
Drug Resistance Patterns of Commonly Used Antibiotics for the Treatment of Helicobacter pylori Infection among South Asian Countries: A Systematic Review and Meta-Analysis
 , , , , , ,
, , , , , ,  , ,
, ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Search Strategy
2.3. Selection Criteria
2.4. Selection Process
2.5. Definitions
2.6. Data Extraction
2.7. Quality Assessment
2.8. Statistical Analysis
3. Results
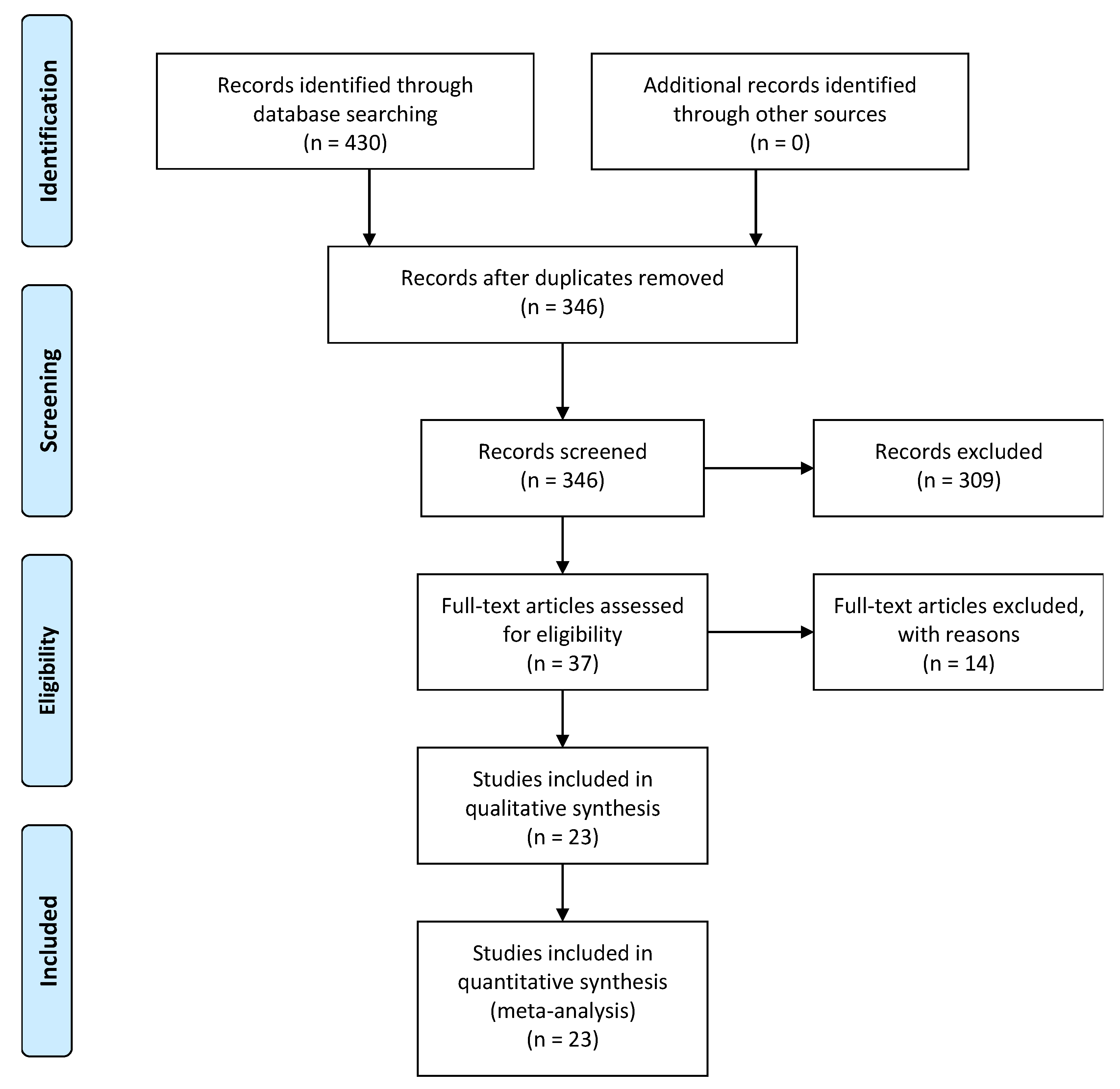
3.1. Study Selection and Characteristics
3.2. Study Quality
3.3. Pooled Prevalence of Helicobacter pylori Resistance
3.4. Subgroup Analysis
3.4.1. Country-Wise Analysis
3.4.2. Analysis of the Trend
3.4.3. Method of Detection of H. pylori and Antibiotic Resistance Detection Method
3.5. Sensitivity Analysis
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kusters Johannes, G.; van Vliet Arnoud, H.M.; Kuipers Ernst, J. Pathogenesis of Helicobacter pylori Infection. Clin. Microbiol. Rev. 2006, 19, 449–490. [Google Scholar] [CrossRef] [Green Version]
- Ernst, P.B.; Gold, B.D. The disease spectrum of Helicobacter pylori: The immunopathogenesis of gastroduodenal ulcer and gastric cancer. Annu. Rev. Microbiol. 2000, 54, 615–640. [Google Scholar] [CrossRef]
- Schistosomes, liver flukes and Helicobacter pylori. IARC Monogr. Eval. Carcinog. Risks Hum. 1994, 61, 1–241.
