
Neurological Diseases Define the Cytokine Profile in CFS during SARS-CoV-2 Infection in Highly Ill Patients
Abstract
:1. Introduction
2. Relevant Section
3. Discussion
4. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harapan, B.N.; Yoo, H.J. Neurological symptoms, manifestations, and complications associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19). J. Neurol. 2021, 268, 3059–3071. [Google Scholar] [CrossRef]
- Méndez-García, L.A.; Escobedo, G.; Minguer-Uribe, A.G.; Viurcos-Sanabria, R.; Aguayo-Guerrero, J.A.; Carrillo-Ruiz, J.D.; Solleiro-Villavicencio, H. Role of the renin-angiotensin system in the development of COVID-19-associated neurological manifestations. Front. Cell. Neurosci. 2022, 16, 488. [Google Scholar] [CrossRef]
- Zubair, A.S.; McAlpine, L.S.; Gardin, T.; Farhadian, S.; Kuruvilla, D.E.; Spudich, S. Neuropathogenesis and Neurologic Manifestations of the Coronaviruses in the Age of Coronavirus Disease 2019: A Review. JAMA Neurol. 2020, 77, 1018–1027. [Google Scholar] [CrossRef]
- Ju, J.; Su, Y.; Zhou, Y.; Wei, H.; Xu, Q. The SARS-CoV-2 envelope protein disrupts barrier function in an in vitro human blood-brain barrier model. Front. Cell. Neurosci. 2022, 16, 432. [Google Scholar] [CrossRef]
- Taipa, R.; das Neves, S.P.; Sousa, A.L.; Fernandes, J.; Pinto, C.; Correia, A.P.; Santos, E.; Pinto, P.S.; Carneiro, P.; Costa, P.; et al. Proinflammatory and anti-inflammatory cytokines in the CSF of patients with Alzheimer’s disease and their correlation with cognitive decline. Neurobiol. Aging 2019, 76, 125–132. [Google Scholar] [CrossRef]
- Rizo-Téllez, S.A.; Méndez-García, L.A.; Flores-Rebollo, C.; Alba-Flores, F.; Alcántara-Suárez, R.; Manjarrez-Reyna, A.N.; Baltazar-López, N.; Hernández-Guzmán, V.A.; León-Pedroza, J.I.; Zapata-Arenas, R.; et al. The Neutrophil-to-Monocyte Ratio and Lymphocyte-to-Neutrophil Ratio at Admission Predict In-Hospital Mortality in Mexican Patients with Severe SARS-CoV-2 Infection (COVID-19). Microorganisms 2020, 8, 1560. [Google Scholar] [CrossRef]
