
The Durability and Efficacy of Cryopreserved Human Umbilical Cord Tissue Allograft for the Supplementation of Cartilage Defects Associated with the Sacroiliac Joint: A Case Series
Abstract
:1. Introduction
2. Case Presentation Section
2.1. Material Collection and Preperation
2.2. Study Population
2.3. Allograft Application
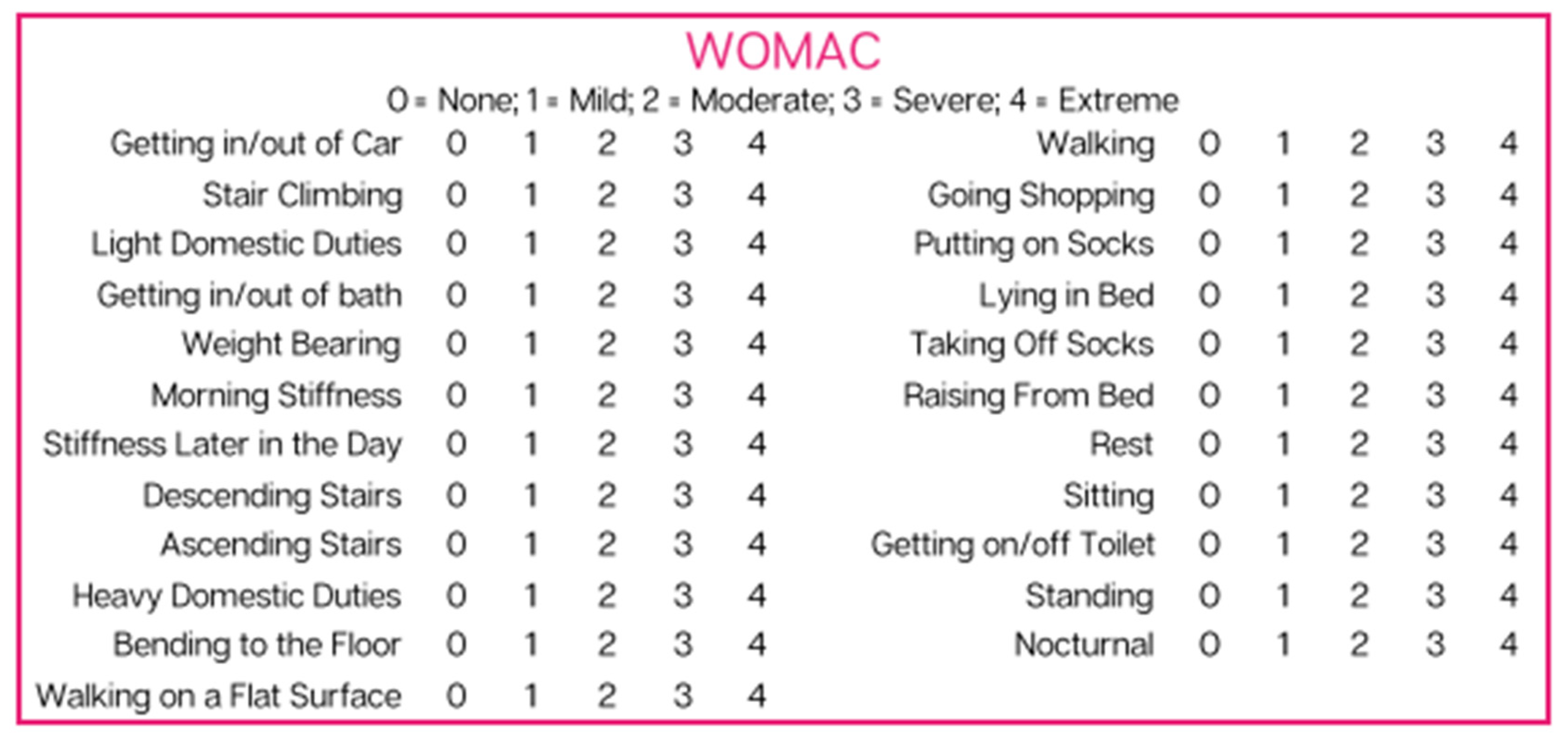
2.4. Questionnaire Composition
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Test Kits
- HBcAb: Catalog number: 06P06, Abbott Laboratories, Abbott Park, IL, USA;
- HbsAg: Catalog number: 06P02, Abbott Laboratories, Abbott Park, IL, USA;
- HCV: Catalog number: 06P04, Abbott Laboratories, Abbott Park, IL, USA;
- HIV1, HIV2, plus O: Catalog number: 06P01, Abbott Laboratories, Abbott Park, IL, USA;
- HTLV-I/II: Catalog number: 06P07, Abbott Laboratories, Abbott Park, IL, USA;
- RPR: Catalog number: 900025, Arlington Scientific, Springville, UT, USA;
- HIV1, HCV, HBV, NAT: Catalog number: 303330, 303331, 303719, 303334, 303344;
- WNV: Catalog number: 07001061190, Roche Diagnostics, Indianapolis, IN, USA.