- Zamani, M.; Ebrahimtabar, F.; Zamani, V.; Miller, W.H.; Alizadeh-Navaei, R.; Shokri-Shirvani, J.; Derakhshan, M.H. Systematic review with meta-analysis: The worldwide prevalence of Helicobacter pylori infection. Aliment. Pharm. 2018, 47, 868–876. [Google Scholar] [CrossRef] [Green Version]
- Group, H.a.C.C. Gastric cancer and Helicobacter pylori: A combined analysis of 12 case control studies nested within prospective cohorts. Gut 2001, 49, 347–353. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.-M.; Schulz, C.; Gasbarrini, A.; Hunt, R.H.; Leja, M.; Morain, C.; et al. Management of Helicobacter pylori infection: The Maastricht VI/Florence consensus report. Gut 2022, 71, 1724. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Choi, D.J.; Chung, J.W. Antibiotic treatment for Helicobacter pylori: Is the end coming? World J. Gastrointest. Pharm. 2015, 6, 183–198. [Google Scholar] [CrossRef] [PubMed]
- Thung, I.; Aramin, H.; Vavinskaya, V.; Gupta, S.; Park, J.Y.; Crowe, S.E.; Valasek, M.A. Review article: The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharm. 2016, 43, 514–533. [Google Scholar] [CrossRef] [Green Version]
- Nyssen, O.P.; McNicholl, A.G.; Megraud, F.; Savarino, V.; Oderda, G.; Fallone, C.A.; Fischbach, L.; Bazzoli, F.; Gisbert, J.P. Sequential versus standard triple first-line therapy for Helicobacter pylori eradication. Cochrane Database Syst. Rev. 2016, 2016, Cd009034. [Google Scholar] [CrossRef] [PubMed]
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Render, C.; Leontiadis, G.I.; Moayyedi, P.; et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology 2016, 151, 51–69.e14. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Kuo, Y.T.; Liou, J.M.; El-Omar, E.M.; Wu, J.Y.; Leow, A.H.R.; Goh, K.L.; Das, R.; Lu, H.; Lin, J.T.; Tu, Y.K.; et al. Primary antibiotic resistance in Helicobacter pylori in the Asia-Pacific region: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Nepal, G.; Bhatta, S. Self-medication with Antibiotics in WHO Southeast Asian Region: A Systematic Review. Cureus 2018, 10, e2428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vagarali, M.A.; Metgud, S.C.; Bannur, H.; Karadesai, S.G.; Nagmoti, J.M. Clinical significance of various diagnostic techniques and emerging antimicrobial resistance pattern of Helicobacter Pylori from Gastric Biopsy Samples. Indian J. Med. Microbiol. 2015, 33, 560–564. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, T.R.; Ahmed, W.; Arif, A.; Bibi, S.; Khan, A. Emerging trends of antimicrobial resistance in Helicobacter pylori isolates obtained from Pakistani patients: The need for consideration of amoxicillin and clarithromycin. J. Pak. Med. Assoc. 2016, 66, 710–716. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ Br. Med. J. 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 January 2023).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Mahant, S.; Sharma, A.K.; Gehlot, V.; Mukhopadhyay, A.K.; Chhawchharia, A.; Dutta, S.; Agarwal, A.; Som, A.; Das, K.; Das, R. Geographically distinct North-East Indian Helicobacter pylori strains are highly sensitive to clarithromycin but are levofloxacin resistant. Indian J. Med. Microbiol. 2019, 37, 337–344. [Google Scholar] [CrossRef]
- Pandya, H.B.; Agravat, H.H.; Patel, J.S.; Sodagar, N.R. Emerging antimicrobial resistance pattern of Helicobacter pylori in central Gujarat. Indian J. Med. Microbiol. 2014, 32, 408–413. [Google Scholar] [CrossRef]
- Aftab, H.; Miftahussurur, M.; Subsomwong, P.; Ahmed, F.; Khan, A.K.; Yamaoka, Y. Helicobacter pylori antibiotic susceptibility patterns in Bangladesh: Emerging levofloxacin resistance. J. Infect. Dev. Ctries 2016, 10, 245–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mujtaba, A.; Masud, T.; Ahmad, A.; Naqvi, S.M.S.; Ismail, A.; Tahir, M.I.; Yousaf, A.A.; Ibrahim, M.S. Isolation and antimicrobial susceptibility testing of Helicobacter pylori strains from gastric biopsies from Pakistani patients. Pak. J. Pharm. Sci. 2019, 32, 2279–2285. [Google Scholar]
- Khan, A.; Farooqui, A.; Manzoor, H.; Akhtar, S.S.; Quraishy, M.S.; Kazmi, S.U. Antibiotic resistance and cagA gene correlation: A looming crisis of Helicobacter pylori. World J. Gastroe.Enterol. 2012, 18, 2245–2252. [Google Scholar] [CrossRef] [PubMed]
- Gehlot, V.; Mahant, S.; Mukhopadhyay, A.K.; Das, K.; De, R.; Kar, P.; Das, R. Antimicrobial susceptibility profiles of Helicobacter pylori isolated from patients in North India. J. Glob. Antimicrob. Resist. 2016, 5, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Miftahussurur, M.; Aftab, H.; Shrestha, P.K.; Sharma, R.P.; Subsomwong, P.; Waskito, L.A.; Doohan, D.; Fauzia, K.A.; Yamaoka, Y. Effective therapeutic regimens in two South Asian countries with high resistance to major Helicobacter pylori antibiotics. Antimicrob. Resist. Infect. Control 2019, 8, 40. [Google Scholar] [CrossRef] [Green Version]
