Favipiravir in the Treatment of Outpatient COVID-19: A Multicenter, Randomized, Triple-Blind, Placebo-Controlled Clinical Trial

 ,
,
Abstract
:Highlights
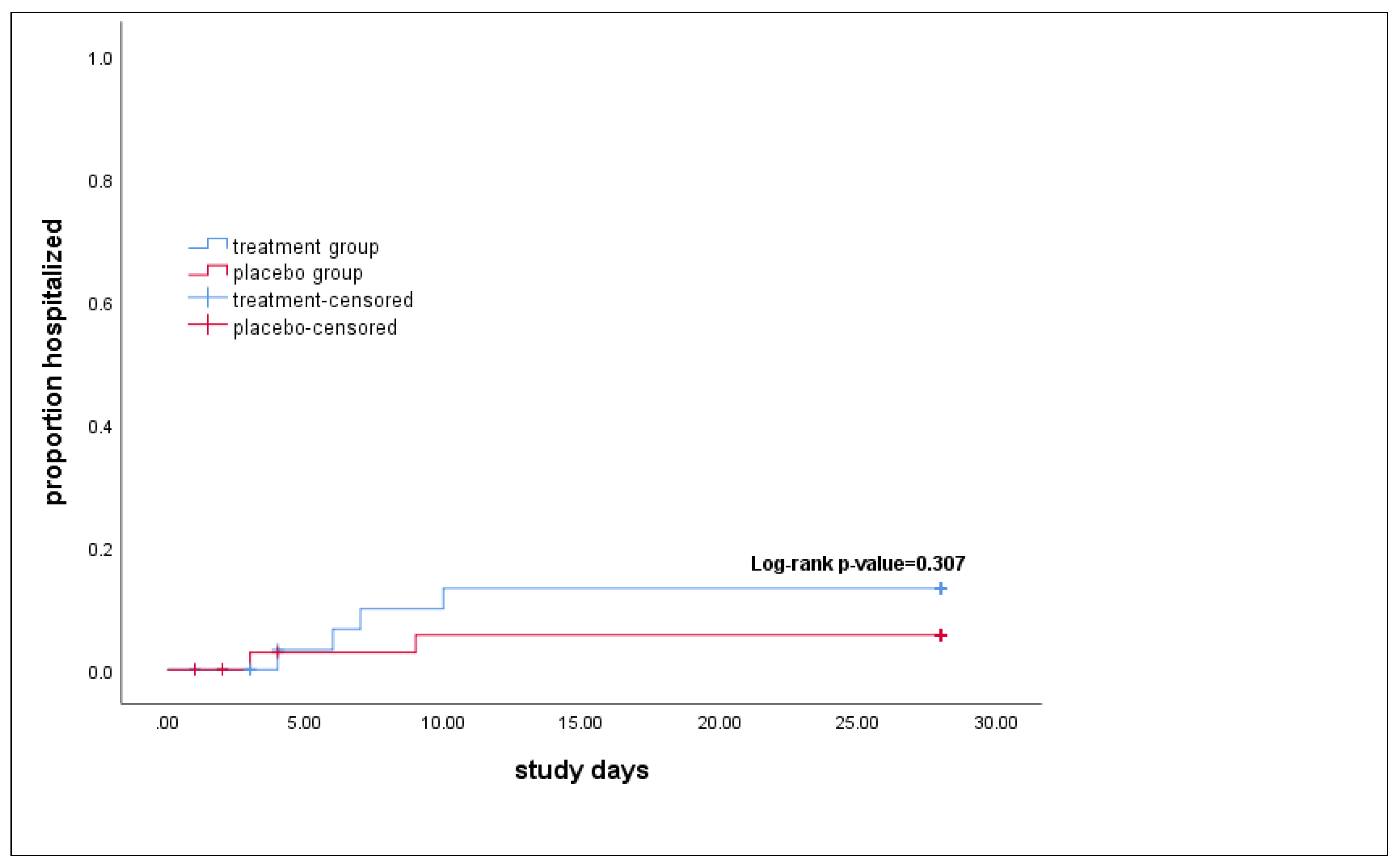
- Favipiravir, an RNA-dependent RNA polymerase inhibitor, shows no benefit in preventing the hospitalization of mild to moderate COVID-19 patients.
