
Biomarkers in Patients with Hand-Arm Vibration Injury Entailing Raynaud’s Phenomenon and Cold Sensitivity, Compared to Referents †

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Questionnaires
2.3. Perception of Touch
2.4. Biomarkers
2.5. Statistics
3. Results
3.1. Biomarkers in Patients with and without RP and Referents
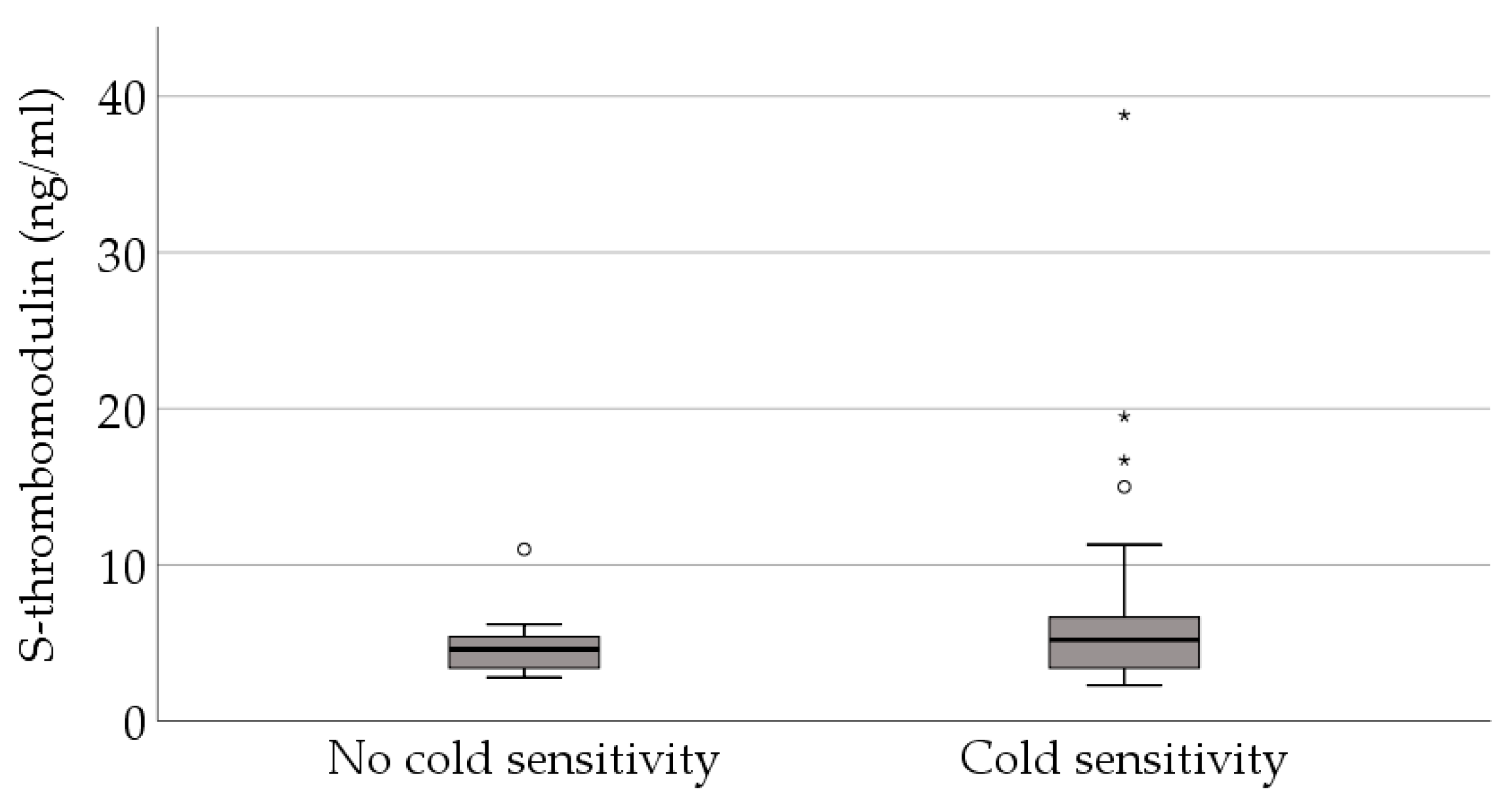
3.2. Biomarkers in Patients without RP and with and without Increased Cold Sensitivity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nilsson, T.; Wahlstrom, J.; Burstrom, L. Hand-arm vibration and the risk of vascular and neurological diseases-A systematic review and meta-analysis. PLoS ONE 2017, 12, e0180795. [Google Scholar] [CrossRef] [PubMed]
- Dahlin, L.B.; Sanden, H.; Dahlin, E.; Zimmerman, M.; Thomsen, N.; Bjorkman, A. Low myelinated nerve-fiber density may lead to symptoms associated with nerve entrapment in vibration-induced neuropathy. J. Occup. Med. Toxicol. 2014, 9, 7. [Google Scholar] [CrossRef] [PubMed]
- Stoyneva, Z.; Lyapina, M.; Tzvetkov, D.; Vodenicharov, E. Current pathophysiological views on vibration-induced Raynaud’s phenomenon. Cardiovasc. Res. 2003, 57, 615. [Google Scholar] [CrossRef] [PubMed]
- Kiedrowski, M.; Waugh, S.; Miller, R.; Johnson, C.; Krajnak, K. The effects of repetitive vibration on sensorineural function: Biomarkers of sensorineural injury in an animal model of metabolic syndrome. Brain Res. 2015, 1627, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Krajnak, K.; Waugh, S. Systemic Effects of Segmental Vibration in an Animal Model of Hand-Arm Vibration Syndrome. J. Occup. Environ. Med. 2018, 60, 886–895. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, T.; Futatsuka, M.; Imanishi, H.; Yamada, S. Pathological changes observed in the finger biopsy of patients with vibration-induced white finger. Scand. J. Work Environ. Health 1986, 12, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Govindaraju, S.R.; Curry, B.D.; Bain, J.L.; Riley, D.A. Comparison of continuous and intermittent vibration effects on rat-tail artery and nerve. Muscle Nerve 2006, 34, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Kao, D.S.; Yan, J.G.; Zhang, L.L.; Kaplan, R.E.; Riley, D.A.; Matloub, H.S. Serological tests for diagnosis and staging of hand-arm vibration syndrome (HAVS). Hand 2008, 3, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Kanazuka, M.; Shigekiyo, T.; Toibana, N.; Saito, S. Increase in plasma thrombomodulin level in patients with vibration syndrome. Thromb. Res. 1996, 82, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Rossor, A.M.; Reilly, M.M. Blood biomarkers of peripheral neuropathy. Acta Neurol. Scand. 2022, 146, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Ising, E.; Åhrman, E.; Thomsen, N.O.B.; Eriksson, K.F.; Malmström, J.; Dahlin, L.B. Quantitative proteomic analysis of human peripheral nerves from subjects with type 2 diabetes. Diabet. Med. J. Br. Diabet. Assoc. 2021, 38, e14658. [Google Scholar] [CrossRef] [PubMed]
