


Impact of the COVID-19 Pandemic on Malaria Control in Africa: A Preliminary Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods and Materials
2.1. Study Design and Data Source
2.2. Literature Research Strategies to Evaluate the Impact of the COVID-19 Pandemic on Malaria Control in Africa
3. Results
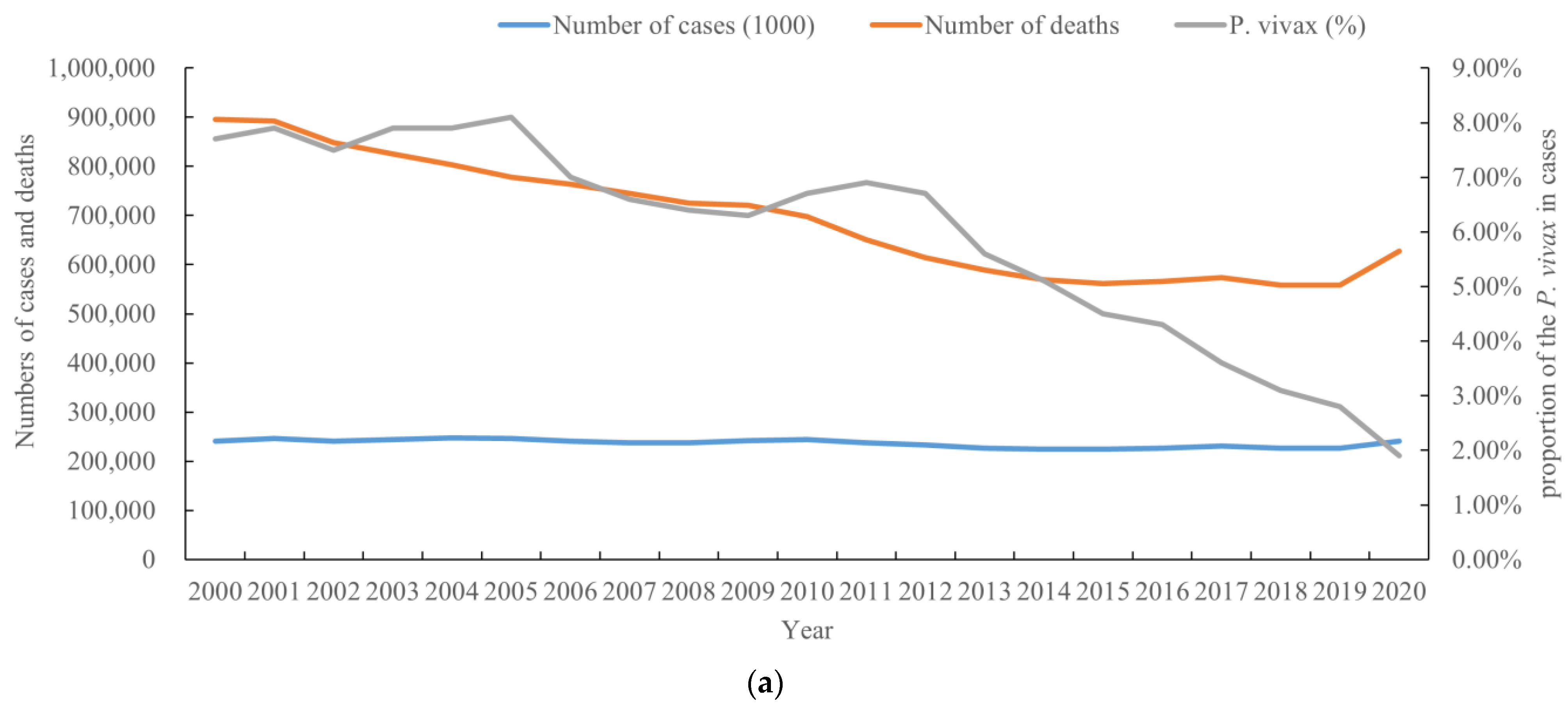
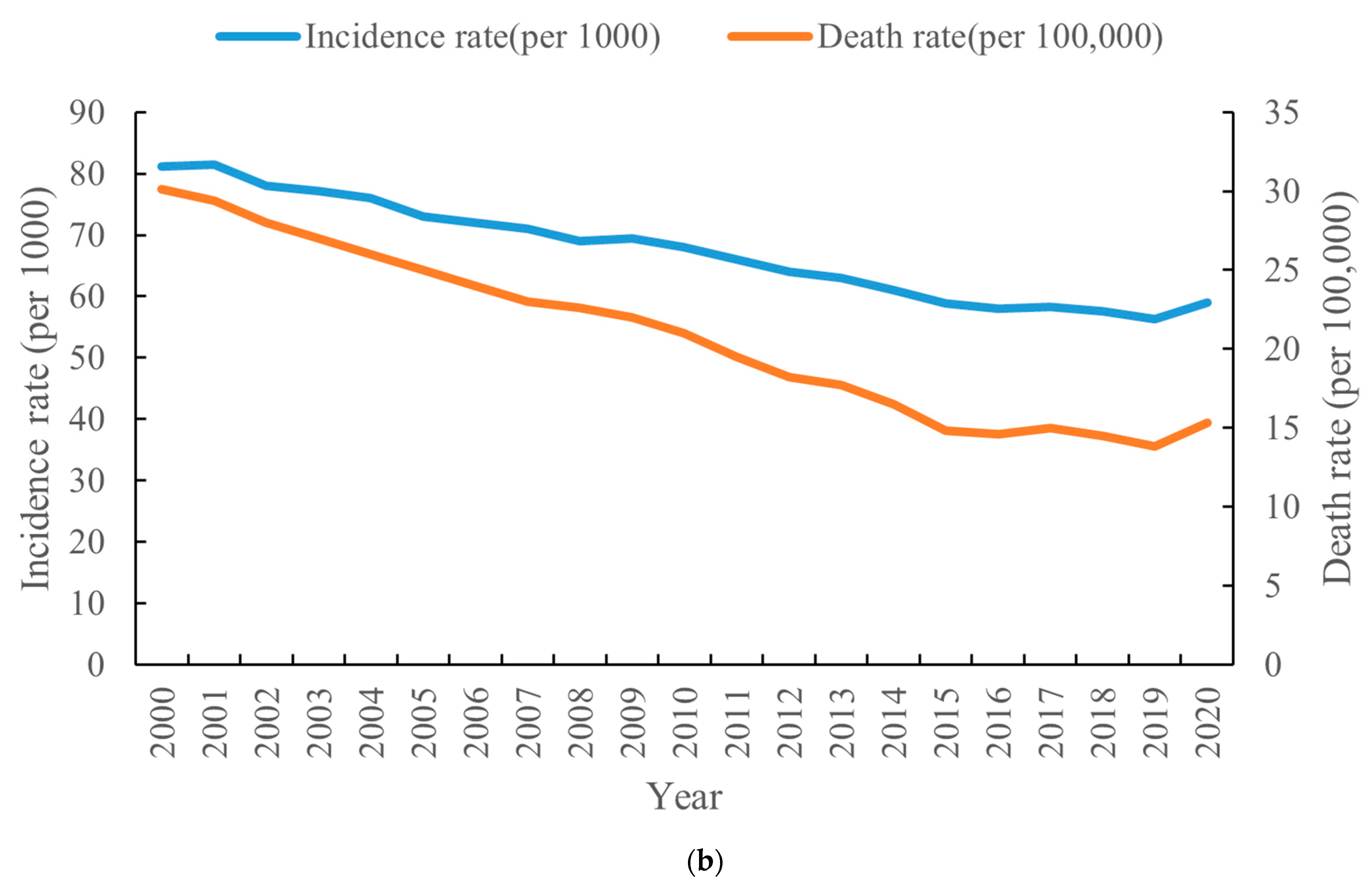
3.1. Epidemic Profile of Malaria at the Global Level, 2000–2020
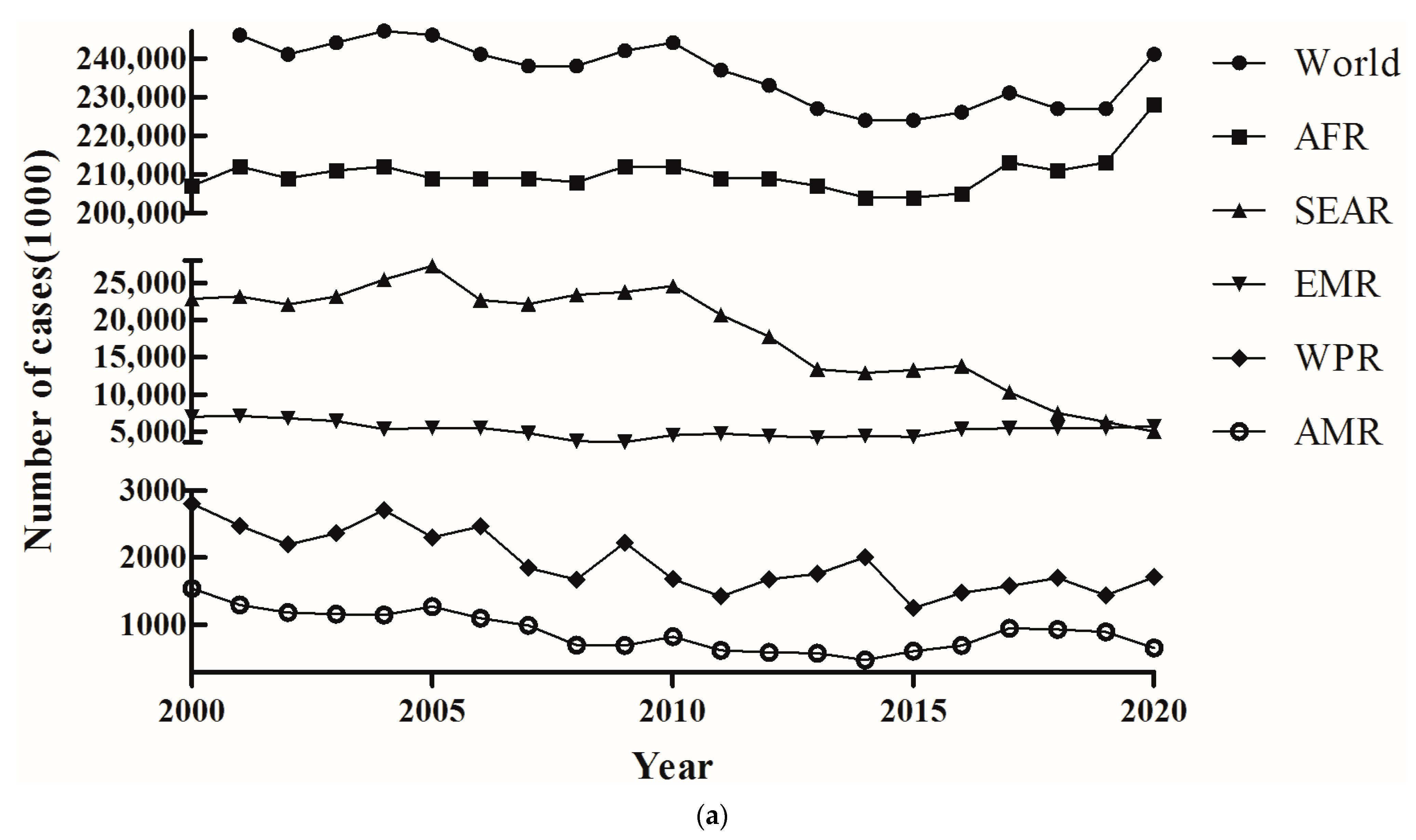
