
The Impact of Anxiety and Depression in Chronic Obstructive Pulmonary Disease

 , , , ,
, , , ,
Abstract
:Highlights
- COPD patients with comorbid anxiety or depression experience more acute exacerbations, incidences of rehospitalization, and carry a higher risk of mortality than COPD patients without these comorbidities.
- COPD patients benefit from non-pharmacological and pharmacological intervention based on severity of depression.
- Ongoing investigation and research are necessary to ensure appropriate screening, diagnosis, and management of COPD patient with anxiety and/or depression.
- Adequate treatment of COPD patients with comorbid mental health conditions can decrease the burden on the healthcare system by improving symptomatology and rehospitalizations.
Abstract
1. Introduction
2. Epidemiology and Prevalence
3. Pathophysiology
4. Clinical Features
5. Clinical Implication of Anxiety and Depression on Patients with COPD
5.1. Impact on Acute Exacerbation of COPD
5.2. Impact on Mortality
5.3. Impact on Medication Adherence
5.4. Impact on Pulmonary Rehabilitaion
5.5. Impact on Quality of Life
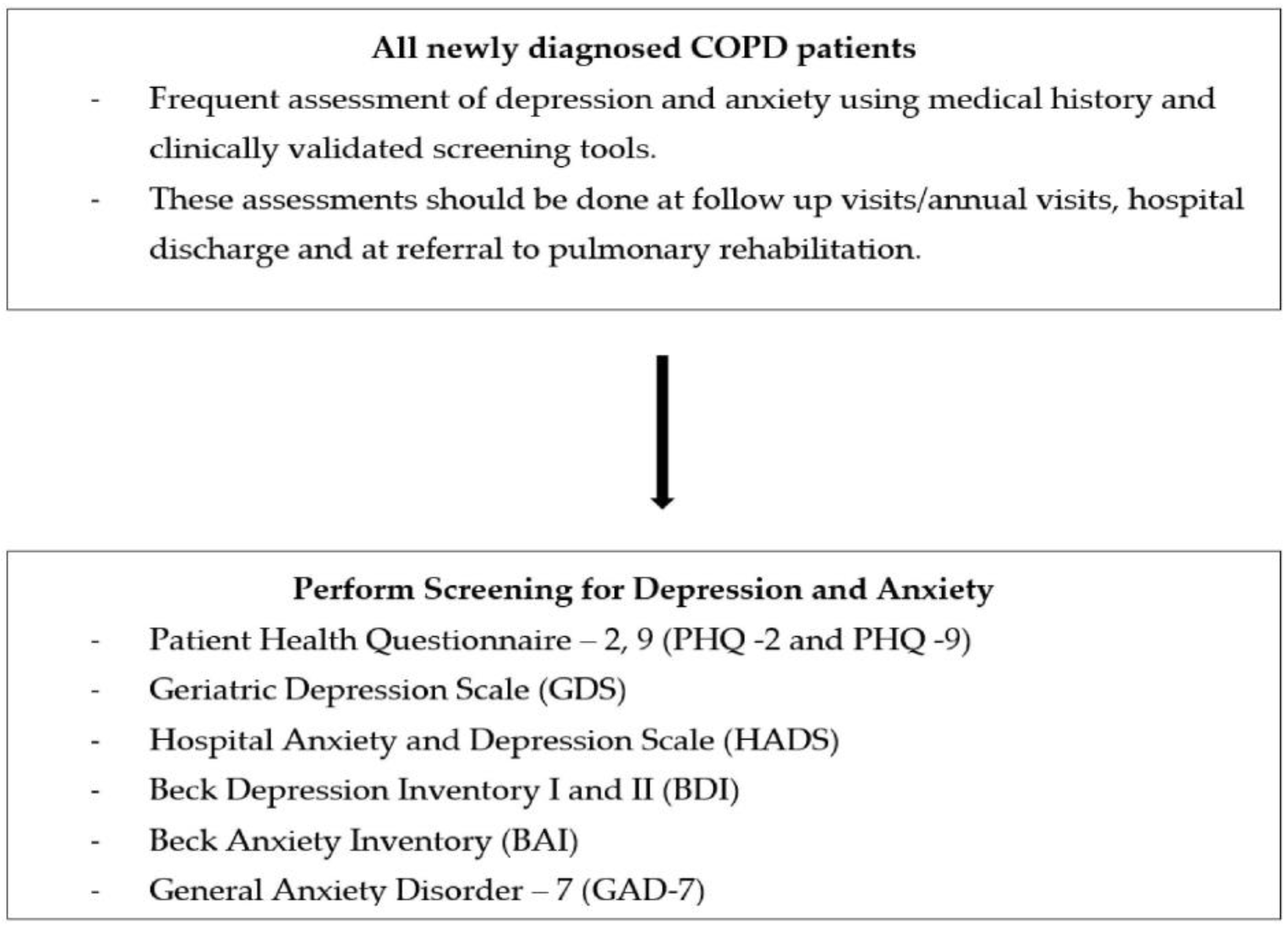
6. Screening and Diagnosis
- Patient Health Questionnaire-2, 9 (PHQ -2 and 9): widely used with 2 and 9 item versions [53].
