

Nose-to-Brain Targeting via Nanoemulsion: Significance and Evidence


1
School of Pharmaceutical Sciences, CSJM University, Kanpur 208024, Uttar Pradesh, India
2
Faculty of Pharmacy, Uttar Pradesh University of Medical Sciences Saifai, Etawah 206130, Uttar Pradesh, India
*
Author to whom correspondence should be addressed.
Colloids Interfaces 2023, 7(1), 23; https://doi.org/10.3390/colloids7010023
Submission received: 17 January 2023
/
Revised: 12 March 2023
/
Accepted: 14 March 2023
/
Published: 17 March 2023
(This article belongs to the Special Issue Recent Advances in Emulsions and Applications)
Abstract
:Background: Non-invasive and patient-friendly nose-to-brain pathway is the best-suited route for brain delivery of therapeutics as it bypasses the blood–brain barrier. The intranasal pathway (olfactory and trigeminal nerves) allows the entry of various bioactive agents, delivers a wide array of hydrophilic and hydrophobic drugs, and circumvents the hepatic first-pass effect, thus targeting neurological diseases in both humans and animals. The olfactory and trigeminal nerves make a bridge between the highly vascularised nasal cavity and brain tissues for the permeation and distribution, thus presenting a direct pathway for the entry of therapeutics into the brain. Materials: This review portrays insight into recent research reports (spanning the last five years) on the nanoemulsions developed for nose-to-brain delivery of actives for the management of a myriad of neurological disorders, namely, Parkinson’s disease, Alzheimer’s, epilepsy, depression, schizophrenia, cerebral ischemia and brain tumours. The information and data are collected and compiled from more than one hundred Scopus- and PubMed-indexed articles. Conclusions: The olfactory and trigeminal pathways facilitate better biodistribution and bypass BBB issues and, thus, pose as a possible alternative route for the delivery of hydrophobic, poor absorption and enzyme degradative therapeutics. Exploring these virtues, intranasal nanoemulsions have proven to be active, non-invasiveand safe brain-targeting cargos for the alleviation of the brain and other neurodegenerative disorders.

1. Introduction
Brain diseases, including dementia, epilepsy, migraine, autoimmune disorders (Parkinson’s, Alzheimer’s and prion’s disease), brain tumours and acute ischemic brain haemorrhages, require extensive clinical care due to a significantly high rate of morbidity and mortality worldwide [1]. Most of the developed brain-targeting medications relieve symptomatic brain deregulatory functions and are inefficient in providing satisfactory therapeutic responses. The major issues overlaid are (i) lipophilic blood–brain barrier (BBB), (ii) complexity of the microenvironment of the brain and (iii) abnormal protein status. Central nervous system (CNS)vessels containing arterioles and venules are regular, continuous and non-apertured. These vessels are involved in the regulation and exchange of ions and molecules throughout the braincells. The exclusive morphology of CNS vessels and the barrier function of the BBB guard the brain from the entry of antigens, toxins and pathogens. The BBB diverts blood from the interstitial fluid and serves as an efficient barricade for the diffusion of most of the actives to reach the brain receptors of the CNS. Functionally, it is a dynamic regulator that transports nutrients and checks the entry of heavy and undesirable (lipophilic) molecules across the extracellular fluid of the brain. Lipophilic molecules with an optimum Log P (approximately 1.5–2.7) and molecularweight of 600 Daltons can freely permeate the BBB [2].
The brain endothelial cells (BECs) form the walls of brain blood vessels and are highly polarized in contrast to the endothelial cells of other tissues. BECs are jointed together by tight junctions that again confine the paracellular flux of ions and limit transcellular exchange between blood and brain cells, i.e., transcytosis and pinocytosis. BECs coordinate a series of metabolic, transportation and physiological functions with the interaction of several neural, vascular and neural components involved in the management of health and diseased conditions of the body. BBB-adorned p-glycoprotein efflux transporters also restrict the movement of bioactive/macromolecules and their receptor binding for a desired pharmacological response. Expression of both efflux and influx transporters between blood and brain cells ismediated via BECs. Efflux transporters (such as p-gp) that removetoxins tend to diffuse cell membranes passively, while the influx transporters are a kind of carrier that engage to deliver nutrients and ions to the brain cells [3]. Apart from being an active cellular self-defence barrier, the BBB strictly monitors the CNS microenvironment and communicates and acclimatises with the conduct of CNS cells in the progression of brain disorders [4].
These attributes of BBB create hurdles for the permeation of therapeutic or bioactive agents to reach the brain tissues, thus exhibiting obstructions to combat CNS diseases. A report of WHO healthcare statistics states that approximately 1.5 million people are sufferers of CNS disorders, including autoimmune Parkinson’s, Alzheimer’s diseases and schizophrenia [5].
Although the current drug delivery approaches have displayed a vibrant picture of effective CNS treatments with survival rates surging, still, there are unsolved issues for the complete cure/therapy of most CNS disorders. There is definitely a need for an advanced therapeutic system that enables the potential crossing of the BBB at an adequate level to attain the desired pharmacological action. The BBB limits the entry of 98% of the low molecular weight molecules and hence, drastically reduces bioavailability. A report retrieved from the comprehensive medicinal chemistry database signifies that a mere 5% of therapeutics out of 7000 with 357 Dalton molecular weight and 2.57 Log P (partition coefficient) have the potential to penetrate the BBB and exhibit potent action for mitigation of insomnia, depression and schizophrenia [6]. Invasive strategies, including intra parenchymal, intracranial and intra-cerebro ventricular injections, are administered for direct drug delivery to the brain. These local strategies are interlinked and emphasize the use of electromagnetic field and ultrasound approaches. These are preferred to treat psychological and neurological disorders but are painful and risky as well [7]. Hence, a non-invasive approach such as the nose-to-brain delivery pathway is suggested that bypasses the BBB, reduces toxicity and delivers the therapeutics at the target site. The intranasal delivery route facilitates the direct delivery of the drug into the cerebrospinal fluid following the olfactory path [8].
Complexity of Nose-to-Brain Drug Delivery Path
The nose is an integral human olfactory/respiratory part and contains a 60 µm thick area of 1.25–2 m2. The nasal septum divides the nasal cavity into the nasal vestibule, olfactory and respiratory regions. The nose entrance or nasal vestibule is covered with squamous epithelium that contains vibrissae (nasal hair) and oil glands. The respiratory region comprises the maximum surface area and holds the ciliated respiratory epithelium and vascularised nasal turbinate made up of erectile and sinusoid tissues [9]. The olfactory part is positioned on the rooftop of the nasal cavity and lined with olfactory epithelium (pseudostratified). Adhered olfactory nerves directly connect with CNS by circumventing the BBB. The olfactory region has a surface area of 2–10 cm2. After crossing the olfactory epithelium, a therapeutic agent transports intracellularly along the associated olfactory nerve. Lipophilic molecules follow paracellular passive diffusion, while hydrophilic drugs move through a carrier-mediated transport way [10].
The nasal region contains two nerve terminations, i.e., olfactory and trigeminal. Both neuropathways originate from the nasal cavity at the olfactory neuroepithelium and terminate in the brain.
Interestingly, these routes are the single way that links the brain to the exterior environment and transports countless neurotherapeutic agents. A diverse range of neurotherapeutics (macro and low molecular weight) is generously distributed to the CNS via this route [11]. Figure 1 portrays the typical route, including diverse transport systems and nerves for the effective delivery of therapeutic agents following the nose-to-brain pathway. Moreover, the associated blood–nerve barrier comprising the end oneurial microvessels and perineurium is involved in the regulation of the permeability of ions and molecules from both these pathways into the CNS. Hence, the blood–nerve barrier is equally important, and proper attention must be specified while designing a nose-to-brain drug delivery system. The non-invasive intranasal pathway bypasses both the BBB and first-pass metabolism. Hence, it is assumed to be superior by virtue of myriad merits, including lower dose strength, ease of administration, safety, instant therapeutic action and reduced systemic toxicity with improved patient compliance [12]. The focus of intranasal delivery is to transport brain-targeted therapeutics in the desired concentration at a predetermined rate. Drug metabolism, degradation and clearance can influence the efficiency of the drug at the site [13].
The enhanced surface area of the stratified squamous naso-epithelium is extremely permeable, porous and vascularised, hence permitting fast drug absorption to occur at a smaller dose. Nasal drug delivery systems do not need any drug modification or coupling with a carrier for the distribution and effectiveness of therapeutic agents [14].
2. Nanoemulsions
Researchers are consistently engaged in the development of promising and potential non-invasive brain drug delivery systems. To achieve the targeted CNS response, various scientific investigations have been reported that define the olfactory and trigeminal routes and successfully deliver CNS medicaments following the nose-to-brain pathway. Emulsions are colloidal systems with two distinct phases, in which one is dispersed and another is dispersion media. Their droplet or globular dimension typically varies from 200 nm to 100 µm. Countless bioactive, nutraceutical and therapeutic agents can be feasibly incorporated or encapsulated in this biphasic system for conventional and controlled effects as well [15]. However, conventional emulsions exhibit issues such asphysical instability (aggregation and gravitational separation) and a poor ability to control the release of the entrapped active pharmaceutical agent (API) at the target site.
Nanoemulsions are formulated via two broad methodologies, low-energy (phase inversion) and high-energy methods (ultrasonication, microfluidic, high-pressure homogenization). The low-energy method is based on phase inversion temperature and produces a smaller globular dimension with the involvement of less energy, whereas the high-energy methods are reliant on energetic mechanical strategies and disruptive forces for the generation of smaller oil globules.
A few advanced emulsions, including multilayer emulsion, multiple emulsion, nanoemulsion, pickering emulsion and high internal phase emulsion, have been introduced for the delivery of bioactive agents. Table 1 compiles salient features of advanced types of emulsion as drug delivery systems. However, these advanced emulsions are not cost-effective and are tedious to formulate.
These lipophilic systems have a fine globular size, preferably in nanodimensions. These structures are well absorbed through the mucosal layer and are hence suitable for site-specific drug delivery. Among all, the nanoemulsions are the most successful among other advanced systems due to their fine size, leveraged surface area, the onset of action, biodistribution and stability. Both the o/w and w/o types of emulsions are modulated to target naso-mucosa for drug delivery across the brain tissues. Exceptionally high encapsulation of lipophilic drugs in o/w type nanoemulsion offers enhanced solubility, better absorption and improved bioavailability with minimum enzymatic degradation [21]. Nanoemulsions are also preferred for the formulation of mucoadhesive systems as these facilitate a long residence time and enhanced nasal absorption with limited clearance. The o/w type of nanoemulsions is better suited for brain-targeting delivery systems owing to their small size, lipophilicity and efficiency in permeating the BBB. Despite the merits offered, nose-to-brain delivery faces significant challenges and limits its frequent use. Lower bioavailability, susceptibility to enzymatic degradation and higher nasal clearance present the grey side of this route.
Moreover, mucociliary clearance, a smaller volume of the nasal cavity and its limited surface area further limit the absorption of sensitive drugs aimed to target brain tissues. Therefore, different nanoengineered mucoadhesive and in situ nanoemulgels (thermo-responsive and pH-responsive) have been designed to provide prolonged and effective drug delivery.
2.1. Oil and Globule Size
Newly discovered drug molecules display poor aqueous solubility, which hence, severely affects the pharmacokinetic and pharmacodynamic characters. Oil, an integral part of nanoemulsion, resolves this issue and favours the maximum solubility of the drug entity. One can choose vegetable oil, triglycerides/diglycerides and essential polyunsaturated fatty acids depending upon the lipophilicity of the therapeutic agent. Higher oil concentration increases the globule scale of nanoemulsion and causes poor permeation across nasal mucosa [22]. Reports demonstrated that linolenic acid with two cis-double bonds and eighteen carbon monocarboxylic fatty acids couldefficiently cross the BBB, suggesting that entry of these oils in brain cells is carried out in a selective and distinct manner. Hence, it is suitable for the formulation of nanoemulsion [23]. For brain targeting, the lipidic component (5–20%) is selected for the formulation of the o/w type of nanoemulsion. Solubility of the oil highly matters in the selection of oil, as it must solubilize the drug molecule for efficient action at the brain target site. Usually, lipids, including cottonseed oil, coconut oil, sesame oil and soybean oil, are preferred alone to their mixture [24]. Further, added materials (surfactant and co-surfactant), process parameters (viscosity ratio, mixing time), rheology (shearing stress and shear rate) and type of methodology (microfluidization, phaseinversion, ultrasonication and high-pressure homogenization) decisively control the globule size distribution in nanoemulsion [25]. As discussed earlier, the nasal route comprises the olfactory and trigeminal pathways that are the foremost channels for brain-targeting drug delivery systems. Anatomically, the typical diameter of the olfactory axon in a human goes up to 700 nm [26]. Thus, the oil globular size should be kept within this limit to maintain adequate transportation and retention as well. Reports state that the smaller the oil globular dimension, i.e., 80, 100 and 200 nm, the higher the mucosal retention property for 16, 14 and12 h, respectively, in the arena of the nostril, exhibiting sluggish mucociliary clearance compared to the larger-scaled particles. Moreover, larger particles (greater than 900 nm) are also unable to reach the olfactory bulb and havepoor bioavailability inthe region of the brain [27].
Further, the type of oils and their properties are also significant while aiming brain targeting through nanoemulsion. The literature envisages that linolenic acid, omega-6 fatty acids, oleic acid and linolenic acids are frequently employed for the development of nanoemulsion to be delivered through the intranasal route. Ahmad et al. have developed an intranasal nanoemulsion containing amiloride (drug), oleic acid (oil) and Tween 20 and Carbitol as surfactant and cosurfactant. The selection of oil, its concentration and developed globular size played a prominent role in enhancing bioavailability in brain tissues. Outcomes suggested that an average globular size of 100 nm with a polydispersity index of 0.231 and negative zeta potential (−9.83 mV) assisted hurdle-free transportation and validated the biodistribution. Formulated nanoemulsion exhibited high drug content. i.e., ~98.38% at pH 6.4 ± 0.18. Both nose-to-brain transport (approximately 586%) and brain targeting efficacy (1992%) in rodents explained higher bioavailability compared to the intravenous route, thus suggesting the efficacy of the drug in epileptic sufferers [28].
2.2. Surfactant and Stability
Surfactants not only reduce the interfacial tension between two distinct phases but also manage the stability of the biphasic colloidal system by preventing phase separation [29]. Further, the surfactants improve the solubility of therapeutics; alter the fluidity of the epithelium cell junctions, thus enhancing the permeation of these drugs through the nasal–mucosal pathway.