- Malhotra, Y.; Khare, R.L.; Varma, S.; Toppo, A. Assessment of pattern of antimicrobial resistance of Helicobacter pylori in patients of dyspepsia of rural area. J. Evol. Med. Dent. Sci. 2015, 4, 10849. [Google Scholar] [CrossRef]
- Anis, S.; Farooqi, S.R.; Niaz, S.K. Characterization of Domain V Mutations in Clinical Isolates of Helicobacter pylori in Pakistan and Their Effect on Clarithromycin MIC. Infect. Drug Resist. 2021, 14, 3393–3403. [Google Scholar] [CrossRef]
- Datta, S.; Chattopadhyay, S.; Patra, R.; De, R.; Ramamurthy, T.; Hembram, J.; Chowdhury, A.; Bhattacharya, S.K.; Berg, D.E.; Nair, G.B.; et al. Most Helicobacter pylori strains of Kolkata in India are resistant to metronidazole but susceptible to other drugs commonly used for eradication and ulcer therapy. Aliment. Pharm. 2005, 22, 51–57. [Google Scholar] [CrossRef]
- Nahar, S.; Mukhopadhyay, A.K.; Khan, R.; Ahmad, M.M.; Datta, S.; Chattopadhyay, S.; Dhar, S.C.; Sarker, S.A.; Engstrand, L.; Berg, D.E.; et al. Antimicrobial susceptibility of Helicobacter pylori strains isolated in Bangladesh. J. Clin. Microbiol. 2004, 42, 4856–4858. [Google Scholar] [CrossRef] [Green Version]
- Hallur, V.; Panigrahi, M.; Sable, M.; Ghosh, M.; Mohanty, S.; Purkait, S.; Praharaj, A. Low clarithromycin resistance in virulent Helicobacter pylori from dyspeptic patients at a tertiary care centre in Odisha. Indian J. Med. Microbiol. 2022, 40, 211–216. [Google Scholar] [CrossRef]
- Rajper, S.; Khan, E.; Ahmad, Z.; Alam, S.M.; Akbar, A.; Hasan, R. Macrolide and fluoroquinolone resistance in Helicobacter pylori isolates: An experience at a tertiary care centre in Pakistan. J. Pak. Med. Assoc. 2012, 62, 1140–1144. [Google Scholar] [PubMed]
- Rasheed, F.; Campbell, B.J.; Alfizah, H.; Varro, A.; Zahra, R.; Yamaoka, Y.; Pritchard, D.M. Analysis of clinical isolates of Helicobacter pylori in Pakistan reveals high degrees of pathogenicity and high frequencies of antibiotic resistance. Helicobacter 2014, 19, 387–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shetty, V.; Lamichhane, B.; Tay, C.Y.; Pai, G.C.; Lingadakai, R.; Balaraju, G.; Shetty, S.; Ballal, M.; Chua, E.G. High primary resistance to metronidazole and levofloxacin, and a moderate resistance to clarithromycin in Helicobacter pylori isolated from Karnataka patients. Gut Pathog. 2019, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Varsha, S.; Shrutkirti, M.; Pushpa, M.; Rao, G.R.; Ashok Kumar, J.; Vinod Kumar, D.; Anil Kumar, G.; Gopal, N. Drug resistance pattern and clonality in H. pylori strains. J. Infect. Dev. Ctries. 2009, 3, 130–136. [Google Scholar] [CrossRef] [Green Version]
- Thyagarajan, S.P.; Ray, P.; Das, B.K.; Ayyagari, A.; Khan, A.A.; Dharmalingam, S.; Rao, U.A.; Rajasambandam, P.; Ramathilagam, B.; Bhasin, D.; et al. Geographical difference in antimicrobial resistance pattern of Helicobacter pylori clinical isolates from Indian patients: Multicentric study. J. Gastroenterol. Hepatol. 2003, 18, 1373–1378. [Google Scholar] [CrossRef]
- Vilaichone, R.K.; Yamaoka, Y.; Shiota, S.; Ratanachu-ek, T.; Tshering, L.; Uchida, T.; Fujioka, T.; Mahachai, V. Antibiotics resistance rate of Helicobacter pylori in Bhutan. World J. Gastroenterol. 2013, 19, 5508–5512. [Google Scholar] [CrossRef]
- Vilaichone, R.-k.; Aumpan, N.; Ratanachu-ek, T.; Uchida, T.; Tshering, L.; Mahachai, V.; Yamaoka, Y. Population-based study of Helicobacter pylori infection and antibiotic resistance in Bhutan. Int. J. Infect. Dis. 2020, 97, 102–107. [Google Scholar] [CrossRef]
- Wani, F.A.; Bashir, G.; Khan, M.A.; Zargar, S.A.; Rasool, Z.; Qadri, Q. Antibiotic resistance in Helicobacter pylori: A mutational analysis from a tertiary care hospital in Kashmir, India. Indian J. Med. Microbiol. 2018, 36, 265–272. [Google Scholar] [CrossRef]
- Yakoob, J.; Abbas, Z.; Jafri, W.; Usman, M.W.; Jafri, F.; Awan, S. Comparison of the virulence markers of Helicobacter pylori and their associated diseases in patients from Pakistan and Afghanistan. Saudi J. Gastroenterol. 2013, 19, 211–218. [Google Scholar] [CrossRef]
- Spellberg, B.; Gilbert, D.N. The future of antibiotics and resistance: A tribute to a career of leadership by John Bartlett. Clin. Infect. Dis. 2014, 59 (Suppl. S2), S71–S75. [Google Scholar] [CrossRef] [Green Version]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382.e1317. [Google Scholar] [CrossRef] [Green Version]
- Kasahun, G.G.; Demoz, G.T.; Desta, D.M. Primary Resistance Pattern of Helicobacter pylori to Antibiotics in Adult Population: A Systematic Review. Infect. Drug Resist. 2020, 13, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- UNICEF. Water, Sanitation And Hygiene (WASH). Available online: https://www.unicef.org/rosa/water-sanitation-and-hygiene-wash (accessed on 12 January 2023).
