Green Version]
- Castelli, L.; Galasso, L.; Mulè, A.; Bruno, E.; Shokohyar, S.; Esposito, F.; Montaruli, A.; Roveda, E. Physical activity, chronotype and sleep in a sample of Italian elderly population. Sport Sci. Health 2019, 16, 55–64. [Google Scholar] [CrossRef]
- Ashworth, N.L.; Chad, K.E.; Harrison, E.; Reeder, B.A.; Marshall, S.C. Home versus center based physical activity programs in older adults. Cochrane Database Syst. Rev. 2005, 2005, CD004017. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Orimo, H. Reviewing the definition of elderly. Geriatr. Gerontol. Int. 2006, 6, 149–158. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.0; Cochrane: London, UK, 2019. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Project T Jamovi. Jamovi. 2022. Available online: https://www.jamovi.org (accessed on 22 January 2023).
- Chen, K.-M.; Chen, M.-H.; Lin, M.-H.; Fan, J.-T.; Lin, H.-S.; Li, C.-H. Effects of yoga on sleep quality and depression in elders in assisted living facilities. J. Nurs. Res. 2010, 18, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Hirano, A.; Suzuki, Y.; Kuzuya, M.; Onishi, J.; Ban, N.; Umegaki, H. Influence of regular exercise on subjective sense of burden and physical symptoms in community-dwelling caregivers of dementia patients: A randomized controlled trial. Arch. Gerontol. Geriatr. 2011, 53, e158–e163. [Google Scholar] [CrossRef]
- Bademli, K.; Lok, N.; Canbaz, M.; Lok, S. Effects of Physical Activity Program on cognitive function and sleep quality in elderly with mild cognitive impairment: A randomized controlled trial. Perspect. Psychiatr. Care 2018, 55, 401–408. [Google Scholar] [CrossRef]
- Falck, R.S.; Davis, J.C.; Best, J.R.; Chan, P.C.; Li, L.C.; Wyrough, A.B.; Bennett, K.J.; Backhouse, D.; Liu-Ambrose, T. Effect of a Multimodal Lifestyle Intervention on Sleep and Cognitive Function in Older Adults with Probable Mild Cognitive Impairment and Poor Sleep: A Randomized Clinical Trial. J. Alzheimer’s Dis. 2020, 76, 179–193. [Google Scholar] [CrossRef] [PubMed]
- Baklouti, S.; Fekih-Romdhane, F.; Guelmami, N.; Bonsaksen, T.; Baklouti, H.; Aloui, A.; Masmoudi, L.; Souissi, N.; Jarraya, M. The effect of web-based Hatha yoga on psychological distress and sleep quality in older adults: A randomized controlled trial. Complement. Ther. Clin. Pract. 2023, 50, 101715. [Google Scholar] [CrossRef] [PubMed]
- Oudegeest-Sander, M.H.; Eijsvogels, T.H.M.; Verheggen, R.J.H.M.; Poelkens, F.; Hopman, M.T.E.; Jones, H.; Thijssen, D.H.J. Impact of physical fitness and daily energy expenditure on sleep efficiency in young and older humans. Gerontology 2013, 59, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.; Wyman, J.F.; Resnick, B.; Savik, K. Yoga for managing knee osteoarthritis in older women: A pilot randomized controlled trial. BMC Complement. Altern. Med. 2014, 14, 160. [Google Scholar] [CrossRef] [Green Version]
- Taşkiran, Ö.Ö.; Cicioğlu, İ.; Golmoghani-Zadeh, N.; Atilgan, A.D.; Bağci, E.; Günay, M.; Atalay, F. Do Pilates and yoga affect quality of life and physical performance of elderly living in a nursing home a preliminary study. Turk. J. Geriatr./Türk Geriatr. Derg. 2014, 17, 262–271. [Google Scholar]
- Vaz Fragoso, C.A.; Miller, M.E.; King, A.C.; Kritchevsky, S.B.; Liu, C.K.; Myers, V.H.; Nadkarni, N.K.; Pahor, M.; Spring, B.J.; Gill, T.M.; et al. Effect of Structured Physical Activity on Sleep-Wake Behaviors in Sedentary Elderly Adults with Mobility Limitations. J. Am. Geriatr. Soc. 2015, 63, 1381–1390. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.-M.; Li, C.-H.; Huang, H.-T.; Cheng, Y.-Y. Feasible modalities and long-term effects of elastic band exercises in nursing home older adults in wheelchairs: A cluster randomized controlled trial. Int. J. Nurs. Stud. 2016, 55, 4–14. [Google Scholar] [CrossRef]