- Notturno, F.; Capasso, M.; DeLauretis, A.; Carpo, M.; Uncini, A. Glial fibrillary acidic protein as a marker of axonal damage in chronic neuropathies. Muscle Nerve 2009, 40, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Tekavec, E.; Löfqvist, L.; Larsson, A.; Fisk, K.; Riddar, J.; Nilsson, T.; Nordander, C. Adverse health manifestations in the hands of vibration exposed carpenters—A cross sectional study. J. Occup. Med. Toxicol. 2021, 16, 16. [Google Scholar] [CrossRef] [PubMed]
- Cooke, R.A.; Lawson, I.J. Cold intolerance and hand-arm vibration syndrome. Occup. Med. 2022, 72, 152–153. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, I.K.; Dahlin, L.B. Self-reported cold sensitivity in patients with traumatic hand injuries or hand-arm vibration syndrome an eight year follow up. BMC Musculoskelet. Disord. 2014, 15, 83. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patients with Raynaud’s Phenomenon (n = 45) | Patients without Raynaud’s Phenomenon (n = 47) | Referents (n = 64) | |
|---|---|---|---|
| Age [years; median (range)] | 45 (24–64) | 45 (21–64) | 43 (26–62) |
| Females [n (%)] | 1 (2) | 5 (11) | 9 (14) |
| Ongoing nicotine use [n (%)] | 23 (51) | 17 (36) | 25 (40) |
| Previous frost bites in hands [n (%)] | 6 (15) a | 4 (9) b | 3 (5) c |
| Raynaud’s phenomenon [n (%)] | 45 (100) | 0 (0) | 6 (10) |
| Cold sensitivity [n (%)] | 44 (98) | 36 (77) | 10 (16) |
| Impaired perception of touch [n (%)] | 29 (64) | 16 (34) | 10 (16) |
| Patients with Raynaud’s Phenomenon (n = 45) Median (Range) | Patients without Raynaud’s Phenomenon (n = 47) Median (Range) | Referents (n = 64) Median (Range) | p-Value | |
|---|---|---|---|---|
| S-TM (ng/mL) | 6.1 (2.7–30) a, b | 5.2 (2.3–39) a | 4.3 (<LOD–40) b | 0.003 |
| S-GFAP (pg/mL) | LOD c (LOD–3070) | LOD (LOD–2528) | LOD (LOD–3376) | 0.28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tekavec, E.; Nilsson, T.; Dahlin, L.B.; Axmon, A.; Nordander, C.; Riddar, J.; Kåredal, M. Biomarkers in Patients with Hand-Arm Vibration Injury Entailing Raynaud’s Phenomenon and Cold Sensitivity, Compared to Referents. Proceedings 2023, 86, 27. https://doi.org/10.3390/proceedings2023086027
Tekavec E, Nilsson T, Dahlin LB, Axmon A, Nordander C, Riddar J, Kåredal M. Biomarkers in Patients with Hand-Arm Vibration Injury Entailing Raynaud’s Phenomenon and Cold Sensitivity, Compared to Referents. Proceedings. 2023; 86(1):27. https://doi.org/10.3390/proceedings2023086027
Chicago/Turabian StyleTekavec, Eva, Tohr Nilsson, Lars B. Dahlin, Anna Axmon, Catarina Nordander, Jakob Riddar, and Monica Kåredal. 2023. "Biomarkers in Patients with Hand-Arm Vibration Injury Entailing Raynaud’s Phenomenon and Cold Sensitivity, Compared to Referents" Proceedings 86, no. 1: 27. https://doi.org/10.3390/proceedings2023086027