
Clinical Implications for the Comprehensive Interpretation of Radiologic and Immunodiagnostic Tests in Patients Suspected of Parasitic Hepatic Cyst, a Rare Case in Korea

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Muralidharan, P.; Raj, J.P. An updated review of cystic hepatic lesions. Clin. Exp. Hepatol. 2019, 5, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Feasey, N.; Wansbrough-Jones, M.; Mabey, D.C.; Solomon, A.W. Neglected tropical diseases. Br. Med. Bull. 2010, 93, 179–200. [Google Scholar] [CrossRef] [PubMed]
- Budke, C.M.; White, A.C., Jr.; Garcia, H.H. Zoonotic larval cestode infections: Neglected, neglected tropical diseases? PLoS Negl. Trop. Dis. 2009, 3, e319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giri, S.; Parija, S.C. A review on diagnostic and preventive aspects of cystic echinococcosis and human cysticercosis. Trop. Parasitol. 2012, 2, 99–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, H.H.; Castillo, Y.; Gonzales, I.; Bustos, J.A.; Saavedra, H.; Jacob, L.; Del Brutto, O.H.; Wilkins, P.P.; Gonzalez, A.E.; Gilman, R.H.; et al. Low sensitivity and frequent cross-reactions in commercially available antibody detection ELISA assays for Taenia solium cysticercosis. Trop. Med. Int. Health TM IH 2018, 23, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Hotez, P.J. Neglected Infections of Poverty among the Indigenous Peoples of the Arctic. PLoS Negl. Trop. Dis. 2010, 4, e606. [Google Scholar] [CrossRef] [Green Version]
- Wen, H.; Yang, W.G. Public health importance of cystic echinococcosis in China. Acta Trop. 1997, 67, 133–145. [Google Scholar] [CrossRef]
- Sadjjadi, S.M. Present situation of echinococcosis in the Middle East and Arabic North Africa. Parasitol. Int. 2006, 55, S197–S202. [Google Scholar] [CrossRef]
- Torgerson, P.R.; Oguljahan, B.; Muminov, A.E.; Karaeva, R.R.; Kuttubaev, O.T.; Aminjanov, M.; Shaikenov, B. Present situation of cystic echinococcosis in Central Asia. Parasitol. Int. 2006, 55, S207–S212. [Google Scholar] [CrossRef]
- Colpani, A.; Achilova, O.; D’Alessandro, G.L.; Budke, C.M.; Mariconti, M.; Muratov, T.; Vola, A.; Mamedov, A.; Giordani, M.T.; Urukov, X.; et al. Trends in the Surgical Incidence of Cystic Echinococcosis in Uzbekistan from 2011 to 2018. Am. J. Trop. Med. Hyg. 2021, 106, 724–728. [Google Scholar] [CrossRef]
- Shin, D.H.; Jo, H.C.; Kim, J.-H.; Jun, K.I.; Park, W.B.; Kim, N.-J.; Choi, M.-H.; Kang, C.K.; Oh, M.-D. An Imported Case of Disseminated Echinococcosis in Korea. Korean J. Parasitol. 2019, 57, 429–434. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.C.; Shin, J.U.; Jin, S.S. Hepatic Hydatid Cyst: A Case Report. Korean J. Gastroenterol. 2021, 77, 35–38. [Google Scholar] [CrossRef]