- Our results may inform decisions on the exclusion of Favipiravir from mild to moderate COVID-19 treatment guidelines.
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Randomization and Blinding
2.4. Procedure, Intervention, and Outcome
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Worldometer. COVID-19 Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 1 October 2022).
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef] [PubMed]
- Darab, M.G.; Keshavarz, K.; Sadeghi, E.; Shahmohamadi, J.; Kavosi, Z. The economic burden of coronavirus disease 2019 (COVID-19): Evidence from Iran. BMC Health Serv. Res. 2021, 21, 1–7. [Google Scholar]
- Goyal, A.; Cardozo-Ojeda, E.F.; Schiffer, J.T. Potency and timing of antiviral therapy as determinants of duration of SARS-CoV-2 shedding and intensity of inflammatory response. Sci. Adv. 2020, 6, eabc7112. [Google Scholar] [CrossRef]
- Gonçalves, A.; Bertrand, J.; Ke, R.; Comets, E.; De Lamballerie, X.; Malvy, D.; Pizzorno, A.; Terrier, O.; Calatrava, R.M.; Mentre, F.; et al. Timing of antiviral treatment initiation is critical to reduce SARS-CoV-2 viral load. CPT Pharmacomet. Syst. Pharmacol. 2020, 9, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Soy, M.; Keser, G.; Atagündüz, P.; Tabak, F.; Atagündüz, I.; Kayhan, S. Cytokine storm in COVID-19: Pathogenesis and overview of anti-inflammatory agents used in treatment. Clin. Rheumatol. 2020, 39, 2085–2094. [Google Scholar] [CrossRef] [PubMed]
- Bryant, A.; Lawrie, T.A.; Fordham, E.J. Ivermectin for Prevention and Treatment of COVID-19 Infection: A Systematic Review, Meta-analysis, and Trial Sequential Analysis to Inform Clinical Guidelines. Am. J. Ther. 2021, 28, e434–e460. [Google Scholar] [CrossRef]
- Frediansyah, A.; Nainu, F.; Dhama, K.; Mudatsir, M.; Harapan, H. Remdesivir and its antiviral activity against COVID-19: A systematic review. Clin. Epidemiology Glob. Health 2020, 9, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; Peto, R.; Henao-Restrepo, A.M.; Preziosi, M.P.; Sathiyamoorthy, V.; Abdool Karim, Q.; Alejandria, M.M.; Hernández, C.C.; Kieny, M.-P.; Malekzadeh, R.; et al. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar]
- Hassanipour, S.; Arab-Zozani, M.; Amani, B.; Heidarzad, F.; Fathalipour, M.; Martinez-De-Hoyo, R. Addendum: The efficacy and safety of Favipiravir in treatment of COVID-19: A systematic review and meta-analysis of clinical trials. Sci. Rep. 2022, 12, 1996. [Google Scholar] [CrossRef]
- Baranovich, T.; Wong, S.-S.; Armstrong, J.; Marjuki, H.; Webby, R.J.; Webster, R.G.; Govorkova, E.A. T-705 (Favipiravir) Induces Lethal Mutagenesis in Influenza A H1N1 Viruses In Vitro. J. Virol. 2013, 87, 3741–3751. [Google Scholar] [CrossRef] [Green Version]