- Shankar, P.R.; Partha, P.; Shenoy, N. Self-medication and non-doctor prescription practices in Pokhara valley, Western Nepal: A questionnaire-based study. BMC Fam. Pract. 2002, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Wijesinghe, P.; Jayakody, R.; de A Seneviratne, R. Prevalence and predictors of self-medication in a selected urban and rural district of Sri Lanka. WHO South.-East. Asia J. Public Health 2012, 1, 28–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zafar, S.N.; Syed, R.; Waqar, S.; Zubairi, A.J.; Vaqar, T.; Shaikh, M.; Yousaf, W.; Shahid, S.; Saleem, S. Self-medication amongst university students of Karachi: Prevalence, knowledge and attitudes. J. Pak. Med. Assoc. 2008, 58, 214–217. [Google Scholar]
- Chereau, F.; Opatowski, L.; Tourdjman, M.; Vong, S. Risk assessment for antibiotic resistance in South East Asia. BMJ 2017, 358, j3393. [Google Scholar] [CrossRef] [Green Version]
- Sukri, A.; Lopes, B.S.; Hanafiah, A. The Emergence of Multidrug-Resistant Helicobacter pylori in Southeast Asia: A Systematic Review on the Trends and Intervention Strategies Using Antimicrobial Peptides. Antibiotics 2021, 10, 1061. [Google Scholar] [CrossRef]
- Mahachai, V.; Vilaichone, R.K.; Pittayanon, R.; Rojborwonwitaya, J.; Leelakusolvong, S.; Maneerattanaporn, M.; Chotivitayatarakorn, P.; Treeprasertsuk, S.; Kositchaiwat, C.; Pisespongsa, P.; et al. Helicobacter pylori management in ASEAN: The Bangkok consensus report. J. Gastroenterol. Hepatol. 2018, 33, 37–56. [Google Scholar] [CrossRef] [Green Version]
- Levy, S.B. The 2000 Garrod lecture. Factors impacting on the problem of antibiotic resistance. J. Antimicrob. Chemother. 2002, 49, 25–30. [Google Scholar] [CrossRef]
- Xia, H.X.; Fan, X.G.; Talley, N.J. Clarithromycin resistance in Helicobacter pylori and its clinical relevance. World J. Gastroenterol. 1999, 5, 263–266. [Google Scholar] [CrossRef]
