

A Modular Structure for Immediate and Transitory Interventions to Guarantee Access to Basic Healthcare in Italy

Abstract
:1. Introduction
- the methodology. The aim of the research is to define a modular “ad hoc” solution, calibrated on users’ needs to give a concrete response both to the effective need of health treatment and to social disease. Despite what is generally believed, the health of individuals is not only about the healing process, but includes a range of broader factors, including so-called determinants that involve the context within which each of us lives, our social status related to the work we do and the actual information and care we take of our body;
- the design strategy. The aim is to overcome standard temporary structures, by introducing public areas in the design concept. Migrants are generally young and healthy individuals who lose one or more of these determinants during their journey, causing damage to their health [5]. This worsens due to the fact that, once they arrived in the host country, the procedure for obtaining protection by the primary doctor is impracticable or often very complicated without an intermediary able to request the permission in place of the migrant;
- the technology. Standardized structures generally respond to emergencies and extraordinary events. The objective is to overcome the idea of single function structures, in favor of flexible structures that can be used for various functions. The technological response to the design of public/private spaces, this overcomes the use of container or other rigid codified models. Internal comfort and energy efficiency are requirements in this model;
- the financing model. The model proposes a structure that allows different furniture configuration, in order to make it multifunctional. This characteristic it is essential to optimize the investment. The project is part of a reality that is almost entirely financed through public and private donations. Therefore, the economy of the intervention is fundamental: the aim is to create an economic prototype that is also easy to make, so as to give the greatest number of associations that deal with this issue the possibility to achieve it, with or without the economic contribution of the National public sanitary system.
2. State of the Art
3. Materials and Methods
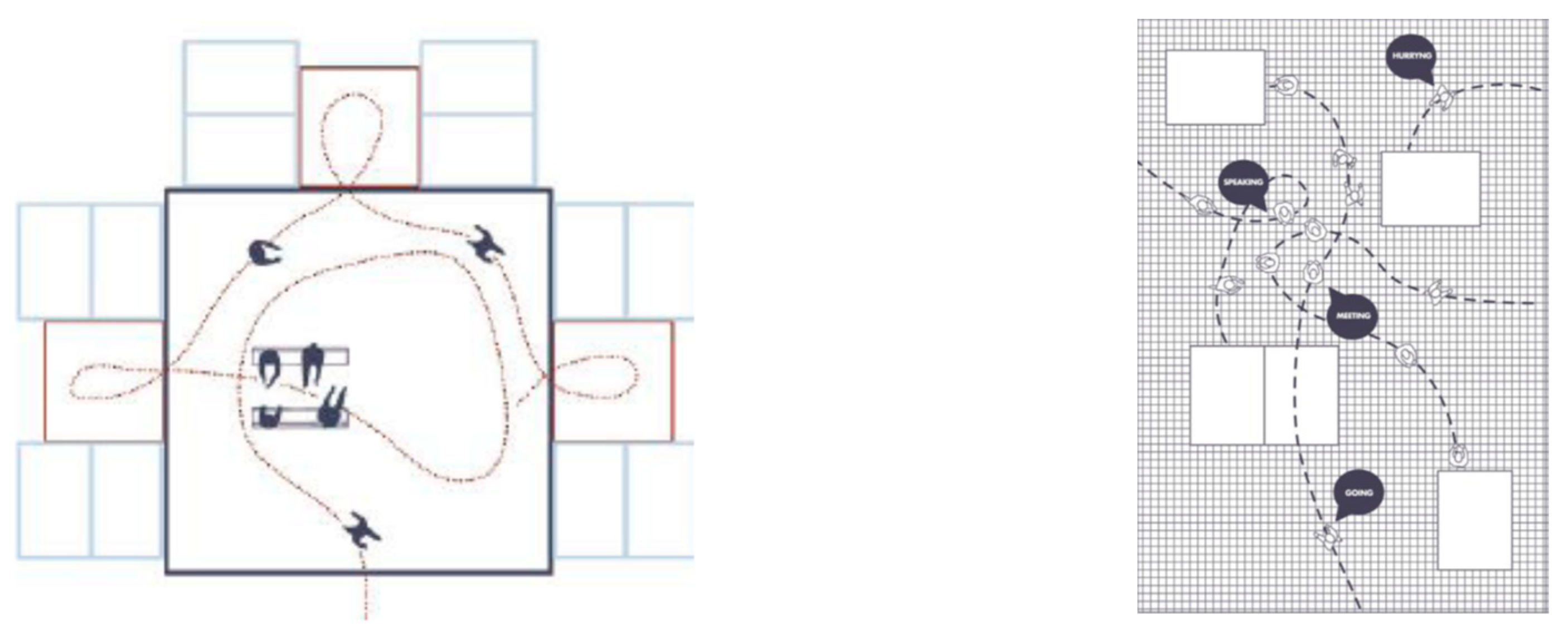
