
Epidemiology and Economic Burden of Chikungunya: A Systematic Literature Review

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
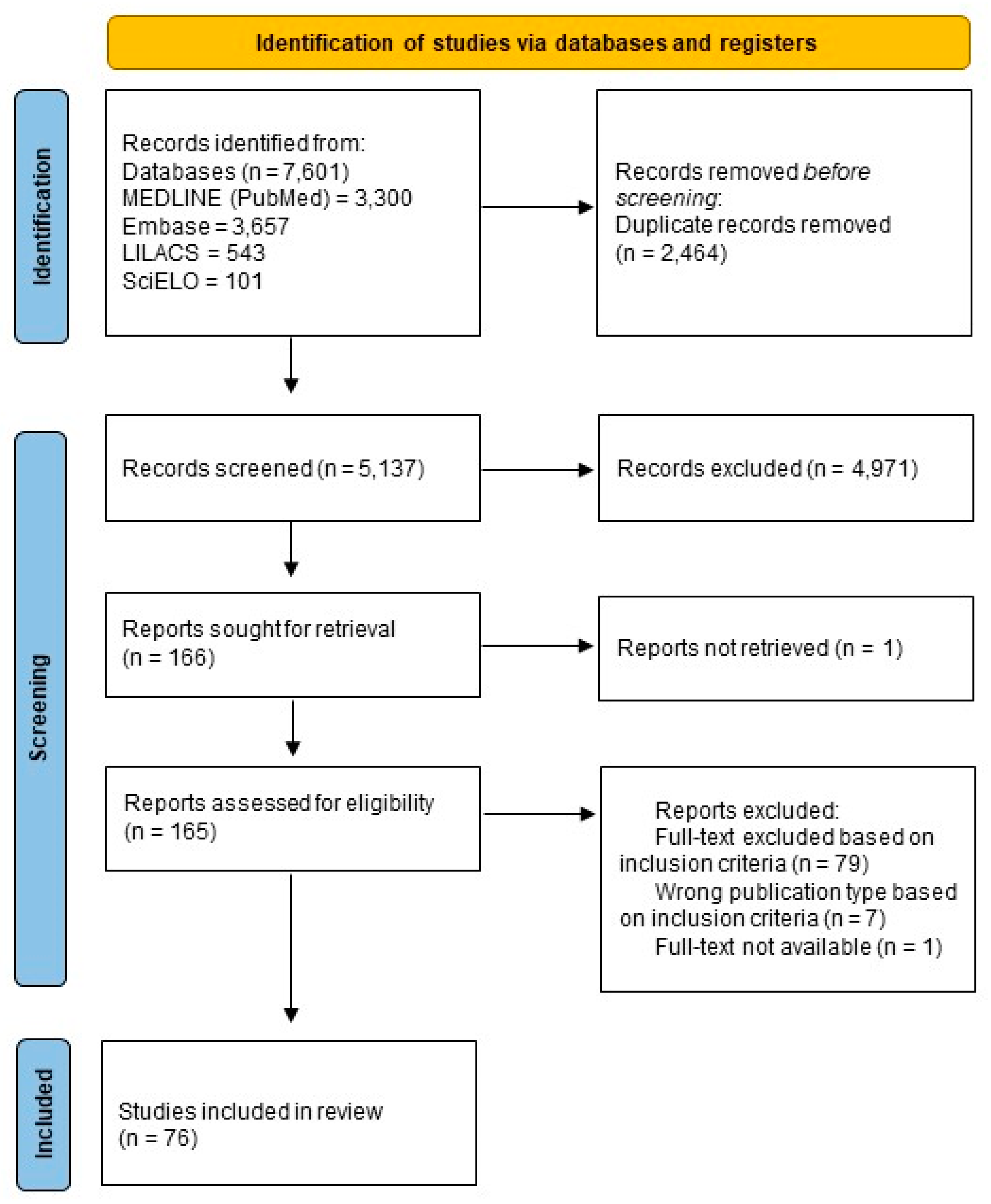
2.1. Study Design, Search Strategy, and Article Selection
2.2. Eligibility Criteria and Study Selection
2.3. Data Extraction and Synthesis
2.4. Quality Assessment
3. Results
3.1. Regional Epidemiology
3.1.1. Africa
3.1.2. Asia
3.1.3. Caribbean and Central America
3.1.4. South America
3.1.5. Worldwide Reviews
3.2. Costs Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Doran, C.; Elsinga, J.; Fokkema, A.; Berenschot, K.; Gerstenbluth, I.; Duits, A.; Lourents, N.; Halabi, Y.; Burgerhof, J.; Bailey, A.; et al. Long-term Chikungunya sequelae and quality of life 2.5 years post-acute disease in a prospective cohort in Curaçao. PLoS Negl. Trop. Dis. 2022, 16, e0010142. [Google Scholar] [CrossRef] [PubMed]
- Freitas, A.R.R.; Alarcón-Elbal, P.M.; Donalisio, M.R. Excess mortality in Guadeloupe and Martinique, islands of the French West Indies, during the chikungunya epidemic of 2014. Epidemiol. Infect. 2018, 146, 2059–2065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frutuoso, L.C.V.; Freitas, A.R.R.; Cavalcanti, L.; Duarte, E.C. Estimated mortality rate and leading causes of death among individuals with chikungunya in 2016 and 2017 in Brazil. Rev. Soc. Bras. Med. Trop. 2020, 53, e20190580. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Ahmed, S.; Parray, H.A.; Das, S. Chikungunya and arthritis: An overview. Travel Med. Infect. Dis. 2021, 44, 102168. [Google Scholar] [CrossRef]
- Khongwichit, S.; Chansaenroj, J.; Chirathaworn, C.; Poovorawan, Y. Chikungunya virus infection: Molecular bi-ology, clinical characteristics, and epidemiology in Asian countries. J. Biomed. Sci. 2021, 28, 84. [Google Scholar] [CrossRef]
- Manzoor, K.N.; Javed, F.; Ejaz, M.; Ali, M.; Mujaddadi, N.; Khan, A.A.; Khattak, A.A.; Zaib, A.; Ahmad, I.; Saeed, W.K.; et al. The global emergence of Chikungunya infection: An integrated view. Rev. Med. Virol. 2022, 32, e2287. [Google Scholar] [CrossRef]
- Matusali, G.; Colavita, F.; Bordi, L.; Lalle, E.; Ippolito, G.; Capobianchi, M.R.; Castilletti, C. Tropism of the chikungunya virus. Viruses 2019, 11, 175. [Google Scholar] [CrossRef] [Green Version]