Additionally, surfactants may change the structural integrity of mucosal lining, so the selection of a concentration of surfactant is crucial while preparation of nanoemulsion aimed atbrain targeting [30].Reports suggest that surfactants such as phosphatidylcholine, bilesalt, chitosan, starch, Tweens (tween 60, 80), sodium dodecyl sulphate and Span (Span 60, 80),poloxamers, casein, polyethylene glycol containing block polymers and few proteins and lipids are frequently utilized for the development of nanoemulsions [31].
Kinetically stable nanoemulsion takes a long time to separate out in its different phases. However, diverse establishment steps, including creaming, cracking, coalescence, flocculation and Ostwald ripening, are often befall with emulsions. The globules come close due to electrostatic attraction force and form a single big entity that mediates flocculation-type destabilization. At the same time, coalescence occurs due to the merging of oil globules or water droplets. In the case of nanoemulsion, steric stabilization is stronger by virtue of the adsorbed coating of surfactant on the droplet, resulting in an enhanced repulsive maximum that checks instabilities. Formulation factors such as surfactant concentration, ionic strength, chemical configuration, solubility and temperature distinctly affect the stability of nanoemulsion. The rate of destabilization is highly concerned with increased concentration of surfactant and more diffusion of oil that reduce Gibbs elasticity. Hence, surfactant plays a critical role in a dual manner; i.e., the formulation and stability of nanoemulsion. Customized polymeric emulsifiers are suggested while preparing nanoemulsions owing to their flexibility, tailored size and hydrophobicity [32].
Cosurfactants assist surfactants in the reduction of boundary tension or interfacial tension up to the desired level. The mechanism or role-play of cosurfactants is similar to the surfactant; hence, an optimized concentration and desired HLB (hydrophilic–lipophilic balance) offering compound should be selected by constructing a ternary phase diagram (concentration of oil, surfactant and cosurfactant). Chiral alcohols, tween 80, polyethylene glycols 600, butan-1-ol and sorbitol are preferred as cosurfactant while formulating nanoemulsions [33]. Zeta potential poses a prominent role in maintaining the thermodynamic stability of nanoemulsions. Reports demonstrate that optimum zeta potential value. i.e., ±30 mV offers an electrostatically stabilized drug delivery system. Further, the retention time in the nasal cavity was also controlled by this parameter. The nasal mucosa is adorned with negatively charged mucin at its surface; hence, positive-charge-containingnanoemulsionsaresuitableforgoodadherence in such cases [34]. Several of the literature reports depict most of the brain-targeted nanoemulsions with a negative charge and zeta potentialof −10 mV [35].
3. Intranasal Nanoemulsions for the Management of Brain Diseases
The intranasal pathway (olfactory and trigeminal nerves) lets the entry of various bioactive agents circumvent the hepatic first-pass effect, thus targetingneurological diseases [36]. Several investigations and research have suggested the vital role ofdrug-loaded nanoemulsions in the mitigation of countless brain disorders proves to be a potential alternative to oral drug delivery systems. Further, mucoadhesive polymer enriched nanoemulsion prolongs residence time and therapeutic effect by weakening rapid clearance from the nasal mucosa. Diedrich et al. (2022) developed a chitosan-coated luteolin nanoemulsion for effective brain targeting after intranasal administration in a neuroblastoma sufferer child. Obtained nanoemulsion possessed ~68 nm average particle size and positive zeta potential (~13 mV). The formulation exhibited 85.5% encapsulation efficiency and 72 h prolonged in vitro release of luteolin. Ex vivo performed Baker–Lonsdale kinetic model depicted approximately six times higher permeation across the nasal mucosa. Moreover, pharmacokinetic studies of the single dose administered intranasal nanoemulsion revealed a tentimes higher drug half-life and nearly a four times higher luteolin biodistribution in brain tissues that further suggested potential usage of developed chitosan-coated luteolin nanoemulsion for the management of brain neuroblastoma. A performed in vivo study exhibited complete inhibition of the growth of blastoma cells at a concentration of 2 µM [37,38].
3.1. Nanoemulsions for Neurological Disorders
Neurological disorders include a broad range of disabilities that progressively impair the nervous system associated with vital functions of the body. i.e., mobility, sensation, coordination, reasoning, and learning [39]. Epilepsy, autism, Parkinson’s, Alzheimer’s and other neuromuscular disorders are just a few to be named in this category. These specific ailments require precise delivery of therapeutic agents inside the brain for effective results. BBB presents a formidable hurdle that limits the efficacy of conventional formulations [40]. For instance, acetylcholinesterase inhibitors such as rivastigmine, memantine and galantamine have the potential to manage Alzheimer’s disease but possess poor brain targeting owing to theirerratic pharmacokinetic and pharmacodynamic profiles [41]. Nanosized nanoemulsion and its structural architecture facilitate site-specific targeted drug release with minimum adverse effects. Figure 2 summarizes the role of nanoemulsions in the management of brain disorders.
Jiang et al. (2022) explored herbal huperzine for the management of the neurological issue. i.e., Alzheimer’s disorder. Huperzine is obtained from Huperzia serrata, a Chinese club moss, and has poor brain transportation. To upgrade its properties, we formulated huperzine nanoemulsion (hup-NE) modified with lactoferrin (Lf-hup-NE) that could transport the drug to the affected sites of the brain via olfactory–trigeminal nerves. Performed pharmacokinetic studies displayed greater mean residence time of modified Lf-hup-NE (4.07 h) compared to non-modified nanoemulsion (3.03 h). Similarly, Cmax and AUC0–t of Lf-hup-NE were also higher. i.e., ~52.29 ng/mL and ~245.09 ng/mL X h compared to developed non-modified nanoemulsions ~50.54 ng/mL and 123.63 ng/mL Xh, respectively. A rat model olfactory nerve transaction was designed to observe nanoemulsion transportation via the nose-to-brain route. Of the nanoemulsion, 50µLwas intranasal administered both in olfactory nerve transacted rats and normal rats, and in vivo fluorescence images of treated rats were collected that depicted retention of the drug in brain regions. The results confirmed successful drug absorption and transportation of hup-NE and modified Lf-hup-NE via blood circulation that implicated both direct and indirect drug delivery. P2 signals intensity of modified Lf-hup-NE was high owing to its greater efficiency of translocation in brain areas through intranasal delivery. Further, the developed modified Lf-hup-NE had the potential to inhibit P-gp efflux protein and enhanced drug concentration there. This novel formulation can be exploited for better transportation and accumulation of herbal huperzine in brain cells and can achieve better therapeutic responses [42].
One of the progressive neurodegenerative motor neuron disorders is amyotrophic lateral sclerosis. It is characterized by symptoms such as the depletion of upper and lower motor neurons. A BCS class II drug, riluzole, has limited bioavailability (60%) due to poor penetration across BBB. This drug is indicated for the management of amyotrophic lateral sclerosis (ALS). Parikh et al. (2016) formulated riluzole containing o/w nanoemulsion by phase titration method. Sefsol 218 and tween 80/carbitol (1:1) were employed as oil substitutes and surfactants, respectively. The developed nanoemulsion was thermodynamically stable with a drop size of ~23 nm. Further, the formulation was free of nasal ciliotoxicity and significantly increased brain uptake of riluzole (p < 4.1 × 10−6) via intranasal delivery on comparing with oral nanoemulsion to the Wistar albino rats. This novel nanoemulsion has displayed a promising alternative approach for the treatment of people living with ALS [43].
Recently, nose-to-brain delivery of bromocriptine mesylate- and glutathione-embedded nanodimension emulsion was designed by Ashhar et al. (2022) for the effective treatment of another distinguished neurodegenerative Parkinson’s disease. This fatal disorder is provoked by the generation of free radicals in neurons (dopaminergic); consequently, oxidative stress-induced neuron degradation occurs. The researchers designed intranasal dosage for containing bromocriptine mesylate and glutathione-embedded nanoemulsion to relieve oxidative stress. Performed DPPH radical scavenging analysis revealed enhanced antioxidant action due to the combined effect of both bromocriptine mesylate and glutathione present in nanoemulsion. The formulated nanoemulsion was estimated for depth of permeation with confocal laser scanning microscopy after intranasal administration, which resulted in superior penetration to the brain cells. Further, the pharmacokinetic study estimated AUC0–8 of nanoemulsion that revealed a higher concentration of both compounds in brain regions of the Wistar rat model after intranasal administration. The nasal ciliotoxicity study in Wistar rats explained the biocompatibility of the formulated nanoemulsion. Thereafter, the biochemical study displayed a reduced level of interleukin-6, alpha tumour necrosis factor and thiobarbituric acid, which are reactive substances, and concluded that bromocriptine mesylate- and glutathione-loaded nanoemulsion has the potential to overcome oxidative stress level in persons living with Parkinson’s disease [44].
Another chronic CNS complaint: ‘epilepsy’ is frequently characterized by instant senseless seizures due to neurons’ electric instabilities in the brain region. BCS class II topiramate(anticonvulsant) has been employed for the clinical management of partial and generalized seizures. Its poor bioavailability on oral administration is due to poor entry across BBB. Being a substrate of P-gp transporter, we reported the limited efficacy against epilepsy. An o/w nanoemulsion was prepared utilizing Capmul MCM C8 (2% w/w) by Patel and coworkers (2020) for the improvement of the brain delivery of topiramate. A blend of 32% surfactant and co-surfactant Tween 20 and carbitol at a ratio of 2:1 was included to customize the globular size, PDI, zeta potential and viscosity. The resulting nanoemulsion possessed a ~4.73 nm mean particle size with a stability of six months. The brain uptake efficiency of the intranasally delivered piramate contained a nanoemulsion that was quite higher (p < 1.8 × 10−8) compared to the orally delivered nanoemulsion. The pharmacokinetic studies in Wistar albino rats depicted enhanced bioavailability with minimum adverse effects after delivering the nanoemulsion through the intranasal route [45]. Table 2 gathers recent studies on developed nanoemulsions and their applications for the treatment of various brain diseases.
Mucoadhesive buspirone-loaded nanoemulsion was formulated for direct delivery to the brain and modification of bioavailability after administering through an intranasal route. A total of 5% of w/v hydroxypropyl beta-cyclodextrin and chitosan hydrochloride (1% w/v) were selected for the preparation of mucoadhesive nanoemulsion. The assay resulted in a 61% improvement in bioavailability, which exhibited peak plasma concentration in rats’ brains at 30 min lesser compared to bare buspirone nanoemulsion (60 min). Further, after nasal administration, buspirone–chitosan nanoemulsion exhibited 2.5 times higher AUC0–480 in the brain (~711 ng/g) compared to I/V administration (~282 ng/g) and bare buspirone nasal formulation (~354 ng/g). Mucoadhesive buspirone–chitosan nanoemulsion revealed a high percentage of drug transport (75.77%) and targeting efficiency in the brain region [63]. Recently, the BCS class II drug ‘melatonin’ was aimed to develop a mucoadhesive nanoemulsion to enhance brain bioavailability and alleviatedepression. The formulated nanoemulsion improved the poor aqueous solubility of melatonin, and added chitosan provided a mucoadhesive property that exhibited prolonged retention time (0.641 min) in the brain region. The locomotor activity of model rats exhibited improved behavioural responses [64].
3.2. Nanoemulsions for Brain Tumour
Managing and treating brain tumours has always remained the most crucial and challenging task, as approximately 0.2 million clinical diagnoses of the brain and other associated CNS malignancies are reported worldwide. One of the WHO surveys stated that nearly 80%of primary brain tumours are concerned with the origin of gliomas (glial cells) [65]. Glioblastoma multiforme, or GBM, is the most prominent and aggressive grade IV glioma that affects nearly8%of individuals in a population of 100,000. This malignant brain tumour is highly fatal, has a very low survival rate (1 year), and requires immediate surgery and other treatments, including neuroimaging and photodynamic/radiotherapy [66]. Scientific reports confirmed that CD73 is accountable for the development of adenosine that is overexpressed in glioblastoma cells and hence targeted to treat this tumour in the brain region. Originally, surface enzyme CD73 was a biomarker and described as a lymphocyte differentiation antigen, and its inhibition checks glioblastoma pathogenesis [67]. Failure in chemotherapy may be due to impaired therapeutic action via poor permeation across BBB. i.e., microvasculature environment of the CNS.
FDA-approved first-line antineoplastic therapeutic ‘temozolomide or temodar®’ is widely employed for the management of glioblastoma multiforme or GBM owing to permeation efficacy across BBB. It is a DNA alkylating drug administered orally and intravenously due to its very short half-life. However, administering high doses leads to severe adverse toxicities, including cardiomyopathy, oral ulceration, myelo-suppression and hematological issues [68]. To avoid these critical issues at present novel strategies such as topical implants, convection-enhanced delivery and nanotechnological-based formulations are clinically required for the management of brain gliomas. The last decade was the era of successful brain-targeted drug delivery approaches following a peculiar nasal path where trigeminal and olfactory nerves facilitate precise drug transportation due to the sole connection between the central nervous system and brain region. This non-invasive and safe route represents the quick onset of action with minimum systemic toxicity and adverse risks that comply with brain tumour sufferers. Moreover, low therapeutic doses and bypassing hepatic first-pass metabolism offer extramerits to the intranasal antineoplastic drug-delivery system.
However, half-life clearance (15–20 min) and limited volume of the formulation (25–200 µL) in a single dose pose strains and must be considered while formulating nose-to-brain delivery [69].