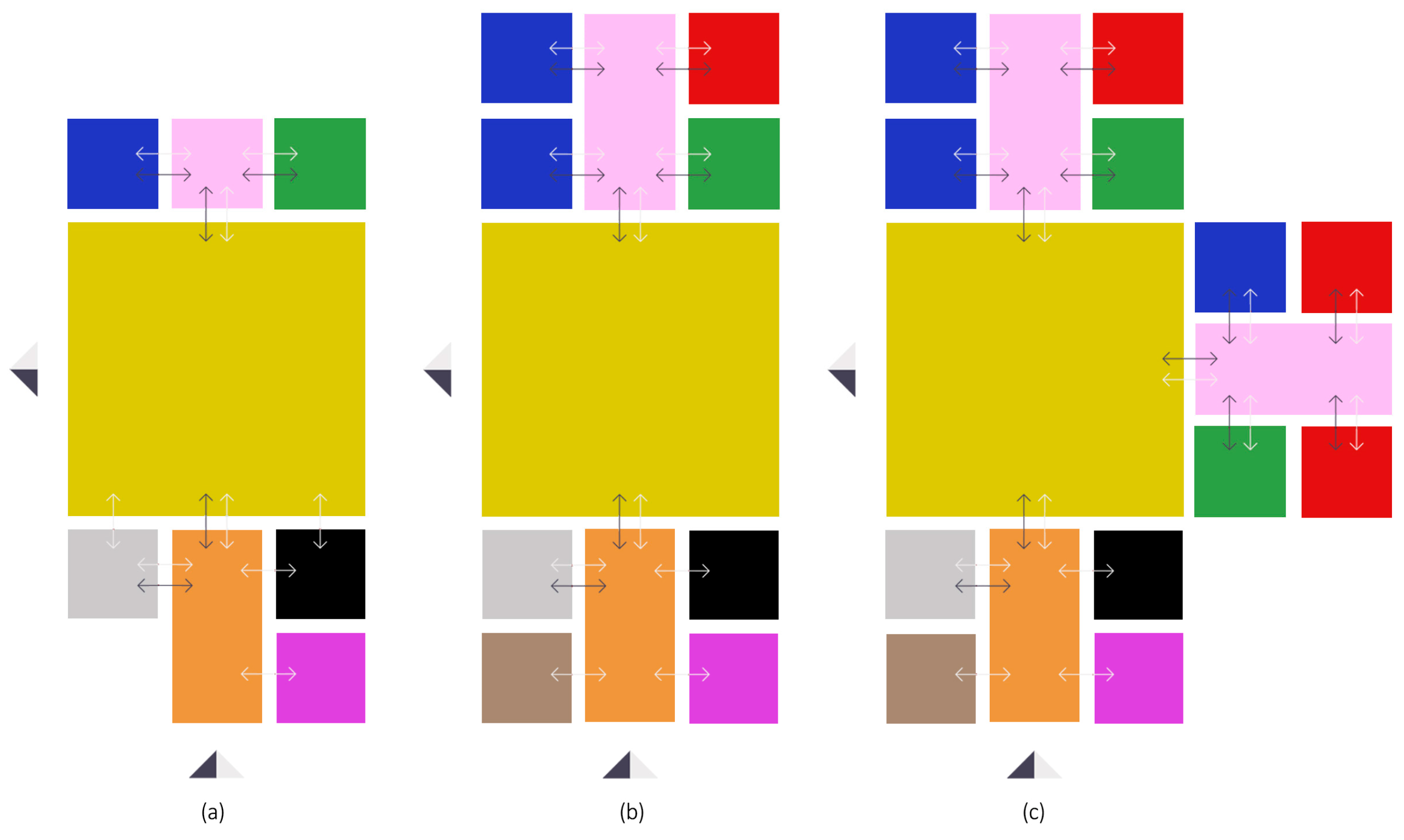
3.1. Conceptual Framework and Preliminary Design
3.2. Technological Features
3.2.1. Platform
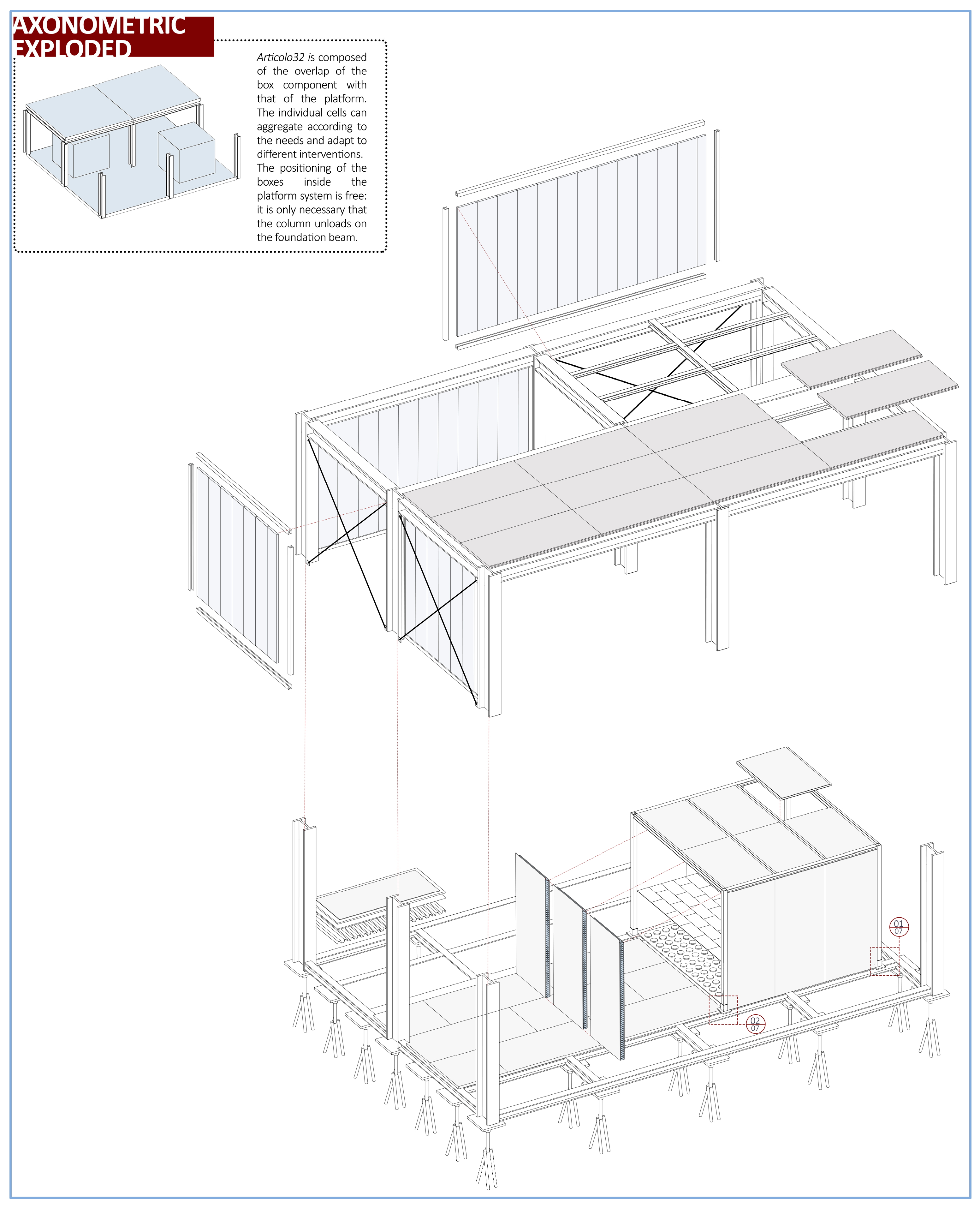
3.2.2. Box
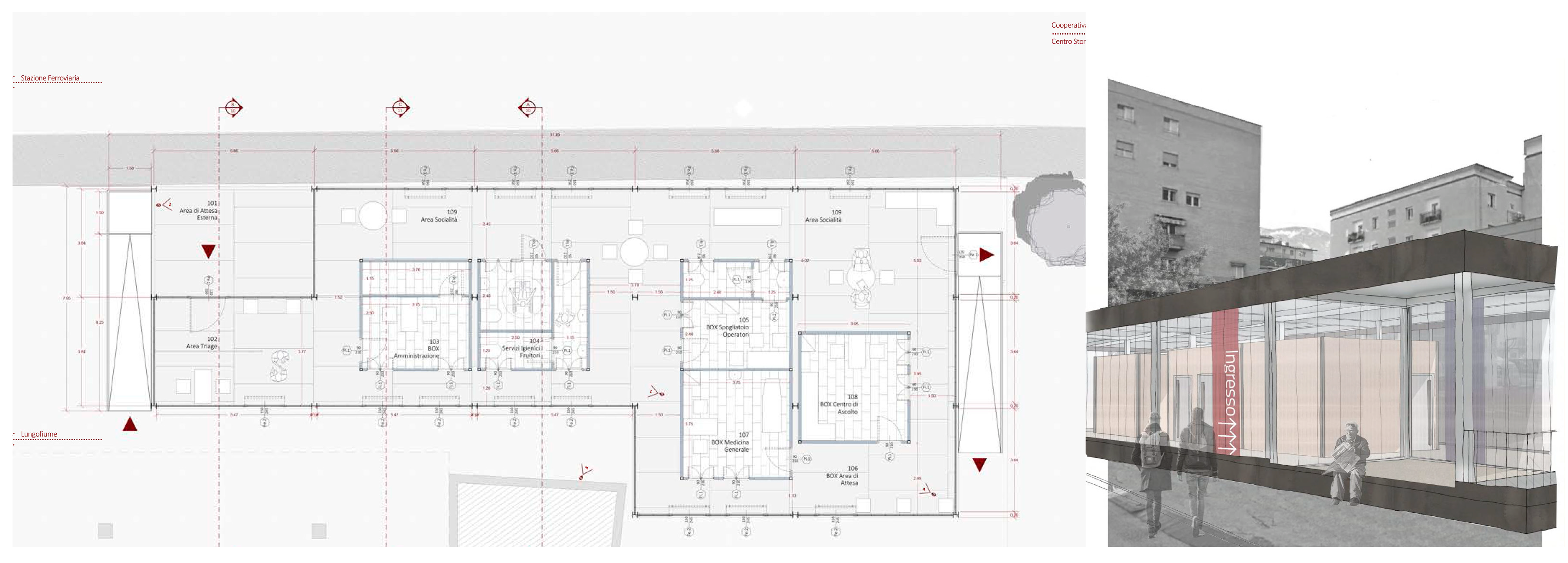
4. Case Study—A Project Application in Italy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, X.; Ma, S.; Chen, S. Healthcare process modularization using design structure matrix. Adv. Eng. Inform. 2019, 39, 320–330. [Google Scholar] [CrossRef]
- Verderber, S. Architects as First Responders: Portable Healthcare Architecture in a Climate-Altered World. Arch. Des. 2017, 87, 100–107. [Google Scholar] [CrossRef]
- Biglino, I.; Olmo, A. La Salute Come Diritto Fondamentale: Una Ricerca sui Migranti a Torino, 1st ed.; il Mulino: Bologna, Italy, 2014. [Google Scholar]
- Smolova, M.; Smolova, D. Emergency architecture. Modular construction of healthcare facilities as a response to pandemic outbreak. E3S Web Conf. 2021, 274, 01013. [Google Scholar] [CrossRef]
- Regione Marche. Gli Ambulatori per Stranieri Temporaneamente Presenti (STP) Europei Non Iscritti (ENI) Nella Regione Marche. Available online: regione.marche.it/portals/0/ODS/2020%20Sito%20ODS/report_STP_12%20%2009%202019_rev_21_1_20.pdf (accessed on 27 December 2021).