Appendix B. Patient Reported Scores
| Gender | Age | Application Site | Initial NPRS | Initial Total WOMAC | 90-Day NPRS | 90-Day Total WOMAC | |
| Patient 1 | M | 70 | R SI | 7 | 59 | 1 | 7 |
| Patient 2 | F | 71 | R SI | 3 | 43 | 4 | 23 |
| Patient 3 | F | 71 | L SI | 4 | 44 | 4 | 23 |
| Patient 4 | F | 73 | R SI | 6 | 52 | 2 | 41 |
| Patient 5 | M | 76 | L SI | 5 | 39 | 2 | 30 |
| Patient 6 | F | 72 | L SI | 8 | 69 | 2 | 38 |
| Patient 7 | M | 74 | L SI | 4 | 47 | 1 | 32 |
| Patient 8 | M | 72 | R SI | 9 | 30 | 2 | 30 |
| Patient 9 | F | 65 | R SI | 9 | 85 | 5 | 84 |
| Patient 10 | F | 52 | L SI | 8 | 68 | 4 | 66 |
| Patient 11 | F | 65 | L SI | 9 | 83 | 4 | 81 |
| Patient 12 | M | 72 | L SI | 9 | 30 | 3 | 30 |
| Patient 13 | F | 52 | R SI | 8 | 68 | 5 | 68 |
| Patient 14 | M | 76 | R SI | 2 | 19 | 1 | 12 |
| Patient 15 | F | 78 | L SI | 8 | 75 | 2 | 23 |
| Patient 16 | M | 66 | L SI | 6 | 36 | 4 | 23 |
| Patient 17 | M | 71 | L SI | 8 | 64 | 4 | 40 |
| Patient 18 | M | 76 | L SI | 4 | 46 | 3 | 44 |
| Patient 19 | M | 77 | L SI | 6 | 46 | 3 | 40 |
| Patient 20 | F | 76 | L SI | 6 | 54 | 9 | 68 |
| Patient 21 | F | 74 | L SI | 5 | 39 | 4 | 28 |
| Patient 22 | M | 65 | R SI | 6 | 71 | 4 | 45 |
| Patient 23 | M | 71 | R SI | 10 | 28 | 4 | 44 |
| Patient 24 | M | 75 | R SI | 10 | 36 | 1 | 31 |
| Patient 25 | M | 69 | R SI | 5 | 45 | 3 | 46 |
| Patient 26 | F | 77 | L SI | 6 | 65 | 4 | 35 |
| Patient 27 | F | 74 | L SI | 7 | 61 | 4 | 65 |
| Patient 28 | F | 70 | L SI | 7 | 66 | 8 | 74 |
| Patient 29 | F | 65 | R SI | 5 | 84 | 4 | 72 |
| Patient 30 | M | 72 | R SI | 2 | 30 | 0 | 2 |
| Patient 31 | M | 65 | R SI | 7 | 60 | 0 | 18 |
| Patient 32 | F | 77 | R SI | 9 | 92 | 10 | 86 |
| Patient 33 | F | 79 | L SI | 10 | 92 | 9 | 78 |
| Patient 34 | F | 84 | L SI | 8 | 73 | 3 | 12 |
| Patient 35 | F | 72 | R SI | 5 | 64 | 3 | 46 |
| Patient 36 | M | 69 | R SI | 6 | 63 | 5 | 60 |
| Patient 37 | M | 75 | L SI | 8 | 45 | 8 | 43 |
| Patient 38 | F | 86 | L SI | 8 | 59 | 4 | 59 |
References
- Raj, M.A.; Ampat, G.; Varacallo, M. Sacroiliac Joint Pain. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470299 (accessed on 4 September 2022).