Biocompatible lipidic nanoemulsions are a highly preferred delivery system for intranasal delivery and brain targeting. The extended residing time in the nasal cavity releases the adequate therapeutic agent from the nanostructured emulsion. Bayanati et al. (2021) designed in situ emulsion-based gel of antineoplastic drug temozolomide through low energy technique for the chemotherapy of glioblastoma. The formulation bypassed BBB after delivering through the intranasal route. A suitable pseudoternary phase diagram with various quantities of triacetin, labrasol (surfactant) and transcutol®P (permeation enhancer) was established and was added for the preparation of the nanoemulsion. The nanoemulsion contained a range of particle sizes from 19–23 nm with PDI from 0.18–0.25. A slight positive zeta potential. i.e., ~1.6 might be due to the non-ionic nature of the selected surfactant/co-surfactant. By contrast, the developed in situ gel with a blend of amphiphilic poloxamer 407 and 188 exhibited a slightly increased mean particle size (16.25 nm) and PDI (~0.35) with an acceptable pH (~6.5) that showed a compatibility with nasal mucosa without irritation. The augmented viscosity (113.57 cp) of the formulation also advocated prolonged nasal retention due to reduced mucociliary clearance. Further, in vitro release efficiencies of both nanoemulsion and its in situ gel were nearly 90% and 87%, respectively, and appeared to be sustained compared to the nasal solution after 6 h. Noticeable risen in percentage mucoadhesion was observed in situ gel (37.03%) compared to nanoemulsion (20.35%) owing to the gel-forming amphiphilic poloxamer that might have formed a noncovalent entanglement with nasal mucosa. Further, the developed in situ nanoemulsion exhibited a 1.52 times higher permeation compared to the control solution. Added labrasol and transcutol®P efficiently enhanced the solubility of temozolomide and worked as permeation enhancers across nasal olfactory–trigeminal pathways. Labrasol inhibited P-gp and acted as an efflux transporter. Both temozolomide nanoemulsion and gel with poloxamer 407 were stable during freeze-thaw cycles and performed centrifugation. Gamma scintigraphy revealed an accumulation of radio-labelled temozolomide in the brain after intranasal delivery and concluded efficient uptake to the affected site of the brain [70]. Table 3 outlines the newly developed nanoemulsions for the amelioration of brain tumours.
An amalgamation of antineoplastic paclitaxel and C (6)-ceramide-loaded oil in water nanoemulsion was developed, including a high concentration of polyunsaturated fatty acid (pinenut oil) for enhanced therapeutic action against human U-118 glioblastoma cells. The average particle size of the nanoemulsion was observed at 200 nm. Epi-fluorescent microscopy was employed for the uptake and biodistribution of rhodamine-labelled paclitaxel and nitro-benzofurazone-labelled C (6)-ceramide nanoemulsion in glioblastoma cells. On intranasal administration, the developed nanoemulsion exhibited prominently high cytotoxicity and apoptosis within the malignant cells, thus suggesting a promising approach for the therapy of aggressive glioblastoma tumours [76]. Disulfiram, an alcohol withdrawal drug, is an FDA-approved antineoplastic drug that has been clinically proven in various cancerous cases, including glioblastoma. Its inclusion complex with copper ions has already gained success in the management of adenosine over-expressive human brain tumour. Qu et al. (2021) designed a novel inclusion complex of disulfiram and hydroxypropyl –β-cyclodextrin with a copper ion that augmented drug solubility and antitumour activity with increased safety in vitro.
Disulfiram is considered an active antitumour agent while complexed with copper ions. Here, disufiram is entrapped within the structure of hydroxyl propyl β-cyclodextrin; thus, the solubility and safety profile of the drug were amplified. An intense fluorescence signal was observed in the Wistar male rat brain model that indicated extreme brain targeting via the intranasal delivery of the drug. Developed inclusion complex embedded nanoemulsion promoted apoptosis after intranasal administration, thus inhibiting cell proliferation and tumour growth. Furthermore, histopathological outcomes displayed nonobvious damage to normal cells [77].
3.3. Nanoemulsions in Cerebral Ischemia
Cerebral ischemia is a condition aroused by acute brain injury that results in inadequate blood flow in the brain region. It is also a medical emergency that, if ignored, may lead to cerebral infarction and, ultimately, permanent brain disability. Broad cerebral ischemia is categorized as global and focal. The former happens due to shock and systemic hypotension.
Structural and functional cardiac issues, including arrhythmia, mediate global ischemia. At the same time, the obstruction of arterial blood flow (thrombosis or embolism) to the brain and the irreversible neuronal loss leads to focal ischemia. Nearly 60–70% of cerebral ischemia clinically reported is due to embolism (formation of a clot) in the heart or in a large artery [78]. Figure 3 portrays focal and global cerebral ischemic conditions that arise due to oxygen deficiency in the brain.
Vitamin D3 entrapped nanoemulsion was formulated using a blend of Tween 20, PEG400 and oleic acid for the improvement in cerebral ischemia. The targeting potential of formulated nanoemulsion was analysed through gamma scintigraphy in a rat model. The developed nanoemulsion possessed an average globular size of ~49.29 nm with a positive 13.7 mV zeta potential. The stable thermodynamic preparation was found to have a permeation coefficient of 7.8 cm/h after 3 h in sheep nasal mucosa. Further, analysed radiometry and gamma scintigraphy displayed an efficient percentage deposition of 99mTc-vitamin D3 nanoemulsion across nasal mucosa compared to IV-administered solution (0.8%). The magnetic resonance imaging on the ischemic rat model confirmed the promising antioxidant action of developed nanoemulsion through the intranasal pathway [79].
The neuroprotective property of antioxidant safranal was explored in a focal ischemic model that contained major issues, including neurobehavioral loss, hippocampal cell loss and release of oxidative stress markers. Sadeghnia et al. (2017) developed a safranal-loaded nanoemulsion for intranasal delivery to overcome the above-said issues related to the cerebral ischemic rat model. The study significantly demonstrated a reduction in neurological, hippocampal cell loss and thiobarbituric acid reactive substances (TBARS). Moreover, marked increases in antioxidant capacity and SH content were also observed, suggesting a potential role of antioxidant herbal safranal in neuroprotection, free radical suppression and the treatment of cerebral ischemic reperfusion [80]. Antioxidant thymoquinone has poor aqueous solubility and bioavailability. Its neuroprotective action and potential to ameliorate cerebral ischemia have attracted researchers to explore the design of nanoemulsion. Mucoadhesive thymoquinone-loaded nanoemulsion was prepared via the ionic–gelation method. The formulated system comprised small globules (average size ~94.8 nm) with negative zeta potential (−13.5 mV). Viscosity and percentage drug content were reported as~110 cp and 99.86%, respectively.
The developed bioanalytical method displayed comparatively enhanced biodistribution and brain bioavailability after nasal route delivery than the intravenous pathway. Thymoquinone brain targeting potential was observed up to 89.97% after post-intranasal delivery of nanoemulsion. A performed neurobehavioral activity on the middle cerebral artery occlusion-persuaded ischemic rat model revealed the potential for antioxidant thymoquinone-embedded nanoemulsion to treat cerebral ischemia [81]. Table 4 lists some intranasal nanoemulsions applied for the control of cerebral ischemia.
3.4. Nanoemulsions in Brain Infections
Brain infections may occur in the regions of the cerebrum, cerebellum, spinal cord and associated nerves. In this context, encephalitis, meningitis and abscess are declared as medical emergencies and their long-term sequelae may result in substantial mortality. Bloodborne pathogens, head trauma and skull fractures can mediate the opening of tight junctions between the CNS and other nerves. Further, neurosurgical procedures and medical device implantation (exterior drainage tube, shunt) may cause infection due to microbial colonization and thus behaveas the foci of infection [86]. Rinaldi et al. (2020) suggested a successful nose-to-brain intranasal delivery route for the management of fatal meningitis and encephalitis. Essential oils composed of nanoemulsions (mean average diameter 100 nm with PDI 0.2) were chosen to transport at the infected site of the central nervous system. In this context, antibacterial oils extracted from Thymus vulgaris and Syzygium aromaticum were individually incorporated in the chitosan-coated nanoemulsions (C-TV-NEs and C-SA-NEs) and investigated against multidrug-resistant methicillin-susceptible S. aureus and carbapenem-resistant A. baumannii and K.pneumonia. Nanoemulsions, i.e., TV-NEs and SA-Nes, exhibited negative zeta potentials as −40 mV and −30 mV, respectively, that were converted into positive charges after chitosan coating by virtue of electrostatic interaction. However, the mean droplet size and PDI were amplified after the coating of the mucoadhesive chitosan polymer.
Intranasally administered nanoemulsions appeared more suitable for the potential curing of brain infections caused by Gram-negative bacteria compared to the intravenously delivered high dose of the formulation, presenting an efficient alternative therapy for the cure of serious meningitis and encephalitis [87]. A blend of essential oils is widely used to manage different virus infections caused by human rhinovirus, bovine rotavirus, herpes virus, H5N1 and HIV. Essential oils, such as thyme oil, eucalyptol, borneol, alpha terpineol and sage oil, are reported to be included in the formulation of nanoemulsion. Their mixture initiates nucleoprotein trafficking abnormalities in the surface protein of the virus, hence interfering or masking the virion envelope and blocking virus internalization [88]. A myriad of viruses, including poliovirus, rabies, herpes simplex and HIV, can reach the CNS through an intraneural path, causing encephalitis and brain abscesses, whereas meningitis is spread through bacterial pathogen at the subarachnoid space. Any breaches or damages (necrosis, microhemorrhage) of the BBB mechanical obstruction (infected RBCs, WBCs or platelets) and excessive production of cytokines disturb the structural architecture (tight junction) of BBB that led to the brain infection. Several reported pathogens, including a wide range of bacteria, fungi, viruses, cerebral malaria and spirochetes, are extensive causes of CNS or brain infections [89].
The immunologically privileged central nervous system (CNS) remains the residing site for human immunodeficiency virus 1. Poor permeability across the tight junctions of BBB leads to inadequate and limited delivery of most of the anti-HIV therapeutics. Therefore, nanotechnology-based formulations have attracted medical scientists and researchers to design novel strategies for the management of neuro-AIDS. Saquinavir mesylate, a protease inhibitor, has been explored as an antiretroviral drug, but due to poor solubility and bioavailability (4%), its use is limited. O/W intranasal nanoemulsion containing saquinavir mesylate was formulated via a spontaneous emulsification method to enhance CNS bioavailability. The developed nanoemulsion was thermodynamically stable on analysing through freeze–thaw and heating–cooling cycles. The obtained low PDI (0.078) and smaller globular diameter (176.3 nm) indicated the development of monodispersed nanoemulsion that would be suitable for brain targeting via intranasal delivery. Estimated optimum zeta potential (−10.3 mV), pH (5.8) and refractive index (1.412) depicted good stability, non-irritancy and the compatibility of nanoemulsion. Higher-percentage drug permeation and permeability coefficients after 4 h on intranasal administration were observed as 76.96% and 0.51 cm/h, respectively, compared to the pure drug (26.73%, 0.17 cm/h).
The in vivo study in sheep nasal mucosa displayed higher drug permeation and biodistribution rate of nanoemulsion on comparing with its suspension. Further, the cilia-toxicity study depicted no prominent adverse action on the sheep nasal mucosa. Gamma scintigraphy images demonstrated higher drug transportation region in the rat brain that concluded its efficiency for treating neuro-AIDS by reducing the devastating viral load from reservoir sites [90].
3.5. Nanoemulsions in Migraine and Cerebral Vasospasm
Another neuron-disabling disorder, ‘migraine’, is characterized by intense throbbing headaches in one of the halves of the brain. One of the surveys demonstrated that migraine is the sixth most prevailing brain disorder and affects approximately 15% of sufferers worldwide [91].
Recurrent episodes of pain in unilateral headaches are allied with other visual, auditory and autonomic nervous disorders. Mostly, females are more affected due to their poor lifestyle. The pain is so intense and unbearable that the patient needs quick relief from it [92]. Poor solubility, erratic absorption, inadequate permeation and fewerpenetration properties of most of the conventional therapies across BBB led to poor efficacy in the brain region. Delayed gastric emptying, first-pass metabolism, slow onset of action, nausea and vomiting and the intake of high doses are undesirable issues associated with anti-migraine drugs if given orally.
The intranasal route is more effective for the delivery of anti-migraine therapeutics owing to the involvement of olfactory and trigeminal nerves. These anatomical features are potentially involved in the greater distribution of drugs without facing issues of first-pass metabolism [93].
Rizatriptan, a serotonin 5HT 1B/1D receptor agonist, exhibits only a 40% bioavailability upon oral delivery. An intranasal preparation of rizatriptan benzoate nanoemulsion improved brain tissue deposition and offered a non-invasive alternative approach for brain targeting. Biodistribution through the olfactory pathway directly delivers the drug to the central nervous system [94]. Another well-tolerated anti-migraine drug, zolmitriptan, also possesses low bioavailability after oral administration. Ahigh-dose prescription in conventional preparation causes serious side effects, including irregular heart rhythm, stroke and Raynaud’s disease. Ebtsam et al., 2017 formulated a mucoadhesive nanoemulsion for the direct nose-to-brain transportation of zolmitriptan. The improved and quick onset of action is desired to alleviate acute migraine fulfilled with this formulation. An added 0.3% of chitosan acted as a mucoadhesive agent in the preparation and increased the residing time and drug permeation across associated nasal mucosa, hence assisting the transport of the drug to the brain tissues. Performed in vivo studies displayed shorter Tmax and higher AUC0–8 of intranasally administered nanoemulsion compared to intravenous or nasal zolmitriptan solution [95]. Sumatriptan has been widely employed for the management of severe and painful migraine for decades. High hydrophilicity and less mucoadhesive features limit its application through the nasal route. Ribeiro et al. 2020 have developed a novel nanoemulsion containing sumatriptan, copaiba oil and organic biopolymers. i.e., alginate, pullulan, xanthan and pectin. Mean particle size, PDI and zeta potential of nanoemulsion were observed as approximately 120 nm, 0.2 and −25 mV, respectively.
The developed alginate-based nanoemulsion exhibited long term storage stability (1 year) due to optimised zeta potential. In vitro study depicted extended release from sumatriptan-loaded alginate nanoemulsion upto 24 h. The in vivo toxicity in the zebrafish model revealed no evidence of mortality and other cardiac toxicity and did not disturb spontaneous changes in zebrafish larvae, hence showing a promising alternative approach for the alleviation of brain diseases, including migraine [96].
Cerebral vasospasm is defined as the temporary narrowing or thinning of cerebral arteries. More often, subarachnoid haemorrhage and traumatic brain injuries result in cerebral vasospasm.
The appearance of new focal neurological signs, inflammation, microcirculatory failure, bipolar disorders and loss of consciousness re-associated aspects are addressed with subarachnoid haemorrhage [97]. Cerebral vasospasm is the leading cause of mortality if not identified and treated immediately. It typically affects concerned blood vessels at the skull base that influences arterial contraction, blood pressure and blood viscosity. Figure 4 defines different causes of cerebral vasospasm and its different signs and symptoms that have appeared in the sufferer.
Endovascular therapies are recommended for the management of severe vasospasm cases. However, the radiological and computed tomography evidence suggested that approximately 20% of cases of vasospasm can be treated via performing angiograms within a week of aneurysmal rupture. Some clinical reports also described that the level of nitric oxide was found to be decreased due to vasoconstrictor endothelin and extra vascular oxyhaemoglobin [98].