- Beck Depression Inventory (BDI): 21-item self-reported questionnaire [54].
- Geriatric Depression scale (GDS) [55].
- Centre for Epidemiological studies scale on Depression (CES-D): score of 16 or higher on the CES-D is considered a possible case for depression [56].
- Hospital and Anxiety Depression Scale (HADS) [57].
- Brief Assessment Schedule Depression Cards (BASDEC) [45].
- COPD Anxiety Questionnaire (CAF): early identification of COPD-related anxiety [60].
- Patient Health Questionnaire-3 (PHQ-3) [61].
- Generalized Anxiety Disorder 7-item (GAD-7) scale: scores seven common anxiety symptoms [63].
- General Health Questionnaire-version 20 (GHQ-20) [57].
- Beck Anxiety Inventory (BAI): 21-item self-report questionnaire [54].
7. Management
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Quaderi, S.A.; Hurst, J.R. The unmet global burden of COPD. Glob. Health Epidemiol. Genom. 2018, 3, e4. [Google Scholar] [CrossRef] [Green Version]
- Press, V.G.; Konetzka, R.T.; White, S.R. Insights about the economic impact of chronic obstructive pulmonary disease readmissions post implementation of the hospital readmission reduction program. Curr. Opin. Pulm. Med. 2018, 24, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Safiri, S.; Carson-Chahhoud, K.; Noori, M.; Nejadghaderi, S.A.; Sullman, M.J.M.; Ahmadian Heris, J.; Ansarin, K.; Mansournia, M.A.; Collins, G.S.; Kolahi, A.A.; et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: Results from the Global Burden of Disease Study 2019. BMJ 2022, 378, e069679. [Google Scholar] [CrossRef] [PubMed]
- Zareifopoulos, N.; Bellou, A.; Spiropoulou, A.; Spiropoulos, K. Prevalence, Contribution to Disease Burden and Management of Comorbid Depression and Anxiety in Chronic Obstructive Pulmonary Disease: A Narrative Review. J. Obstr. Pulm. Dis. 2019, 16, 406–417. [Google Scholar] [CrossRef]
- Atlantis, E.; Fahey, P.; Cochrane, B.; Smith, S. Bidirectional associations between clinically relevant depression or anxiety and COPD: A systematic review and meta-analysis. Chest 2013, 144, 766–777. [Google Scholar] [CrossRef]
- Pumar, M.I.; Gray, C.R.; Walsh, J.R.; Yang, I.A.; Rolls, T.A.; Ward, D.L. Anxiety and depression-Important psychological comorbidities of COPD. J. Thorac. Dis. 2014, 6, 1615–1631. [Google Scholar] [CrossRef] [PubMed]
- Schuler, M.; Wittmann, M.; Faller, H.; Schultz, K. The interrelations among aspects of dyspnea and symptoms of depression in COPD patients—A network analysis. J. Affect. Disord. 2018, 240, 33–40. [Google Scholar] [CrossRef]
- Adeloye, D.; Song, P.; Zhu, Y.; Campbell, H.; Sheikh, A.; Rudan, I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: A systematic review and modelling analysis. Lancet. Respir. Med. 2022, 10, 447–458. [Google Scholar] [CrossRef]
- Schneider, C.; Jick, S.S.; Bothner, U.; Meier, C.R. COPD and the risk of depression. Chest 2010, 137, 341–347. [Google Scholar] [CrossRef]
- Van Manen, J.G.; Bindels, P.J.; Dekker, F.W.; CJ, I.J.; van der Zee, J.S.; Schadé, E. Risk of depression in patients with chronic obstructive pulmonary disease and its determinants. Thorax 2002, 57, 412–416. [Google Scholar] [CrossRef] [Green Version]
