
Impact of COVID-19 Vaccination Rates and Public Measures on Case Rates at the Provincial Level, Thailand, 2021: Spatial Panel Model Analyses

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Analysis
2.3. Ethical Considerations
3. Results
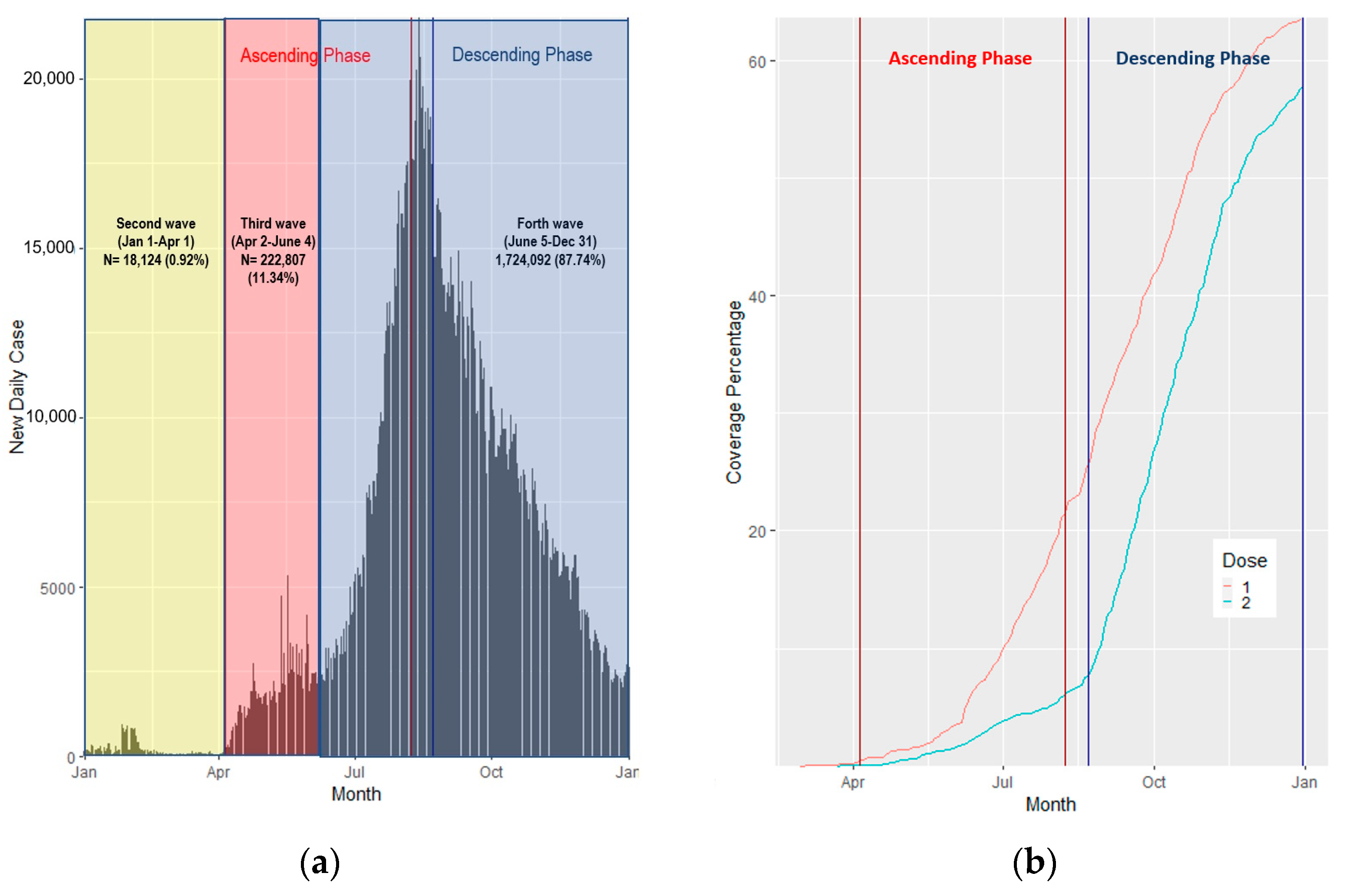
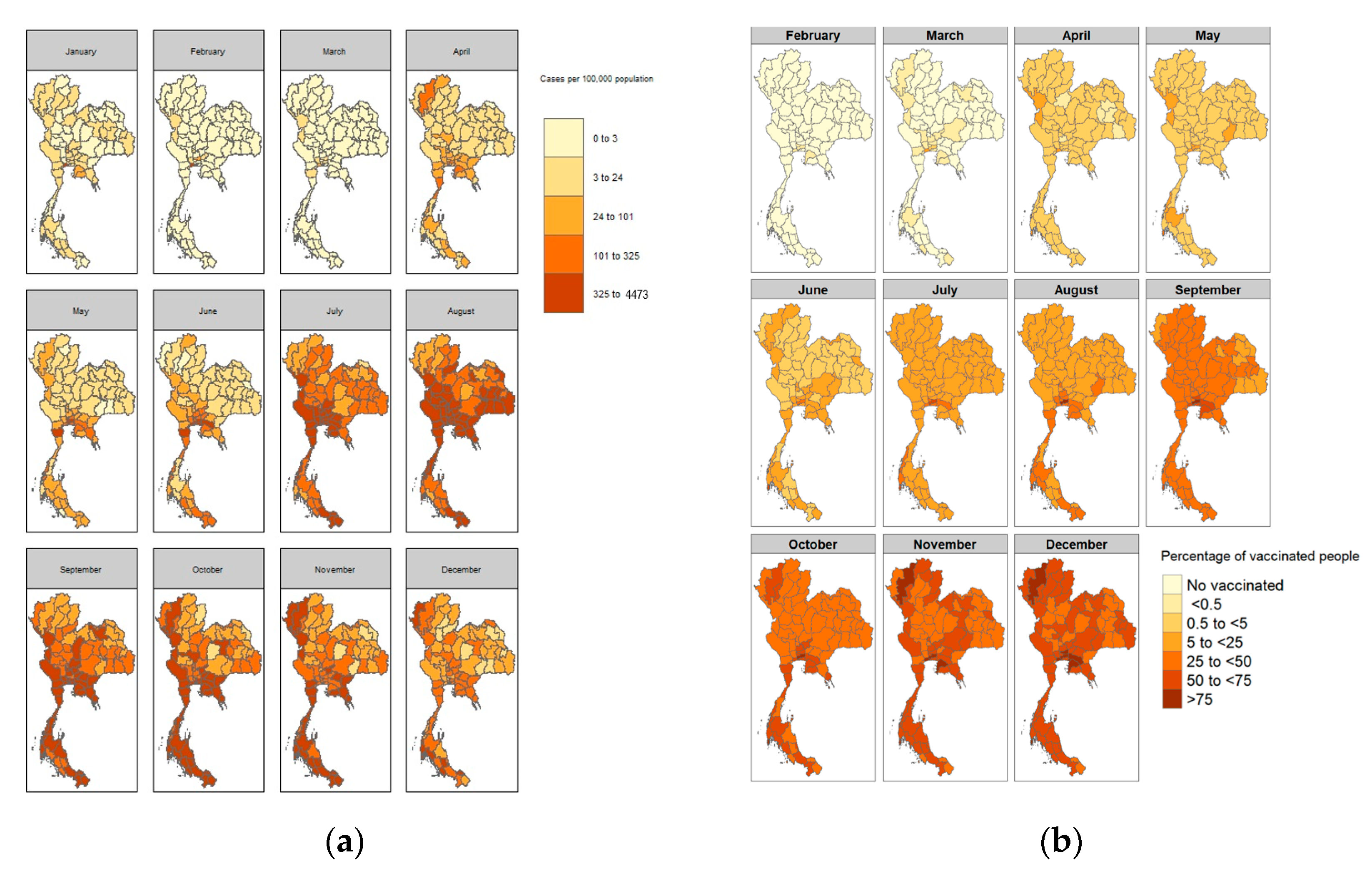
3.1. COVID-19 Cases and Case Rates, Per 100,000 People
3.2. COVID-19 Vaccination Counts and Rates
3.3. COVID-19 Case Rates and Vaccination Rates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. COVID-19 Public Health Emergency of International Concern (PHEIC) Global Research and Innovation Forum. Available online: https://www.who.int/publications/m/item/covid-19-public-health-emergency-of-international-concern-(pheic)-global-research-and-innovation-forum (accessed on 25 April 2022).