- Robinson, M.C. An epidemic of virus disease in Southern Province, Tanganyika territory, in 1952–1953. Trans. R. Soc. Trop. Med. Hyg. 1955, 49, 28–32. [Google Scholar] [CrossRef]
- Ross, R.W. The Newala epidemic: III. The virus: Isolation, pathogenic properties and relationship to the epi-demic. J. Hyg. 1956, 54, 177–191. [Google Scholar] [CrossRef] [Green Version]
- Wahid, B.; Ali, A.; Rafique, S.; Idrees, M. Global expansion of chikungunya virus: Mapping the 64-year history. Int. J. Infect. Dis. 2017, 58, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Grandadam, M.; Caro, V.; Plumet, S.; Thiberge, J.M.; Souarès, Y.; Failloux, A.B.; Tolou, H.J.; Budelot, M.; Cosserat, D.; Leparc-Goffart, I.; et al. Chikungunya virus, Southeastern France. Emerg. Infect. Dis. 2011, 17, 910–913. [Google Scholar] [CrossRef]
- Rezza, G.; Nicoletti, L.; Angelini, R.; Romi, R.; Finarelli, A.C.; Panning, M.; Cordioli, P.; Fortuna, C.; Boros, S.; Magurano, F.; et al. Faculty Opinions recommendation of Infection with chikungunya virus in Italy: An outbreak in a temperate region. Lancet 2007, 370, 1840–1846. [Google Scholar] [CrossRef]
- Cardona-Ospina, J.A.; Henao-SanMartin, V.; Paniz-Mondolfi, A.E.; Rodríguez-Morales, A.J. Mortality and fatality due to Chikungunya virus infection in Colombia. J. Clin. Virol. 2015, 70, 14–15. [Google Scholar] [CrossRef]
- Cardona-Ospina, J.A.; Diaz-Quijano, F.A.; Rodríguez-Morales, A.J. Burden of chikungunya in Latin American countries: Estimates of disability-adjusted life-years (DALY) lost in the 2014 epidemic. Int. J. Infect. Dis. 2015, 38, 60–61. [Google Scholar] [CrossRef] [Green Version]
- Lindh, E.; Argentini, C.; Remoli, M.E.; Fortuna, C.; Faggioni, G.; Benedetti, E.; Amendola, A.; Marsili, G.; Lista, F.; Rezza, G.; et al. The Italian 2017 outbreak chikungunya virus belongs to an emerging aedes albopictus-adapted virus cluster introduced from the Indian sub-continent. In Open Forum Infectious Diseases; Oxford University Press: New York, NY, USA, 2019; Volume 6, Available online: https://www.embase.com/search/results?subaction=viewrecord&id=L626501633&from=export (accessed on 27 November 2022).
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2000. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 29 November 2022).