- Blakemore, A.; Dickens, C.; Guthrie, E.; Bower, P.; Kontopantelis, E.; Afzal, C.; Coventry, P.A. Depression and anxiety predict health-related quality of life in chronic obstructive pulmonary disease: Systematic review and meta-analysis. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 501–512. [Google Scholar] [CrossRef] [Green Version]
- Martucci, V.L.; Richmond, B.; Davis, L.K.; Blackwell, T.S.; Cox, N.J.; Samuels, D.; Velez Edwards, D.; Aldrich, M.C. Fate or coincidence: Do COPD and major depression share genetic risk factors? Hum. Mol. Genet. 2021, 30, 619–628. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Li, X. Risk Factors for Depression in Patients with Chronic Obstructive Pulmonary Disease. Med. Sci. Monit. 2018, 24, 1417–1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
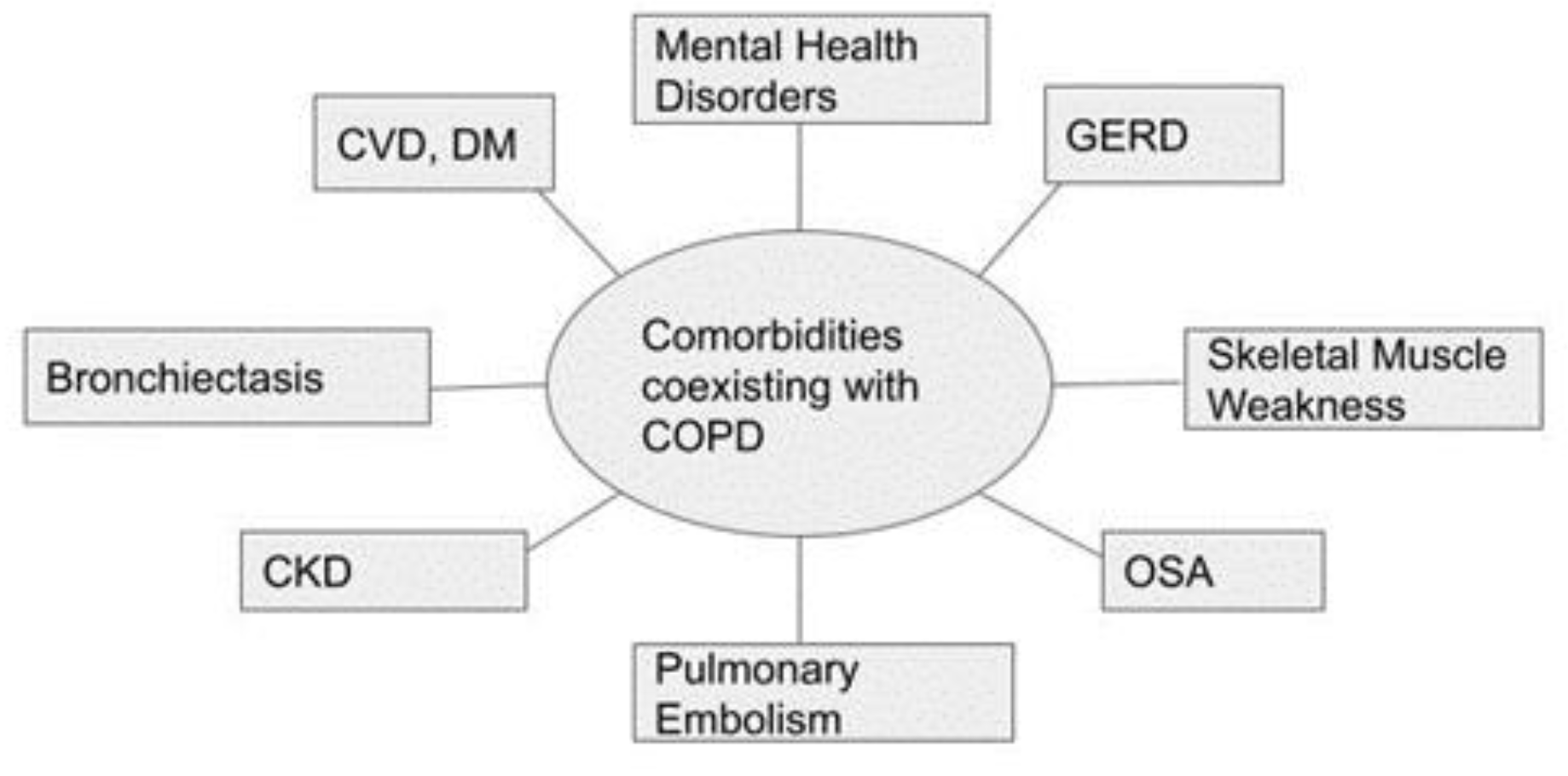
- Chatila, W.M.; Thomashow, B.M.; Minai, O.A.; Criner, G.J.; Make, B.J. Comorbidities in chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2008, 5, 549–555. [Google Scholar] [CrossRef]
- Gunasekaran, K.; Murthi, S.; Elango, K.; Rahi, M.S.; Thilagar, B.; Ramalingam, S.; Voruganti, D.; Paramasivam, V.K.; Kolandaivel, K.P.; Arora, A.; et al. The Impact of Diabetes Mellitus in Patients with Chronic Obstructive Pulmonary Disease (COPD) Hospitalization. J. Clin. Med. 2021, 10, 235. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Alexopoulos, G.S. Depression and anxiety in patients with COPD. Eur. Respir. Rev. 2014, 23, 345–349. [Google Scholar] [CrossRef] [Green Version]
- Hogea, S.P.; Tudorache, E.; Fildan, A.P.; Fira-Mladinescu, O.; Marc, M.; Oancea, C. Risk factors of chronic obstructive pulmonary disease exacerbations. Clin. Respir. J. 2020, 14, 183–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pooler, A.; Beech, R. Examining the relationship between anxiety and depression and exacerbations of COPD which result in hospital admission: A systematic review. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 315–330. [Google Scholar] [CrossRef] [Green Version]
- Radell, M.L.; Abo Hamza, E.G.; Daghustani, W.H.; Perveen, A.; Moustafa, A.A. The Impact of Different Types of Abuse on Depression. Depress. Res. Treat. 2021, 2021, 6654503. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, A.M.; Baldwin, R.C.; Connolly, M.J. Prevalence of sub-threshold depression in elderly patients with chronic obstructive pulmonary disease. Int. J. Geriatr. Psychiatry 2003, 18, 412–416. [Google Scholar] [CrossRef]
- Miravitlles, M.; Molina, J.; Quintano, J.A.; Campuzano, A.; Pérez, J.; Roncero, C. Factors associated with depression and severe depression in patients with COPD. Respir. Med. 2014, 108, 1615–1625. [Google Scholar] [CrossRef] [Green Version]
- Ng, T.P.; Niti, M.; Tan, W.C.; Cao, Z.; Ong, K.C.; Eng, P. Depressive symptoms and chronic obstructive pulmonary disease: Effect on mortality, hospital readmission, symptom burden, functional status, and quality of life. Arch. Intern. Med. 2007, 167, 60–67. [Google Scholar] [CrossRef]