- Albano, P.M.; Notarte, K.I.; Macaranas, I.; Maralit, B. Cross-contamination in Molecular Diagnostic Laboratories in Low- and Middle-income Countries: A Challenge to COVID-19 Testing. Philipp. J. Pathol. 2020, 5, 7–11. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 25 April 2022).
- U.S. Food and Drug Administration. Emergency Use Authorization for Vaccines Explained. Available online: https://www.fda.gov/vaccines-blood-biologics/vaccines/emergency-use-authorization-vaccines-explained (accessed on 25 April 2022).
- World Health Organization. Novel Coronavirus—Thailand (Ex-China). Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON234 (accessed on 25 April 2022).
- Jindahra, P.; Wongboonsin, K.; Wongboonsin, P. Demographic and initial outbreak patterns of COVID-19 in Thailand. J. Popul. Res. 2022, 39, 567–588. [Google Scholar] [CrossRef] [PubMed]
- Center for COVID-19 Situation Administration. The Coronavirus Disease 2019 Situation: Thailand Situation Update on 1 January 2022 (press release). Available online: https://media.thaigov.go.th/uploads/public_img/source/010464.pdf (accessed on 1 January 2022).
- National Vaccine Institute. Situation of COVID-19 Vaccination Use in Thailand. Available online: http://www.nvi.go.th/index.php/blog/2021/04/news2_2564_04_covid-19_vaccineuse_and_report (accessed on 25 April 2022).
- BBC. Covid Vaccine: Thailand Decides to Mix Jabs as Cases Spike. 2021. Available online: https://www.bbc.com/news/world-asia-57801251 (accessed on 25 April 2022).
- Otto, S.P.; Day, T.; Arino, J.; Colijn, C.; Dushoff, J.; Li, M.; Mechai, S.; Van Domselaar, G.; Wu, J.; Earn, D.J.; et al. The origins and potential future of SARS-CoV-2 variants of concern in the evolving COVID-19 pandemic. Curr. Biol. 2021, 31, R918–R929. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tracking SARS-CoV-2 Variants: World Health Organization. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 25 April 2022).
- Scientific Advisory Group for Emergencies. SPI-M-O: Consensus Statement on COVID-19, 3 June 2021. Available online: https://www.gov.uk/government/publications/spi-m-o-consensus-statement-on-covid-19-3-june-2021 (accessed on 25 April 2022).
- World Health Organization Thailand. Coronavirus Disease 2019 (COVID-19): WHO Thailand Situation Report on 02 January 2021 (press release). Available online: https://cdn.who.int/media/docs/default-source/searo/thailand/2021_01_02_tha-sitrep-112-covid19.pdf?sfvrsn=6bce63a3_3 (accessed on 25 April 2022).
- Pan American Health Organization. Virus Variants Are Expected, but Surveillance Should Continue to Monitor Possible Changes in Clinical Patterns, Experts Say. Available online: https://www.paho.org/en/news/14-5-2021-virus-variants-are-expected-surveillance-should-continue-monitor-possible-changes (accessed on 25 April 2022).
- World Health Organization. Guidance for Surveillance of SARS-CoV-2 Variants: Interim Guidance; World Health Organization: Geneva, Switzerland, 9 August 2021. [Google Scholar]
- Department of Medical Sciences MOPH Thailand. SAR-CoV-2 Variants in Thailand; Department of Medical Sciences MOPH: Nonthaburi, Thailand, 2022.
- World Health Organization. The Global COVID-19 Vaccination Strategy. Available online: https://www.who.int/publications/m/item/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022 (accessed on 25 April 2022).
- Department of Disease Control. COVID-19 Vaccines in Thailand (in Thai). Available online: https://ddc.moph.go.th/vaccine-covid19/ (accessed on 25 April 2022).