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observa-tional epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid.-Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Silva EN, D.; Silva, M.T.; Augustovski, F.; Husereau, D.; Pereira, M.G. Roteiro para relato de es-tudos de avaliação econômica. Epidemiol. Serviços Saúde 2017, 26, 895–898. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Renault, P.; Solet, J.L.; Sissoko, D.; Balleydier, E.; Larrieu, S.; Filleul, L.; Lassalle, C.; Thiria, J.; Rachou, E.; de Valk, H.; et al. A major epidemic of chikungunya virus infection on Réunion Island, France, 2005–2006. Am. J. Trop. Med. Hyg. 2007, 77, 727–731. [Google Scholar] [CrossRef] [Green Version]
- Mwanyika, G.O.; Sindato, C.; Rugarabamu, S.; Rumisha, S.F.; Karimuribo, E.D.; Misinzo, G.; Rweyemamu, M.M.; Hamid, M.M.A.; Haider, N.; Vairo, F.; et al. Seroprevalence and associated risk factors of chikungunya, dengue, and Zika in eight districts in Tanzania. Int. J. Infect. Dis. 2021, 111, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Sissoko, D.; Moendandzé, A.; Malvy, D.; Giry, C.; Ezzedine, K.; Solet, J.L.; Pierre, V. Seroprevalence and Risk Factors of Chikungunya Virus Infection in Mayotte, Indian Ocean, 2005–2006: A Population-Based Survey. PLoS ONE 2008, 3, e3066. [Google Scholar] [CrossRef] [PubMed]
- Sergon, K.; Sang, R.; Brown, J.; Onyango, C.; Powers, A.M.; Agata, N.; Njenga, M.K.; Bedja, S.A.; Allaranger, Y.; Konongoi, L.S.; et al. Seroprevalence of Chikungunya virus infection on Grande Comore Island, Union of the Comoros, 2005. Am. J. Trop. Med. Hyg. 2007, 76, 1189–1193. [Google Scholar] [CrossRef] [PubMed]
- Sergon, K.; Njuguna, C.; Kalani, R.; Ofula, V.; Onyango, C.; Konongoi, L.S.; Bedno, S.; Burke, H.; Dumilla, A.M.; Konde, J.; et al. Seroprevalence of Chikungunya virus (CHIKV) infection on Lamu Island, Kenya, October 2004. Am. J. Trop. Med. Hyg. 2008, 78, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Mease, L.E.; Coldren, R.L.; Musila, L.A.; Prosser, T.; Ogolla, F.; Ofula, V.O.; Schoepp, R.J.; Rossi, C.A.; Adungo, N. Seroprevalence and distribution of ar-boviral infections among rural Kenyan adults: A cross-sectional study. Virol. J. 2011, 8, 371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moyen, N.; Thiberville, S.-D.; Pastorino, B.; Nougairede, A.; Thirion, L.; Mombouli, J.-V.; Dimi, Y.; Leparc-Goffart, I.; Capobianchi, M.R.; Lepfoundzou, A.D.; et al. First Reported Chikungunya Fever Outbreak in the Republic of Congo, 2011. PLoS ONE 2014, 9, e115938. [Google Scholar] [CrossRef] [Green Version]
- Endale, A.; Michlmayr, D.; Abegaz, W.E.; Asebe, G.; Larrick, J.W.; Medhin, G.; Legesse, M. Community-based sero-prevalence of chikungunya and yellow fever in the South Omo Valley of Southern Ethiopia. PLOS Negl. Trop. Dis. 2020, 14, e0008549. [Google Scholar] [CrossRef]
- António, V.S.; Muianga, A.F.; Wieseler, J.; Pereira, S.A.; Monteiro, V.O.; Mula, F.; Chelene, I.; Chongo, I.S.; Oludele, J.O.; Kümmerer, B.M.; et al. Seroepidemiology of Chikungunya Virus among Febrile Patients in Eight Health Facilities in Central and Northern Mozambique, 2015–2016. Vector-Borne Zoonotic Dis. 2018, 18, 311–316. [Google Scholar] [CrossRef]
- Abdullahi, I.N.; Akande, A.O.; Muhammed, Y.; Rogo, L.D.; Oderinde, B. Prevalence Pattern of Chikungunya Virus Infection in Nigeria: A Four Decade Systematic Review and Meta-analysis. Pathog. Glob. Health 2020, 114, 120–125. [Google Scholar] [CrossRef]
- Ekong, P.S.; Aworh, M.K.; Grossi-Soyster, E.N.; Wungak, Y.S.; Maurice, N.A.; Altamirano, J.; Ekong, M.J.; Olugasa, B.O.; Nwosuh, C.I.; Shamaki, D.; et al. A Retrospective Study of the Seroprevalence of Dengue Virus and Chikungunya Virus Exposures in Nigeria, 2010–2018. Pathogens 2022, 11, 762. [Google Scholar] [CrossRef]