- Furuta, Y.; Gowen, B.B.; Takahashi, K.; Shiraki, K.; Smee, D.F.; Barnard, D.L. Favipiravir (T-705), a novel viral RNA polymerase inhibitor. Antivir. Res. 2013, 100, 446–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y.; et al. Experimental Treatment with Favipiravir for COVID-19: An Open-Label Control Study. Engineering 2020, 6, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Solaymani-Dodaran, M.; Ghanei, M.; Bagheri, M.; Qazvini, A.; Vahedi, E.; Hassan Saadat, S.; Setarehdan, S.A.; Ansarifar, A.; Biganeh, H.; Mohazzab, A.; et al. Safety and efficacy of Favipiravir in moderate to severe SARS-CoV-2 pneumonia. Int. Immunopharmacol. 2021, 95, 107522. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. J. Pharmacol. Pharmacother. 2010, 1, 100–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassaniazad, M.; Farshidi, H.; Gharibzadeh, A.; Bazram, A.; Khalili, E.; Noormandi, A.; Fathalipour, M. Efficacy and safety of favipiravir plus interferon-beta versus lopinavir/ritonavir plus interferon-beta in moderately ill patients with COVID-19: A randomized clinical trial. J. Med. Virol. 2022, 94, 3184–3191. [Google Scholar] [CrossRef]
- Khamis, F.; Al Naabi, H.; Al Lawati, A.; Ambusaidi, Z.; Al Sharji, M.; Al Barwani, U.; Pandak, N.; Al Balushi, Z.; Al Bahrani, M.; Al Salmi, I.; et al. Randomized controlled open label trial on the use of favipiravir combined with inhaled interferon beta-1b in hospitalized patients with moderate to severe COVID-19 pneumonia. Int. J. Infect. Dis. 2021, 102, 538–543. [Google Scholar] [CrossRef]
- AlQahtani, M.; Kumar, N.; Aljawder, D.; Abdulrahman, A.; Mohamed, M.W.; Alnashaba, F.; Abu Fayyad, M.; Alshaikh, F.; Alsahaf, F.; Saeed, S.; et al. Randomized controlled trial of favipiravir, hydroxychloroquine, and standard care in patients with mild/moderate COVID-19 disease. Sci. Rep. 2022, 12, 4925. [Google Scholar] [CrossRef]
- Ivashchenko, A.A.; A Dmitriev, K.; Vostokova, N.V.; Azarova, V.N.; A Blinow, A.; Egorova, A.N.; Gordeev, I.G.; Ilin, A.P.; Karapetian, R.N.; Kravchenko, D.V.; et al. AVIFAVIR for Treatment of Patients With Moderate Coronavirus Disease 2019 (COVID-19): Interim Results of a Phase II/III Multicenter Randomized Clinical Trial. Clin. Infect. Dis. 2021, 73, 531–534. [Google Scholar] [CrossRef]
- Sirijatuphat, R.; Manosuthi, W.; Niyomnaitham, S.; Owen, A.; Copeland, K.K.; Charoenpong, L.; Rattanasompattikul, M.; Mahasirimongkol, S.; Wichukchinda, N.; Chokephaibulkit, K. Early treatment of Favipiravir in COVID-19 patients without pneumonia: A multicentre, open-labelled, randomized control study. Emerg. Microbes Infect. 2022, 11, 2197–2206. [Google Scholar] [CrossRef]
- Bosaeed, M.; Alharbi, A.; Mahmoud, E.; Alrehily, S.; Bahlaq, M.; Gaifer, Z.; Alturkistani, H.; Alhagan, K.; Alshahrani, S.; Tolbah, A.; et al. Efficacy of favipiravir in adults with mild COVID-19: A randomized, double-blind, multicentre, placebo-controlled clinical trial. Clin. Microbiol. Infect. 2022, 28, 602–608. [Google Scholar] [CrossRef]
- Deng, W.; Yang, C.; Yang, S.; Chen, H.; Qiu, Z.; Chen, J. Evaluation of favipiravir in the treatment of COVID-19 based on the real-world. Expert Rev. Anti-Infect. Ther. 2022, 20, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, D.B.; Budhathoki, P.; Khadka, S.; Shah, P.B.; Pokharel, N.; Rashmi, P. Favipiravir versus other antiviral or standard of care for COVID-19 treatment: A rapid systematic review and meta-analysis. Virol. J. 2020, 17, 141. [Google Scholar] [CrossRef] [PubMed]