- Kampen, W.U.; Tillmann, B. Age-related changes in the articular cartilage of human sacroiliac joint. Anat. Embryol. 1998, 198, 505–513. [Google Scholar] [CrossRef]
- Ou-Yang, D.C.; York, P.J.; Kleck, C.J.; Patel, V.V. Diagnosis and Management of Sacroiliac Joint Dysfunction. J. Bone Jt. Surg. 2017, 99, 2027–2036. [Google Scholar] [CrossRef] [PubMed]
- Dreyfuss, P.; Dreyer, S.J.; Cole, A.; Mayo, K. Sacroiliac Joint Pain. J. Am. Acad. Orthop. Surg. 2004, 12, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.W. Sacroiliac Joint Dysfunction: Evaluation and Management. Orthop. Nurs. 2011, 30, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Calvillo, O.; Skaribas, I.; Turnipseed, J. Anatomy and pathophysiology of the sacroiliac joint. Curr. Rev. Pain 2000, 4, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Kompel, A.J.; Roemer, F.W.; Murakami, A.M.; Diaz, L.E.; Crema, M.D.; Guermazi, A. Intra-articular Corticosteroid Injections in the Hip and Knee: Perhaps Not as Safe as We Thought? Radiology 2019, 293, 656–663. [Google Scholar] [CrossRef]
- Ostergaard, M.; Halberg, P. Intra-Articular Corticosteroids in Arthritic Disease: A guide to treatment. Biodrugs 1998, 9, 95–103. [Google Scholar] [CrossRef]
- Stone, S.; Malanga, G.A.; Capella, T. Corticosteroids: Review of the history, the effectiveness, and adverse effects in the treatment of joint pain. Pain Physician 2021, 24, S233–S246. [Google Scholar]
- Jüni, P.; Hari, R.; Rutjes, A.W.; Fischer, R.; Silletta, M.G.; Reichenbach, S.; da Costa, B.R. Intra-articular corticosteroid for knee osteoarthritis. Cochrane Database Syst. Rev. 2015, 2015, CD005328. [Google Scholar] [CrossRef] [Green Version]
- Stanbury, R.M.; Graham, E.M. Systemic corticosteroid therapy—Side effects and their management. Br. J. Ophthalmol. 1998, 82, 704–708. [Google Scholar] [CrossRef] [Green Version]
- Hanly, J.G.; Mitchell, M.; Macmillan, L.; Mosher, D.; Sutton, E. Efficacy of sacroiliac corticosteroid injections in patients with inflammatory spondyloarthropathy: Results of a 6 month controlled study. J. Rheumatol. 2000, 27, 719–722. [Google Scholar] [PubMed]
- Migliore, A.; Procopio, S. Effectiveness and utility of hyaluronic acid in osteoarthritis. Clin. Cases Miner. Bone Metab. 2015, 12, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Heiney, J.; Capobianco, R.; Cher, D. A systematic review of minimally invasive sacroiliac joint fusion utilizing a lateral transarticular technique. Int. J. Spine Surg. 2015, 9, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, K.Y.; Lee, J.S.; Kim, K.W. Degeneration of Sacroiliac Joint After Instrumented Lumbar or Lumbosacral Fusion: A Prospective Cohort Study Over Five-Year Follow-up. Spine 2008, 33, 1192–1198. [Google Scholar] [CrossRef] [Green Version]
- Ackerman, S.J.; Polly, D.W., Jr.; Knight, T.; Schneider, K.; Holt, T.; Cummings, J. Comparison of the costs of nonoperative care to minimally invasive surgery for sacroiliac joint disruption and degenerative sacroiliitis in a United States Medicare population: Potential economic implications of a new minimally-invasive technology. Clin. Outcomes Res. 2013, 5, 575–587. [Google Scholar] [CrossRef] [Green Version]
- Schoell, K.; Buser, Z.; Jakoi, A.; Pham, M.; Patel, N.N.; Hsieh, P.C.; Liu, J.C.; Wang, J.C. Postoperative complications in patients undergoing minimally invasive sacroiliac fusion. Spine J. 2016, 16, 1324–1332. [Google Scholar] [CrossRef]
- Wampler, A.T.; Pace, L.H.; Thorne, J.M. Intra-Articular Injections of Wharton’s Jelly Allograft Combined with Amniotic Membrane Allograft are Safe and Effective for Relieving Knee Pain Associated with Osteoarthritis; A Retrospective Case Report. Elite Integr. Med. J. 2021, 4, 13. [Google Scholar] [CrossRef]