- Notarte, K.I.; Catahay, J.A.; Peligro, P.J.; Velasco, J.V.; Ver, A.T.; Guerrero, J.J.; Liu, J.; Lippi, G.; Benoit, S.W.; Henry, B.M.; et al. Humoral Response in Hemodialysis Patients Post-SARS-CoV-2 mRNA Vaccination: A Systematic Review of Literature. Vaccines 2023, 11, 724. [Google Scholar] [CrossRef] [PubMed]
- Fine, P.; Eames, K.; Heymann, D.L. “Herd Immunity”: A Rough Guide. Clin. Infect. Dis. 2011, 52, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Wellenius, G.A.; Vispute, S.; Espinosa, V.; Fabrikant, A.; Tsai, T.C.; Hennessy, J.; Dai, A.; Williams, B.; Gadepalli, K.; Boulanger, A.; et al. Impacts of social distancing policies on mobility and COVID-19 case growth in the US. Nature Communications. Nat. Commun. 2021, 12, 3118. [Google Scholar] [CrossRef] [PubMed]
- Center for COVID-19 Situation Administration. The Coronavirus Disease 2019 Situation: Thailand Situation Update on 23 December 2020 (in Thai) (Press Release). Available online: https://media.thaigov.go.th/uploads/public_img/source/231263.pdf (accessed on 1 January 2022).
- Rarueysong, S. Thai Cabinet Approves Immediate Registration of Undocumented Migrant Workers. Available online: https://thainews.prd.go.th/en/news/detail/TCATG210929115601501 (accessed on 25 April 2022).
- Center for COVID-19 Situation Administration. The Coronavirus Disease 2019 Situation: Thailand Situation Update on 30 May 2021 (Press Release). Available online: https://media.thaigov.go.th/uploads/public_img/source/300564.pdf (accessed on 1 January 2022).
- Center for COVID-19 Situation Administration. The Coronavirus Disease 2019 Situation: Thailand Situation Update on 29 September 2021 (Press Release). Available online: https://media.thaigov.go.th/uploads/public_img/source/290964.pdf (accessed on 1 January 2022).
- Suphanchaimat, R.; Tuangratananon, T.; Rajatanavin, N.; Phaiyarom, M.; Jaruwanno, W.; Uansri, S. Prioritization of the Target Population for Coronavirus Disease 2019 (COVID-19) Vaccination Program in Thailand. Int. J. Environ. Res. Public Health 2021, 18, 10803. [Google Scholar] [CrossRef] [PubMed]
- Suphanchaimat, R.; Nittayasoot, N.; Thammawijaya, P.; Teekasap, P.; Ungchusak, K. Predicted Impact of Vaccination and Active Case Finding Measures to Control Epidemic of Coronavirus Disease 2019 in a Migrant-Populated Area in Thailand. Risk Manag. Healthc Policy 2021, 14, 3197–3207. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.K.; Gazi, M.A.I.; Bhuiyan, M.A.; Rahaman, M.A. Effect of Covid-19 pandemic on tourist travel risk and management perceptions. PLoS ONE 2021, 16, e0256486. [Google Scholar] [CrossRef] [PubMed]
- Lagos, D.G.; Poulaki, P.; Lambrou, P. COVID-19 and Its Impact on Tourism Industry. Adv. Exp. Med. Biol. 2021, 1318, 815–824. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Cases (%) | Vaccinated (%) |