Cerebral vasospasm is often evident after aneurysmal subarachnoid haemorrhage. However, in some instances, it is observed after skull surgery associated with intractable epilepsy and amygdala-hippocampectomy. Carbamazepine 400 mg is recommended to overcome developed issues in this case. Dhobale et al., 2018 formulated carbamazepine nanoemulsion for efficient brain targeting via the intranasal route. A spontaneous emulsification method was employed for the formulation of nanoemulsion utilizing Capmul MCM (oil) and TWEEN 80/PEG-600 (3:1) as surfactant and co-surfactant, respectively. The developed nanoemulsion contained a smaller globular size of ~71.7 nm with a 0.256 ± 0.002 polydispersity index. The in vivo study depicted efficient drug distribution in 5 h [99]. Survival from cerebral vasospasm or aneurysmal subrachanoid haemorrhage was improved. FDA-approved nimodine is a calcium channel blocker and is widely prescribed clinically to treat subarachnoid haemorrhage. In this series, fasudil (Rho-kinase inhibitor), nicardipine (calcium channel blocker), statins (hypolipidemic), clazosentan (endothelin receptor antagonist), cilostazol (platelet aggregation factor and heparin (anticoagulant) has also been added as effective therapeutics in clinical practice [100].
Ahmad et al. have discussed a novel bioimaging tool. i.e., targeting probe that is based on an on–off signal and significantly traces the translocation of the therapeutic agent throughout the nose-to-brain pathway. A cargo was developed containing environmentally responsive dye P2 and P4, caumarin 6 and DiR conventional probes. Translocation of nanoemulsion (prepared with Labrafac®CC/ WL1349 and solutol®HS15) after intranasal administration was evident either via bioimaging or through histopathological examination in rats. Outcomes concluded that nanoemulsions (coated with chitosan and naked) with a mean particle size of 100 nm exhibited higher retention duration in the nasal cavity with slower clearance compared to larger particles. Weak P2 and P4 signals were also observed in the region of the olfactory bulb for coated nanoemulsions of particle size 100 nm. Moreover, nanoemulsion particle sizes of more than 900 nm were unable to reach the olfactory bulb. Signals obtained from caumarin 6 and DiR represented significant transportation of nanoemulsion in the brain region.
The importance of particle size and their cytoprotective efficiency under the circumstances of oxygen–glucose deprivation and reoxygenation were also signified by Varlamova and coworkers in 2022. It was reported that the average particle size of selenium (50 nm) could induce calcium ion responses and inhibit apoptosis in the brain cortex cells. At the same time, upon increasing particle size, i.e., 100 nm and 400 nm, exhibited induction of calcium ion oscillation and mixed pattern of calcium signals, respectively. Hence, cryoprotective action under oxygen–glucose deprivation and reoxygenation conditions can be provided at the size range 50–400 nm that is required to protect brain tissues from ischemic conditions through modulation of the calcium ions signal system of astrocytes [101,102].
4. Future Prospects and Conclusions
Although intranasal nanoemulsions successfully deliver therapeutics with minimum side effects at the site, several formulation aspects (type of oil, polymer and surfactant/cosurfactant), process stabilizing parameters (methodology, temperature, rheology, particle size) and pharmacokinetic issues (solubility, absorption, bioavailability) always create challenges for the competent treatment of brain disorders. High molecular weight containing hydrophilic therapeutics poses problems for nanoemulsion formulation. Enormous work on the preparation and evaluation of intranasal nanoemulsions has been reported within 5 years for the management of myriad brain-associated ailments. Nanoemulsions prepared with mucoadhesive polymers and in situ nanoemulgels confine fast nasal clearance and improve residing time and permeation of bioactive across the nose-to-brain pathway.
Mucoadhesive starch-based polymers (potato starch, wheat starch, rice starch), gaur gum, xanthan gum and tragacanth are not only safe, cost-effective and eco-friendly but also are proven natural components that make intimate contact between nasomucosal membrane and nanoemulsions system. Similarly, in situ nanoemulgels embedded with nanocarriers comprise stimuli-sensitive (pH, temperature, ionic concentration) ingredients that respond to the environment of the nasal cavity and augment the viscosity of the nanoemulsion system. Therefore, surged biodistribution and improved contact time across nasomucosal membranes overcome shortcomings of nanoemulsions and offer a safe and desirable benchmark for targeting brain diseases. Although mucoadhesive and in situ nanoemulgels are fascinating strategies, formulation aspects (osmolarity, pH, buffer capacity, viscosity, drug concentration) and physiological parameters (absorption, nasal blood flow, mucociliary clearance, enzymatic action, pathophysiological issue) are still to be monitored for the effective delivery of therapeutics via the nose-to-brain route.
Currently, nose-to-brain targeted rationally designed nanoemulsions have been proven as a successful alternate approach for the precise alleviation of countless brain-associated disorders. Adequate endothelial cell internalization by nanoemulsion via transcytosis and endocytosis mechanisms mediate desirable therapeutic effects with minimum adverse effects. Associated olfactory and trigeminal pathways facilitate biodistribution and bypass issues with the BBB barrier and drug first-pass metabolism. Exploring these virtues, intra-nasal nanoemulsions have proven brain-targeting cargos with their broad array of applications. Recently, targeting probes that contain environment-responsive dyes have been employed for the tracking of bio translocation of the nanoemulsion via fluorescence bioimaging technology. This strategy validates the efficacy of the nanoemulsion with evidence.
Author Contributions
Conceptualization, review and editing: K.P., original draft preparation: S.K.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data is generated.
Acknowledgments
The authors thankfully acknowledge the amenities provided by the School of Pharmaceutical Sciences, Chhatrapati Shahu Ji Maharaj University, Kanpur, for consenting to all working facilities for drafting this manuscript. Our sincere acknowledgments also go to the Faculty of Pharmacy, Uttar Pradesh University of Medical Sciences, Saifai, Etawah, for their generous assistance in assembling the data presented in this review article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Liu, P.; Jiang, C. Brain-targeting drug delivery systems. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2022, 14, e1818. [Google Scholar] [CrossRef]
- Pajouhesh, H.; Lenz, G.R. Medicinal chemical properties of successful central nervous system drugs. NeuroRx 2005, 2, 541–553. [Google Scholar] [CrossRef] [Green Version]
- Daneman, R.; Prat, A. The blood-brain barrier. Cold Spring Harb. Perspect. Biol. 2015, 7, a020412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banks, W.A. From blood-brain barrier to blood-brain interface: New opportunities for CNS drug delivery. Nat. Rev. Drug. Discov. 2016, 15, 275–292. [Google Scholar] [CrossRef]
- Kaushik, A.; Jayant, R.D.; Bhardwaj, V.; Nair, M. Personalized nano medicine for CNS diseases. Drug. Discov. Today 2018, 23, 1007–1015. [Google Scholar] [CrossRef]
- Jaiswal, M.; Dudhe, R.; Sharma, P.K. Nanoemulsion: An advanced mode of drug delivery system. 3 Biotech. 2015, 5, 123–127. [Google Scholar] [CrossRef] [Green Version]
- Dhuria, S.V.; Hanson, L.R.; Frey, W.H. Intranasal delivery to the central nervous system: Mechanisms and experimental considerations. J. Pharm. Sci. 2010, 99, 1654–1673. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.M.; Bleier, B.S. The blood-brain barrier and nasal drug delivery to the central nervous system. Am. J. Rhinol. Allergy 2015, 29, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Jones, N. The nose and paranasal sinuses physiology and anatomy. Adv. Drug. Deliv. Rev. 2001, 51, 5–19. [Google Scholar] [CrossRef]
- Pardeshi, C.V.; Belgamwar, V.S. Direct nose to brain drug delivery via integrated nerve pathways by passing the blood-brainbarrier: An excellent platform for brain targeting. Expert. Opin. Drug. Deliv. 2013, 10, 957–972. [Google Scholar] [CrossRef]