- Kaneko, F.; Suzuki, H.; Hasegawa, N.; Kurabayshi, K.; Saito, H.; Otani, S.; Nakamizo, H.; Kawata, K.; Miyairi, M.; Ishii, K.; et al. High prevalence rate of Helicobacter pylori resistance to clarithromycin during long-term multiple antibiotic therapy for chronic respiratory disease caused by non-tuberculous mycobacteria. Aliment. Pharmacol. Ther. 2004, 20, 62–67. [Google Scholar] [CrossRef]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [Green Version]
- Bilal, H.; Khan, M.N.; Rehman, T.; Hameed, M.F.; Yang, X. Antibiotic resistance in Pakistan: A systematic review of past decade. BMC Infect. Dis. 2021, 21, 244. [Google Scholar] [CrossRef] [PubMed]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfell, B.T.; Levin, S.A.; Laxminarayan, R. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect. Dis 2014, 14, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Niederman, M.S. Review of treatment guidelines for community-acquired pneumonia. Am. J. Med. 2004, 117 (Suppl. S3A), 51s–57s. [Google Scholar] [CrossRef]
- Ansari, S.; Yamaoka, Y. Helicobacter pylori Virulence Factor Cytotoxin-Associated Gene A (CagA)-Mediated Gastric Pathogenicity. Int. J. Mol. Sci. 2020, 21, 7430. [Google Scholar] [CrossRef]
- Pormohammad, A.; Mohtavinejad, N.; Gholizadeh, P.; Dabiri, H.; Salimi Chirani, A.; Hashemi, A.; Nasiri, M.J. Global estimate of gastric cancer in Helicobacter pylori-infected population: A systematic review and meta-analysis. J. Cell Physiol. 2019, 234, 1208–1218. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [Green Version]
- Rahman, R.; Asombang, A.W.; Ibdah, J.A. Characteristics of gastric cancer in Asia. World J. Gastroenterol. 2014, 20, 4483–4490. [Google Scholar] [CrossRef]
- Rolfe, R.; Kwobah, C.; Muro, F.; Ruwanpathirana, A.; Lyamuya, F.; Bodinayake, C.; Nagahawatte, A.; Piyasiri, B.; Sheng, T.; Bollinger, J.; et al. Barriers to implementing antimicrobial stewardship programs in three low- and middle-income country tertiary care settings: Findings from a multi-site qualitative study. Antimicrob. Resist. Infect. Control 2021, 10, 60. [Google Scholar] [CrossRef] [PubMed]