|---|---|---|
| Age; Median (IQR) | 34 (47–23) | |
| - Less than 15 years old | 266,055 (13.5) | 2,204,217 (4.8) |
| - 16 to 30 years old | 581,236 (29.6) | 11,675,207 (25.5) |
| - 31 to 45 years old | 574,452 (29.2) | 12,318,571 (26.9) |
| - 46 to 60 years old | 363,541 (18.5) | 11,519,634 (15.2) |
| - 61 to 75 years old | 140,066 (7.1) | 6,330,258 (13.8) |
| - 76 to 90 years old | 36,959 (1.9) | 1,658,310 (3.6) |
| - More than 90 years old | 2714 (0.1) | 82,118 (0.2) |
| Gender | ||
| - Male | 946,355 (48.2) | 21,888,301 (47.8) |
| - Female | 1,018,668 (51.8) | 23,900,014 (52.2) |
| Total | 1,965,023 | 45,788,315 1 |
| Variables | Time | Overall | Ascending Phase (wk 14–32) | Descending Phase (wk 34–52) | |||
|---|---|---|---|---|---|---|---|
| Estimate (95% CI) | p-Value | Estimate (95% CI) | p-Value | Estimate (95% CI) | p-Value | ||
| Vaccinated Rates | Week 0 | 0.14 (0.07, 0.20) | <0.001 | 2.15 (1.89, 2.42) | <0.01 | −0.52 (−0.67, −0.36) | <0.001 |
| Lagged 2 wks | 0.11 (0.04, 0.17) | <0.001 | 2.42 (2.11, 2.74) | <0.01 | −0.59 (−0.73, −0.45) | <0.001 | |
| Lagged 4 wks | 0.08 (0.01, 0.15) | 0.02 | 2.68 (2.30, 3.06) | <0.01 | −0.65 (−0.79, −0.51) | <0.001 | |
| Lagged 6 wks | 0.06 (−0.02, 0.13) | 0.14 | 3.14 (2.64, 3.64) | <0.01 | −0.73 (−0.88, −0.59) | <0.001 | |
| Lagged 8 wks | 0.03 (−0.05, 0.10) | 0.50 | 3.96 (3.28, 4.63) | <0.01 | −0.83 (−0.97, −0.68) | <0.001 | |
| COVID-19 Zones | Week 0 | ||||||
| - Green zone | - | - | - | - | - | - | |
| - Yellow zone | −0.63 (−13.42, 12.16) | 0.92 | −2.47 (−12.99, 8.06) | 0.65 | - | - | |
| - Orange zone | −2.37 (−14.40, 9.66) | 0.70 | −4.79 (−14.39, 4.81) | 0.33 | −7.35 (−17.28, 2.58) | 0.25 | |
| - Light red zone | 10.51 (−1.46, 22.48) | 0.09 | 10.01 (0.17, 19.83) | 0.05 | 2.74 (−6.41, 11.89) | 0.56 | |
| - Dark red zone | 71.74 (59.03, 84.45) | <0.001 | 93.16 (81.19, 105.12) | <0.01 | 49.95 (39.15, 60.74) | <0.001 | |
| - Blue zone | 24.92 (5.56, 44.29) | 0.01 | - | - | −6.54 (−25.75, 12.66) | 0.50 | |
| Lagged 2 wks | |||||||
| - Green zone | - | - | - | - | - | - | |
| - Yellow zone | 0.90 (−7.44, 9.23) | 0.83 | −0.14 (−6.79, 6.51) | 0.97 | - | - | |
| - Orange zone | −2.68 (−9.75, 4.39) | 0.46 | −5.13 (−10.67, 0.40) | 0.07 | −3.60 (−15.82, 8.62) | 0.56 | |
| - Light red zone | 7.20 (0.28, 14.11) | 0.04 | 9.12 (2.98, 15.25) | <0.01 | −2.74 (−14.13, 8.66) | 0.64 | |
| - Dark red zone | 48.08 (40.08, 56.07) | <0.001 | 83.82 (72.70, 94.95) | <0.01 | 34.12 (21.34, 46.89) | <0.001 | |
| - Blue zone | 14.24 (−4.43, 32.92) | 0.13 | - | - | −8.12 (−29.84, 13.61) | 0.46 | |
| Lagged 4 wks | |||||||
| - Green zone | 2.84 (−5.54, 11.22) | 0.51 | 1.67 (−4.61, 7.95) | 0.60 | - | - | |
| - Yellow zone | 8.50 (0.75, 16.25) | 0.03 | 6.18 (0.27, 12.08) | 0.04 | - | - | |