- Rassu, G.; Soddu, E.; Cossu, M.; Brundu, A.; Cerri, G.; Marchetti, N.; Ferraro, L.; Regan, R.F.; Giunchedi, P.; Gavini, E.; et al. Solid microparticles based on chitosan or methyl-β-cyclodextrin: A first formulative approach to increase the nose-to-brain transport of deferoxamine mesylate. J. Control. Release 2015, 201, 68–77. [Google Scholar] [CrossRef] [Green Version]
- Erdő, F.; Bors, L.A.; Farkas, D.; Bajza, Á.; Gizurarson, S. Evaluation of intranasal delivery route of drug administration for brain targeting. Brain Res. Bull. 2018, 143, 155–170. [Google Scholar] [CrossRef]
- Mistry, A.; Stolnik, S.; Illum, L. Nose-to-brain delivery: Investigation of the transport of nanoparticles with different surface characteristics and sizes in excised porcine olfactory epithelium. Mol. Pharm. 2015, 12, 2755–2766. [Google Scholar] [CrossRef] [PubMed]
- Quintana, D.S.; Guastella, A.J.; Westlye, L.T.; Andreassen, O.A. The promise and pitfalls of intranasally administering psychopharmacological agents for the treatment of psychiatric disorders. Mol. Psychiatry 2016, 21, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.; McClements, D.J. Application of advanced emulsion technology in the food industry: A review and critical evaluation. Foods 2021, 10, 812. [Google Scholar] [CrossRef] [PubMed]
- Siasios, I.; Kapsalaki, E.Z.; Fountas, K.N. Cerebral vasospasm pharmacological treatment: An update. Neurol. Res. Int. 2013, 2013, 571328. [Google Scholar] [CrossRef]
- Shen, R.; Yang, X.; Lin, D. pH sensitive double-layered emulsions stabilized by bacterial cellulose nanofibers/soy protein isolate/chitosan complex enhanced the bio accessibility of curcumin: In vitro study. Food Chem. 2023, 402, 134262. [Google Scholar] [CrossRef]
- Piacentini, E.; Figoli, A.; Giorno, L.; Drioli, E. Membrane Emulsification. In Comprehensive Membrane Science and Engineering; Drioli, E., Ed.; Elsevier: Amsterdam, The Netherlands, 2010; pp. 47–78. [Google Scholar]
- Guzmán, E.; Ortega, F.; Rubio, R.G. Pickering Emulsions: A Novel Tool for Cosmetic Formulators. Cosmetics 2022, 9, 68. [Google Scholar] [CrossRef]
- Gao, H.; Ma, L.; Cheng, C.; Liu, J.; Liang, R.; Zou, L.; Liu, W.; McClements, D.J. Review of recent advances in the preparation, properties, and applications of high internal phase emulsions. Trends Food Sci. Technol. 2021, 112, 36–49. [Google Scholar] [CrossRef]
- Costa, C.P.; Moreira, J.N.; Sousa, L.J.M.; Silva, A.C. Intranasal delivery of nanostructured lipid carriers, solid lipid nanoparticles and nanoemulsions: A current overview of in vivo studies. Acta Pharm. Sin. B 2021, 11, 925–940. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, H.; Gorain, B.; Karmakar, S.; Biswas, E.; Dey, G.; Barik, R.; Mandal, M.; Pal, T.K. Improvement of cellular uptake, in vitro antitumor activity and sustained release profile with increased bioavailability from a nanoemulsion platform. Int. J. Pharm. 2014, 460, 131–143. [Google Scholar] [CrossRef]
- Edmond, J. Essential polyunsaturated fatty acids and the barrier to the brain: The components of a model for transport. J. Mol. Neurosci. 2001, 16, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Singh, Y.; Meher, J.G.; Raval, K.; Khan, F.A.; Chaurasia, M.; Jain, N.K.; Chourasia, M.K. Nanoemulsion: Concepts, development and applications in drug delivery. J. Control. Release 2017, 252, 28–49. [Google Scholar] [CrossRef] [PubMed]
- Kumar, G.; Virmani, T.; Pathak, K.; Kamaly, O.A.; Saleh, A. Central Composite Design Implemented Azilsartan Medoxomil Loaded Nanoemulsion to Improve Its Aqueous Solubility and Intestinal Permeability: In Vitro and Ex Vivo Evaluation. Pharmaceuticals 2022, 15, 1343. [Google Scholar] [CrossRef]
- Morrison, E.E.; Costanzo, R.M. Morphology of olfactory epithelium in humans and other vertebrates. Microsc. Res. Tech. 1992, 23, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Phukan, K.; Nandy, M.; Sharma, R.B.; Sharma, H.K. Nanosized Drug Delivery Systems for Direct Nose to Brain Targeting: A Review. Recent. Pat. Drug. Deliv. Formul. 2016, 10, 156–164. [Google Scholar] [CrossRef]
- Djupesland, P.G.; Messina, J.C.; Mahmoud, R.A. The nasal approach to delivering treatment for brain diseases: An anatomic, physiologic, and delivery technology overview. Ther. Deliv. 2014, 5, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Hosny, K.M.; Banjar, Z.M. The formulation of a nasal nanoemulsion zaleplon in situ gel for the treatment of insomnia. Expert Opin. Drug. Deliv. 2013, 10, 1033–1041. [Google Scholar] [CrossRef]
- Chatterjee, B.; Gorain, B.; Mohananaidu, K.; Sengupta, P.; Mandal, U.K.; Choudhury, H. Targeted drug delivery to the brain via intranasal nanoemulsion: Available proof of concept and existing challenges. Int. J. Pharm. 2019, 565, 258–268. [Google Scholar] [CrossRef]
- Bonferoni, M.C.; Rossi, S.; Sandri, G.; Ferrari, F.; Gavini, E.; Rassu, G.; Giunchedi, P. Nanoemulsions for "Nose-to-Brain" Drug Delivery. Pharmaceutics 2019, 11, 84. [Google Scholar] [CrossRef] [Green Version]
- Izquierdo, P.; Esquena, J.; Tadros, T.F.; Dederen, C.; Garcia, M.J.; Azemar, N.; Solans, C. Formation and stability of nanoemulsions prepared using the phase inversion temperature method. Langmuir 2002, 18, 26–30. [Google Scholar] [CrossRef]
- Sood, S.; Jain, K.; Gowthamarajan, K. Optimization of curcumin nanoemulsion for intranasal delivery using design of experiment and its toxicity assessment. Colloids Surf. B Bio. Interfaces 2014, 113, 330–337. [Google Scholar] [CrossRef]
- Bahadur, S.; Pardhi, D.M.; Rautio, J.; Rosenholm, J.M.; Pathak, K. Intranasal nanoemulsions for direct nose-to-brain delivery of actives for CNS disorders. Pharmaceutics 2020, 12, 1230. [Google Scholar] [CrossRef]
- Samaridou, E.; Alonso, M.J. Nose-to-brain peptide delivery—The potential of nano technology. Bioorg. Med. Chem. 2018, 26, 2888–2905. [Google Scholar] [CrossRef] [PubMed]
- Dalpiaz, A.; Fogagnolo, M.; Ferraro, L.; Capuzzo, A.; Pavan, B.; Rassu, G.; Salis, A.; Giunchedi, P.; Gavini, E. Nasal chitosan microparticles target a zidovudine prodrug to brain HIV sanctuaries. Antiviral. Res. 2015, 123, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Diedrich, C.; Camargo, Z.I.; Schineider, M.C.; Taise, F.M.; Maissar, K.N.; Badea, I.; Mara, M.R. Mucoadhesive nanoemulsion enhances brain bioavailability of luteolin after intranasal administration and induces apoptosis to SH-SY5Y neuroblastoma cells. Int. J. Pharm. 2022, 626, 122142. [Google Scholar] [CrossRef]
- Rassu, G.; Porcu, E.P.; Fancello, S.; Obinu, A.; Senes, N.; Galleri, G.; Migheli, R.; Gavini, E.; Giunchedi, P. Intranasal delivery of genistein-loaded nanoparticles as a potential preventive system against neurodegenerative disorders. Pharmaceutics 2018, 11, 8. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Eral, H.B.; Hatton, T.A.; Doyle, P.S. Nanoemulsions: Formation, properties and applications. Soft Matter 2016, 12, 2826–2841. [Google Scholar] [CrossRef] [Green Version]
- Prakash, R.T.; Thiagarajan, P. Nanoemulsions for drug delivery through different routes. Res. Biotechnol. 2011, 2, 1–13. [Google Scholar]
- Mehta, M.; Adem, A.; Sabbagh, M.N. New acetylcholinesterase inhibitors for Alzheimer’s disease. Int. J. Alzheimer’s Dis. 2012, 2012, 728983. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Jiang, Y.; Ding, Z.; Yu, Q. Investigation of the "Nose-to-Brain" pathways in intranasal Hup Anan emulsions and evaluation of their in vivo pharmacokinetics and brain-targeting ability. Int. J. Nanomed. 2022, 17, 3443–3456. [Google Scholar] [CrossRef] [PubMed]
- Parikh, H.R.; Patel, J.R. Nanoemulsions for intranasal delivery of riluzole to improve brain bioavailability: Formulation development and pharmacokinetic studies. Curr. Drug. Deliv. 2016, 13, 1130–1143. [Google Scholar] [CrossRef]
- Usama, A.M.; Vyas, P.; Vohora, D.; Kumar, S.P.; Nigam, K.; Dang, S.; Ali, J.; Baboota, S. Amelioration of oxidative stress utilizing nanoemulsion loaded with bromocriptine and glutathione for the management of Parkinson’s disease. Int. J. Pharm. 2022, 618, 121683. [Google Scholar] [CrossRef]
- Patel, R.J.; Parikh, R.H. Intranasal delivery of topiramate nanoemulsion: Pharmacodynamic, pharmacokinetic and brain uptake studies. Int. J. Pharm. 2020, 585, 119486. [Google Scholar] [CrossRef] [PubMed]
- Kaur, A.; Nigam, K.; Srivastava, S.; Tyagi, A.; Dang, S. Memantine nanoemulsion: A new approach to treat alzheimer’s disease. J. Microencapsul. 2020, 37, 355–365. [Google Scholar] [CrossRef]