- Eckert, J.; Deplazes, P. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin. Microbiol. Rev. 2004, 17, 107–135. [Google Scholar] [CrossRef] [Green Version]
- Craig, P.S.; McManus, D.P.; Lightowlers, M.W.; Chabalgoity, J.A.; Garcia, H.H.; Gavidia, C.M.; Gilman, R.H.; Gonzalez, A.E.; Lorca, M.; Naquira, C.; et al. Prevention and control of cystic echinococcosis. Lancet Infect. Dis. 2007, 7, 385–394. [Google Scholar] [CrossRef]
- Wen, H.; Vuitton, L.; Tuxun, T.; Li, J.; Vuitton, D.A.; Zhang, W.; McManus, D.P. Echinococcosis: Advances in the 21st Century. Clin. Microbiol. Rev. 2019, 32, e00075-18. [Google Scholar] [CrossRef] [Green Version]
- Mandal, S.; Deb Mandal, M. Human cystic echinococcosis: Epidemiologic, zoonotic, clinical, diagnostic and therapeutic aspects. Asian Pac. J. Trop. Med. 2012, 5, 253–260. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, D.J.; Romig, T.; Thompson, R.C. Emergence/re-emergence of Echinococcus spp.--a global update. Int. J. Parasitol. 2005, 35, 1205–1219. [Google Scholar] [CrossRef]
- Rogan, M.T.; Hai, W.Y.; Richardson, R.; Zeyhle, E.; Craig, P.S. Hydatid cysts: Does every picture tell a story? Trends Parasitol. 2006, 22, 431–438. [Google Scholar] [CrossRef]
- Kang, M.K.; Kim, K.H.; Choi, J.H. Hepatic cystic echinococcosis due to Echinococcus granulosus, grossly observed by needle aspiration. Korean J. Intern. Med. 2019, 34, 1394–1395. [Google Scholar] [CrossRef] [Green Version]
- Chaudhary, V.; Bano, S.; Kumar, P.; Narula, M.K.; Anand, R. Hepatic cysticercosis: A rare entity. Abdom. Imaging 2014, 39, 1182–1185. [Google Scholar] [CrossRef]
- Singh, N.; Singh, D.K.; Parihar, A.; Singh, R. Disseminated cysticercosis: Rare manifestation of a common disease. BMJ Case Reports 2012, 2012, bcr2012007876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
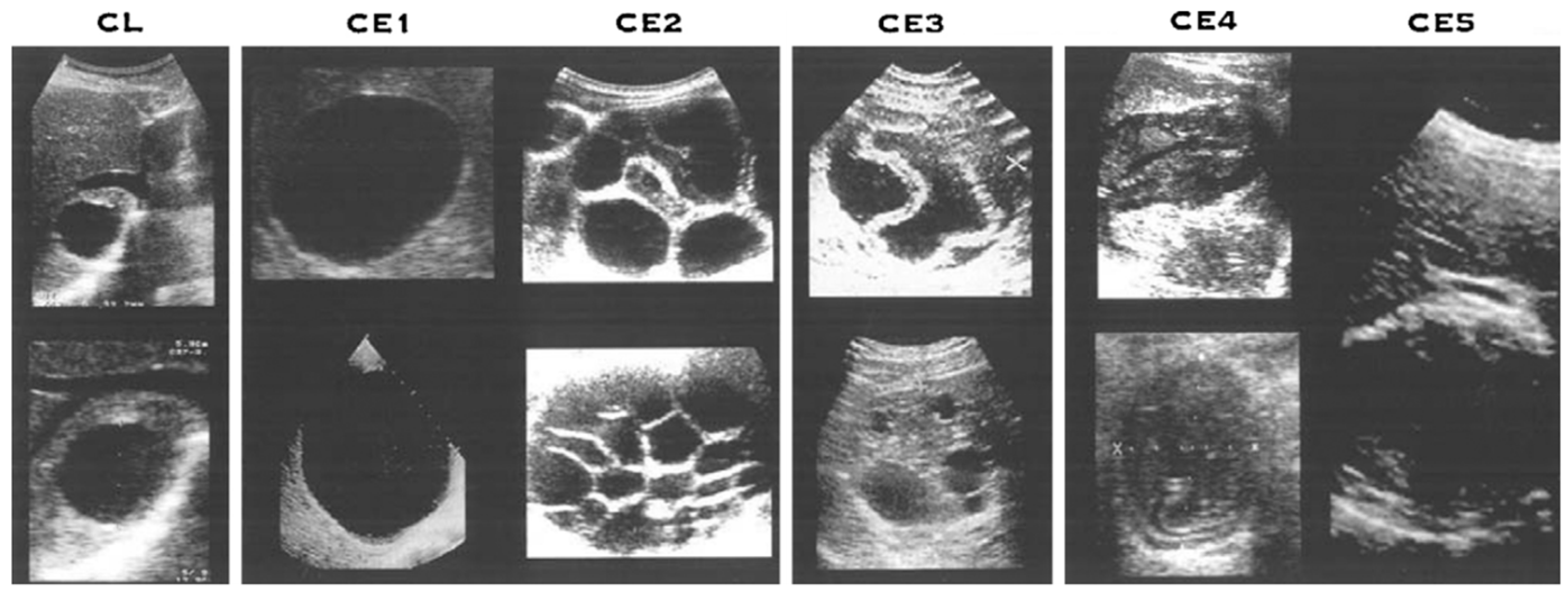
- WHO Informal Working Group. International classification of ultrasound images in cystic echinococcosis for application in clinical and field epidemiological settings. Acta Trop. 2003, 85, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Brunetti, E.; Kern, P.; Vuitton, D.A. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop 2010, 114, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, B.; Abbara, A.; Kadaba, R.; Sheth, H.; Sandhu, G. Spontaneous Intraperitoneal Rupture of a Hepatic Hydatid Cyst with Subsequent Anaphylaxis: A Case Report. Case Rep. Hepatol. 2013, 2013, 320418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, M.J.; Lee, S.H.; Kim, S.J.; Chei, Y.H.; Park, J.H.; Park, D.H.; Park, S.H.; Kim, S.J. A case of multiple intraperitoneal cysts from ruptured hepatic hydatid cysts. Korean J. Gastroenterol. 2007, 50, 203–206. [Google Scholar]