| - Orange zone | 2.79 (−3.75, 9.32) | 0.40 | −1.11 (−6.22, 4.01) | 0.67 | −11.46 (−33.27, 10.36) | 0.30 | |
| - Light red zone | 8.82 (2.46, 15.18) | 0.01 | 10.25 (3.98, 16.52) | <0.001 | −12.82 (−24.57, 8.93) | 0.25 | |
| - Dark red zone | 34.03 (26.88, 41.18) | <0.001 | 74.40 (62.41, 86.51) | <0.001 | 9.73 (−12.69, 32.15) | 0.40 | |
| - Blue zone | 11.30 (−11.16, 33.75) | 0.32 | - | - | −23.34 (−54.22, 7.55) | 0.14 | |
| Lagged 6 wks | |||||||
| - Green zone | 2.04 (−5.18, 9.27) | 0.58 | 0.87 (−4.68, 6.41) | 0.76 | - | - | |
| - Yellow zone | 10.52 (3.96, 17.09) | 0.01 | 8.28 (2.43, 14.14) | <0.001 | - | - | |
| - Orange zone | 5.80 (0.72, 10.89) | 0.03 | 1.39 (−2.81, 5.59) | 0.52 | −1.42 (−1.88, 15.15) | 0.87 | |
| - Light red zone | 10.08 (5.20, 14.96) | <0.001 | 10.87 (5.09,16.64) | <0.001 | −0.60 (−16.74, 15.54) | 0.94 | |
| - Dark red zone | 22.66 (16.84, 28.49) | <0.001 | 65.53 (51.48, 79.58) | <0.001 | 3.12 (−14.34, 20.59) | 0.73 | |
| - Blue zone | 3.42 (−26.36, 33.21) | 0.82 | - | - | −26.60 (−59.25, 6.05) | 0.11 | |
| Lagged 8 wks | |||||||
| - Green zone | 2.39 (−4.52, 9.30) | 0.50 | 1.43 (−4.23, 7.08) | 0.62 | - | - | |
| - Yellow zone | 9.92 (3.66, 16.19) | 0.01 | 1.63 (−11.02, 14.27) | 0.80 | - | - | |
| - Orange zone | 10.30 (5.68, 14.93) | <0.001 | 4.21 (0.22, 8.20) | 0.04 | 9.91 (−0.15, 19.97) | 0.05 | |
| - Light red zone | 13.76 (9.34, 18.18) | <0.001 | 16.17 (10.35, 22.00) | <0.001 | 1.44 (−6.11, 9.01) | 0.71 | |
| - Dark red zone | 12.54 (7.11, 17.98) | <0.001 | 58.22 (41.46, 74.97) | <0.001 | −19.02 (−29.16, −8.88) | <0.001 | |
| - Blue zone | −4.02 (−54.23, 46.19) | 0.88 | - | - | −31.66 (−79.55, 16.24) | 0.20 | |
| Curfew | Week 0 | 56.43 (51.36, 61.49) | <0.001 | 66.48 (59.04, 73.92) | <0.001 | 49.43 (42.65, 56.22) | <0.001 |
| Lagged 2 wks | 40.97 (36.04, 45.91) | <0.001 | 61.11 (51.73, 70.49) | <0.001 | 37.21 (30.25, 44.16) | <0.001 | |
| Lagged 4 wks | 27.63 (22.80, 32.47) | <0.001 | 56.44 (46.00, 66.89) | <0.001 | 22.48 (14.99, 29.97) | <0.001 | |
| Lagged 6 wks | 15.96 (11.20, 20.72) | <0.001 | 39.45 (27.64, 51.26) | <0.001 | 4.98 (−2.92, 12.89) | 0.21 | |
| Lagged 8 wks | 5.57 (0.80, 10.34) | 0.02 | 30.59 (17.6, 43.53) | <0.001 | −20.68 (−29.27, −12.09) | <0.001 | |
| Migrants | Week 0 | 7.46 (5.74, 9.17) | <0.001 | 8.26 (6.40, 10.13) | <0.001 | 7.17 (4.93, 9.40) | <0.001 |
| Lagged 2 wks | 7.80 (6.07, 9.53) | <0.001 | 8.46 (6.59, 10.33) | <0.001 | 7.09 (4.86, 9.32) | <0.001 | |
| Lagged 4 wks | 8.17 (6.43, 9.91) | <0.001 | 8.55 (6.67, 10.43) | <0.001 | 7.15 (4.92, 9.37) | <0.001 | |
| Lagged 6 wks | 8.38 (6.63, 10.13) | <0.001 | 8.63 (6.74, 10.51) | <0.001 | 7.03 (4.81, 9.25) | <0.001 | |
| Lagged 8 wks | 8.33 (6.60, 10.07) | <0.001 | 8.65 (6.76, 10.55) | <0.001 | 6.79 (4.58, 9.00) | <0.001 | |