- Kaur, A.; Nigam, K.; Bhatnagar, I.; Sukhpal, H.; Awasthy, S.; Shanka r, S.; Tyagi, A.; Dang, S. Treatment of Alzheimer’s disease using donepezil nanoemulsion: An intranasal approach. Drug. Deliv. Transl. Res. 2020, 10, 1862–1875. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Liu, C.; Zhai, W.; Zhuang, N.; Han, T.; Ding, Z. The optimization design of lactoferrin loaded hup A nanoemulsion for targeted drug transport via intranasal route. Int. J. Nanomed. 2019, 14, 9217–9234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotta, S.; Mubarak, A.H.; Badr-Eldin, S.M.; Alhakamy, N.A.; Md, S. Coconut oil-based resveratrol nanoemulsion: Optimization using response surface methodology, stability assessment and pharmacokinetic evaluation. Food Chem. 2021, 357, 129721. [Google Scholar] [CrossRef]
- Das, S.S.; Sarkar, A.; Chabattula, S.C.; Verma, P.R.P.; Nazir, A.; Gupta, P.K.; Ruokolainen, J.; Kesari, K.K.; Singh, S.K. Food-grade quercetin-loaded nanoemulsion ameliorates effects associated with Parkinson’s disease and cancer: Studies employing atransgenic C. elegans model and human cancer cell lines. Antioxidants 2022, 11, 1378. [Google Scholar] [CrossRef]
- Gaba, B.; Khan, T.; Haider, M.F.; Alam, T.; Baboota, S.; Parvez, S.; Ali, J. Vitamin Eloaded naringenin nanoemulsion via intranasal delivery for the management of oxidative stress in a 6-OHDA Parkinson’s disease model. Biomed Res. Int. 2019, 2019, 2382563. [Google Scholar] [CrossRef]
- Kumar, S.; Ali, J.; Baboota, S. Design Expert(®) Supported optimization and predictive analysis of selegiline nanoemulsion via the olfactory region with enhanced behavioural performance in Parkinson’s disease. Nanotechnology 2016, 27, 435101. [Google Scholar] [CrossRef] [PubMed]
- Nasr, M. Development of An optimized hyaluronic acid-based lipidic nanoemulsion co-encapsulating two polyphenols for nose to brain delivery. Drug. Deliv. 2016, 23, 1444–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, N.; Ahmad, R.; Alam, M.A.; Ahmad, F.J.; Amir, M. Impact of ultrasonication techniques on the preparation of novel amiloride-nanoemulsion used for intranasal delivery in the treatment of epilepsy. Artif. Cells Nanomed. Biotechnol. 2018, 46, S192–S207. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, R.; Ahmed, S.; Jain, G.K.; Vohora, D. Design and development of letrozolen an emulsion: A comparative evaluation of brain targeted nanoemulsion with free letrozole against status epilepticus and neurodegeneration in mice. Int. J. Pharm. 2019, 565, 20–32. [Google Scholar] [CrossRef] [PubMed]
- El-Zaafarany, G.M.; Soliman, M.E.; Mansour, S.; Cespi, M.; Palmieri, G.F.; Illum, L.; Casettari, L.; Awad, G.A.S. A Tailored Thermosensitive PLGA-PEG-PLGA/emulsomes composite for enhanced oxcarbazepine brain delivery via the nasal route. Pharmaceutics 2018, 10, 217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Md, S.; Gan, S.Y.; Haw, Y.H.; Ho, C.L.; Wong, S.; Choudhury, H. In vitro neuroprotective effects of naringenin nanoemulsion against β-amyloid toxicity through the regulation of amyloid genesis and tau phosphorylation. Int. J. Biol. Macromol. 2018, 118, 1211–1219. [Google Scholar] [CrossRef]
- Ramires Júnior, O.V.; Alves, B.D.S.; Barros, P.A.B.; Rodrigues, J.L.; Ferreira, S.P.; Monteiro, L.K.S.; Araújo, G.M.S.; Fernandes, S.S.; Vaz, G.R.; Dora, C.L.; et al. Nanoemulsion improves the neuroprotective effects of curcumin in an experimental model of Parkinson’s disease. Neurotox. Res. 2021, 39, 787–799. [Google Scholar] [CrossRef]
- Geetha, K.M.; Shankar, J.; Wilson, B. Neuroprotective effect of chia seed oil nanoemulsion against rotenone induced motor impairment and oxidative stress in mice model of Parkinson’s disease. Adv. Tradit. Med. 2022. [Google Scholar] [CrossRef]
- Pandey, Y.R.; Kumar, S.; Gupta, B.K.; Ali, J.; Baboota, S. Intranasal delivery of paroxetine nanoemulsion via the olfactory region for the management of depression: Formulation, behavioural and biochemical estimation. Nanotechnology 2016, 27, 025102. [Google Scholar] [CrossRef]
- Samiun, W.S.; Ashari, S.E.; Salim, N.; Ahmad, S. Optimization of processing parameters of nanoemulsion containing aripiprazole using response surface methodology. Int. J. Nanomed. 2020, 15, 1585–1594. [Google Scholar] [CrossRef] [Green Version]
- Kumbhar, S.A.; Kokare, C.R.; Shrivastava, B.; Gorain, B.; Choudhury, H. Preparation, characterization, and optimization of asenapine maleate mucoadhesive nanoemulsion using Box-Behnken design: In vitro and in vivo studies for brain targeting. Int. J. Pharm. 2020, 586, 119499. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Patil, K.; Yeole, P.; Gaikwad, R. Brain targeting studies on buspirone hydrochloride after intranasal administration of mucoadhesive formulation in rats. J. Pharm. Pharmacol. 2009, 61, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N.; Khalid, M.S.; Al Ramadhan, A.M.; Alaradi, M.Z.; Al Hammad, M.R.; Ansari, K.; Alqurashi, Y.D.; Khan, M.F.; Albassam, A.A.; Ansari, M.J.; et al. Preparation of melatonin novel-mucoadhesive nanoemulsion used in the treatment of depression. Polym. Bull. 2022, 1–40. [Google Scholar] [CrossRef]
- Saenzdel Burgo, L.; Hernández, R.M.; Orive, G.; Pedraz, J.L. Nanotherapeutic approaches for brain cancer management. Nanomedicine 2014, 10, 905–919. [Google Scholar] [CrossRef] [PubMed]
- Chu, L.; Wang, A.; Ni, L.; Yan, X.; Song, Y.; Zhao, M.; Sun, K.; Mu, H.; Liu, S.; Wu, Z.; et al. Nose-to-brain delivery of temozolomide-loaded PLGA nano particles functionalized with anti-EPHA3 for glioblastoma targeting. Drug. Deliv. 2018, 25, 1634–1641. [Google Scholar] [CrossRef] [Green Version]
- Yan, A.; Joachims, M.L.; Thompson, L.F.; Miller, A.D.; Canoll, P.D.; Bynoe, M.S. CD73 promotes glioblastoma pathogenesis and enhances its chemoresistance via A2B adenosine receptor signaling. J. Neurosci. 2019, 39, 4387–4402. [Google Scholar] [CrossRef] [Green Version]
- Chaskis, E.; Luce, S.; Goldman, S.; Sadeghi, N.; Melot, C.; De Witte, O.; Devriendt, D.; Lefranc, F. Early postsurgical temozolomide treatment in newly diagnosed bad prognosis glioblastoma patients: Feasibility study. Bull. Cancer 2018, 105, 664–670. [Google Scholar] [CrossRef]
- Ban, M.M.; Chakote, V.R.; Dhembre, G.N.; Rajguru, J.R.; Joshi, D.A. In-situ gel for nasal drug delivery. Int. J. Dev. Res. 2013, 8, 18763–18769. [Google Scholar]
- Bayanati, M.; Khosroshahi, A.G.; Alvandi, M.; Mahboobian, M.M. Fabrication of a Thermosensitive In Situ Gel Nanoemulsion for Nose to Brain Delivery of Temozolomide. J. Nanomater. 2021, 2021, 1–11. [Google Scholar] [CrossRef]
- Colombo, M.; Figueiró, F.; de Fraga, D.A.; Teixeira, H.F.; Battastini, A.M.O.; Koester, L.S. Kaempferol-loaded mucoadhesive nanoemulsion for intranasal administration reduces glioma growth in vitro. Int. J. Pharm. 2018, 543, 214–223. [Google Scholar] [CrossRef]
- Mahajan, H.S.; Patil, N.D. Nanoemulsion containing a synergistic combination of curcumin and quercetin for nose-to-brain delivery: In vitro and in vivo studies. Asian Pac. J. Trop. Biomed. 2021, 11, 510–518. [Google Scholar] [CrossRef]
- Azambuja, J.H.; Schuh, R.S.; Michels, L.R.; Gelsleichter, N.E.; Beckenkamp, L.R.; Iser, I.C.; Lenz, G.S.; de Oliveira, F.H.; Venturin, G.; Greggio, S.; et al. Nasal Administration of cationic nanoemulsions as CD73-siRNA delivery system for glioblastoma to treatment: A new therapeutical approach. Mol. Neurobiol. 2020, 57, 635–649. [Google Scholar] [CrossRef]
- Qu, Y.; Li, A.; Ma, L.; Iqbal, S.; Sun, X.; Ma, W.; Li, C.; Zheng, D.; Xu, Z.; Zhao, Z.; et al. Nose-to-brain delivery of disulfiram nanoemulsion in situ gel formulation for glioblastoma targeting therapy. Int. J. Pharm. 2021, 597, 120250. [Google Scholar] [CrossRef]
- Savale, S.K. Formulation and evaluation of quercetin nanoemulsions for treatment of brain tumor via intranasal pathway. Asian J. Biomater. Res. 2017, 3, 28–32. [Google Scholar]
- Desai, A.; Vyas, T.; Amiji, M. Cytotoxicity and apoptosis enhancement in brain tumor cells upon coadministration of paclitaxel and ceramide in nanoemulsion formulations. J. Pharm. Sci. 2008, 97, 2745–2756. [Google Scholar] [CrossRef]
- Qu, Y.; Sun, X.; Ma, L.; Li, C.; Xu, Z.; Ma, W.; Zhou, Y.; Zhao, Z.; Ma, D. Therapeutic effect of disulfiram inclusion complex embedded in hydroxypropyl-β-cyclodextrin on intracranial glioma-bearing male rats via intranasal route. Eur. J. Pharm. Sci. 2021, 156, 105590. [Google Scholar] [CrossRef]