- Hertz, J.T.; Munishi, O.M.; Ooi, E.E.; Howe, S.; Lim, W.Y.; Chow, A.; Morrissey, A.B.; Bartlett, J.A.; Onyango, J.J.; Maro, V.P.; et al. Chikungunya and dengue fever among hospitalized febrile patients in northern Tanzania. Am. J. Trop. Med. Hyg. 2012, 86, 171–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinimi, E.; Shayo, M.J.; Patrick, B.N.; Angwenyi, S.O.; Kasanga, C.J.; Weyer, J.; Jansen van Vuren, P.; Paweska, J.T.; Mboera, L.E.; Misinzo, G. Evidence of chikungunya virus infection among febrile patients seeking healthcare in selected districts of Tanzania. Infect. Ecol. Epidemiol. 2018, 8, 1553460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sergon, K.; Njuguna, C.; Kalani, R.; Ofula, V.; Onyango, C.; Konongoi, L.S.; Bedno, S.; Burke, H.; Dumilla, A.M.; Konde, J.; et al. Chikungunya Virus-associated Long-term Arthralgia: A 36-month Prospective Longitudinal Study. PLoS Negl. Trop. Dis. 2013, 7, e2137. [Google Scholar]
- Soumahoro, M.K.; Gerardin, P.; Boelle, P.Y.; Perrau, J.; Fianu, A.; Pouchot, J.; Malvy, D.; Flahault, A.; Favier, F.; Hanslik, T. Impact of Chikungunya Virus Infection on Health Status and Quality of Life: A Retrospective Cohort Study. Klein R, editor. PLoS ONE 2009, 4, e7800. [Google Scholar] [CrossRef]
- Gérardin, P.; Fianu, A.; Malvy, D.; Mussard, C.; Boussaïd, K.; Rollot, O.; Michault, A.; Gaüzere, B.A.; Bréart, G.; Favier, F. Perceived morbidity and community burden after a Chikungunya outbreak: The TELECHIK survey, a population-based cohort study. BMC Med. 2011, 9, 5. [Google Scholar] [CrossRef] [Green Version]
- Economopoulou, A.; Dominguez, M.; Helynck, B.; Sissoko, D.; Wichmann, O.; Quenel, P.; Germonneau, P.; Quatresous, I. Atypical Chikungunya virus infections: Clinical manifestations, mortality and risk factors for severe disease during the 2005–2006 outbreak on Réunion. Epidemiol. Infect. 2009, 137, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Azami, N.A.M.; Salleh, S.A.; Shah, S.A.; Neoh, H.M.; Othman, Z.; Zakaria, S.Z.S.; Jamal, R. Emergence of chikungunya seropositivity in healthy Malaysian adults residing in outbreak-free locations: Chikungunya seroprevalence results from the Malaysian Cohort. BMC Infect. Dis. 2013, 13, 67. [Google Scholar] [CrossRef] [Green Version]
- Khatun, S.; Chakraborty, A.; Rahman, M.; Nasreen Banu, N.; Rahman, M.M.; Hasan, S.M.; Luby, S.P.; Gurley, E.S. An outbreak of chikungunya in rural Bangladesh, 2011. PLoS Negl. Trop. Dis. 2015, 9, e0003907. [Google Scholar] [CrossRef] [Green Version]
- Hossain, M.S.; Hasan, M.M.; Islam, M.S.; Islam, S.; Mozaffor, M.; Khan, M.A.S.; Ahmed, N.; Akhtar, W.; Chowdhury, S.; Arafat, S.Y.; et al. Chikungunya outbreak (2017) in Bangladesh: Clinical profile, economic impact and quality of life during the acute phase of the disease. PLoS Negl. Trop. Dis. 2018, 12, e0006561. [Google Scholar] [CrossRef]
- Ray, P.; Ratagiri, V.H.; Kabra, S.K.; Lodha, R.; Sharma, S.; Sharma, B.S.; Kalaivani, M.; Wig, N. Chikungunya infection in India: Results of a prospective hospital based multi-centric study. PLoS ONE 2012, 7, e30025. [Google Scholar] [CrossRef] [Green Version]
- Chattopadhyay, S.; Mukherjee, R.; Nandi, A.; Bhattacharya, N. Chikungunya virus infection in West Bengal, India. Indian J. Med. Microbiol. 2016, 34, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.S.; Kamaraj, P.; Khan, S.A.; Allam, R.R.; Barde, P.V.; Dwibedi, B.; Kanungo, S.; Mohan, U.; Mohanty, S.S.; Roy, S.; et al. Seroprevalence of chikungunya virus infection in India, 2017: A cross-sectional population-based serosurvey. Lancet Microbe 2021, 2, e41–e47. [Google Scholar] [CrossRef] [PubMed]
- Khongwichit, S.; Chansaenroj, J.; Thongmee, T.; Benjamanukul, S.; Wanlapakorn, N.; Chirathaworn, C.; Poovorawan, Y. Large-scale outbreak of Chikungunya virus infection in Thailand, 2018–2019. PLoS ONE 2021, 16, e0247314. [Google Scholar]