- Kiyotoki, S.; Nishikawa, J.; Sakaida, I. Efficacy of Vonoprazan for Helicobacter pylori Eradication. Intern. Med. 2020, 59, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rike, S.; Dayu Swasti, K.; Rayhana. Helicobacter pylori Challenge Vaccine for Humans. In Vaccine Development; Yulia, D., Ed.; IntechOpen: Rijeka, Croatia, 2021; Chapter 5. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S.N. | Author | Year | Country | Male | Female | Age in yrs. | Method of H. pylori Detection | Method of Antibiotic Susceptibility Detection | Sample for H. pylori Resistance |
|---|---|---|---|---|---|---|---|---|---|
| 1. | Pandya et al. [21] | 2014 | India | 518 | 337 | 10–90 | Culture | Disk diffusion | 80 |
| 2. | Aftab et al. [22] | 2016 | Bangladesh | 26 § | 30 | 35.2 ± 11.8 | Culture | Agar dilution | 56 |
| 3. | Mujtaba et al. [23] | 2019 | Pakistan | 24 § | 16 | 35–55 | Culture | E-test | 40 |
| 4. | Khan et al. [24] | 2012 | Pakistan | NA | NA | NA | Culture, PCR | PCR | 201 |
| 5. | Gehlot et al. [25] | 2015 | India | 36 § | 32 | 18–86 | Culture | Agar dilution | 68 |
| 6. | Miftahussurer et al. † [26] | 2019 | Nepal | NA | NA | NA | Culture | Agar dilution | 42 |
| 7. | Miftahussurer et al. † [26] | 2019 | Bangladesh | NA | NA | NA | Culture | Agar dilution | 36 |
| 8. | Mahant et al. [20] | 2020 | India | 32 § | 14 | 18–80 | Culture | Agar diffusion, PCR | 46 |
| 9. | Malhotra et al. [27] | 2015 | India | 39 | 11 | 15–50 | Culture | Disk diffusion | 40 |
| 10. | Anis et al. [28] | 2021 | Pakistan | NA | NA | NA | Culture, rapid urease test | Agar dilution | 48 |
| 11. | Datta et al. [29] | 2005 | India | 72 | 31 | 21–71 | Culture | Agar dilution | 67 |
| 12. | Nahar et al. [30] | 2004 | Bangladesh | 202 | 76 | 15–78 | Culture | Agar dilution | 120 |
| 13. | Hallur et al. [31] | 2022 | India | 85 | 28 | 46.85 ± 13.2 | Culture, PCR | E-test | 32 |
| 14. | Rajper et al. [32] | 2012 | Pakistan | 84 § | 78 | 9–75 | H&E | PCR | 162 |
| 15. | Rasheed et al. [33] | 2014 | Pakistan | 71 | 22 | 46 ± 16.4 for males 49.1 ± 15.1 for females | H&E | PCR | 46 |
| 16. | Shetty et al. [34] | 2019 | India | 80 § | 33 | 46.2 ± 14 | H&E | PCR | 113 |
| 17. | Siddiqui et al. [15] | 2016 | Pakistan | 424 | 465 | 35.6 ± 14.32 | Gram staining and urease test | Disk diffusion | 93 |