- Martini, S.R.; Kent, T.A. Ischemic Stroke. In Cardiology Secrets, Ved.; Glenn, N.L., Ed.; Elsevier: Philadelphia, PA, USA, 2018; pp. 493–504. [Google Scholar]
- Kumar, M.; Nishad, D.K.; Kumar, A.; Bhatnagar, A.; Karwasra, R.; Khanna, K.S.K.; Sharma, D.; Dua, K.; Mudaliyar, V.; Sharma, N. Enhancement in brain uptake of vitamin D3 nanoemulsion for treatment of cerebral ischemia: Formulation, gamma scintigraphy andefficacy study in transient middle cerebral artery occlusion rat models. J. Microencapsul. 2020, 37, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Sadeghnia, H.R.; Shaterzadeh, H.; Forouzanfar, F.; Hosseinzadeh, H. Neuroprotective effect of safranal, an active ingredient of Crocus sativus, in a rat model of transient cerebral ischemia. Folia Neuropathol. 2017, 55, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N.; Ahmad, R.; Alam, M.A.; Samim, M.; Iqbal, Z.; Ahmad, F.J. Quantification and evaluation of thymoquinone loadedmucoadhesivenanoemulsionfortreatmentofcerebralischemia. Int. J. Biol. Macromol. 2016, 88, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N.; Ahmad, R.; Abbas, N.A.; Ashafaq, M.; Alam, M.A.; Ahmad, F.J.; Al-Ghamdi, M.S. The effect of safranal loaded mucoadhesive nanoemulsion on oxidative stress markers in cerebral ischemia. Artif. Cells Nanomed. Biotechnol. 2017, 45, 775–787. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, C.; Zhang, W.; Yang, T.; Xia, M.; Lei, X.; Peng, Y.; Wu, Y.; Feng, J.; Li, D.; et al. Preparation, In vitro and in vivo evaluation of nanoemulsion in situ gel for transnasal delivery of traditional Chinese medicine volatile oil from Ligusticumsinense Oliv.cv. Chaxiong. Molecules 2022, 27, 7644. [Google Scholar] [CrossRef]
- Niyaz, A.; Rizwan, A.; Mohd, A.; Md, A.; Alam, M.Z.A.; Abuzer, A.; Ahmad, A.; Ashraf, K. Ischemic brain treated with 6-gingerol loaded mucoadhesive nanoemulsion via intranasal delivery and their comparative pharmacokinetic effect in brain. J. Drug. Deliv. Sci. Technol. 2021, 61, 102130. [Google Scholar]
- Nemade, S.M.; Kakad, S.P.; Kshirsagar, S.J.; Padole, T.R. Development of nanoemulsion of antiviral drug for brain targeting in the treatment of neuro-AIDS. Beni-Suef Univ. J. Basic. Appl. Sci. 2022, 11, 138. [Google Scholar] [CrossRef]
- Solomon, I.H. Molecular and Histologic Diagnosis of Central Nervous System Infections. Surg. Pathol. Clin. 2020, 13, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, F.; Oliva, A.; Sabatino, M.; Imbriano, A.; Hanieh, P.N.; Garzoli, S.; Mastroianni, C.M.; DeAngelis, M.; Miele, M.C.; Arnaut, M.; et al. Antimicrobial essential oil formulation: Chitosan coated nanoemulsions for nose to brain delivery. Pharmaceutics 2020, 12, 678. [Google Scholar] [CrossRef] [PubMed]
- Franklyne, J.S.; Gopinath, P.M.; Mukherjee, A.; Chandrasekaran, N. Nanoemulsions: The rising star of antiviral therapeutics and nano delivery system-current status and prospects. Curr. Opin. Colloid. Interface Sci. 2021, 54, 101458. [Google Scholar] [CrossRef]
- Giovane, R.A.; Lavender, P.D. Central Nervous System Infections. Prim. Care 2018, 45, 505–518. [Google Scholar] [CrossRef]
- Hitendra, S.; Mahajan, M.S.; Mahajan, P.P.; Nerkar Agrawal, A. Nanoemulsion-based intranasal drug delivery system of saquinavir mesylate for brain targeting. Drug. Deliv. 2014, 21, 148–154. [Google Scholar]
- Vos, T.; Abajobir, A.A.; Abate, K.A. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries,1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.K.; Wang, S.J. Non-headache symptoms in migraine patients. F1000Research 2018, 7, 188. [Google Scholar] [CrossRef] [Green Version]
- Tanna, V.; Sawarkar, S.P.; Ravikumar, P. Exploring nose to brain nano delivery for effective management of migraine. Curr. Drug. Deliv. 2023, 20, 144–157. [Google Scholar] [CrossRef] [PubMed]
- Bhanushali, R.S.; Gatne, M.M.; Gaikwad, R.V.; Bajaj, A.N.; Morde, M.A. Nanoemulsion based intranasal delivery of antimigraine drugs for nose to brain targeting. Indian J. Pharm. Sci. 2009, 71, 707–709. [Google Scholar]
- Abdou, E.M.; Kandil, S.M.; Miniawy, H.M.F.E. Brain targeting efficiency of antimigraine drug loaded mucoadhesive intranasal nanoemulsion. Int. J. Pharm. 2017, 529, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, L.N.M.; Rodrigues da Silva, G.H.; Couto, V.M.; Castro, S.R.; Breitkreitz, M.C.; Martinez, C.S.; Igartúa, D.E.; Prieto, M.J.; de Paula, E. Functional hybrid nanoemulsions for sumatriptan intranasal delivery. Front. Chem. 2020, 8, 589503. [Google Scholar] [CrossRef]
- Chan, A.; Choi, E.; Yuki, I.; Suzuki, S.; Golshani, K.; Chen, J.; Hsu, F. Cerebral vasospasm after subarachnoid hemorrhage: Developing treatments. Brain Hemorrhages 2021, 2, 15–23. [Google Scholar] [CrossRef]
- Huang, S.; Huang, Z.; Fu, Z.; Shi, Y.; Dai, Q.; Tang, S.; Gu, Y.; Xu, Y.; Chen, J.; Wu, X.; et al. A novel drug delivery carrier comprised of nimodipine drug solution and a nanoemulsion: Preparation, characterization, invitro, and in vivo studies. Int. J. Nanomed. 2020, 15, 1161–1172. [Google Scholar] [CrossRef] [Green Version]
- Dhobale, A. Formulation and evaluation of carbamazepine nanoemulsion for brain targeted drug delivery via intranasal route. Indo Am. J. Pharm. Sci. 2018, 8, 1437–1452. [Google Scholar]
- Maruhashi, T.; Higashi, Y. An overview of pharmacotherapy for cerebral vasospasm and delayed cerebral ischemia after subarachnoid hemorrhage. Expert Opin. Pharmacother. 2021, 22, 1601–1614. [Google Scholar] [CrossRef]
- Ahmad, E.; Feng, Y.; Qi, J.; Fan, W.; Ma, Y.; He, H.; Xia, F.; Dong, X.; Zhao, W.; Lu, Y.; et al. Evidence of nose-to-brain delivery of nanoemulsions: Cargoes but not vehicles. Nanoscale 2017, 9, 1174–1183. [Google Scholar] [CrossRef]
- Varlamova, E.G.; Gudkov, S.V.; Plotnikov, E.Y.; Turovsky, E.A. Size-Dependent Cytoprotective Effects of Selenium Nanoparticles during Oxygen-Glucose Deprivation in Brain Cortical Cells. Int. J. Mol. Sci. 2022, 23, 7464. [Google Scholar] [CrossRef]
Figure 1.
Complex pathway involved in the transport of therapeutics through nose-to-brainroute.

Figure 2.
Intra nasal delivered nanoemulsion and management of brain disorders.

Figure 3.
Cerebral ischemia developed due to decreased oxygen concentration in carotid arteries.

Figure 4.
Various causes and symptoms of cerebral vasospasm.


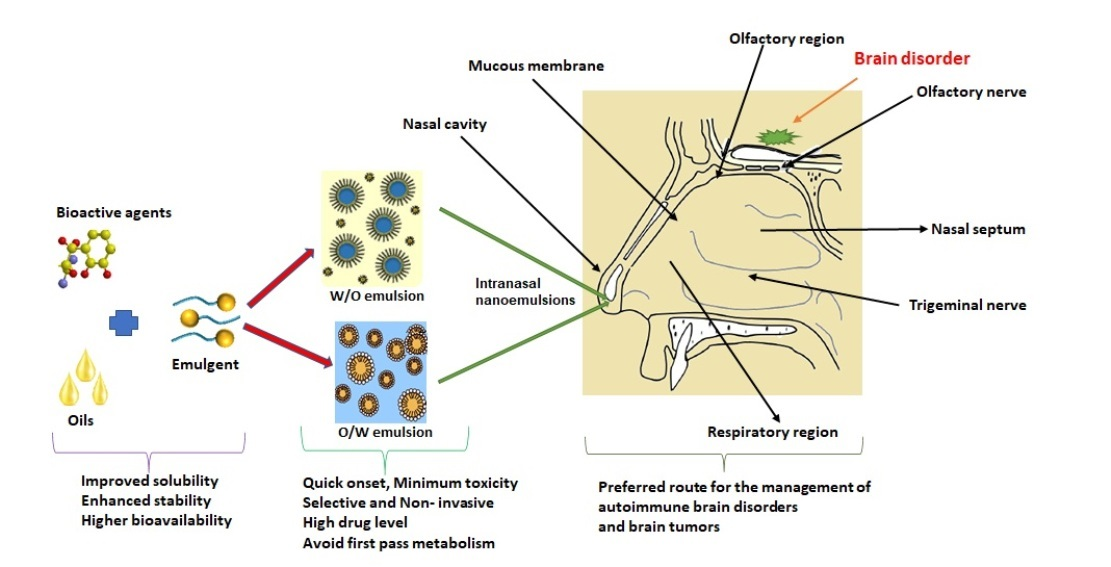{kind=link}
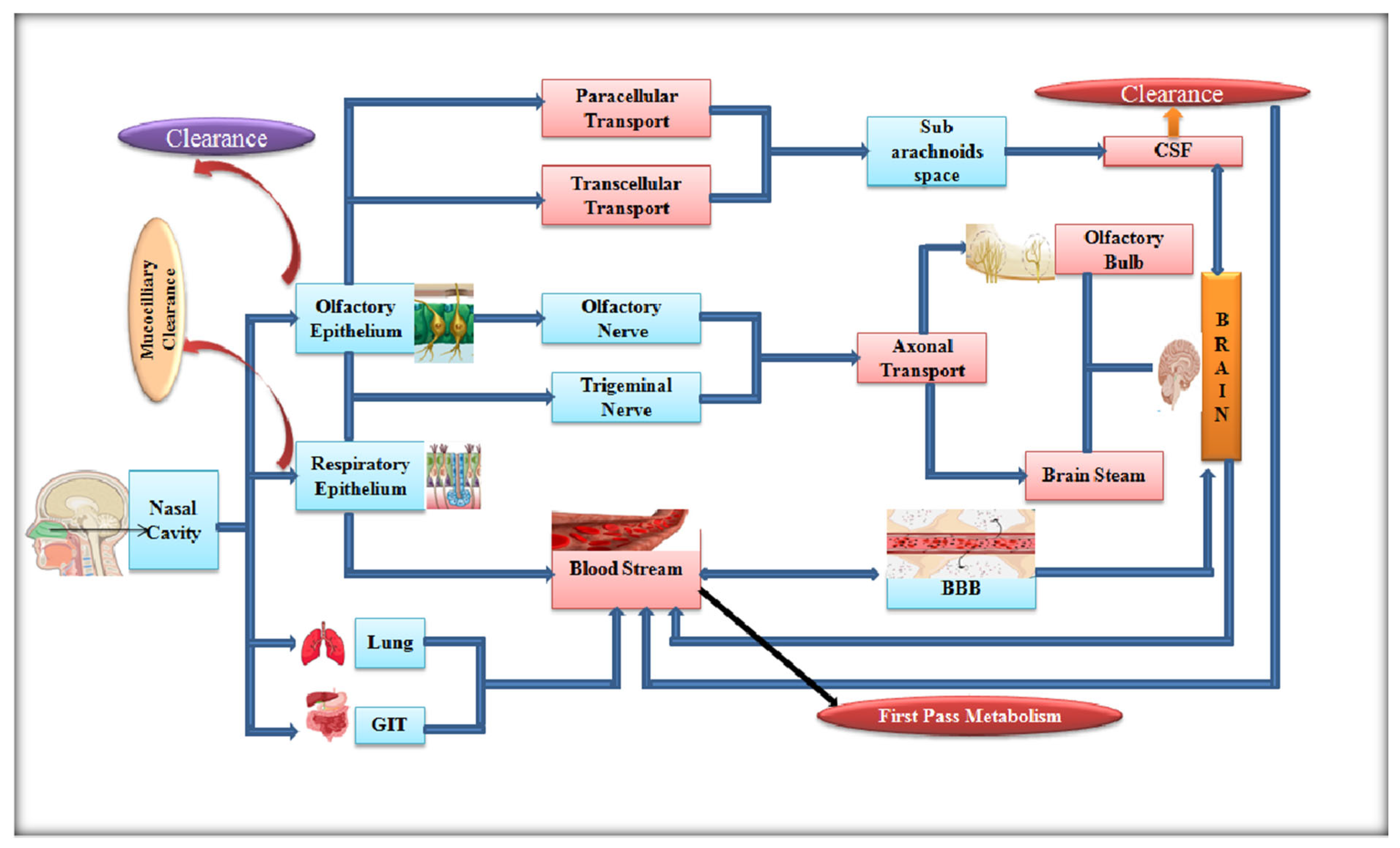{kind=link}
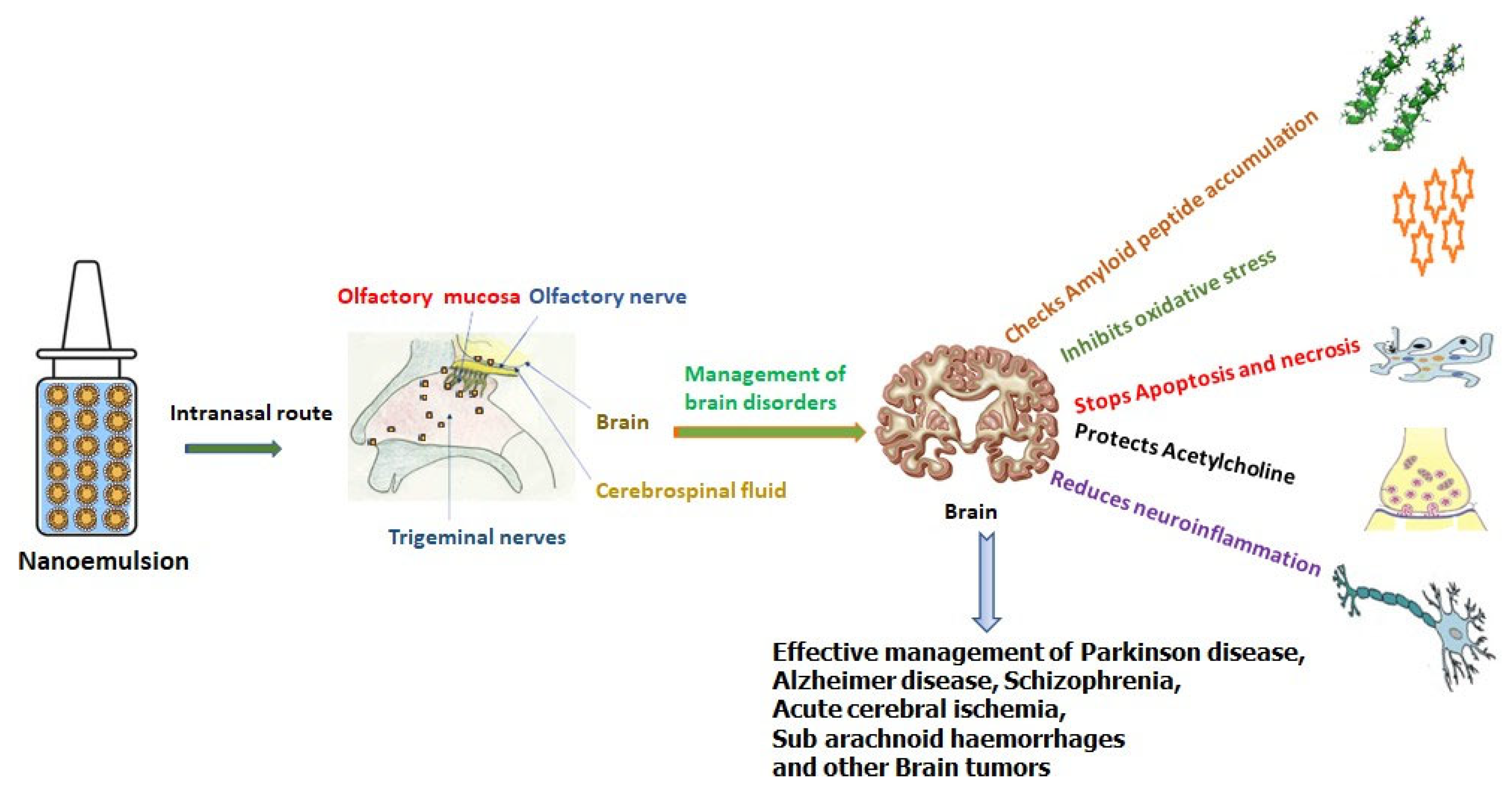{kind=link}
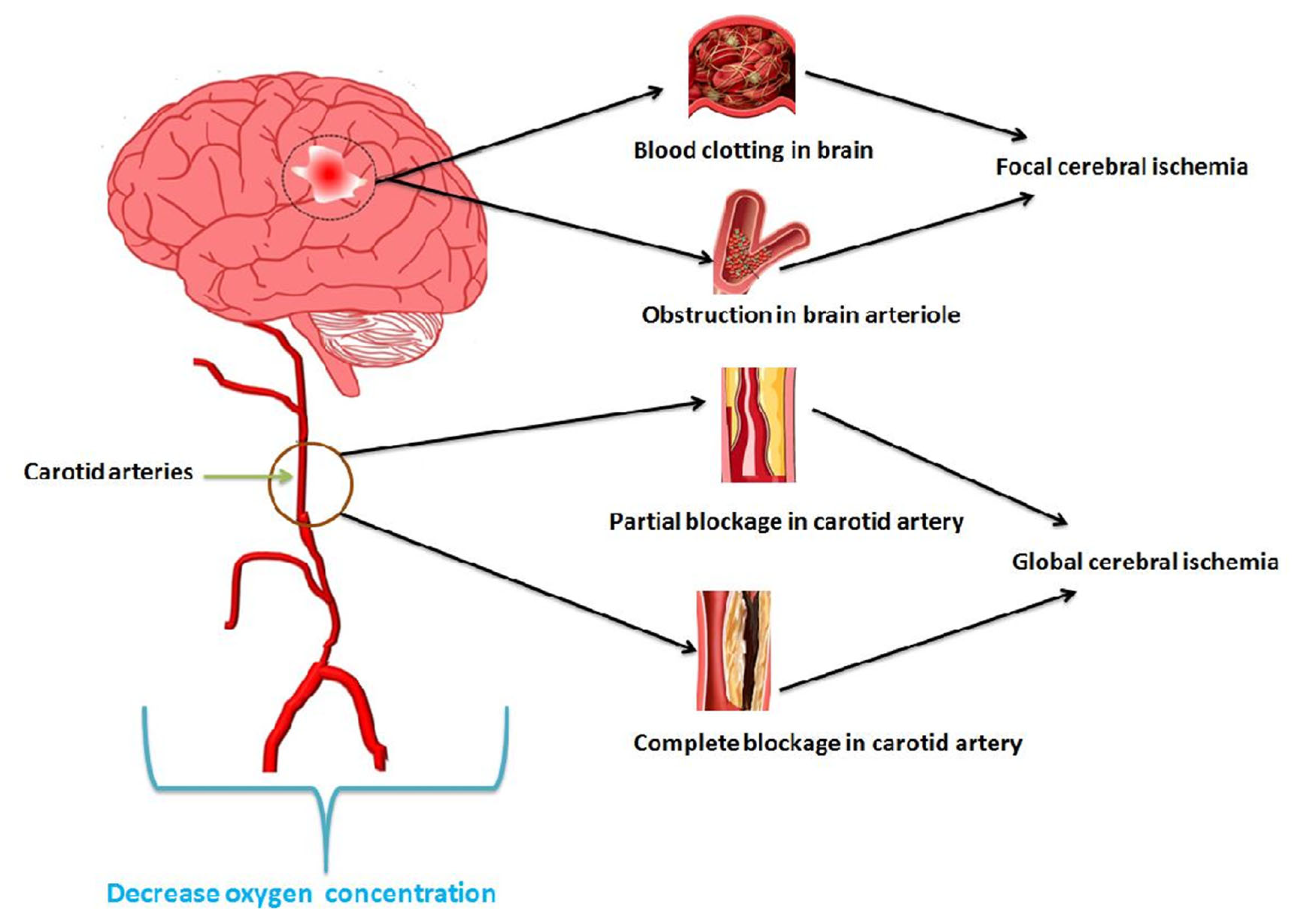{kind=link}
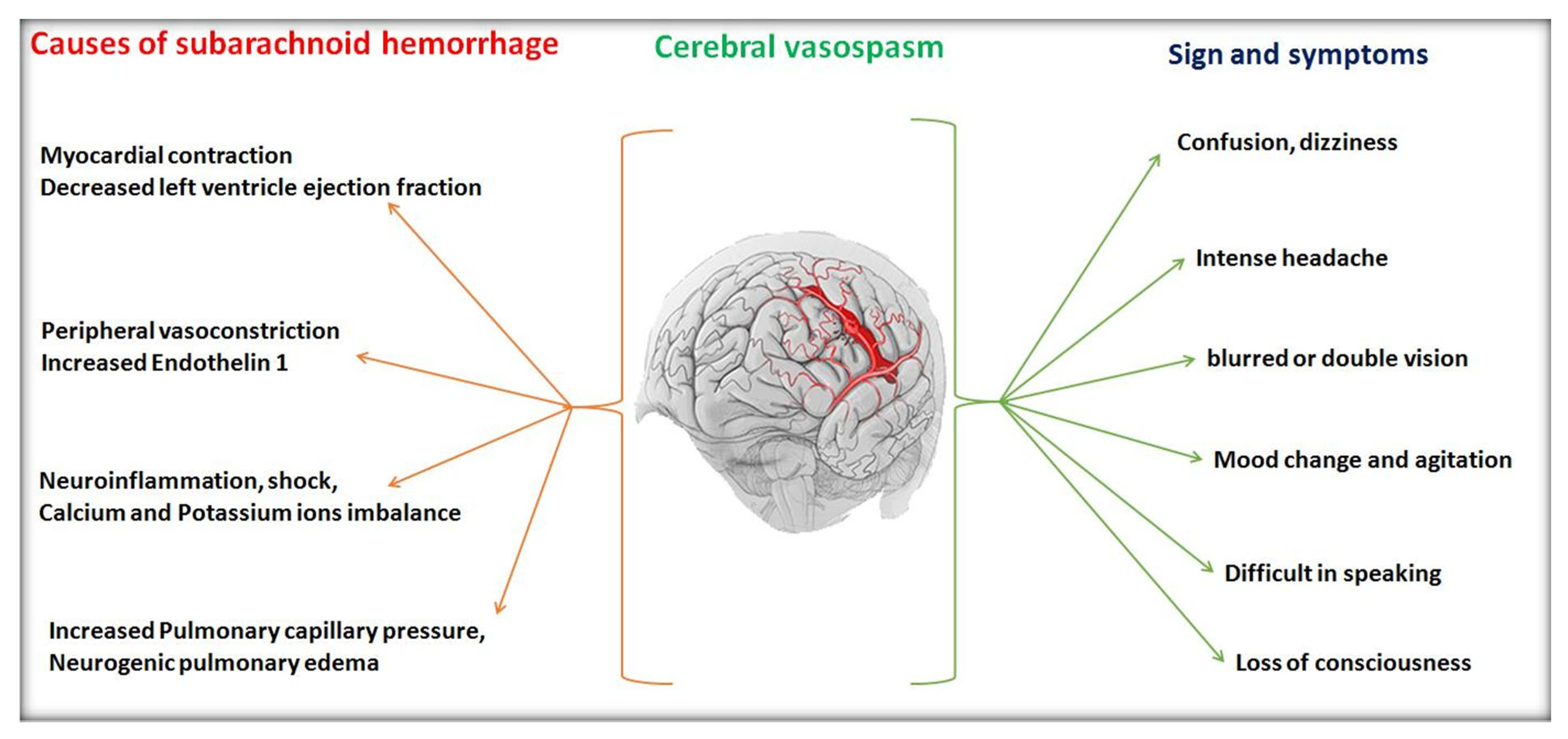{kind=link}
Table 1.
Salient features and drug delivery applications of advanced emulsions.
| Advanced Emulsion | Structure | Salient Features | Applications | Ref. |
|---|---|---|---|---|
| Nanoemulsion |  | Nanoscaled droplets provide thermodynamically (kinetically stable) colloidal dispersions. Controlled and effective lipophilic bioactive agents can be transported. | Widely explored in food industry for its superb stability and shelf life of encapsulated colouring/flavouring components/nutraceutical and bioactive agents | [16] |
| Multilayer emulsion |  | It contains hydrated lipophilic multi-molecular layers around oil (dispersed phase). Formed multilayer film provides adequate viscosity; hence, stable formulation is obtained. | Delivery and bio-accessibility of fat-soluble curcumin and other pH-sensitive bio-active agents | [17] |
| Multiple emulsion |  | These are emulsions within emulsion: i.e., o/w/o and w/o/w. Multiple emulsion limits bioactive degradation and is suitable for drug delivery via diverse routes such as ocular, oral, parenteral, nasal and pulmonary. | Delivery of low caloric food products, designing of easily spreadable creams, controlled and targeted dosages | [18] |
| Pickering emulsion |  | Instead of surface-active agents, solid particles confine at the interface of both phases and provide stability. These emulsions are more stable, tunable, feasible, stimuli-responsive and less toxic compared to the traditional ones. | Photocatalysis, protein recognition, purification of water, cosmeceutical products | [19] |
| High internal phase emulsion |  | HIPEs have high internal phase volume and are used to swap hydrogenated fats added in food stuffs. Hence, they improve stability and functionality and stabilize the system. The volume fraction is more than 0.74, ensuing formation of solid dispersed phase or polyhedral in the form of thin films. | Preparation of food stuffs, fuel and cosmetics | [20] |
Table 2.
Recently developed nanoemulsions for the management of diverse neurologicaldisorders.