- Patton, G.C.; Hibbert, M.; Rosier, M.J.; Carlin, J.B.; Caust, J.; Bowes, G. Is smoking associated with depression and anxiety in teenagers? Am. J. Public Health 1996, 86, 225–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauwels, R.A.; Buist, A.S.; Calverley, P.M.; Jenkins, C.R.; Hurd, S.S. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am. J. Respir. Crit. Care. Med. 2001, 163, 1256–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tselebis, A.; Bratis, D.; Kosmas, E.; Harikiopoulou, M.; Theodorakopoulou, E.; Dumitru, S.; Moussas, G.; Karkanias, A.; Ilias, I.; Siafakas, N.; et al. Psychological symptom patterns and vital exhaustion in outpatients with chronic obstructive pulmonary disease. Ann. Gen. Psychiatry 2011, 10, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, A.; Barusso, M.; De Brandt, J.; Quadflieg, K.; Haesevoets, S.; Daenen, M.; Thomeer, M.; Ruttens, D.; Marques, A.; Burtin, C. Impact of acute exacerbations of COPD on patients’ health status beyond pulmonary function: A scoping review. Pulmonology 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Gestoso, S.; García-Sanz, M.T.; Carreira, J.M.; Salgado, F.J.; Calvo-Álvarez, U.; Doval-Oubiña, L.; Camba-Matos, S.; Peleteiro-Pedraza, L.; González-Pérez, M.A.; Penela-Penela, P.; et al. Impact of anxiety and depression on the prognosis of copd exacerbations. BMC. Pulm. Med. 2022, 22, 169. [Google Scholar] [CrossRef]
- Lecheler, L.; Richter, M.; Franzen, D.P.; Rampini, S.K.; Cheetham, M.; Jenewein, J.; Battegay, E.; Nowak, A. The frequent and underrecognised co-occurrence of acute exacerbated COPD and depression warrants screening: A systematic review. Eur. Respir. Rev. 2017, 26, 170026. [Google Scholar] [CrossRef] [Green Version]
- Iyer, A.S.; Bhatt, S.P.; Garner, J.J.; Wells, J.M.; Trevor, J.L.; Patel, N.M.; Kirkpatrick, d.; Williams, J.C.; Dransfield, M.T. Depression Is Associated with Readmission for Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Ann. Am. Thorac. Soc. 2016, 13, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Laurin, C.; Moullec, G.; Bacon, S.L.; Lavoie, K.L. Impact of anxiety and depression on chronic obstructive pulmonary disease exacerbation risk. Am. J. Respir. Crit. Care. Med. 2012, 185, 918–923. [Google Scholar] [CrossRef]
- Ouaalaya, E.H.; Falque, L.; Dupis, J.M.; Sabatini, M.; Bernady, A.; Nguyen, L.; Ozier, A.; Nocent-Ejnaini, C.; Le Guillou, F.; Molimard, M.; et al. Susceptibility to frequent exacerbation in COPD patients: Impact of the exacerbations history, vaccinations and comorbidities? Respir. Med. 2020, 169, 106018. [Google Scholar] [CrossRef]
- Stage, K.B.; Middelboe, T.; Pisinger, C. Depression and chronic obstructive pulmonary disease (COPD). Impact on survival. Acta. Psychiatr. Scand. 2005, 111, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Abrams, T.E.; Vaughan-Sarrazin, M.; Van der Weg, M.W. Acute exacerbations of chronic obstructive pulmonary disease and the effect of existing psychiatric comorbidity on subsequent mortality. Psychosomatics 2011, 52, 441–449. [Google Scholar] [CrossRef] [PubMed]