- Hsiao, C.-Y.; Chen, K.-M.; Tsai, H.-Y.; Huang, H.-T.; Cheng, Y.-Y.; Tsai, A.Y. Self-Perceived Health and Sleep Quality of Community Older Adults after Acupunch Exercises. Am. J. Geriatr. Psychiatry 2018, 26, 511–520. [Google Scholar] [CrossRef]
- Choi, M.-J.; Sohng, K.-Y. The Effects of Floor-seated Exercise Program on Physical Fitness, Depression, and Sleep in Older Adults: A Cluster Randomized Controlled Trial. Int. J. Gerontol. 2018, 12, 116–121. [Google Scholar] [CrossRef]
- Laredo-Aguilera, J.A.; Carmona-Torres, J.M.; García-Pinillos, F.; Latorre-Román, P.Á. Effects of a 10-week functional training programme on pain, mood state, depression, and sleep in healthy older adults. Psychogeriatrics 2018, 18, 292–298. [Google Scholar] [CrossRef]
- Scullin, M.K.; Bliwise, D.L. Sleep, cognition, and normal aging: Integrating a half century of multidisciplinary research. Perspect. Psychol. Sci. J. Assoc. Psychol. Sci. 2015, 10, 97–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, S.; Yorifuji, T.; Sugiyama, M.; Ohta, T.; Ishikawa-Takata, K.; Doi, H. Does habitual physical activity prevent insomnia? A cross-sectional and longitudinal study of elderly Japanese. J. Aging Phys. Act. 2013, 21, 119–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlsen, T.; Stensvold, D.; Wisløff, U.; Ernstsen, L.; Halvorsen, T. The association of change in peak oxygen uptake with use of psychotropics in community-dwelling older adults—The Generation 100 study. BMC Geriatr. 2022, 22, 575. [Google Scholar] [CrossRef]
- Jennum, P.; Baandrup, L.; Ibsen, R.; Kjellberg, J. Increased all-cause mortality with use of psychotropic medication in dementia patients and controls: A population-based register study. Eur. Neuropsychopharmacol. 2015, 25, 1906–1913. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Satoh, H.; Miki, A.; Urushihara, H.; Sawada, Y. Medications associated with falls in older people: Systematic review of publications from a recent 5-year period. Eur. J. Clin. Pharmacol. 2015, 71, 1429–1440. [Google Scholar] [CrossRef]
- Bakken, M.S.; Engeland, A.; Engesæter, L.B.; Ranhoff, A.H.; Hunskaar, S.; Ruths, S. Risk of hip fracture among older people using anxiolytic and hypnotic drugs: A nationwide prospective cohort study. Eur. J. Clin. Pharmacol. 2014, 70, 873–880. [Google Scholar] [CrossRef] [Green Version]
- Gutsmiedl, K.; Krause, M.; Bighelli, I.; Schneider-Thoma, J.; Leucht, S. How well do elderly patients with major depressive disorder respond to antidepressants: A systematic review and single-group meta-analysis. BMC Psychiatry 2020, 20, 102. [Google Scholar] [CrossRef] [Green Version]
- Yang, P.-Y.; Ho, K.-H.; Chen, H.-C.; Chien, M.-Y. Exercise training improves sleep quality in middle-aged and older adults with sleep problems: A systematic review. J. Physiother. 2012, 58, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Mendelson, M.; Lyons, O.D.; Yadollahi, A.; Inami, T.; Oh, P.; Bradley, T.D. Effects of exercise training on sleep apnoea in patients with coronary artery disease: A randomised trial. Eur. Respir. J. 2016, 48, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Torres-Castro, R.; Vasconcello-Castillo, L.; Puppo, H.; Cabrera-Aguilera, I.; Otto-Yáñez, M.; Rosales-Fuentes, J.; Vilaró, J. Effects of Exercise in Patients with Obstructive Sleep Apnoea. Clocks Sleep 2021, 3, 227–235. [Google Scholar] [CrossRef]