- Aubry, M.; Kama, M.; Henderson, A.D.; Teissier, A.; Vanhomwegen, J.; Mariteragi-Helle, T.; Paoaafaite, T.; Manuguerra, J.C.; Christi, K.; Watson, C.H.; et al. Low chikungunya virus seroprevalence two years after emergence in Fiji. Int. J. Infect. Dis. 2020, 90, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Dutta, P.; Khan, S.A.; Phukan, A.C.; Hazarika, S.; Hazarika, N.K.; Chetry, S.; Khan, A.M.; Kaur, H. Surveillance of Chikungunya virus activity in some North-eastern states of India. Asian Pac. J. Trop. Med. 2019, 12, 1–7. [Google Scholar] [CrossRef]
- Barr, K.L.; Khan, E.; Farooqi, J.Q.; Imtiaz, K.; Prakoso, D.; Malik, F.; Lednicky, J.A.; Long, M.T. Evidence of Chikungunya Virus Disease in Pakistan Since 2015 With Patients Demonstrating Involvement of the Central Nervous System. Front. Public Health 2018, 6, 186. [Google Scholar] [CrossRef] [Green Version]
- Badar, N.; Ikram, A.; Salman, M.; Alam, M.M.; Umair, M.; Arshad, Y.; Mushtaq, N.; Mirza, H.A.; Ahad, A.; Yasin, M.T.; et al. Epidemiology of Chikungunya virus isolates 2016–2018 in Pakistan. J. Med. Virol. 2021, 93, 6124–6131. [Google Scholar] [CrossRef]
- Joshi, P.; Yadav, P.; Mourya, D.; Sahare, L.; Ukey, M.; Khedekar, R.; Patil, D.; Barde, P.V. Laboratory surveillance of chikungunya in Madhya Pradesh, India (2016–2017). Indian J. Med. Res. 2020, 151, 87–92. [Google Scholar]
- Mathew, A.J.; Goyal, V.; George, E.; Thekkemuriyil, D.V.; Jayakumar, B.; Chopra, A. Rheumatic-musculoskeletal pain and disorders in a naïve group of individuals 15 months following a Chikungunya viral epidemic in south India: A population based observational study. Int. J. Clin. Pract. 2011, 65, 1306–1312. [Google Scholar] [CrossRef]
- Ramachandran, V.; Malaisamy, M.; Ponnaiah, M.; Kaliaperuaml, K.; Vadivoo, S.; Gupte, M.D. Impact of Chikungunya on health related quality of life Chennai, South India. PLoS ONE 2012, 7, e51519. [Google Scholar]
- Vongpunsawad, S.; Intharasongkroh, D.; Thongmee, T.; Poovorawan, Y. Seroprevalence of antibodies to dengue and chikungunya viruses in Thailand. PLoS ONE 2017, 12, e0180560. [Google Scholar] [CrossRef] [Green Version]
- Murhekar, M.; Kanagasabai, K.; Shete, V.; Joshua, V.; Ravi, M.; Kirubakaran, B.K.; Ramachandran, R.; Sabarinathan, R.; Gupta, N. Epidemiology of chikungunya based on laboratory surveillance data—India, 2016–2018. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 259–262. [Google Scholar] [CrossRef]
- Luvai, E.A.C.; Kyaw, A.K.; Sabin, N.S.; Yu, F.; Hmone, S.W.; Thant, K.Z.; Inoue, S.; Morita, K.; Ngwe Tun, M.M. Evidence of Chikungunya virus seroprevalence in Myanmar among denguesuspected patients and healthy volunteers in 2013, 2015, and 2018. PLoS Negl. Trop. Dis. 2021, 15, e0009961. [Google Scholar] [CrossRef]
- Chopra, A.; Ghorpade, R.; Venugopalan, A.; Saluja, M.; Adam, K. Increased Burden of Painful Arthritis and Rheumatism Following the Chikungunya Epidemic 2006: India Rural Population Survey 2018. Arthritis Rheumatol. 2020, 72, 1124–1125. [Google Scholar]
- Henry, M.; Francis, L.; Asin, V.; Polson-Edwards, K.; Olowokure, B. Chikungunya virus outbreak in Sint Maarten, 2013–2014. Rev. Panam. Salud Publica 2017, 41, e61. [Google Scholar] [CrossRef]
- Couzigou, B.; Criquet-Hayot, A.; Javelle, E.; Tignac, S.; Mota, E.; Rigaud, F.; Alain, A.; Troisgros, O.; Pierre-Francois, S.; Abel, S.; et al. Occurrence of Chronic Stage Chikungunya in the General Population of Martinique during the First 2014 Epidemic: A Prospective Epidemiological Study. Am. J. Trop. Med. Hyg. 2018, 99, 182–190. [Google Scholar] [CrossRef]
- Gallian, P.; Leparc-Goffart, I.; Richard, P.; Maire, F.; Flusin, O.; Djoudi, R.; Chiaroni, J.; Charrel, R.; Tiberghien, P.; de Lamballerie, X. Epidemiology of Chikungunya Virus Outbreaks in Guadeloupe and Martinique, 2014: An Observational Study in Volunteer Blood Donors. PLoS Negl. Trop. Dis. 2017, 11, e0005254. [Google Scholar] [CrossRef] [Green Version]