- Venet, M.; Ribeiro, M.S.; Décembre, E.; Bellomo, A.; Joshi, G.; Nuovo, C.; Villard, M.; Cluet, D.; Perret, M.; Pescamona, R.; et al. Severe COVID-19 patients have impaired plasmacytoid dendritic cell-mediated control of SARS-CoV-2. Nat. Commun. 2023, 14, 694. [Google Scholar] [CrossRef]
- Zhang, S.; Asquith, B.; Szydlo, R.; Tregoning, J.S.; Pollock, K.M. Peripheral T cell lymphopenia in COVID-19: Potential mechanisms and impact. Immunother. Adv. 2021, 1, ltab015. [Google Scholar] [CrossRef]
- Deschler, S.; Kager, J.; Erber, J.; Fricke, L.; Koyumdzhieva, P.; Georgieva, A.; Lahmer, T.; Wiessner, J.R.; Voit, F.; Schneider, J.; et al. Mucosal-Associated Invariant T (MAIT) Cells Are Highly Activated and Functionally Impaired in COVID-19 Patients. Viruses 2021, 13, 241. [Google Scholar] [CrossRef]
- Xue, G.; Jiang, M.; Zhao, R.; Le, A.; Li, J. Elevated frequencies of CD14+HLA-DRlo/neg MDSCs in COVID-19 patients. Aging 2021, 13, 6236–6246. [Google Scholar] [CrossRef]
- Guartazaca-Guerrero, S.; Rodríguez-Morales, J.; Rizo-Téllez, S.A.; Solleiro-Villavicencio, H.; Hernández-Valencia, A.F.; Carrillo-Ruiz, J.D.; Escobedo, G.; Méndez-García, G.E.A.L.A. High Levels of IL-8 and MCP-1 in Cerebrospinal Fluid of COVID-19 Patients with Cerebrovascular Disease. Exp. Neurobiol. 2021, 30, 256–261. [Google Scholar] [CrossRef]
- Rodríguez-Morales, J.; Guartazaca-Guerrero, S.; Rizo-Téllez, S.A.; Viurcos-Sanabria, R.; Barrón, E.V.; Hernán-dez-Valencia, A.F.; Nava, P.; Escobedo, G.; Carrillo-Ruiz, J.D.; Méndez-García, L.A. Blood-brain Barrier Damage is Pivotal for SARS-CoV-2 Infection to the Central Nervous System. Exp. Neurobiol. 2022, 31, 270–276. [Google Scholar] [CrossRef]
- Kuzior, H.; Fiebich, B.L.; Yousif, N.M.; Saliba, S.W.; Ziegler, C.; Nickel, K.; Maier, S.J.; Süß, P.; Runge, K.; Matysik, M.; et al. Increased IL-8 concentrations in the cerebrospinal fluid of patients with unipolar depression. Compr. Psychiatry 2020, 102, 152196. [Google Scholar] [CrossRef]