3.2. Distribution of the Number of Cases of and Deaths from Malaria in Different Continents, 2000–2020
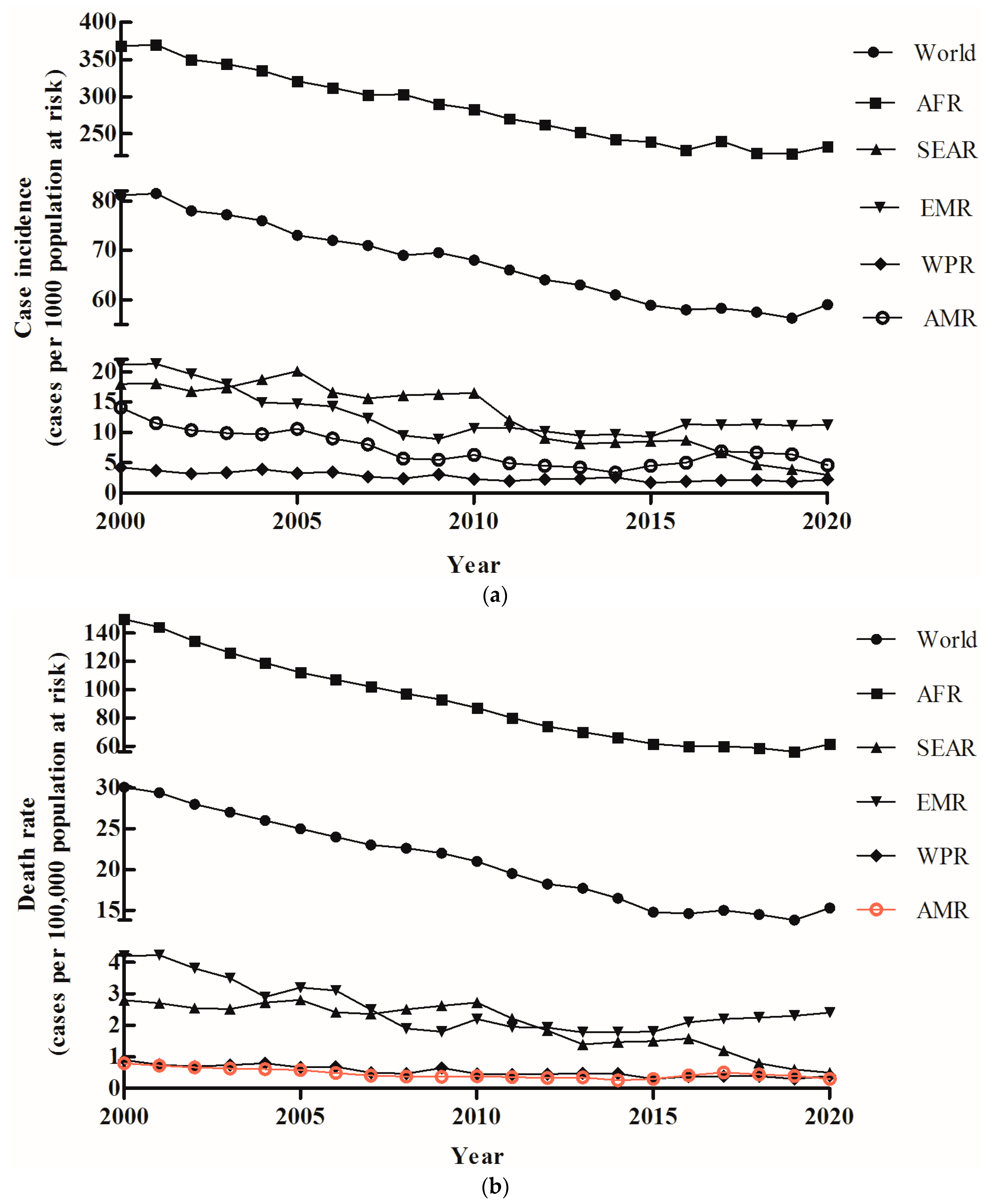
3.3. Malaria Incidence and Death Rate Distribution in Different Continents, 2000–2020
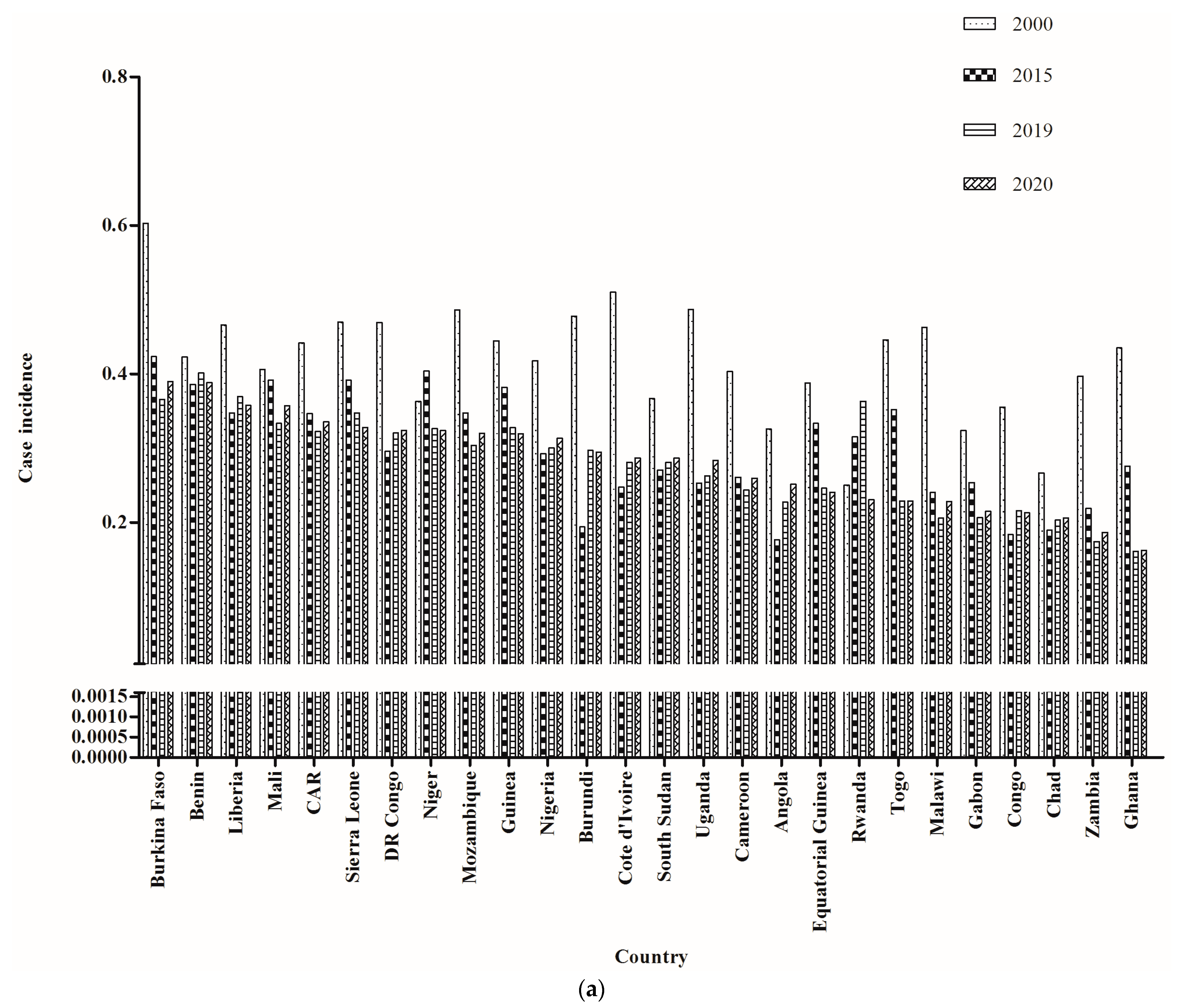
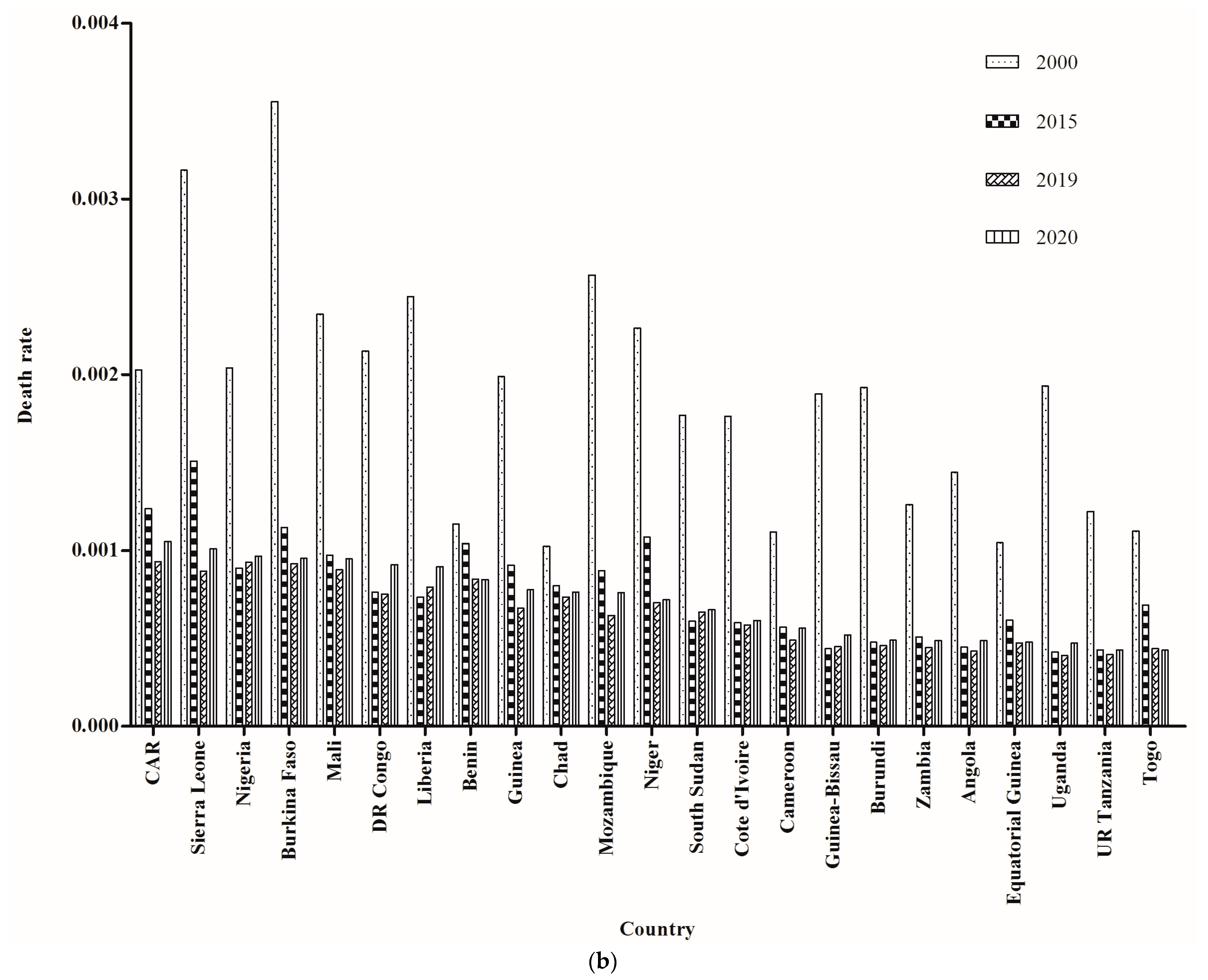
3.4. Epidemic Characteristics of Malaria in African Countries, 2000–2020
3.5. COVID-19 Pandemic Disruption to Health Services and Malaria Control in Africa
3.6. Gap in Financial Investment in Malaria Control