- De Voogd, J.N.; Wempe, J.B.; Koëter, G.H.; Postema, K.; van Sonderen, E.; Ranchor, A.V.; Coyne, J.C.; Sanderman, R. Depressive symptoms as predictors of mortality in patients with COPD. Chest 2009, 135, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Fan, V.S.; Ramsey, S.D.; Giardino, N.D.; Make, B.J.; Emery, C.F.; Diaz, P.T.; Benditt, J.O.; Mosenifar, Z.; McKenna, R., Jr.; Curtis, J.L.; et al. Sex, depression, and risk of hospitalization and mortality in chronic obstructive pulmonary disease. Arch. Intern. Med. 2007, 167, 2345–2353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crockett, A.J.; Cranston, J.M.; Moss, J.R.; Alpers, J.H. The impact of anxiety, depression and living alone in chronic obstructive pulmonary disease. Qual. Life. Res. 2002, 11, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Schoepf, D.; Heun, R. Anxiety disorders and physical comorbidity: Increased prevalence but reduced relevance of specific risk factors for hospital-based mortality during a 12.5-year observation period in general hospital admissions. Eur. Arch. Psychiatry. Clin. Neurosci. 2015, 265, 387–398. [Google Scholar] [CrossRef]
- Vikjord, S.A.A.; Brumpton, B.M.; Mai, X.M.; Vanfleteren, L.; Langhammer, A. The association of anxiety and depression with mortality in a COPD cohort. The HUNT study, Norway. Respir. Med. 2020, 171, 106089. [Google Scholar] [CrossRef]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression is a risk factor for noncompliance with medical treatment: Meta-analysis of the effects of anxiety and depression on patient adherence. Arch. Intern. Med. 2000, 160, 2101–2107. [Google Scholar] [CrossRef] [Green Version]
- Khdour, M.R.; Hawwa, A.F.; Kidney, J.C.; Smyth, B.M.; McElnay, J.C. Potential risk factors for medication non-adherence in patients with chronic obstructive pulmonary disease (COPD). Eur. J. Clin. Pharmacol. 2012, 68, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Van Boven, J.F.; Chavannes, N.H.; van der Molen, T.; Rutten-van Mölken, M.P.; Postma, M.J.; Vegter, S. Clinical and economic impact of non-adherence in COPD: A systematic review. Respir. Med. 2014, 108, 103–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourbeau, J.; Bartlett, S.J. Patient adherence in COPD. Thorax 2008, 63, 831–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Leupoldt, A.; Taube, K.; Lehmann, K.; Fritzsche, A.; Magnussen, H. The impact of anxiety and depression on outcomes of pulmonary rehabilitation in patients with COPD. Chest 2011, 140, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Tsiligianni, I.; Kocks, J.; Tzanakis, N.; Siafakas, N.; van der Molen, T. Factors that influence disease-specific quality of life or health status in patients with COPD: A review and meta-analysis of Pearson correlations. Prim. Care. Respir. J. 2011, 20, 257–268. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Baldwin, R.C.; Connolly, M.J. Depression and anxiety in elderly outpatients with chronic obstructive pulmonary disease: Prevalence, and validation of the BASDEC screening questionnaire. Int. J. Geriatr. Psychiatry 2000, 15, 1090–1096. [Google Scholar] [CrossRef] [PubMed]
- Felker, B.; Katon, W.; Hedrick, S.C.; Rasmussen, J.; McKnight, K.; McDonnell, M.B.; Fihn, S.D. The association between depressive symptoms and health status in patients with chronic pulmonary disease. Gen. Hosp. Psychiatry 2001, 23, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.; Geist, R.; Goldstein, R.S.; Lacasse, Y. Anxiety and depression in end-stage COPD. Eur. Respir. J. 2008, 31, 667–677. [Google Scholar] [CrossRef] [Green Version]