- Hennessey, M.J.; Ellis, E.M.; Delorey, M.J.; Panella, A.J.; Kosoy, O.I.; Kirking, H.L.; Appiah, G.D.; Qin, J.; Basile, A.J.; Feldstein, L.R.; et al. Seroprevalence and symptomatic attack rate of chikungunya virus infection, United States virgin islands, 2014–2015. Am. J. Trop. Med. Hyg. 2018, 99, 1321–1326. [Google Scholar] [CrossRef] [Green Version]
- Sharp, T.M.; Ryff, K.R.; Alvarado, L.; Shieh, W.J.; Zaki, S.R.; Margolis, H.S.; Rivera-Garcia, B. Surveillance for chikungunya and dengue during the first year of chikungunya virus circulation in puerto rico. J. Infect. Dis. 2016, 214, S475–S481. [Google Scholar] [CrossRef] [Green Version]
- Ministerio del Poder Ciudadano para la Salud de Nicaragua. Seroprevalencia y tasa de ataque clínica por chikungunya en Nicaragua, 2014–2015. Rev. Panam. Salud Pública 2017, 41, e59. [Google Scholar]
- Gordon, A.; Gresh, L.; Ojeda, S.; Chowell, G.; Gonzalez, K.; Sanchez, N.; Saborio, S.; Mercado, J.C.; Kuan, G.; Balmaseda, A.; et al. Differences in Transmission and Disease Severity between 2 Successive Waves of Chikungunya. Clin. Infect. Dis. 2018, 67, 1760–1767. [Google Scholar] [CrossRef] [PubMed]
- Dorléans, F.; Hoen, B.; Najioullah, F.; Herrmann-Storck, C.; Schepers, K.M.; Abel, S.; Lamaury, I.; Fagour, L.; Cesaire, R.; Guyomard, S.; et al. Outbreak of chikungunya in the French caribbean islands of martinique and guadeloupe: Findings from a hospital-Based surveillance system (2013–2015). Am. J. Trop. Med. Hyg. 2018, 98, 1819–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crosby, L.; Perreau, C.; Madeux, B.; Cossic, J.; Armand, C.; Herrmann-Storke, C.; Najioullah, F.; Valentino, R.; Thiéry, G. Severe manifestations of chikungunya virus in critically ill patients during the 2013–2014 Caribbean outbreak. Int. J. Infect. Dis. 2016, 48, 78–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crosby, L.; Perreau, C.; Madeux, B.; Cossic, J.; Armand, C.; Herrmann-Storke, C.; Najioullah, F.; Valentino, R.; Thiéry, G. Prevalence of chronic chikungunya and associated risks factors in the French West Indies (La Martinique): A prospective cohort study. PLoS Negl. Trop. Dis. 2020, 14, e0007327. [Google Scholar]
- Huits, R.; De Kort, J.; Berg, R.V.D.; Chong, L.; Tsoumanis, A.; Eggermont, K.; Bartholomeeusen, K.; Arien, K.K.; Jacobs, J.; Van Esbroeck, M.; et al. Chikungunya virus infection in Aruba: Diagnosis, clinical features and predictors of post-chikungunya chronic polyarthralgia. PloS ONE 2018, 13, e0196630. [Google Scholar] [CrossRef]
- Mercado-Reyes, M.; Acosta-Reyes, J.; Navarro-Lechuga, E.; Corchuelo, S.; Rico, A.; Parra, E.; Tolosa, N.; Pardo, L.; González, M.; Martìn-Rodriguez-Hernández, J.; et al. Dengue, chikungunya and zika virus coinfection: Results of the national surveillance during the zika epidemic in Colombia. Epidemiol. Infect. 2019, 147, e77. [Google Scholar] [CrossRef] [Green Version]
- Ster, I.C.; Rodriguez, A.; Romero, N.C.; Lopez, A.; Chico, M.; Montgomery, J.; Cooper, P. Age-dependent seroprevalence of dengue and chikungunya: Inference from a cross-sectional analysis in Esmeraldas Province in coastal Ecuador. BMJ Open 2020, 10, e040735. [Google Scholar] [CrossRef]
- Bailly, S.; Rousset, D.; Fritzell, C.; Hozé, N.; Ben Achour, S.; Berthelot, L.; Enfissi, A.; Vanhomwegen, J.; Salje, H.; Fernandes-Pellerin, S.; et al. Spatial distribution and burden of emerging arboviruses in French Guiana. Viruses 2021, 13, 1299. [Google Scholar] [CrossRef]
- Dias, J.P.; Maria da Conceição, N.C.; Campos, G.S.; Paixão, E.S.; Natividade, M.S.; Barreto, F.R.; Itaparica, M.S.C.; Goes, C.; Oliveira, F.L.; Santana, E.B.; et al. Seroprevalence of Chikungunya Virus after Its Emergence in Brazil. Emerg. Infect. Dis. 2018, 24, 1773. [Google Scholar] [CrossRef] [Green Version]