- Bologna, R.; Terpolilli, C. Emergenza del Progetto. Progetto dell’Emergenza. Architetture Con-Temporaneità; Federico Motta Editore: Milano, Italy, 2005. [Google Scholar]
- Jodidio, P. (Ed.) Temporary Architecture Now! TASCHEN GMBH: Bonn, Germany, 2011. [Google Scholar]
- Falasca, C.C. Architetture ad Assetto Variabile. Modelli Evolutivi per L’habitat Provvisorio; Tecnologia e Progetto 3; Alinea Editrice: Firenze, Italy, 2000. [Google Scholar]
- Pan, W.; Zhang, Z. Evaluating Modular Healthcare Facilities for COVID-19 Emergency Response—A Case of Hong Kong. Buildings 2022, 12, 1430. [Google Scholar] [CrossRef]
- Navaratnam, S.; Nguyen, K.; Selvaranjan, K.; Zhang, G.; Mendis, P.; Aye, L. Designing Post COVID-19 Buildings: Approaches for Achieving Healthy Buildings. Buildings 2022, 12, 74. [Google Scholar] [CrossRef]
- Carlo Ratti Associati Designs. SHIPPING-CONTAINER Intensive Care Units for Coronavirus Treatment; Carlo Ratti Associati Designs: Turin, Italy, 2020; Available online: https://www.dezeen.com/2020/03/24/shipping-container-intensive-care-units-coronavirus-covid-19-carlo-ratti/ (accessed on 6 April 2021).