- Covino, N.A.; Dirks, J.F.; Kinsman, R.A.; Seidel, J.V. Patterns of depression in chronic illness. Psychother. Psychosom. 1982, 37, 144–153. [Google Scholar] [CrossRef]
- Janssen, D.J.A.; Spruit, M.A.; Schols, J.; Cox, B.; Nawrot, T.S.; Curtis, J.R.; Wouters, E.F.M. Predicting changes in preferences for life-sustaining treatment among patients with advanced chronic organ failure. Chest 2012, 141, 1251–1259. [Google Scholar] [CrossRef]
- Maurer, J.; Rebbapragada, V.; Borson, S.; Goldstein, R.; Kunik, M.E.; Yohannes, A.M.; Hanania, N.A. Anxiety and depression in COPD: Current understanding, unanswered questions, and research needs. Chest 2008, 134, 43s–56s. [Google Scholar] [CrossRef] [Green Version]
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care. Med. 2013, 187, 347–365. [Google Scholar] [CrossRef]
- Sundh, J.; Ställberg, B.; Lisspers, K.; Kämpe, M.; Janson, C.; Montgomery, S. Comparison of the COPD Assessment Test (CAT) and the Clinical COPD Questionnaire (CCQ) in a Clinical Population. COPD 2016, 13, 57–65. [Google Scholar] [CrossRef]
- Arroll, B.; Goodyear-Smith, F.; Crengle, S.; Gunn, J.; Kerse, N.; Fishman, T.; Falloon, K.; Hatcher, S. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann. Fam. Med. 2010, 8, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Julian, L.J.; Gregorich, S.E.; Earnest, G.; Eisner, M.D.; Chen, H.; Blanc, P.D.; Yelin, E.H.; Katz, P.P. Screening for depression in chronic obstructive pulmonary disease. Copd 2009, 6, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Radloff, L.S. The CES-D Scale. A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Bratås, O.; Grønning, K.; Forbord, T. Psychometric properties of the Hospital Anxiety and Depression Scale and The General Health Questionnaire-20 in COPD inpatients. Scand. J. Caring. Sci. 2014, 28, 413–420. [Google Scholar] [CrossRef]
- Willgoss, T.G.; Goldbart, J.; Fatoye, F.; Yohannes, A.M. The development and validation of the anxiety inventory for respiratory disease. Chest 2013, 144, 1587–1596. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, A.M.; Dryden, S.; Hanania, N.A. The Responsiveness of the Anxiety Inventory for Respiratory Disease Scale Following Pulmonary Rehabilitation. Chest 2016, 150, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Kühl, K.; Kuhn, C.; Kenn, K.; Rief, W. The COPD-Anxiety-Questionnaire (CAF): A new instrument to assess illness specific anxiety in COPD patients. Psychother. Psychosom. Med. Psychol. 2011, 61, e1–e9. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary Care Evaluation of Mental Disorders. J. Am. Med. Assoc. 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamburrino, M.B.; Lynch, D.J.; Nagel, R.W.; Smith, M.K. Primary care evaluation of mental disorders (PRIME-MD) screening for minor depressive disorder in primary care. Prim. Care. Companion. J. Clin. Psychiatry 2009, 11, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbody, S.; House, A.O.; Sheldon, T.A. Screening and case finding instruments for depression. Cochrane Database Syst. Rev. 2005, 2005, Cd002792. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Kaplan, A.; Hanania, N.A. Anxiety and Depression in Chronic Obstructive Pulmonary Disease: Recognition and Management. Cleve. Clin. J. Med. 2018, 85 (Suppl. S1), S11–S18. [Google Scholar] [CrossRef] [Green Version]