- Sejbuk, M.; Mirończuk-Chodakowska, I.; Witkowska, A.M. Sleep Quality: A Narrative Review on Nutrition, Stimulants, and Physical Activity as Important Factors. Nutrients 2022, 14, 1912. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.; van Egmond, L.T.; Cedernaes, J.; Benedict, C. The role of exercise-induced peripheral factors in sleep regulation. Mol. Metab. 2020, 42, 101096. [Google Scholar] [CrossRef] [PubMed]
- Kredlow, M.A.; Capozzoli, M.C.; Hearon, B.A.; Calkins, A.W.; Otto, M.W. The effects of physical activity on sleep: A meta-analytic review. J. Behav. Med. 2015, 38, 427–449. [Google Scholar] [CrossRef] [PubMed]
- Ritsche, K.; Nindl, B.C.; Wideman, L. Exercise-Induced growth hormone during acute sleep deprivation. Physiol. Rep. 2014, 2, e12166. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Hughes, C.M.; McCullough, C.A.; Bradbury, I.; Boyde, C.; Hume, D.; Yuan, J.; Quinn, F.; McDonough, S. Acupuncture and reflexology for insomnia: A feasibility study. Acupunct. Med. 2009, 27, 163–168. [Google Scholar] [CrossRef]
- Lu, T.; Li, Y.; Pan, J.; Wu, D. Study on minimal important difference of the Pittsburgh sleep quality index based on clinical trial of traditional Chinese medicine. J. Guangzhou Univ. Tradit. Chin. Med. 2013, 30, 574–578. [Google Scholar]
- Landry, G.J.; Best, J.R.; Liu-Ambrose, T. Measuring sleep quality in older adults: A comparison using subjective and objective methods. Front. Aging Neurosci. 2015, 7, 166. [Google Scholar] [CrossRef] [Green Version]
- Jones, C.; Chen, K.-M.; Weeks, B.; Qi, M.; Moyle, W. Healthy Beat Acupunch exercise program: Validation and feasibility study for older adults with reduced physical capacity or probable sarcopenia. Explore 2021, 17, 498–504. [Google Scholar] [CrossRef]
- Tsai, H.-Y.; Chen, K.-M.; Huang, H.-T. Acupunch Exercise Program Development and Feasibility Evaluation for Older Adults. Rehabil. Nurs. J. 2020, 45, 195–203. [Google Scholar] [CrossRef]
- Anderson, E.; Durstine, J.L. Physical activity, exercise, and chronic diseases: A brief review. Sport Med. Health Sci. 2019, 1, 3–10. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Population | Group, n | Gender (M/F) | Age (Years) | BMI (kg/m2) |
|---|---|---|---|---|---|---|
| Chen et al., 2010 | Taiwan | Older adult residents of assisted living facilities | IG: 31 | NR | 75.4 ± 6.7 | NR |
| CG: 24 | NR | NR | ||||
| Hirano et al., 2011 | Japan | Community-dwelling caregivers | IG: 17 | 6/11 | 72.6 ± 4.0 | NR |
| CG: 14 | 4/10 | 75.0 ± 4.6 | NR | |||
| Oudegeest-Sander et al., 2012 | UK | Community healthy older adults | IG: 11 | 5/6 | 68 ± 2 | 25.5 ± 2.1 |
| CG: 10 | 5/5 | 70 ± 2 | 24.5 ± 2.8 | |||
| Cheung et al., 2014 | USA | Community-dwelling older women with knee osteoarthritis | IG: 11 | 5/6 | 71.9 (69.3–74.6) * | 29.1 (26.7–31.7) * |
| CG: 10 | 5/5 | 71.9 (69.0–75.0) * | 28.8 (26.0–31.7) * | |||
| Ozyemisci Taskiran et al., 2014 | Turkey | Older adults living in a nursing home | IG1 (Pilates): 18 | 3/15 | 76.2 ± 7.5 | 29.4 ± 3.5 |
| IG2 (Yoga): 18 | 3/15 | 77.2 ± 6.4 | 31.5 ± 3.6 | |||
| CG: 18 | 9/13 | 80.0 ± 6.2 | 31.0 ± 1.9 | |||
| Vaz Fragoso et al., 2015 | USA | Community-dwelling older adults with mobility limitations | IG: 818 | 271/547 | 78.7 ± 5.2 | 30.1 ± 5.7 |
| CG: 817 | 266/551 | 79.1 ± 5.2 | 30.3 ± 6.2 | |||
| Chen et al., 2016 | Taiwan | Nursing home older adults in wheelchairs | IG:64 | 32/32 | 78.8 ±7.7 | NR |
| CG: 63 | 32/31 | 80.1 ± 6.4 | NR | |||
| Hsiao et al., 2018 | Taiwan | Community-dwelling older adults | IG: 113 | 20/93 | 74.7 ± 6.0 | NR |
| CG: 119 | 30/89 | 73.9 ± 5.4 | NR | |||
| Choi and Sohng, 2018 | Republic of Korea | Older adults in community centres | IG: 33 | 3/30 | 77.6 ± 5.7 | NR |