- Martínez, H.; Escamilla-Ocañas, C.; Camara-Lemarroy, C.; González-Garza, M.; Moreno-Cuevas, J.; Sarreón, M.G. Increased cerebrospinal fluid levels of cytokines monocyte chemoattractant protein-1 (MCP-1) and macrophage inflammatory protein-1β (MIP-1β) in patients with amyotrophic lateral sclerosis. Neurologia 2020, 35, 165–169. [Google Scholar] [CrossRef]
- Guasp, M.; Muñoz-Sánchez, G.; Martínez-Hernández, E.; Santana, D.; Carbayo, Á.; Naranjo, L.; Bolós, U.; Framil, M.; Saiz, A.; Balasa, M.; et al. CSF Biomarkers in COVID-19 Associated Encephalopathy and Encephalitis Predict Long-Term Outcome. Front. Immunol. 2022, 13, 1600. [Google Scholar] [CrossRef]
- Montazersaheb, S.; Khatibi, S.M.H.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Sorbeni, F.G.; Farahzadi, R.; Ghasemnejad, T. COVID-19 infection: An overview on cytokine storm and related interventions. Virol. J. 2022, 19, 92. [Google Scholar] [CrossRef]
- Dekay, J.T.; Emery, I.F.; Rud, J.; Eldridge, A.; Lord, C.; Gagnon, D.J.; May, T.L.; Herrera, V.L.M.; Ruiz-Opazo, N.; Riker, R.R.; et al. DEspRhigh neutrophils are associated with critical illness in COVID-19. Sci. Rep. 2021, 11, 22463. [Google Scholar] [CrossRef]
- De Stricker Borch, J.; Haslund-Vinding, J.; Vilhardt, F.; Maier, A.D.; Mathiesen, T. Meningioma–Brain Crosstalk: A Scoping Review. Cancers 2021, 13, 4267. [Google Scholar] [CrossRef]
- Albulescu, R.; Codrici, E.; Popescu, I.D.; Mihai, S.; Necula, L.G.; Petrescu, D.; Teodoru, M.; Tanase, C.P. Cytokine patterns in brain tumour progression. Mediat. Inflamm. 2013, 2013, 979748. [Google Scholar] [CrossRef]