- Pollok, J.; van Agteren, J.E.; Esterman, A.J.; Carson-Chahhoud, K.V. Psychological therapies for the treatment of depression in chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2019, 3, Cd012347. [Google Scholar] [CrossRef]
- McCarthy, B.; Casey, D.; Devane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, 2, CD003793. [Google Scholar] [CrossRef]
- Kunik, M.E.; Braun, U.; Stanley, M.A.; Wristers, K.; Molinari, V.; Stoebner, D.; Orengo, C.A. One session cognitive behavioural therapy for elderly patients with chronic obstructive pulmonary disease. Psychol. Med. 2001, 31, 717–723. [Google Scholar] [CrossRef]
- Ma, R.C.; Yin, Y.Y.; Wang, Y.Q.; Liu, X.; Xie, J. Effectiveness of cognitive behavioural therapy for chronic obstructive pulmonary disease patients: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2020, 38, 101071. [Google Scholar] [CrossRef]
- Usmani, Z.A.; Carson, K.V.; Heslop, K.; Esterman, A.J.; De Soyza, A.; Smith, B.J. Psychological therapies for the treatment of anxiety disorders in chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2017, 3, Cd010673. [Google Scholar] [CrossRef] [PubMed]
- Farver-Vestergaard, I.; Danielsen, J.T.T.; Løkke, A.; Zachariae, R. Psychosocial Intervention in Chronic Obstructive Pulmonary Disease: Meta-Analysis of Randomized Controlled Trials. Psychosom. Med. 2022, 84, 347–358. [Google Scholar] [CrossRef]
- Pollok, J.; van Agteren, J.E.; Carson-Chahhoud, K.V. Pharmacological interventions for the treatment of depression in chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2018, 12, Cd012346. [Google Scholar] [CrossRef] [PubMed]
- Fritzsche, A.; Clamor, A.; von Leupoldt, A. Effects of medical and psychological treatment of depression in patients with COPD—A review. Respir. Med. 2011, 105, 1422–1433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vozoris, N.T.; Wang, X.; Austin, P.C.; Stephenson, A.L.; O’Donnell, D.E.; Gershon, A.S.; Gill, S.S.; Rochon, P.A. Serotonergic antidepressant use and morbidity and mortality among older adults with COPD. Eur. Respir. J. 2018, 52, 1800475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stage, K.B.; Middelboe, T.; Stage, T.B.; Sørensen, C.H. Depression in COPD—Management and quality of life considerations. Int. J. Chron. Obstruct. Pulmon. Dis. 2006, 1, 315–320. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Non-Pharmacologic Interventions |
|---|
| Cognitive Behavioral Therapy (CBT) Exercise |
| Education |
| Relaxation techniques (Breathing exercises, sequential muscle relaxation, hypnosis, mindfulness meditation) |
| Home-based psycho-educational intervention using telephone health mentoring |
| Lifestyle modification (smoking cessation, nutritional foods, quality sleep and physical exercise) |
| Multidisciplinary pulmonary rehabilitation |
| Yoga |
| Counseling |