| 18. | Singh et al. [35] | 2009 | India | 68 | 40 | 18–75 | Gram staining and urease test and PCR | Agar dilution and E-test method | 63 |
| 19. | Thyagarajan et al. [36] | 2003 | India | NA | NA | NA | H&E and urease, catalase test | Disk diffusion, and E-test | 259 |
| 20. | Vagarali et al. [14] | 2015 | India | 152 | 48 | NA | Culture, H&E, and urease test | Disk diffusion | 5 |
| 21. | Vilaichone et al. [37] | 2013 | Bhutan | 51 § | 60 | 36.8 ± 13.9 | Culture | E-test | 111 |
| 22. | Vilaichone et al. [38] | 2020 | Bhutan | 514 | 664 | 41.5 ± 15.2 | Histopathology, urease, and culture | E-test | 357 |
| 23. | Wani et al. [39] | 2018 | India | 54 | 41 | 46.78 | Histopathology, urease, and culture | PCR | 60 |
| 24. | Yakoob et al. [40] | 2013 | Pakistan | 80 | 40 | 41 ± 13 | Histopathology, urease, C14 urea breath test, and culture | E-test | 47 |
| A. Amoxicillin (Pooled prevalence: 23%) | |
| Bangladesh | 5% (95%CI: 0.02–0.09); p = 0.36 |
| India | 29% (95%CI: 0.15–0.44); p < 0.001 |
| Pakistan | 30% (95%CI: −0.21–0.81); p < 0.001 |
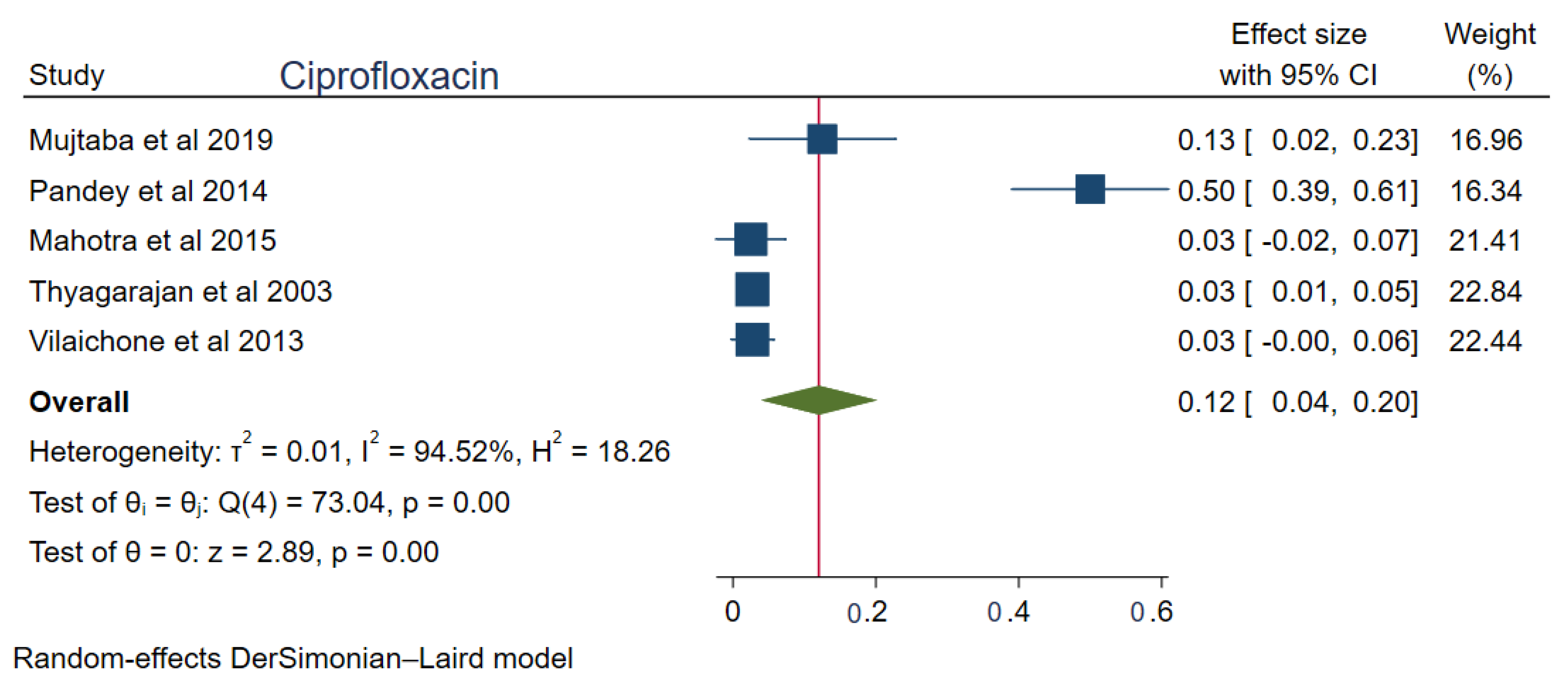
| B. Ciprofloxacin (Pooled prevalence: 12%) | |
| Bhutan | 3% (95%CI: 0.00–0.06); p < 0.001 |
| India | 17% (95%CI: 0.01–0.34); p < 0.001 |
| Pakistan | 13% (95%CI: 0.02–0.23); p < 0.001 |
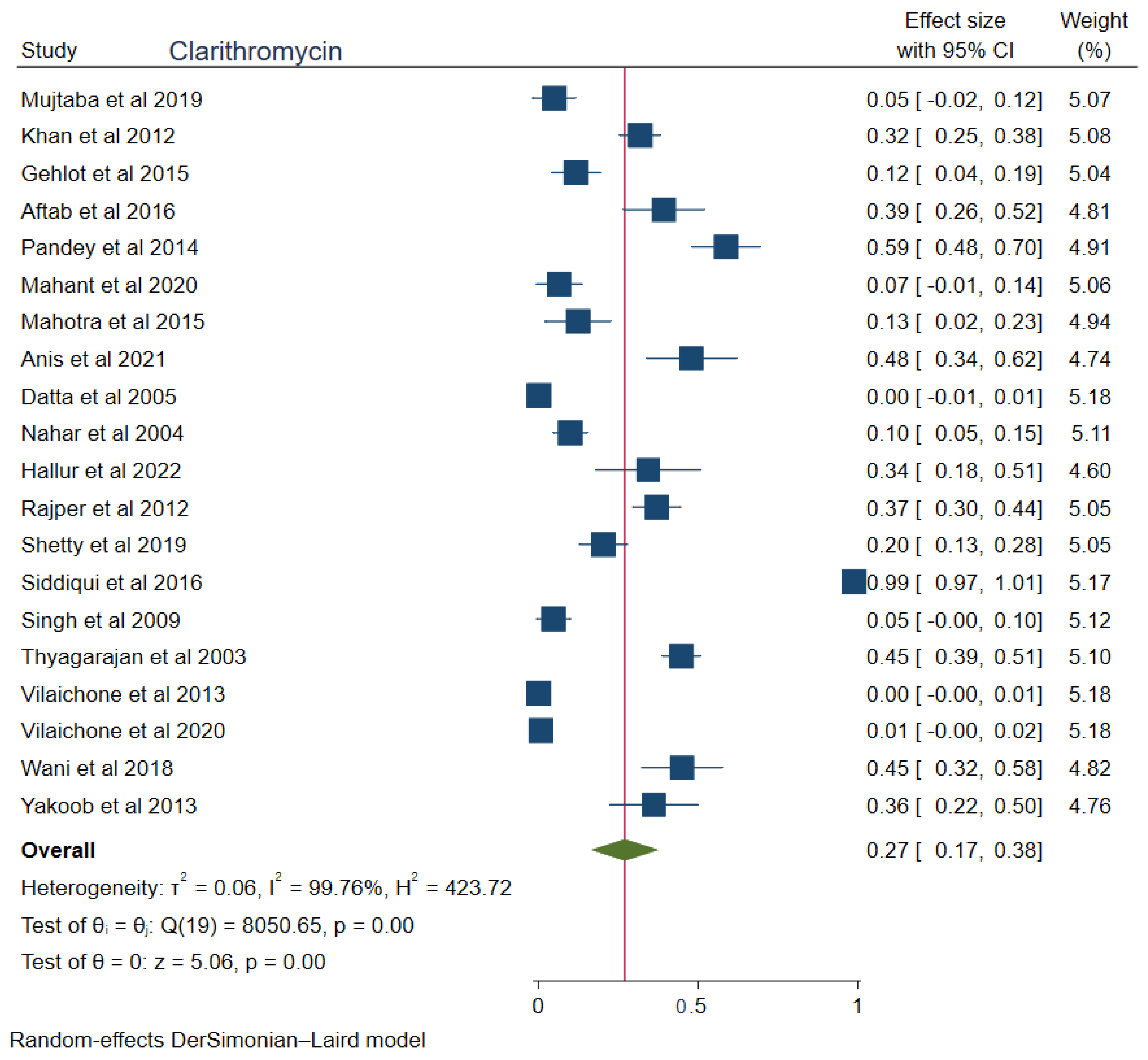
| C. Clarithromycin (Pooled prevalence: 27%) | |
| Bangladesh | 24% (95%CI: 0.05–0.53); p < 0.001 |
| India | 23% (95%CI: 0.11–0.36); p < 0.001 |
| Pakistan | 43% (0.03–0.82); p < 0.001 |
| D. Metronidazole (Pooled prevalence: 69%) | |
| Bangladesh | 63% (95%CI: 0.26–1.00); p < 0.001 |
| Bhutan | 81% (95%CI: 0.78–0.85); p = 0.64 |
| India | 80% ((95%CI: 0.7–0.9); p < 0.001 |
| Nepal | 21% (95%CI: 0.09–0.34); p < 0.001 |
| Pakistan | 49% (95%CI: 0.03–0.94); p < 0.001 |
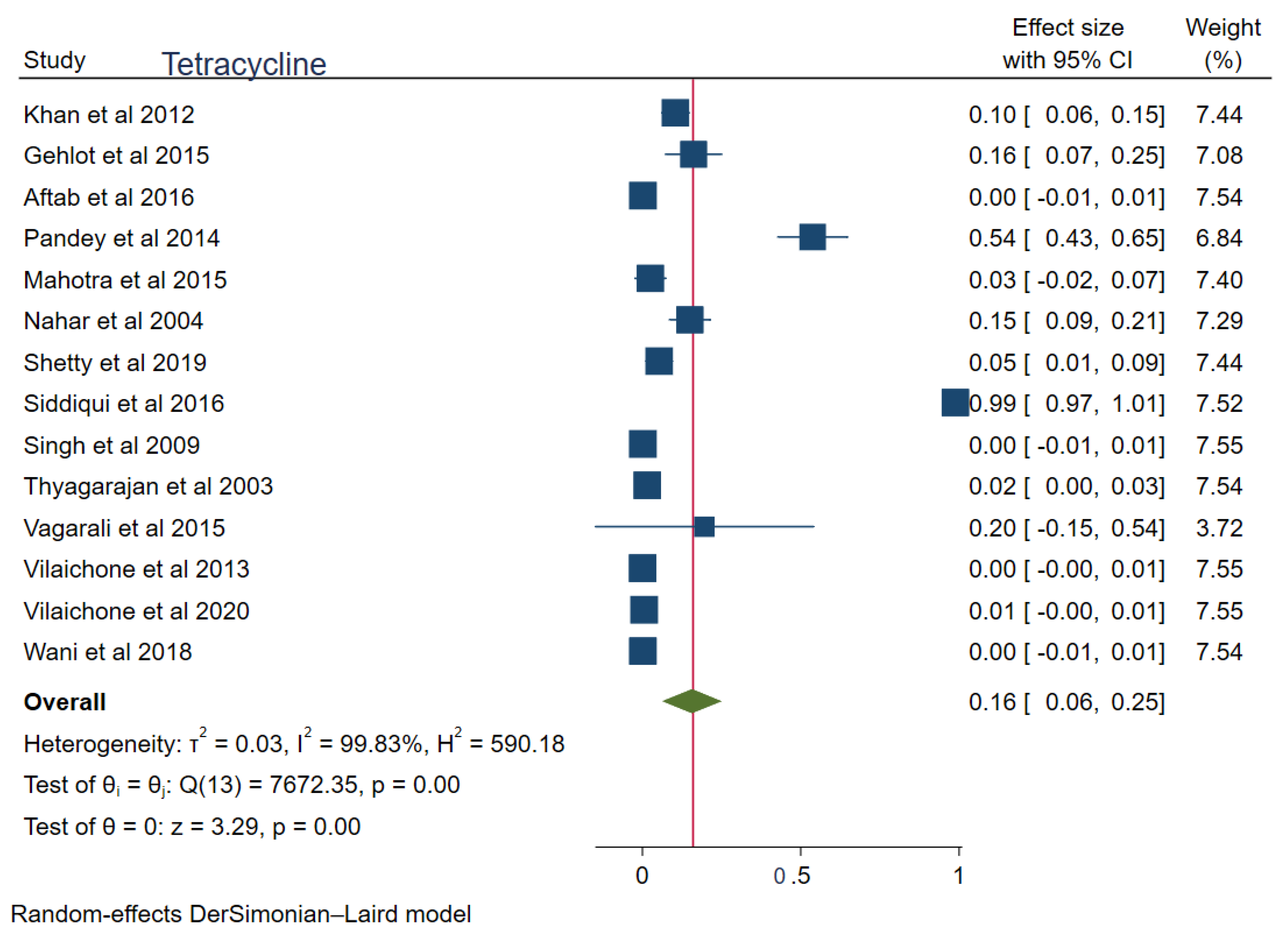
| E. Tetracycline (Pooled prevalence: 16%) | |
| Bangladesh | 7% (95%CI: –0.07–0.22); p < 0.001 |
| India | 7% (95%CI: 0.03–0.10); p < 0.001 |
| Pakistan | 55% (95%CI: –0.32–1.41); p < 0.001 |