- Cunha, R.V.; Trinta, K.S.; Montalbano, C.A.; Sucupira, M.V.F.; de Lima, M.M.; Marques, E.; Romanholi, I.H.; Croda, J. Seroprevalence of Chikungunya Virus in a Rural Community in Brazil. PLOS Neglected Trop. Dis. 2017, 11, e0005319. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, M.G.; Skalinski, L.M.; Paixão, E.S.; Costa, M.D.C.N.; Barreto, F.R.; Campos, G.S.; Sardi, S.I.; Carvalho, R.H.; Natividade, M.; Itaparica, M.; et al. Seroprevalence of Chikungunya virus and living conditions in Feira de Santana, Bahia-Brazil. PLOS Negl. Trop. Dis. 2021, 15, e0009289. [Google Scholar] [CrossRef] [PubMed]
- Nicacio, J.M.; Khouri, R.; da Silva, A.M.L.; Barral-Netto, M.; Lima, J.A.C.; Ladeia, A.M.T.; Carmo, R.F.D.; Armstrong, A.D.C. Anti-chikungunya virus seroprevalence in Indigenous groups in the São Francisco Valley, Brazil. PLOS Negl. Trop. Dis. 2021, 15, e0009468. [Google Scholar] [CrossRef] [PubMed]
- Anjos, R.O.; Mugabe, V.A.; Moreira, P.S.; Carvalho, C.X.; Portilho, M.M.; Khouri, R.; Sacramento, G.A.; Nery, N.R.; Reis, M.G.; Kitron, U.D.; et al. Transmission of Chikungunya Virus in an Urban Slum, Brazil. Emerg. Infect. Dis. 2020, 26, 1364–1373. [Google Scholar] [CrossRef] [PubMed]
- Simião, A.R.; Barreto, F.K.D.A.; Oliveira, R.D.M.A.B.; Cavalcante, J.W.; Neto, A.S.L.; Barbosa, R.B.; Lins, C.D.S.; Meira, A.G.; Araújo, F.M.D.C.; Lemos, D.R.Q.; et al. A major chikungunya epidemic with high mortality in northeastern Brazil. Rev. Soc. Bras. Med. Trop. 2019, 52, e20190266. [Google Scholar] [CrossRef] [PubMed]
- Barreto, M.C.A.; Gomes, I.P.; de Castro, S.S. Qualidade de vida dos pacientes com chikungunya: Fatores associados durante uma epidemia ocorrida no nordeste do Brasil. J. Health Biol. Sci. 2021, 9, 1–8. [Google Scholar] [CrossRef]
- Barreto, F.K.A.; Alencar, C.H.; Araújo, F.M.D.C.; Oliveira, R.D.M.A.B.; Cavalcante, J.W.; Lemos, D.R.Q.; Farias, L.A.B.G.; Boriz, I.L.F.; Medeiros, L.Q.; Melo, M.N.P.; et al. Seroprevalence, spatial dispersion and factors associated with flavivirus and chikungunya infection in a risk area: A population-based seroprevalence study in Brazil. BMC Infect. Dis. 2020, 20, 881. [Google Scholar] [CrossRef]
- Périssé, A.R.S.; Souza-Santos, R.; Duarte, R.; Santos, F.; De Andrade, C.R.; Rodrigues, N.C.P.; Schramm, J.M.D.A.; Da Silva, E.D.; Jacobson, L.D.S.V.; Lemos, M.C.F.; et al. Zika, dengue and chikungunya population prevalence in Rio de Janeiro city, Brazil, and the importance of seroprevalence studies to estimate the real number of infected individuals. PLoS ONE 2020, 15, e0243239. [Google Scholar] [CrossRef]
- Vidal, E.R.N.; Frutuoso, L.C.V.; Duarte, E.C.; Peixoto, H.M. Epidemiological burden of Chikungunya fever in Brazil, 2016 and 2017. Trop. Med. Int. Health 2021, 27, 174–184. [Google Scholar] [CrossRef]
- Li, Z.; Wang, J.; Cheng, X.; Hu, H.; Guo, C.; Huang, J.; Chen, Z.; Lu, J. The worldwide seroprevalence of DENV, CHIKV and ZIKV infection: A systematic review and meta-analysis. PloS Negl. Trop. Dis. 2021, 15, e0009337. [Google Scholar] [CrossRef]
- Badawi, A.; Ryoo, S.G.; Vasileva, D.; Yaghoubi, S. Prevalence of chronic comorbidities in chikungunya: A system-atic review and meta-analysis. Int. J. Infect. Dis. 2018, 67, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Morales, A.J.; Cardona-Ospina, J.A.; Fernanda Urbano-Garzón, S.; Sebastian Hurtado-Zapata, J. Preva-lence of Post-Chikungunya Infection Chronic Inflammatory Arthritis: A Systematic Review and Meta-Analysis. Arthritis Care Res. 2016, 68, 1849–1858. [Google Scholar] [CrossRef]
- Krishnamoorthy, K.; Harichandrakumar, K.T.; Kumari, A.K.; Das, L.K. Burden of chikungunya in India: Estimates of disability adjusted life years (DALY) lost in 2006 epidemic. J. Vector Borne Dis. 2009, 46, 26–35. [Google Scholar]
- Gopalan, S.S.; Das, A. Household economic impact of an emerging disease in terms of catastrophic out-of-pocket health care expenditure and loss of productivity: Investigation of an outbreak of chikungunya in Orissa, India. J. Vector Borne Dis. 2009, 46, 57–64. [Google Scholar]