| Collaborative care model |
| Social support and respite care for caregivers |
| Pharmacologic Interventions |
|---|
| Norepinephrine and dopamine-reuptake inhibitor: Bupropion |
| Norepinephrine and serotonin modulator: Mirtazapine |
| Atypical antipsychotics |
| Tricyclic antidepressants: Nortriptyline |
| Selective Serotonin-reuptake inhibitors (SSRIs) |
| NCT Identifier and/or Author | Study Design | Intervention | Primary Outcome Measurement Tool |
|---|---|---|---|
| NCT04868357 | Trial: HYPNOBPCO_2; 2-arm, cluster-randomized, statistician-blinded superiority monocenter trial, 100 participants with Hypnosis” (treatment) and “Relaxation” (active control). “Hypnosis” will consist Pulmonary Rehabilitation Program, supplemented by two educational sessions for teaching self-hypnosis. Relaxation group will be identical, except standard relaxation exercises will be taught instead of hypnosis. | Hypnosis as a tool to manage anxiety and dyspnea post pulmonary rehabilitation program (PRP). | State-Trait Anxiety Inventory (STAI-6) Hospital Anxiety and Depression inventory (HADS) Multidimensional Dyspnea Profile (MDP) |
| NCT05506202 | Randomized clinical trial; n = 36 | Treatment group: Basic body awareness therapy Control group: basic and advanced respiratory physiotherapy interventions | Modified Medical Research Council scale for breathlessness Dyspnoea-12 (Chinese version) St. George’s Respiratory Questionnaire (Chinese version) COPD Self-Efficacy Scale (CSES) (Chinese version) 6 min walking test |
| NCT04860375 | Prospective, open label, cohort study; n = 110 | Treatment group: Multidisciplinary patient care (dietary program, adjusted exercise program, psychological counseling, treatment of comorbidities) Control group: Standard care | Total number of hospitalizations |
| NCT04898972 | Randomized clinical trial; n = 80 | Mindfulness-based stress reduction (body scan; sitting meditation; awareness movement exercises; and walking meditation) Control group: informative booklet on stress reduction strategies | Perceived Stress Scale (PSS) Generalized Anxiety Disorder scale (GAD-7) Patient Health Questionnaire (PHQ-9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahi, M.S.; Thilagar, B.; Balaji, S.; Prabhakaran, S.Y.; Mudgal, M.; Rajoo, S.; Yella, P.R.; Satija, P.; Zagorulko, A.; Gunasekaran, K. The Impact of Anxiety and Depression in Chronic Obstructive Pulmonary Disease. Adv. Respir. Med. 2023, 91, 123-134. https://doi.org/10.3390/arm91020011
Rahi MS, Thilagar B, Balaji S, Prabhakaran SY, Mudgal M, Rajoo S, Yella PR, Satija P, Zagorulko A, Gunasekaran K. The Impact of Anxiety and Depression in Chronic Obstructive Pulmonary Disease. Advances in Respiratory Medicine. 2023; 91(2):123-134. https://doi.org/10.3390/arm91020011
Chicago/Turabian StyleRahi, Mandeep Singh, Bright Thilagar, Swetha Balaji, Sivaguha Yadunath Prabhakaran, Mayuri Mudgal, Suganiya Rajoo, Prashanth Reddy Yella, Palak Satija, Alsu Zagorulko, and Kulothungan Gunasekaran. 2023. "The Impact of Anxiety and Depression in Chronic Obstructive Pulmonary Disease" Advances in Respiratory Medicine 91, no. 2: 123-134. https://doi.org/10.3390/arm91020011