| Tourists | Week 0 | −0.10 (−0.20, −0.01) | 0.03 | −0.39 (−0.66, −0.13) | <0.001 | −0.43 (−0.56, −0.29) | <0.001 |
| Lagged 2 wks | −0.23 (−0.34, −0.13) | <0.001 | −0.30 (−0.49, −0.12) | <0.001 | −0.49 (−0.63, −0.35) | <0.001 | |
| Lagged 4 wks | −0.39 (−0.51, −0.27) | <0.001 | −0.24 (−0.38, −0.09) | <0.001 | −0.60 (−0.77, −0.43) | <0.001 | |
| Lagged 6 wks | −0.54 (−0.67, −0.42) | <0.001 | −0.26 (−0.39, −0.13) | <0.001 | −0.79 (−1.00, −0.57) | <0.001 | |
| Lagged 8 wks | −0.60 (−0.72, −0.47) | <0.001 | −0.32 (−0.46, −0.19) | <0.001 | −0.93 (−1.20, −0.65) | <0.001 | |
| Variables | Overall | Ascending Phase (wk 14–32) | Descending Phase (wk 34–52) | |||
|---|---|---|---|---|---|---|
| Estimate (95% CI) | p-Value | Estimate (95% CI) | p-Value | Estimate (95% CI) | p-Value | |
| Vaccinated Rates (Lagged 2 wks] | 0.05 (−0.07, 0.17) | 0.40 | 1.94 (1.54, 2.34) | <0.001 | −0.80 (−1.09, −0.52) | <0.001 |
| COVID-19 zones (Lagged 2 wks] | ||||||
| - Green zone | - | - | - | - | - | - |
| - Yellow zone | −1.69 (−10.63, 7.24) | 0.71 | −10.71 (−18.55, −2.88) | <0.001 | - | - |
| - Orange zone | −5.92 (−13.67, 1.84) | 0.13 | −9.74 (−16.27, −3.21) | <0.001 | −11.32 (−25.37, 2.74) | 0.11 |
| - Light red zone | 3.33 (−5.09, 11.76) | 0.44 | 1.41 (−6.31, 9.13) | 0.72 | −18.62 (−33.41, −3.82) | 0.01 |
| - Dark red zone | 42.63 (32.12, 53.15) | <0.001 | 64.18 (50.70, 77.66) | <0.001 | 17.56 (−0.56, 35.68) | 0.06 |
| - Blue zone | 12.57 (−7.82, 32.97) | 0.23 | - | - | −10.70 (−34.08, 12.67) | 0.37 |
| Migrants (Lagged 2 wks] | 6.44 (4.90, 7.99) | <0.001 | 3.12 (1.49, 4.76) | <0.001 | 8.38 (6.03, 10.72) | <0.001 |
| Tourists (Lagged 2 wks] | −0.28 (−0.45, −0.10) | <0.001 | 0.06 (−0.19, 0.32) | 0.62 | 0.14 (−0.18, 0.47) | 0.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jitpeera, C.; Wongsanuphat, S.; Thammawijaya, P.; Sonthichai, C.; Iamsirithaworn, S.; McNabb, S.J.N. Impact of COVID-19 Vaccination Rates and Public Measures on Case Rates at the Provincial Level, Thailand, 2021: Spatial Panel Model Analyses. Trop. Med. Infect. Dis. 2023, 8, 311. https://doi.org/10.3390/tropicalmed8060311
Jitpeera C, Wongsanuphat S, Thammawijaya P, Sonthichai C, Iamsirithaworn S, McNabb SJN. Impact of COVID-19 Vaccination Rates and Public Measures on Case Rates at the Provincial Level, Thailand, 2021: Spatial Panel Model Analyses. Tropical Medicine and Infectious Disease. 2023; 8(6):311. https://doi.org/10.3390/tropicalmed8060311
Chicago/Turabian StyleJitpeera, Charuttaporn, Suphanat Wongsanuphat, Panithee Thammawijaya, Chaninan Sonthichai, Sopon Iamsirithaworn, and Scott J. N. McNabb. 2023. "Impact of COVID-19 Vaccination Rates and Public Measures on Case Rates at the Provincial Level, Thailand, 2021: Spatial Panel Model Analyses" Tropical Medicine and Infectious Disease 8, no. 6: 311. https://doi.org/10.3390/tropicalmed8060311