- Kow, C.S.; Ramachandram, D.S.; Hasan, S.S. Future of antivirals in COVID-19: The case of favipiravir. Int. Immunopharmacol. 2022, 103, 108455. [Google Scholar] [CrossRef]
- Reddy, P.K.; Patil, S.; Khobragade, A.; Balki, A.; Raj, A.; Kalikar, M.; Reddy, R.; Shinde, R.; Cr, J.; Mutha, A.; et al. Evaluation of the Safety and Efficacy of Favipiravir in Adult Indian Patients with Mild-to-Moderate COVID-19 in a Real-World Setting. Int. J. Gen. Med. 2022, 15, 4551–4563. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Parkar, J.; Ansari, A.; Vora, A.; Talwar, D.; Tiwaskar, M.; Patil, S.; Barkate, H. Role of favipiravir in the treatment of COVID-19. Int. J. Infect. Dis. 2021, 102, 501–508. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Favipiravir (n = 38) | Placebo (n = 39) | p-Value |
|---|---|---|---|
| Age, year Mean (±SD) | 41.1 (±12.88) | 40.9 (±12.93) | 0.9 |
| Gender | 0.3 | ||
| Male | 19 (50.0) | 24 (61.5) | |
| Female | 19 (50.0) | 15 (38.5) | |
| Job | 0.8 | ||
| Self-employed | 15 (39.5) | 13 (33.3) | |
| Housekeeper or retired | 11 (28.9) | 12 (30.8) | |
| Students | 2 (5.3) | 1 (2.6) | |
| Employee | 10 (26.3) | 13 (33.3) | |
| Education | 0.9 | ||
| Diploma and lower | 18 (47.4) | 18 (46.2) | |
| Higher education | 20 (52.6) | 21 (53.8) | |
| Any comorbidities | 5 (13.2) | 6 (16.2) | 0.7 |
| BMI ≥ 25 | 26 (68.4) | 22 (57.9) | 0.3 |
| Signs and symptoms | |||
| Fever | 29 (76.3) | 24 (61.5) | 0.1 |
| Cough | 21 (55.3) | 21 (53.8) | 0.9 |
| Headache | 21 (55.3) | 21 (53.8) | 0.9 |
| Dyspnea | 11 (28.9) | 9 (23.1) | 0.5 |
| Gastrointestinal | 13 (34.2) | 13 (33.3) | 0.9 |
| Sore throat | 11 (28.9) | 13 (33.3) | 0.6 |
| Rhinorrhea | 16 (42.1) | 11 (28.2) | 0.2 |
| Chills | 21 (55.3) | 19 (48.7) | 0.5 |
| Body pain | 27 (71.1) | 25 (64.1) | 0.5 |
| Loss of appetite | 15 (39.5) | 10 (25.6) | 0.1 |
| Loss of smell or taste | 8 (21.1) | 10 (25.6) | 0.6 |
| Fatigue | 28 (73.7) | 26 (66.7) | 0.5 |
| Mean days (±SD) between symptom initiation and entering the study | 3.9 (±1.49) | 3.8 (±1.45) | 0.87 |
| Outcome | Favipiravir (n = 38) | Placebo (n = 39) | p-Value |
|---|---|---|---|
| Primary outcome | 4 (10.5) | 2 (5.1) | 0.3 * |
| Hospitalization | |||
| Secondary outcome | 0 | 1 (2.6) | - |
| Adverse events |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaezi, A.; Salmasi, M.; Soltaninejad, F.; Salahi, M.; Javanmard, S.H.; Amra, B. Favipiravir in the Treatment of Outpatient COVID-19: A Multicenter, Randomized, Triple-Blind, Placebo-Controlled Clinical Trial. Adv. Respir. Med. 2023, 91, 18-25. https://doi.org/10.3390/arm91010004
Vaezi A, Salmasi M, Soltaninejad F, Salahi M, Javanmard SH, Amra B. Favipiravir in the Treatment of Outpatient COVID-19: A Multicenter, Randomized, Triple-Blind, Placebo-Controlled Clinical Trial. Advances in Respiratory Medicine. 2023; 91(1):18-25. https://doi.org/10.3390/arm91010004
Chicago/Turabian StyleVaezi, Atefeh, Mehrzad Salmasi, Forogh Soltaninejad, Mehrdad Salahi, Shaghayegh Haghjooy Javanmard, and Babak Amra. 2023. "Favipiravir in the Treatment of Outpatient COVID-19: A Multicenter, Randomized, Triple-Blind, Placebo-Controlled Clinical Trial" Advances in Respiratory Medicine 91, no. 1: 18-25. https://doi.org/10.3390/arm91010004