- Gupta, A.; El-Amin, S.F.; Levy, H.J.; Sze-Tu, R.; Ibim, S.E.; Maffulli, N. Umbilical cord-derived Wharton’s jelly for regenerative medicine applications. J. Orthop. Surg. Res. 2020, 15, 49. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.M.; Purita, J.R.; Shou, J.; Barrett, T.C. Three-Dimensional Electron Microscopy of Human Umbilical Cord Tissue Allograft Pre and Post Processing: A Literature Comparison. J. Biomed. Res. Environ. Sci. 2022, 3, 934–940. Available online: https://www.jelsciences.com/articles/jbres1535.pdf. [CrossRef]
- Timmons, R.B.; Sugaya, K.; Bane, L.D. Homologous Use of Allogeneic Umbilical Cord Tissue to Reduce Knee Pain and Improve Knee Function. Life 2022, 12, 260. [Google Scholar] [CrossRef]
- Gupta, A.; Maffulli, N.; Rodriguez, H.C.; Carson, E.W.; Bascharon, R.A.; Delfino, K.; Levy, H.J.; El-Amin, S.F. Safety and efficacy of umbilical cord-derived Wharton’s jelly compared to hyaluronic acid and saline for knee osteoarthritis: Study protocol for a randomized, controlled, single-blind, multi-center trial. J. Orthop. Surg. Res. 2021, 16, 352. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Liu, S.; Bai, Y.; Lu, S.; Peng, J.; Zhang, L.; Huang, J.; Zhao, B.; Xu, W.; Guo, Q. hWJECM-Derived Oriented Scaffolds with Autologous Chondrocytes for Rabbit Cartilage Defect Repairing. Tissue Eng. Part A 2018, 24, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.M.; Sheinkop, M.B.; Barrett, T.C. Evaluation of the Efficacy of Cryopreserved Human Umbilical Cord Tissue Allografts to Augment Functional and Pain Outcome Measures in Patients with Knee Osteoarthritis: An Observational Data Collection Study. Physiologia 2022, 2, 109–120. [Google Scholar] [CrossRef]
- Lindsey, D.P.; Kiapour, A.; Yerby, S.A.; Goel, V.K. Sacroiliac Joint Fusion Minimally Affects Adjacent Lumbar Segment Motion: A Finite Element Study. Int. J. Spine Surg. 2015, 9, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Scale | Average Initial Score | Average Final Score | Percent Change |
|---|---|---|---|
| NPRS | 6.7 | 3.6 | 42% decrease |
| WOMAC | 56.1 | 43.3 | 22% decrease |
| ANOVA | ||||||
|---|---|---|---|---|---|---|
| Source of Variation | Sum of Squares | df | Mean Square | F-value | p-value | |
| WOMAC | 3069.59210 | 1 | 3069.59 | 7.06082 | 0.00964 | significant |
| Gender | Avg. Initial NPRS | Avg. Final NPRS | % Change NPRS | Avg. Initial WOMAC | Avg. Final WOMAC | % Change WOMAC |
|---|---|---|---|---|---|---|
| Females | 6.9 | 4.3 | 37% decrease | 66.4 | 51.2 | 22.9% decrease |
| Males | 6.3 | 2.7 | 57% decrease | 44.1 | 32 | 27.4% decrease |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, A.; Shou, J.; Traina, S.A.; Barrett, T. The Durability and Efficacy of Cryopreserved Human Umbilical Cord Tissue Allograft for the Supplementation of Cartilage Defects Associated with the Sacroiliac Joint: A Case Series. Reports 2023, 6, 12. https://doi.org/10.3390/reports6010012
Lai A, Shou J, Traina SA, Barrett T. The Durability and Efficacy of Cryopreserved Human Umbilical Cord Tissue Allograft for the Supplementation of Cartilage Defects Associated with the Sacroiliac Joint: A Case Series. Reports. 2023; 6(1):12. https://doi.org/10.3390/reports6010012
Chicago/Turabian StyleLai, Albert, Jon Shou, Steve A. Traina, and Tyler Barrett. 2023. "The Durability and Efficacy of Cryopreserved Human Umbilical Cord Tissue Allograft for the Supplementation of Cartilage Defects Associated with the Sacroiliac Joint: A Case Series" Reports 6, no. 1: 12. https://doi.org/10.3390/reports6010012