3.7. Delays and Disruption to Pillar Countermeasures
3.8. Clinical Service Disruption during the Pandemic
3.9. Reduction in Medicine Resources
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chhim, S.; Piola, P.; Housen, T.; Herbreteau, V.; Tol, B. Malaria in Cambodia: A Retrospective Analysis of a Changing Epidemiology 2006–2019. Int. J. Environ. Res. Public Health 2021, 18, 1960. [Google Scholar] [CrossRef]
- WHO. World Malaria Report 2020; WHO: Geneva, Switzerland, 2020.
- Annan, K. In-Host Analysis of Malaria Dynamics in Humans. Open J. Appl. 2020, 10, 191–209. [Google Scholar] [CrossRef]
- Holzschuh, A.; Gruenberg, M.; Hofmann, N.E.; Wampfler, R.; Kiniboro, B.; Robinson, L.J.; Mueller, I.; Felger, I.; White, M.T. Co-infection of the four major Plasmodium species: Effects on densities and gametocyte carriage. PLoS Negl. Trop. Dis. 2022, 16, e0010760. [Google Scholar] [CrossRef]
- Moita, D.; Maia, T.G.; Duarte, M.; Andrade, C.M.; Albuquerque, I.S.; Dwivedi, A.; Silva, J.C.; González-Céron, L.; Janse, C.J.; Mendes, A.M.; et al. A genetically modified Plasmodium berghei parasite as a surrogate for whole-sporozoite vaccination against P. vivax malaria. NPJ Vaccin. 2022, 7, 163. [Google Scholar] [CrossRef]
- Varo, R.; Chaccour, C.; Bassat, Q. Update on malaria. Med. Clin. 2020, 155, 395–402. [Google Scholar] [CrossRef]
- Mbacham, W.F.; Ayong, L.; Guewo-Fokeng, M.; Makoge, V. Current Situation of Malaria in Africa. Methods Mol. Biol. 2019, 2013, 29–44. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Malaria Report 2021; WHO: Geneva, Switzerland, 2021.