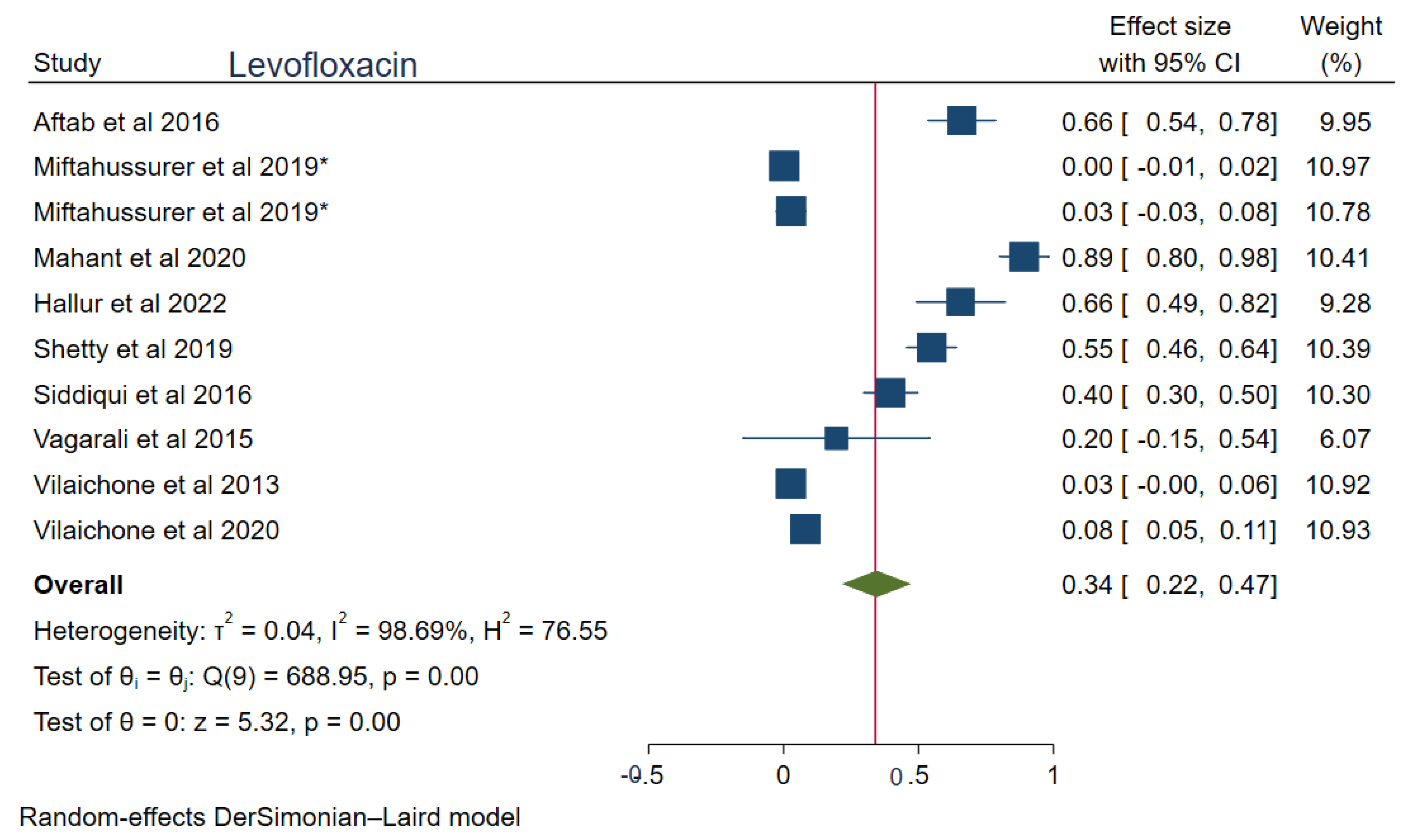
| F. Levofloxacin (Pooled prevalence: 34%) | |
| Bangladesh | 34% (95%CI: –0.28–0.96); p < 0.001 |
| Bhutan | 5% (95%CI: 0.00–0.11); p = 0.01 |
| India | 61% (95%CI: 0.38–0.84); p < 0.001 |
| Pakistan | 40% (95%CI: 0.30–0.50); p < 0.001 |
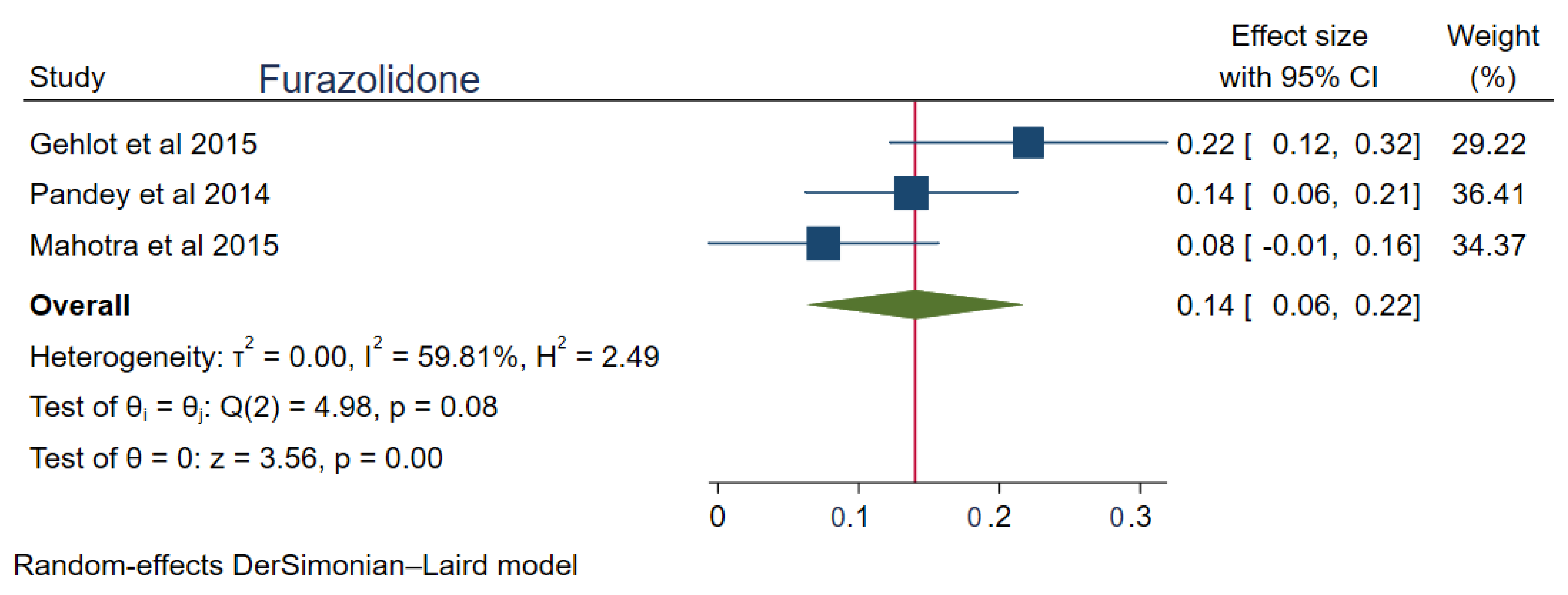
| G. Furazolidone (Pooled prevalence: 14%) | |
| India | 14% (95%CI: 0.06–0.22); p < 0.001 |
| Antibiotic | 2003–2012 (95%CI) | 2013–2022 (95%CI) | p-Value |
|---|---|---|---|
| Ciprofloxacin | 3% (0.01–0.05) | 16% (0.02–0.30) | 0.28 |
| Clarithromycin | 21% (0.06–0.37) | 30% (0.14–0.46) | 0.25 |
| Tetracycline | 5% (0.02–0.09) | 20% (0.07–0.27) | 0.04 |
| Metronidazole | 83% (0.69–0.97) | 63% (0.48–0.78) | 0.82 |
| Amoxicillin | 26% (0.09–0.44) | 22% (0.12–0.32) | 0.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shrestha, A.B.; Pokharel, P.; Sapkota, U.H.; Shrestha, S.; Mohamed, S.A.; Khanal, S.; Jha, S.K.; Mohanty, A.; Padhi, B.K.; Asija, A.; et al. Drug Resistance Patterns of Commonly Used Antibiotics for the Treatment of Helicobacter pylori Infection among South Asian Countries: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2023, 8, 172. https://doi.org/10.3390/tropicalmed8030172
Shrestha AB, Pokharel P, Sapkota UH, Shrestha S, Mohamed SA, Khanal S, Jha SK, Mohanty A, Padhi BK, Asija A, et al. Drug Resistance Patterns of Commonly Used Antibiotics for the Treatment of Helicobacter pylori Infection among South Asian Countries: A Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease. 2023; 8(3):172. https://doi.org/10.3390/tropicalmed8030172
Chicago/Turabian StyleShrestha, Abhigan Babu, Pashupati Pokharel, Unnat Hamal Sapkota, Sajina Shrestha, Shueb A. Mohamed, Surakshya Khanal, Saroj Kumar Jha, Aroop Mohanty, Bijaya Kumar Padhi, Ankush Asija, and et al. 2023. "Drug Resistance Patterns of Commonly Used Antibiotics for the Treatment of Helicobacter pylori Infection among South Asian Countries: A Systematic Review and Meta-Analysis" Tropical Medicine and Infectious Disease 8, no. 3: 172. https://doi.org/10.3390/tropicalmed8030172