- Mouaqit, O.; Hibatallah, A.; Oussaden, A.; Maazaz, K.; Taleb, K.A. Acute intraperitoneal rupture of hydatid cysts: A surgical experience with 14 cases. World J. Emerg. Surg. 2013, 8, 28. [Google Scholar] [CrossRef] [Green Version]
- Junghanss, T.; da Silva, A.M.; Horton, J.; Chiodini, P.L.; Brunetti, E. Clinical management of cystic echinococcosis: State of the art, problems, and perspectives. Am. J. Trop. Med. Hyg. 2008, 79, 301–311. [Google Scholar] [CrossRef] [Green Version]
- van Doorn, H.R.; Wentink-Bonnema, E.; Rentenaar, R.J.; van Gool, T. Specific cross-reactivity in sera from cystic echinococcosis patients in an enzyme-linked immunoelectrotransfer blot for cysticercosis diagnostics. Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 948–950. [Google Scholar] [CrossRef]
- Ishida, M.M.; Rubinsky-Elefant, G.; Ferreira, A.W.; Hoshino-Shimizu, S.; Vaz, A.J. Helminth antigens (Taenia solium, Taenia crassiceps, Toxocara canis, Schistosoma mansoni and Echinococcus granulosus) and cross-reactivities in human infections and immunized animals. Acta Trop. 2003, 89, 73–84. [Google Scholar] [CrossRef]
- Kim, H.R.; Lee, M.K.; Hong, S.T.; Chai, J.Y. Comparison of Two Enzyme-Linked Immunosorbent Assays for Detecting Parasitic Diseases. Korean J. Clin. Microbiol. 2008, 11, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Gottstein, B.; Tsang, V.C.; Schantz, P.M. Demonstration of species-specific and cross-reactive components of Taenia solium metacestode antigens. Am. J. Trop. Med. Hyg. 1986, 35, 308–313. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, J.-S.; Kang, M.-K.; Park, J.-G.; Kim, H.-J.; Choi, J.-H. Clinical Implications for the Comprehensive Interpretation of Radiologic and Immunodiagnostic Tests in Patients Suspected of Parasitic Hepatic Cyst, a Rare Case in Korea. Trop. Med. Infect. Dis. 2023, 8, 155. https://doi.org/10.3390/tropicalmed8030155
Yoo J-S, Kang M-K, Park J-G, Kim H-J, Choi J-H. Clinical Implications for the Comprehensive Interpretation of Radiologic and Immunodiagnostic Tests in Patients Suspected of Parasitic Hepatic Cyst, a Rare Case in Korea. Tropical Medicine and Infectious Disease. 2023; 8(3):155. https://doi.org/10.3390/tropicalmed8030155
Chicago/Turabian StyleYoo, Jae-Sung, Min-Kyu Kang, Jung-Gil Park, Hyung-Joo Kim, and Joon-Hyuk Choi. 2023. "Clinical Implications for the Comprehensive Interpretation of Radiologic and Immunodiagnostic Tests in Patients Suspected of Parasitic Hepatic Cyst, a Rare Case in Korea" Tropical Medicine and Infectious Disease 8, no. 3: 155. https://doi.org/10.3390/tropicalmed8030155