- Chen, K.; Ponnusamy, L.; Mouhamadou, C.S.; Fodjo, B.K.; Sadia, G.C.; Affoue, F.P.K.; Deguenon, J.M.; Roe, R.M. Internal and external microbiota of home-caught Anopheles coluzzii (Diptera: Culicidae) from Côte d’Ivoire, Africa: Mosquitoes are filthy. PLoS ONE 2022, 17, e0278912. [Google Scholar] [CrossRef] [PubMed]
- Mburu, M.M.; Mzilahowa, T.; Amoah, B.; Chifundo, D.; Phiri, K.S.; van den Berg, H.; Takken, W.; McCann, R.S. Biting patterns of malaria vectors of the lower Shire valley, southern Malawi. Acta Trop. 2019, 197, 105059. [Google Scholar] [CrossRef]
- Verra, F.; Angheben, A.; Martello, E.; Giorli, G.; Perandin, F.; Bisoffi, Z. A systematic review of transfusion-transmitted malaria in non-endemic areas. Malar. J. 2018, 17, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monroe, A.; Olapeju, B.; Moore, S.; Hunter, G.; Merritt, A.P.; Okumu, F.; Babalola, S. Improving malaria control by understanding human behaviour. Bull. World Health Organ. 2021, 99, 837–839. [Google Scholar] [CrossRef]
- Patlolla, A.K.; Smith, Z.; Tchounwou, P. Indirect Impacts of COVID-19 on the Environment: A Global Review. Int. J. Biomed. Clin. Anal. 2022, 2, 9–19. [Google Scholar]
- Mahajan, N.N.; Gajbhiye, R.K.; Bahirat, S.; Lokhande, P.D.; Mathe, A.; Rathi, S.; Warty, N.; Mahajan, K.N.; Srivastava, V.; Kuppusamy, P.; et al. Co-infection of malaria and early clearance of SARS-CoV-2 in healthcare workers. J. Med. Virol. 2021, 93, 2431–2438. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.A.; Emina, J.B.; Eckert, E.; Ye, Y. Prompt access to effective malaria treatment among children under five in sub-Saharan Africa: A multi-country analysis of national household survey data. Malar. J. 2015, 14, 329. [Google Scholar] [CrossRef] [Green Version]
- Manana, P.N.; Kuonza, L.; Musekiwa, A.; Mpangane, H.D.; Koekemoer, L.L. Knowledge, attitudes and practices on malaria transmission in Mamfene, KwaZulu-Natal Province, South Africa 2015. BMC Public Health 2017, 18, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. World Malaria Report 2019; WHO: Geneva, Switzerland, 2019.
- Ajayi, I.O.; Ajumobi, O.O.; Falade, C. Malaria and COVID-19: Commonalities, intersections and implications for sustaining malaria control. Pan Afr. Med. J. 2020, 37, 1. [Google Scholar] [CrossRef]
- Narain, K.; Rackimuthu, S.; Nawaz, F.A.; Okonji, O.C.; Ashworth, H.; Du Plessis, S.S.; Shah, J. Strategies for malaria vaccination during the COVID-19 pandemic in African countries. Bull. World Health Organ. 2022, 100, 582. [Google Scholar] [CrossRef]
- Cheng, N.I.; Tabong, P.T.; Netongo, P.M.; Mensah, B.A.; Chu, C.E.; Yaw, E.B.; Enos, J.Y.; Malm, K.; Ahorlu, C.S. The impact of COVID-19 on implementation of mass testing, treatment and tracking of malaria in rural communities in Ghana: A qualitative study. PLoS ONE 2022, 17, e0275976. [Google Scholar] [CrossRef]
- Siddiqui, J.A.; Aamar, H.; Siddiqui, A.; Essar, M.Y.; Khalid, M.A.; Mousavi, S.H. Malaria in Afghanistan: Challenges, efforts and recommendations. Ann. Med. Surg. 2022, 81, 104424. [Google Scholar] [CrossRef] [PubMed]
- Lendongo-Wombo, J.B.; Oyegue-Liabagui, S.L.; Biteghe-Bi-Essone, J.C.; Ngoungou, E.B.; Lekana-Douki, J.B. Epidémiology of malaria from 2019 to 2021 in the southeastern city of Franceville, Gabon. BMC Public Health 2022, 22, 2313. [Google Scholar] [CrossRef]
- Liu, Q.; Yan, W.; Qin, C.; Du, M.; Liu, M.; Liu, J. Millions of excess cases and thousands of excess deaths of malaria occurred globally in 2020 during the COVID-19 pandemic. J. Glob. Health 2022, 12, 05045. [Google Scholar] [CrossRef] [PubMed]
- Chanda-Kapata, P.; Ntoumi, F.; Kapata, N.; Lungu, P.; Mucheleng’anga, L.A.; Chakaya, J.; Tembo, J.; Himwaze, C.; Ansumana, R.; Asogun, D.; et al. Tuberculosis, HIV/AIDS and Malaria Health Services in sub-Saharan Africa—A Situation Analysis of the Disruptions and Impact of the COVID-19 Pandemic. Int. J. Infect. Dis. 2022, 124, S41–S46. [Google Scholar] [CrossRef]
- Walker, P.G.; White, M.T.; Griffin, J.T.; Reynolds, A.; Ferguson, N.M.; Ghani, A.C. Malaria morbidity and mortality in Ebola-affected countries caused by decreased health-care capacity, and the potential effect of mitigation strategies: A modelling analysis. Lancet Infect. Dis. 2015, 15, 825–832. [Google Scholar] [CrossRef] [Green Version]
- WHO. Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic: Interim Report 27 August 2020; WHO: Geneva, Switzerland, 2020.