- Soumahoro, M.-K.; Boelle, P.-Y.; Gaüzere, B.-A.; Atsou, K.; Pelat, C.; Lambert, B.; La Ruche, G.; Gastellu-Etchegorry, M.; Renault, P.; Sarazin, M.; et al. The Chikungunya Epidemic on La Réunion Island in 2005–2006: A Cost-of-Illness Study. PLOS Negl. Trop. Dis. 2011, 5, e1197. [Google Scholar] [CrossRef] [Green Version]
- Alvis-Zakzuk, N.J.; Díaz-Jiménez, D.; Castillo-Rodríguez, L.; Castañeda-Orjuela, C.; Paternina-Caicedo, Á.; Pinzón-Redondo, H.; Carrasquilla-Sotomayor, M.; Alvis-Guzmán, N.; De La Hoz-Restrepo, F. Economic Costs of Chikungunya Virus in Colombia. Value Health Reg. Issues 2018, 17, 32–37. [Google Scholar] [CrossRef]
- Vázquez-Cruz, I.; Juanico-Morales, G.; Sanchez-Ramos, A.; de Jesús Morales-Sánchez, O. Costs and sick leave due to chikungunya in the Instituto Mexicano del Seguro Social in Guerrero, Mexico. Rev. Médica Del Inst. Mex. Del Seguro Soc. 2018, 56, 54–63. [Google Scholar]
- Feldstein, L.R.; Ellis, E.M.; Rowhani-Rahbar, A.; Hennessey, M.J.; Staples, J.E.; Halloran, M.E.; Weaver, M.R. Estimating the cost of illness and burden of disease associated with the 2014–2015 chikungunya outbreak in the US Virgin Islands. PloS Negl. Trop. Dis. 2019, 13, e0007563. [Google Scholar] [CrossRef] [Green Version]
- Mora-Salamanca, A.F.; Porras-Ramírez, A.; Restrepo, F.P.D.L.H. Estimating the burden of arboviral diseases in Colombia between 2013 and 2016. Int. J. Infect. Dis. 2020, 97, 81–89. [Google Scholar] [CrossRef]
- Teich, V.; Arinelli, R.; Fahham, L. Aedes aegypti e sociedade: O impacto econômico das rboviruses no Brasil. J. Bras. Econ. Saúde 2017, 9, 267–276. [Google Scholar] [CrossRef]
- De Almeida Barreto, F.K.; Montenegro, R.M.; Fernandes, V.O.; Oliveira, R.; de Araújo Batista, L.A.; Hussain, A.; de Góes Cavalcanti, L.P. Chikungunya and diabetes, what do we know? Diabetol. Metab. Syndr. 2018, 10, 32. [Google Scholar] [CrossRef]
- Fernandes, S.; Pinto, M.; Barros, L.; Moreira, M.E.L.; de Araújo, T.V.B.; Lyra, T.M.; Valongueiro, S.; Jofre-Bonet, M.; Kuper, H. The economic burden of congenital Zika Syndrome in Brazil: An overview at 5 years and 10 years. BMJ Glob. Health 2022, 7, e008784. [Google Scholar] [CrossRef] [PubMed]
- Gopakumar, H.; Ramachandran, S. Congenital chikungunya. J. Clin. Neonatol. 2012, 1, 155–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Country/Region | Direct Costs (USD) | Loss in Productivity (USD) | DALYs |
|---|---|---|---|
| India/Asia | 16.680 | 2.57–4.69 million | 25,588 |
| Reunion Islands/French Department | 36.72 million | 18.79 million | - |
| Colombia/South America | 121.7–563.8 per patient | 72.2–203.2 per patient | 350,531 |
| Brazil/South America | - | 2.13 billion | 0.036 |
| Mexico/North America | - | 130 thousand | - |
| USA/North America | 2.9 million | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, L.B.; Barreto, F.K.d.A.; Barreto, M.C.A.; Santos, T.H.P.d.; Andrade, M.d.M.O.d.; Farias, L.A.B.G.; Freitas, A.R.R.d.; Martinez, M.J.; Cavalcanti, L.P.d.G. Epidemiology and Economic Burden of Chikungunya: A Systematic Literature Review. Trop. Med. Infect. Dis. 2023, 8, 301. https://doi.org/10.3390/tropicalmed8060301
Costa LB, Barreto FKdA, Barreto MCA, Santos THPd, Andrade MdMOd, Farias LABG, Freitas ARRd, Martinez MJ, Cavalcanti LPdG. Epidemiology and Economic Burden of Chikungunya: A Systematic Literature Review. Tropical Medicine and Infectious Disease. 2023; 8(6):301. https://doi.org/10.3390/tropicalmed8060301
Chicago/Turabian StyleCosta, Lourrany Borges, Francisca Kalline de Almeida Barreto, Marina Carvalho Arruda Barreto, Thyago Henrique Pereira dos Santos, Maria de Margarette Oliveira de Andrade, Luís Arthur Brasil Gadelha Farias, André Ricardo Ribas de Freitas, Miguel Julian Martinez, and Luciano Pamplona de Góes Cavalcanti. 2023. "Epidemiology and Economic Burden of Chikungunya: A Systematic Literature Review" Tropical Medicine and Infectious Disease 8, no. 6: 301. https://doi.org/10.3390/tropicalmed8060301