| A. Alzheimer Disease | ||||
|---|---|---|---|---|
| Therapeutic Agent | Objective | Study Model | Outcome | Ref. |
| Memantine | To bypass BBB for effective management of Alzheimer’s disease | Particle size, in vitro release and radiolabelling with technetiumpertechnetate (99mTc). | Average globular size~11 nm. 80% drug release in nasal simulated fluid. ~98% cell viability. Higher uptake of drug (3.6% radioactivity) within 1.5 h in brain of rat. | [46] |
| Donepezil | To enhance drug delivery in brain | Particle size In vitro release radio labelling with Technetium pertechnetate | ~65 nm average globular size, 0.084 poly dispersity index (PDI) and −10.7 mV Zeta potential | [47] |
| 99% drug release in phosphatebuffer and 98% in simulated cerebrospinal mediawithin 4 h and 2 h, respectively. Dose-dependent radical scavenging and toxicity | ||||
| Huperzine A | Selectively Acetylcholinesterase inhibition via huperzine loaded nanoemulsion modified with lactoferrin | Particle size and zeta potential, in vitromodel (hCMEC/D3cells), drug-targeting index | 15.24 average particle size, 0.12 PDI and negative 4.48 mV zetapotential Drug-targetingindexwas 3.2 ± 0.75 Nanoemulsion was uptake by transcytosis and transported via specific multidrug resistance associated proteins transporters | [48] |
| Resveratrol | Coconut oil-based resveratrol nanoemulsion was targeted for the alleviation of Alzheimer’s disease | Effect of process variables, in vitro and in vivo permeation study in goat | Average particle size ~110 nm, −21.13 mV and 88.54% drug release in 8 h. Added coconut oil enhanced permeation efficiency. Optimum drugconcentrationwas 2.64 mg/mL. Higher resveratrol concentration in blood and brain (~1234.87 ng/mL and~5762.30 ng/mL in the brain, respectively, at 2 mg/kg dose. Superior permeation of prepared nanoemulsion compared to suspension in Goat nasal mucosa. | [49] |
| B. Parkinson disease | ||||
| Quercetin | Nanoemulsion comprising food-grade quercetin and oil (Capmul MCM NF) was aimed at neuroprotective action | HR-TEM, area electron diffraction studies and in vivo studies (cytotoxic study) and oxidative stress in wild-type Caenorhabditis elegans N2 strain | Spherical and ~50 nm particle size nanoemulsion potentially enhanced mitochondrial (3.080 ± 1.1) and fat content (2.64 ± 0.1) and reduced aggregation. Downregulated reactive Oxygen species content in | [50] |
| C elegans N2 strain. Dose and time-dependent toxicity. i.e., for A549 cells 300 µg/mL in 48 h. No toxicity against lymphocytes. | ||||
| Naringenin | Vitamin E adorned naringenin nanoemulsion was aimed at combating Parkinson’s disease | Structural property, refractive index and transmittance. Multiple behavioural analysis and oxidative study | Average smaller droplet size (~38.7 nm), 0.14 PDI with optimum zetapotential (−27.4 mV) and 19.6 Pas dynamic viscosity. 1.43 Refractive index and 98.1% transmittance indicated isotropic nature and stability of prepared nanoemulsion Three times high permeation coefficient and flux of nanoemulsion compared to suspension AUC0–48 hfor NE in brain 5345.1 and blood 3777.6 ng/mL X h Intranasally administered NE reversed Parkinson’s in 6-OHDA-persuaded rats while given with levodopa | [51] |
| Selegiline | Intranasal delivery monoamine oxidase B inhibitor (selegiline) nanoemulsion for better treatment of neuro degenerative disease | Quality by design approach for optimization of variables and behavioural study in rats | Optimized nanoemulsion (~61 nm) was quite stable (−34 mV). PDI (~0.203) Transmittance (~99.8%) and refractive index (1.30 ± 0.01) Almost 3.7-fold selegiline drug permeation observed compared to its oral suspension. Significantly improved locomotor activity and muscle coordination in experimental rat model on comparing with oral route. | [52] |
| Hyaluronic acid coloaded with resveratrol and curcumin) | Mucoadhesive polyphenols containing nanoemulsion were targeted for brain delivery | Antioxidant potential, in vitro and ex vivo and in vivo assessment of polyphenols in rat brain | Average particle size ~115 nm with negative zeta potential (23.9 mV). Higher nasal mucosa adhesive potential of the developed nanoemulsion Preserved polyphenolic antioxidant efficacy and protected from their degradation. Controlled diffusion was achieved for 6 h and showed ex vivo permeation efflux for resveratrol (2.86 µg/cm2) and curcumin (2.09 µg/cm2) across sheep nasal mucosa. Increased amount of two polyphenols in brain | [53] |
| C. Epilepsy | ||||
| Amiloride | To enhance brain bioavailability of nanoemulsion containing diuretic amiloride | 33 factorial central composite design, Physicochemical parameters, in vitro drug release and antiepileptic effect in mice | Concentration of olei cacid (2.5%), Tween 20 and Carbitol (10%) and sonication time (45 s) were optimised, which resulted in ~89 nm hydrodynamic diameter. ~1.38 refractive index, 6.4 ± 0.2 pH and ~41 cp viscosity of nanoemulsion ~99% percentage transmittance and ~80% cumulative drug release. Drastically increased nose-to-brain transport (~586%) and efficiency (~1992%) in mice model Improved seizure threshold in epileptic rodent model and induced seizure in mice. | [54] |
| Letrozole | Nanoemulsion contained aromatase inhibitor letrozole designed for brain delivery while avoiding peripheral responses | Structural analysis, in vitro and ex vivo drug diffusion study and behavioural study | Spherical and smaller particles of mean diameter. i.e., 96 nm and 0.162 PDI. Negative −7.12 zetapotential Prolonged drug release during intranasal administration that results in high concentration letrozole in brain region. Enhanced neuroprotective and antiepileptic effects. Inhibition and diversion of aromatomization and metabolic pathways of testosterone into 17-beta estradiol observed. | [55] |
| Oxcarbazepine | PLGA tri-block polymer admixed oxcarbazepine emulsome (emulsion +liposome) and its thermogel were developed to amplify drug concentration in brain | In vitro study, histopathological analysis, and pharmacokinetic parameters | Concentration dependent rheological behaviour. The emulsome exhibited sustained effect of 81.1% for 24 h. Higher drug transport in brain tissue uptake in rat model compared to drug solution and suspension (Trileptal®). 3818.8 ng/mL and 5699.9 ng/mL Cmax of nanoemul gels in plasma and brain, respectively. Histopathology study of nasal tissues revealed mild anti-inflammatory response and vascular congestion without toxicity. | [56] |
| D. Neuroprotection | ||||
| Naringenin | To explore bioflavonoid naringenin for its neuroprotective effect owing to its antioxidant and anti-inflammatory virtues | Particle size and zeta potential, neuroprotective assay (Aβ triggered ROS, total tau, amyloid precursor protein) against neuroblastoma cells, i.e., SH-SY5Y | Average droplet size 113.8 nm with narrow PDI~0.312. Percentage transmittance ~97.01% and +12.4 mV zeta potential. Enhanced neurotoxic effects SH-SY5Y cells due to down-regulation of amyloid precursor protein. Nanoemulsion checked | [57] |
| amyloid-genesis and reduced level of phosphorylated tau at low concentration of 0.125 µM in comparison with bare drug 25 µM. | ||||
| Curcumin | Improvement of solubility and bioavailability issues of curcumin added in nanoemulsion for the novel neuroprotective action | Oxidative stress and mitochondrial complex I activity | Curcumin-loaded nanoemulsion significantly enhanced motor activity at 25 mg/kg dose Lessened lipoperoxidation and improved antioxidant activity in mitochondria while compared to free curcumin. Curcumin-loaded nanoemulsion inhibited Mitochondrial complex 1 activity | [58] |
| Chia seed oil | Developed nanoemulsion containing Chia seed oil had potential to overcome issues of Parkinson’s disease and neuroprotective actions | Motor and behavioural evaluation. i.e., rotarod and locomotor tests and biochemical evaluation | Solubility, bioavailability, and stability of Chia seed oil contained nanoemulsion was escalated Potential application of developed nanoemulsion is suggested for neuroprotective effect in neurodegenerative disorders | [59] |
| E. Depression and Schizophrenia | ||||
| Paroxetine | Selective serotonin reuptake inhibitor ‘paroxetine ‘embedded intranasal nanoemulsion was explored for treatment of depression that also avoided first-pass metabolism | Average particle size, PDI, zetapotential, permeation, behavioural studies, Forced swimming test in Wistar rat and antidepressant studies | Spherical droplets of size ~58 nm with 0.339 PDI and −33 mV zeta potential. Good% transmittance and refractive index. i.e., 100.6% and 1.41, respectively 2.57 times higher permeation of nanoemulsion compared to paroxetine suspension. Improved anti-depression action due to enhancement of reduced level of glutathione on intranasal delivery. Decreased level of | [60] |
| Thiobarbituric acid reactive Substance (TBARS). | ||||
| Aripiprazole | Quinolinone derivative antidepressant aripiprazole nanoemulsion was designed for treatment of schizophrenia and bipolar disorder | Response surface method and central composite rotatable design for optimization | Optimized overhead stirring time (120 min), high shear homogenization (15 min) and rpm (4400) resulted in nanosized (~62 nm) droplets and 3.72 mPa viscosity. At pH 7.4, osmolality of nanoemulsion was ~297 mOsm/kg Stable for three months at variable temperatures. i.e., 4 °C, 25 °C and 45 °C. | [61] |
| Asenapine maleate | Mucoadhesive nanoemulsion of antipsychotic asenapine maleate prepared for improved nasomucosal adhesion, efficient brain-targeting and safety | Sigle-dose pharmacokinetic study, animal behaviour study, ex vivo ciliotoxicity in sheep nasal mucosa | Spherical particles with average diameter of 21.2 nm with narrow PDI (0.355). Increased drug concentration in Wistar rat brain (within 1 h) after intranasal delivery compared to intravenous route (3 h). Enhanced brain targeting capacity (284.33 ng/mL). Improved locomotor activity with no extrapyramidal symptoms in sheep nasal mucosa. | [62] |
Table 3.
Recently developed nanoemulsion for the treatment of brain glioblastoma (data collected for last 5 years).
Table 3.
Recently developed nanoemulsion for the treatment of brain glioblastoma (data collected for last 5 years).
| Therapeutic Agent | Objective | Evaluated Parameters | Result | Application | Ref. |
|---|---|---|---|---|---|
| Kaempferol | Investigation of glioma cells inhibition efficacy with and without chitosan-loaded kaempferol nanoemulsion and compared mucoadhesive properties after intranasal delivery | Average droplet size (180 nm) pH (5.56 ± 0.02) Viscosity (11.48 ± 0.13 cp25 °C) Drug content (96.37 ± 2.67%) Association efficiency (99.35 ± 0.10%) Permeation Efficiency across nasal mucosa (13.04 µg/cm2) | Chitosan improved residing properties in the nasal mucosa owing to its mucoadhesive property, hence enhancing permeation and reducing nasal clearance of drug. Further, chitosan-KPF nanoemulsion inhibited C6 glioma cells viability via rapidly triggering apoptosis compared to without chitosan-loaded kaempferol nanoemulsion. | Treatment of glioma | [71] |
| Curcumin(CUR) and quercetin(QUE) | Two phytoconstituents containing nanoemulsions were designed for synergistically inhibiting growth of glioblastoma U373MG cells | Average droplet size 93 nm PDI 0.149 Drug content 42.4% for CUR and 55.1% for QUE Zetapotential –14.8 mV Drug release in pH6.4 For CUR, 95.84% For QUE, 94.0% | Optimized nanoemulsion displayed significantly high percentage of brain targeting efficiency, i.e., ~178% for curcumin and ~170% for quercetin. Successful nose-to-brain delivery of both curcumin and quercetin (~44% and ~38%, respectively) indicated potential CNS targeting through intranasal pathway. Further, the nanoemulsion exhibited synergistically site-specific targeting of human glioblastoma cells compared to doxorubicin drug. | Treatment of human glioblastoma | [72] |
| CD73SiRNA | Cationic nanoemulsion composed of si-RNACD73R was successfully developed and targeted to inhibit brain tumour growth | Cell viability 30–50% Glioma cells inhibition 60–80% Tumour growth reduction 60% decreased adenosine level 95% | Developed si-RNA-CD73R Nanoemulsion enabled silencing of surface enzyme CD73 and overexpression of adenosine in the brain of rats after nasal delivery. Administered nanoemulsion reduced growth of glioblastoma cells and adenosine level in cancerous cells. | Treatment of brain tumour | [73] |
| Disulfiram inclusion complex with copper ion | Ion-sensitive disulfiram nanoemulsion was explored for the management of glioblastoma | Average particlesize ~63.4 nm. Zeta potential (−23.5 mV) Prolonged drug release 50% at 4 h and and 75% at 12 h | Performed in vitro studies indicated effective inhibition of proliferation of glioblastoma cells. i.e., C6 andU87. Further, formulated in situ gel nanoemulsion showed excellent uptake and brain target capability by producing highest signal fluorescence in the brain of rats. | Glioblastoma targeting therapy | [74] |
| Polyphenolic flavonoid quercetin | Enhancement of bioavailability and permeability of quercetin-loaded nanoemulsion across blood–brain barrier | Mean droplet size 125.5 nm PDI 0.251 Entrapment efficiency ~87.0%. Cmax 5962.7 ng/mL after 4 h Mean resident time 46.13 h. AUC is 5.32 times higher than pure drug | Intranasal-administered quercetin nanoemulsion improved solubility, therapeutic index and permeability in the brain region. | Brain cancer | [75] |
Table 4.
Recently reported nanoemulsions for the management of cerebral ischemia.
| Therapeutic Agent | Purpose | Evaluated Parameters | Outcomes | Application | Ref. |
|---|---|---|---|---|---|
| Safranal | Nanoemulsion containing antioxidant safranal was prepared to reduce oxidative stress in brain injury | Optimized mean size 89.64 nm Zetapotential −11.39 mV Drug content 98.47% Viscosity 124 cp | Improved locomotor activity, grip strength and antioxidant activity observed. Significantly decrease in glutathione reductase, superoxide dismutase and lipid peroxidation in model rat brain. | Treatment for cerebral ischemia-reperfusion injury | [82] |
| Chaxiong volatile oil | Thermosensitive intranasal in situ nanoemulsion gel was developed for brain targeting | Mean particle size ~21.02 nm, PDI 0.14 Negative zeta potential −20.4 mV pH 4.52 Viscosity 32.5 mV, gelling strength 42–47 s Mucoadhesive strength 5.2 × 102 dy/cm2 Release kinetics Ritger–Peppas model. | Both nanoemulsion and in situ gel had potential to lessen neurological deficit score in ischemic rat model. Cerebral infarction size was reduced, which improved ischemic stroke. | Cerebral ischemic stroke | [83] |
| 6-Gingerol | Mucoadhesive intranasal nanoemulsion was designed to improve brain bioavailability and Neuro-protectiveness effect of 6-gingerol | Average particle size ~94.89 nm, Narrow PDI 0.129 Zetapotential +1.892 mV Retention time 1.27 min | Nanoemulsion preparedwith antioxidant 6-gingerol and lauroglycol 90 was then converted in to mucoadhesive with chitosan. Improved Cmax and AUC after intranasal administration exhibited and histopathological assay displayed reduction in infarction volume in induced Ischemic model. | Treatment of cerebral ischemia | [84] |
| Tenofovir disoproxil fumarate | Stable nucleotide reductase inhibitor tenofovir disproxil fumerate-loaded nanoemulsion was developed and optimized by phase diagram to target neuro-AIDS in brain. | Phase diagram for optimization of surfactant and co-surfactant (45%). Zeta potential (−18.7 mV) Average globular size (156.2 nm) PDI (0.463) Drug diffusion (egg membrane) 74.98% and sheep nasal mucosa (75.98%) after 3 h. | Developed nanoemulsion increased surface area and provided lipophilicity to the formulation. This alternate strategy provided quick onset of action against viral infection for all age groups sufferers. | Neuro-AIDS treatment | [85] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Misra, S.K.; Pathak, K. Nose-to-Brain Targeting via Nanoemulsion: Significance and Evidence. Colloids Interfaces 2023, 7, 23. https://doi.org/10.3390/colloids7010023
AMA Style
Misra SK, Pathak K. Nose-to-Brain Targeting via Nanoemulsion: Significance and Evidence. Colloids and Interfaces. 2023; 7(1):23. https://doi.org/10.3390/colloids7010023
Chicago/Turabian StyleMisra, Shashi Kiran, and Kamla Pathak. 2023. "Nose-to-Brain Targeting via Nanoemulsion: Significance and Evidence" Colloids and Interfaces 7, no. 1: 23. https://doi.org/10.3390/colloids7010023