- WHO. Second Round of the National Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic; WHO: Geneva, Switzerland, 2021.
- Prabhu, S.R.; Ware, A.P.; Saadi, A.V.; Brand, A.; Ghosh, S.K.; Kamath, A.; Satyamoorthy, K. Malaria Epidemiology and COVID-19 Pandemic: Are They Interrelated? Omics 2022, 26, 179–188. [Google Scholar] [CrossRef] [PubMed]
- WHO. Third Round of the Global Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic; WHO: Geneva, Switzerland, 2021.
- Likwela, J.L.; Ngwala, P.L.; Ntumba, A.K.; Ntale, D.C.; Sompwe, E.M.; Mpiana, G.K.; Tshula, J.K.; Likwela, T.K.; Kanku-Ka-Munabe, P.; Kumbi, A.N.; et al. Digitalized long-lasting insecticidal nets mass distribution campaign in the context of Covid-19 pandemic in Kongo Central, Democratic Republic of Congo: Challenges and lessons learned. Malar. J. 2022, 21, 253. [Google Scholar] [CrossRef] [PubMed]
- Noor, A.M.; Alonso, P.L. The message on malaria is clear: Progress has stalled. Lancet 2022, 399, 1777. [Google Scholar] [CrossRef]
- Cohen, J.M.; Smith, D.L.; Cotter, C.; Ward, A.; Yamey, G.; Sabot, O.J.; Moonen, B. Malaria resurgence: A systematic review and assessment of its causes. Malar. J. 2012, 11, 122. [Google Scholar] [CrossRef] [Green Version]
- Ihekweazu, C. Lessons from Nigeria’s Adaptation of Global Health Initiatives during the COVID-19 Pandemic. Emerg. Infect. Dis. 2022, 28, S299–S301. [Google Scholar] [CrossRef]
- Shretta, R.; Silal, S.P.; Malm, K.; Mohammed, W.; Narh, J.; Piccinini, D.; Bertram, K.; Rockwood, J.; Lynch, M. Estimating the risk of declining funding for malaria in Ghana: The case for continued investment in the malaria response. Malar. J. 2020, 19, 196. [Google Scholar] [CrossRef]
- Shretta, R.; Zelman, B.; Birger, M.L.; Haakenstad, A.; Singh, L.; Liu, Y.; Dieleman, J. Tracking development assistance and government health expenditures for 35 malaria-eliminating countries: 1990–2017. Malar. J. 2017, 16, 251. [Google Scholar] [CrossRef]
- Hardy, H.; Hopkins, R.; Mnyone, L.; Hawkes, F.M. Manure and mosquitoes: Life history traits of two malaria vector species enhanced by larval exposure to cow dung, whilst chicken dung has a strong negative effect. Parasit. Vectors 2022, 15, 472. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.; Tusting, L.S.; Bottomley, C.; Saito, K.; Djouaka, R.; Lines, J. Malaria transmission and prevalence in rice-growing versus non-rice-growing villages in Africa: A systematic review and meta-analysis. Lancet Planet Health 2022, 6, e257–e269. [Google Scholar] [CrossRef]
- Kibret, S.; McCartney, M.; Lautze, J.; Nhamo, L.; Yan, G. The impact of large and small dams on malaria transmission in four basins in Africa. Sci. Rep. 2021, 11, 13355. [Google Scholar] [CrossRef] [PubMed]
- Tangena, J.A.; Hendriks, C.M.J.; Devine, M.; Tammaro, M.; Trett, A.E.; Williams, I.; DePina, A.J.; Sisay, A.; Herizo, R.; Kafy, H.T.; et al. Indoor residual spraying for malaria control in sub-Saharan Africa 1997 to 2017: An adjusted retrospective analysis. Malar. J. 2020, 19, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diouf, I.; Rodriguez Fonseca, B.; Caminade, C.; Thiaw, W.M.; Deme, A.; Morse, A.P.; Ndione, J.A.; Gaye, A.T.; Diaw, A.; Ndiaye, M.K.N. Climate Variability and Malaria over West Africa. Am. J. Trop. Med. Hyg. 2020, 102, 1037–1047. [Google Scholar] [CrossRef]
- Weedall, G.D.; Riveron, J.M.; Hearn, J.; Irving, H.; Kamdem, C.; Fouet, C.; White, B.J.; Wondji, C.S. An Africa-wide genomic evolution of insecticide resistance in the malaria vector Anopheles funestus involves selective sweeps, copy number variations, gene conversion and transposons. PLoS Genet. 2020, 16, e1008822. [Google Scholar] [CrossRef]
- Balikagala, B.; Fukuda, N.; Ikeda, M.; Katuro, O.T.; Tachibana, S.I.; Yamauchi, M.; Opio, W.; Emoto, S.; Anywar, D.A.; Kimura, E.; et al. Evidence of Artemisinin-Resistant Malaria in Africa. N. Engl. J. Med. 2021, 385, 1163–1171. [Google Scholar] [CrossRef]
- WHO. World Malaria Report 2015. Global Malaria Programme; WHO: Geneva, Switzerland, 2015.