| CG: 30 | 1/29 | 78.8 ± 5.8 | NR | |||
| Laredo-Aguilera et al., 2018 | Spain | Community healthy older adults | IG: 20 | 5/15 | 75.4 ± 5.3 | 23.4 ± 17.7 |
| CG: 18 | 5/13 | 76.4 ± 6.5 | 30.3 ± 3.9 | |||
| Bademli et al., 2019 | Turkey | Older adults living in a nursing home with a mild cognitive impairment | IG: 30 | 12/18 | 72.2 ± 7.2 | NR |
| CG: 30 | 13/17 | 70.7 ± 8.3 | NR | |||
| Falck et al., 2020 | Canada | Community older adults with probable mild cognitive impairment | IG: 48 | 25/23 | 72 ± 6 | 26.9 ± 4.2 |
| CG: 48 | 16/32 | 74 ± 5 | 26.3 ± 4.7 | |||
| Baklouti et al., 2023 | Tunisia | Community-dwelling older adults | IG: 65 | 42/23 | 65–75: 71% 76–85: 29% | NR |
| CG: 95 | 56/39 | 65–75: 78% 76–85: 22% | NR |
| Author, Year | Type of Exercise | Setting | Duration | Intensity | Frequency | Control Group |
|---|---|---|---|---|---|---|
| Chen et al., 2010 | Yoga | Assisted living facilities | 6 months | NR | 3 times per week | No intervention |
| Hirano et al., 2011 | Walking | Home | 12 weeks | Moderate | NR | No intervention |
| Oudegeest-Sander et al., 2012 | Cycling | NR | 12 months | 70–85% HRR | 3 times per week | No intervention |
| Cheung et al., 2014 | Yoga | Home and yoga studio | 8 weeks | According to the patient’s performance | 5 times per week | Wait list |
| Ozyemisci Taskiran et al., 2014 | G1: Pilates G2: Yoga | Nursing home | 8 weeks | According to the patient’s performance | 3 times per week | No intervention |
| Vaz Fragoso et al., 2015 | Multicomponent | Home- and centre-based | 24–30 months | Moderate | 5 times per week | Health education |
| Chen et al., 2016 | Resistance exercise | Nursing home | 12 months | Basic (3 m) and advanced (9 m) level | 3 times per week | No intervention |
| Hsiao et al., 2018 | Healthy beat acupunch | Community care centre | 12 months | NR | 3 times per week | Usual activities |
| Choi and Sohng, 2018 | Yoga | Senior community centre | 12 weeks | 8–14 RPE | 4 times per week | Usual care |
| Laredo-Aguilera et al., 2018 | Multicomponent | NR | 10 weeks | Self-determined to perform 8–12 rep | 3 times per week | Usual activities |
| Bademli et al., 2019 | Multicomponent | Nursing home | 20 weeks | Moderate | 3–4 times per week | No intervention |
| Falck et al., 2020 | Walking | Home | 24 months | Individually tailored | 150 min per week | Health enrichment lectures |
| Baklouti et al., 2023 | Yoga | Home | 8 weeks | NR | 2 times per week | No intervention |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solis-Navarro, L.; Masot, O.; Torres-Castro, R.; Otto-Yáñez, M.; Fernández-Jané, C.; Solà-Madurell, M.; Coda, A.; Cyrus-Barker, E.; Sitjà-Rabert, M.; Pérez, L.M. Effects on Sleep Quality of Physical Exercise Programs in Older Adults: A Systematic Review and Meta-Analysis. Clocks & Sleep 2023, 5, 152-166. https://doi.org/10.3390/clockssleep5020014
Solis-Navarro L, Masot O, Torres-Castro R, Otto-Yáñez M, Fernández-Jané C, Solà-Madurell M, Coda A, Cyrus-Barker E, Sitjà-Rabert M, Pérez LM. Effects on Sleep Quality of Physical Exercise Programs in Older Adults: A Systematic Review and Meta-Analysis. Clocks & Sleep. 2023; 5(2):152-166. https://doi.org/10.3390/clockssleep5020014
Chicago/Turabian StyleSolis-Navarro, Lilian, Olga Masot, Rodrigo Torres-Castro, Matías Otto-Yáñez, Carles Fernández-Jané, Mireia Solà-Madurell, Andrea Coda, Erika Cyrus-Barker, Mercè Sitjà-Rabert, and Laura Mónica Pérez. 2023. "Effects on Sleep Quality of Physical Exercise Programs in Older Adults: A Systematic Review and Meta-Analysis" Clocks & Sleep 5, no. 2: 152-166. https://doi.org/10.3390/clockssleep5020014