- Ziai, W.C.; Parry-Jones, A.R.; Thompson, C.B.; Sansing, L.H.; Mullen, M.T.; Murthy, S.B.; Mould, A.; Nekoovaght-Tak, S.; Hanley, D.F. Early inflammatory cytokine expression in cerebrospinal fluid of patients with spontaneous intraventricular hemorrhage. Biomolecules 2021, 11, 1123. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Lukiw, W.J. SARS-CoV-2 Neuroinvasion, Inflammatory Neurodegeneration and Alzheimer’s Disease. Front. Cell. Neurosci. 2022, 16, 322. [Google Scholar] [CrossRef]
- Romagnolo, A.; Balestrino, R.; Imbalzano, G.; Ciccone, G.; Riccardini, F.; Artusi, C.A.; Bozzali, M.; Ferrero, B.; Montalenti, E.; Montanaro, E.; et al. Neurological comorbidity and severity of COVID-19. J. Neurol. 2020, 268, 762–769. [Google Scholar] [CrossRef]
- Jarvis, J.N.; Meintjes, G.; Bicanic, T.; Buffa, V.; Hogan, L.; Mo, S.; Tomlinson, G.; Kropf, P.; Noursadeghi, M.; Harrison, T.S. Cerebrospinal Fluid Cytokine Profiles Predict Risk of Early Mortality and Immune Reconstitution Inflammatory Syndrome in HIV-Associated Cryptococcal Meningitis. PLoS Pathog. 2015, 11, e1004754. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Gender | Age (Years) | Pre-Existing Neurological Disease | Respiratory/Neurological Symptoms Due to COVID-19 | Neurological Symptoms at Arrival to the Hospital | Presence of SARS-CoV-2 Nasopharyngeal/CSF | Deregulated Biochemical Parameters | Immunological Parameters | Cytokine Profile in CSF | ||
|---|---|---|---|---|---|---|---|---|---|---|
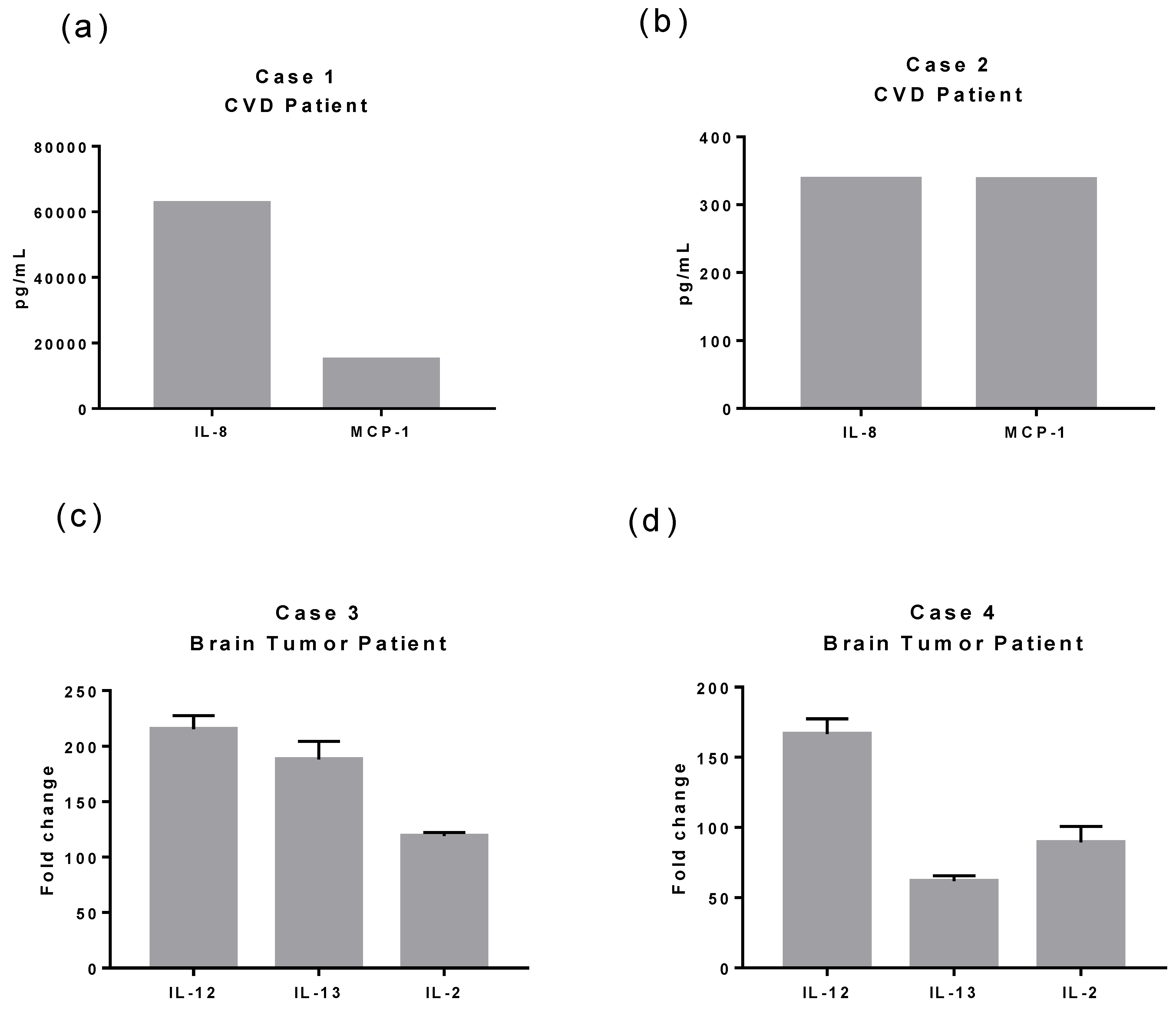
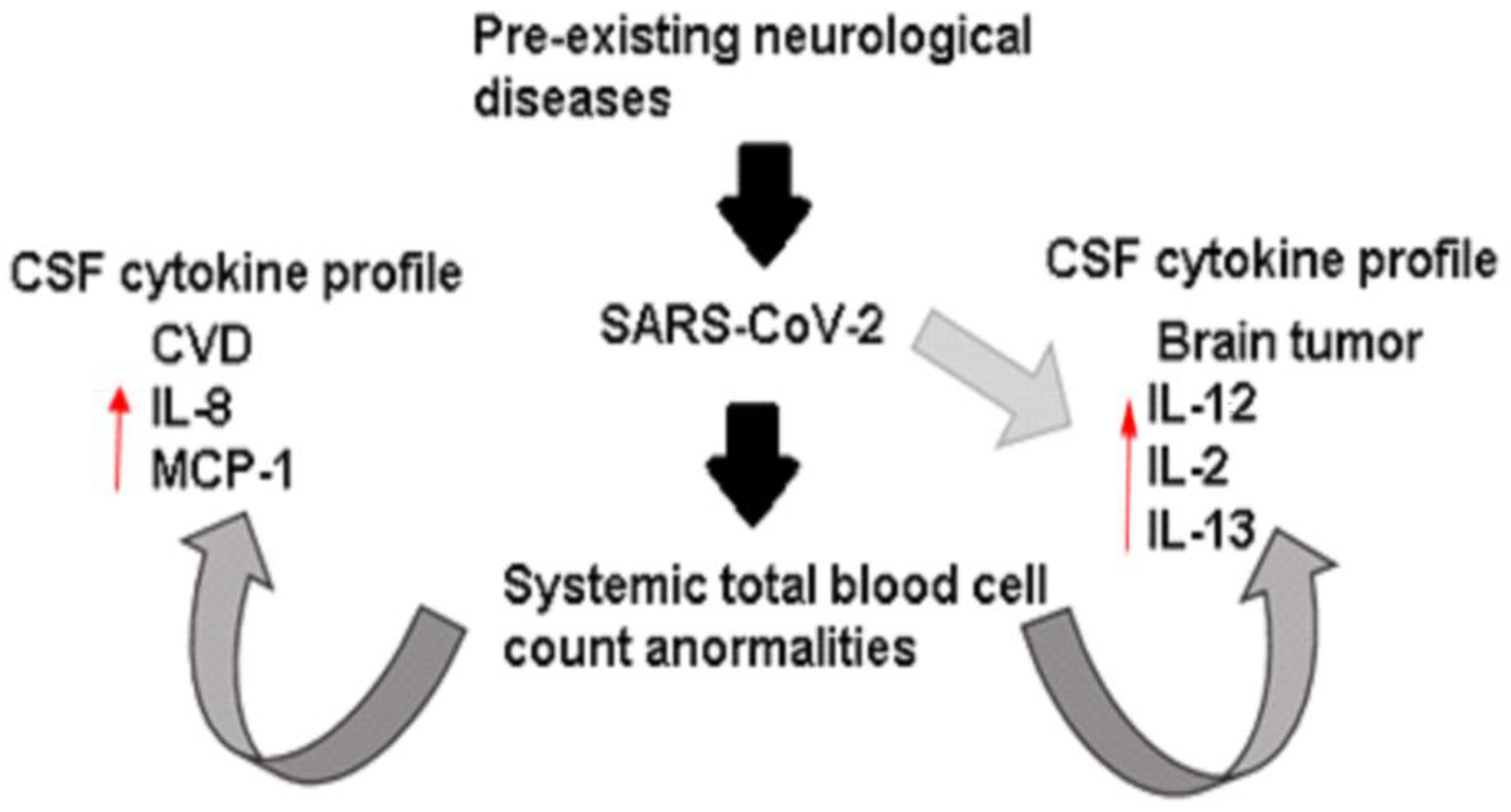
| Case 1 | Female | 54 | CVD (acute intra-axial hemorrhage) | Without symptoms | -Moderate headache -Balance impairment -Weakness -Loss of consciousness | Positive/Negative | Dimer-D (14,760 Ug/L) Glucose (161 mg/dL) Total cholesterol (236 mg/dL) | Leukocytosis (12.10 × 103/mm3) Lymphopenia (0.70 × 103/ mm3) Neutrophilia (11.30 × 103/ mm3) Monocytopenia (0.1 × 103/ mm3) |  | IL-8 MCP-1 IFN-α |
| Case 2 | Male | 45 | CVD (diffuse subarachnoid hemorrhage) | Without symptoms | -Seizure -Psychomotor agitation -Disorientation | Positive/Negative | Dimer-D (4304 Ug/L) Fibrinogen (562 mg/dL) | Leukocytosis (15.70 × 103/ mm3) Lymphopenia (0.90 × 103/ mm3) Neutrophilia (14.20 × 103/ mm3) |  | IL-8 MCP-1 IFN-α |