- Gunalan, K.; Lo, E.; Hostetler, J.B.; Yewhalaw, D.; Mu, J.; Neafsey, D.E.; Yan, G.; Miller, L.H. Role of Plasmodium vivax Duffy-binding protein 1 in invasion of Duffy-null Africans. Proc. Natl. Acad. Sci. USA 2016, 113, 6271–6276. [Google Scholar] [CrossRef] [Green Version]
- Giesen, C.; Roche, J.; Redondo-Bravo, L.; Ruiz-Huerta, C.; Gomez-Barroso, D.; Benito, A.; Herrador, Z. The impact of climate change on mosquito-borne diseases in Africa. Pathog. Glob. Health 2020, 114, 287–301. [Google Scholar] [CrossRef]
- Wiysonge, C.S.; Ndwandwe, D.; Ryan, J.; Jaca, A.; Batouré, O.; Anya, B.M.; Cooper, S. Vaccine hesitancy in the era of COVID-19: Could lessons from the past help in divining the future? Hum. Vaccin. Immunother. 2022, 18, 1–3. [Google Scholar] [CrossRef]
- Coker, M.; Folayan, M.O.; Michelow, I.C.; Oladokun, R.E.; Torbunde, N.; Sam-Agudu, N.A. Things must not fall apart: The ripple effects of the COVID-19 pandemic on children in sub-Saharan Africa. Pediatr. Res. 2021, 89, 1078–1086. [Google Scholar] [CrossRef]
- Musa, S.S.; Abdullahi, Z.U.; Zhao, S.; Bello, U.M.; Hussaini, N.; Habib, A.G.; He, D. Transmission Dynamics of Monkeypox Virus in Nigeria during the Current COVID-19 Pandemic and Estimation of Effective Reproduction Number. Vaccines 2022, 10, 2153. [Google Scholar] [CrossRef] [PubMed]
- Saied, A.A.; Metwally, A.A.; Dhawan, M.; Choudhary, O.P.; Aiash, H. Strengthening vaccines and medicines manufacturing capabilities in Africa: Challenges and perspectives. EMBO Mol. Med. 2022, 14, e16287. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Regional Health-Western, P. Back on track towards malaria elimination—Lessons and innovations. Lancet Reg Health West Pac 2022, 21, 100473. [Google Scholar] [CrossRef] [PubMed]
- Ghansah, A.; Kamau, E.; Amambua-Ngwa, A.; Ishengoma, D.S.; Maiga-Ascofare, O.; Amenga-Etego, L.; Deme, A.; Yavo, W.; Randrianarivelojosia, M.; Ochola-Oyier, L.I.; et al. Targeted Next Generation Sequencing for malaria research in Africa: Current status and outlook. Malar. J. 2019, 18, 324. [Google Scholar] [CrossRef] [Green Version]
- Teboh-Ewungkem, M.I.; Ngwa, G.A. COVID-19 in malaria-endemic regions: Potential consequences for malaria intervention coverage, morbidity, and mortality. Lancet Infect. Dis. 2021, 21, 5–6. [Google Scholar] [CrossRef]
- Cohee, L.M.; Opondo, C.; Clarke, S.E.; Halliday, K.E.; Cano, J.; Shipper, A.G.; Barger-Kamate, B.; Djimde, A.; Diarra, S.; Dokras, A.; et al. Preventive malaria treatment among school-aged children in sub-Saharan Africa: A systematic review and meta-analyses. Lancet Glob. Health 2020, 8, e1499–e1511. [Google Scholar] [CrossRef]
- Shi, B.; Zheng, J.; Xia, S.; Lin, S.; Wang, X.; Liu, Y.; Zhou, X.N.; Liu, J. Accessing the syndemic of COVID-19 and malaria intervention in Africa. Infect. Dis. Poverty 2021, 10, 5. [Google Scholar] [CrossRef]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, L.; Shi, Q.; Liu, Z.; Li, Z.; Dong, X. Impact of the COVID-19 Pandemic on Malaria Control in Africa: A Preliminary Analysis. Trop. Med. Infect. Dis. 2023, 8, 67. https://doi.org/10.3390/tropicalmed8010067
Gao L, Shi Q, Liu Z, Li Z, Dong X. Impact of the COVID-19 Pandemic on Malaria Control in Africa: A Preliminary Analysis. Tropical Medicine and Infectious Disease. 2023; 8(1):67. https://doi.org/10.3390/tropicalmed8010067
Chicago/Turabian StyleGao, Liping, Qi Shi, Zhiguo Liu, Zhenjun Li, and Xiaoping Dong. 2023. "Impact of the COVID-19 Pandemic on Malaria Control in Africa: A Preliminary Analysis" Tropical Medicine and Infectious Disease 8, no. 1: 67. https://doi.org/10.3390/tropicalmed8010067