| Case 3 | Female | 43 | Brain tumor (petroclival meningioma) | Pneumonia | -Severe headache -Drowsiness | Positive/Positive | Triglycerides (372 mg/dL) Glucose (110 mg/dL) ALT (70 U/L) Q-albumin (7.3 × 10−3 g/dL) | Leukocytosis (12.40 × 103/ mm3) Neutrophilia (9.10 × 103/ mm3) Monocytopenia (0.2 × 103/ mm3) |  | IL-12 IL-2 IL-13 |
| Case 4 | Male | 43 | Brain tumor (in the fourth ventricle) | Anosmia Peripheral oxygen saturation of 89% Neurological impairment Pneumonia | -Intense headache -Syncope -Gait abnormalities -Decreased alertness | Positive/Negative | ALT (79 U/L) | Leukocytosis (12.40 × 103/ mm3) Neutrophilia (14.20 × 103/ mm3) Lymphopenia (0.90 × 103/ mm3) Monocytopenia (0.1 × 103/ mm3) |  | IL-12 IL-2 IL-13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Méndez-García, L.A.; Solleiro-Villavicencio, H.; Guartazaca-Guerrero, S.; Rodríguez-Morales, J.; Carrillo-Ruiz, J.D. Neurological Diseases Define the Cytokine Profile in CFS during SARS-CoV-2 Infection in Highly Ill Patients. Trop. Med. Infect. Dis. 2023, 8, 290. https://doi.org/10.3390/tropicalmed8060290
Méndez-García LA, Solleiro-Villavicencio H, Guartazaca-Guerrero S, Rodríguez-Morales J, Carrillo-Ruiz JD. Neurological Diseases Define the Cytokine Profile in CFS during SARS-CoV-2 Infection in Highly Ill Patients. Tropical Medicine and Infectious Disease. 2023; 8(6):290. https://doi.org/10.3390/tropicalmed8060290
Chicago/Turabian StyleMéndez-García, Lucía Angélica, Helena Solleiro-Villavicencio, Sebastián Guartazaca-Guerrero, Jahir Rodríguez-Morales, and José Damián Carrillo-Ruiz. 2023. "Neurological Diseases Define the Cytokine Profile in CFS during SARS-CoV-2 Infection in Highly Ill Patients" Tropical Medicine and Infectious Disease 8, no. 6: 290. https://doi.org/10.3390/tropicalmed8060290