- Binkin, N.; Salmaso, S.; Michieletto, F.; Russo, F. Protecting our health care workers while protecting our communities during the COVID-19 pandemic: A comparison of approaches and early outcomes in two Italian regions, Italy, 2020. medrXiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Openpolis. Una Mappa Dell’accoglienza. Centri d’Italia. 2021. Available online: https://www.actionaid.it/app/uploads/2021/03/Centri_Italia_una-mappa_accoglienza.pdf (accessed on 1 April 2023).
- Cocina, G.G.; De Filippi, F. Salute e Spazi per la Cura. Ripensare le Strutture Sanitarie in una Prospettiva Multiculturale, 1st ed.; Tabedizioni: Roma, Italy, 2012. [Google Scholar]
- Pan, W.; Yang, Y.; Zhang, Z.; Chan, S. Modularisation for Modernisation: A Strategy Paper Rethinking Hong Kong Construction; CICID, The University of Hong Kong: Hong Kong, China, 2019; Available online: http://hdl.handle.net/10722/275575 (accessed on 20 August 2022).
- McAndrew, F.T. Environmental Psychology, 1st ed.; Thomson Brooks, Cole Publishing Co.: Pacific Grove, CA, USA, 1993; p. 121. [Google Scholar]
- Baroni, M.R. Psicologia Ambientale, 1st ed.; Il Mulino: Bologna, Italy, 1998. [Google Scholar]
- Loizou, L.; Barati, K.; Shen, X.; Li, B. Quantifying Advantages of Modular Construction: Waste Generation. Buildings 2021, 11, 622. [Google Scholar] [CrossRef]
- Paudel, P.; Dulal, S.; Bhandari, M.; Tomar Amit, K. Study on Pre-fabricated Modular and Steel Structures. SSRG Int. J. Civ. Eng. (SSRG—IJCE) 2016, 3, 7–14. [Google Scholar]
- Serranzanetti, F. TAMassociati. Taking Care. Architetture Con Emergency, 2nd ed.; Electa: Firenze, Italy, 2017. [Google Scholar]
- Cacciamani, C. Real Estate, Manuale di Economia e Finanza Immobiliare; Egea: Milano, Italy, 2006. [Google Scholar]
- Grünewald, D.N. A Typological Analysis of Temporary Medical Structures before and during the COVID-19 Pandemic: How Can Design Help Us to Deal with Situations of Crisis and Emergency? TU Delft Architecture and the Built Environment; Delft University of Technology: Delft, The Netherlands, 2021; Available online: https://repository.tudelft.nl/islandora/object/uuid%3A9e58a6b2-8a18-4c27-b677-ce4b448e3d6f (accessed on 1 April 2023).
- Ismalia, R.; Djimantoro, M.I. Creating healing environment in cancer rehabilitation center: A comparison study. In Proceedings of the IOP Conference Series: Earth and Environmental Science. In Proceedings of the 3rd International Conference on Eco Engineering Development, Solo, Indonesia, 13–14 November 2019. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structure | Average Number of Users per Year (2017–2020) | Main Provenience (More than 10%) | Type of Care |
|---|---|---|---|
| Caritas Diocesana di Ferrara e Comacchio—FERRARA | 1688 | - | General medicine 73% Specialist medicine a 17% Pediatrics 10% |
| Ambulatorio“Querce di Mamre, Caritas Reggiana—REGGIO EMILIA | 1066 | Georgia 13% Nigeria 10% Albania 8% | Specialist medicine 100% (Dentistry 19% Orthopedic 13% Cardiovascular 11% Gynecology 8% Dermatology 8% Mental 7% Other 34%) |
| Ambulatorio Paolo Simone, Maundodé, Caritas— SENIGALLIA | 254 | Tunisia 12% Romania 8% Afghanistan 8% Marocco 7% | General medicine 62% Specialist medicine a 35% Pediatrics 3% |
| Ambulatorio SOKOS— BOLOGNA | 3500 | - | Specialist medicine 100% (Gynecology 16% Dentistry 14% Cardiology 9% Cardiovascular 5% Diabetes 5% Mental 4% Other 47%) |
| Ambulatorio Giovanni Paolo II, SERMIG—TORINO | Marocco 22% Nigeria 10% Romania 7% | Specialist medicine 100% (Orthopedic 20% Gynecology 16% Dermatology 11% Dentistry 9% Cardiovascular 5% Dressing/sutures 3% Mental 3% Other 32%) | |
| Ambulatorio Biavati, BOLOGNA | 3836 | - | General medicine 75% Specialist medicine a 17% Pepediatrics 8% |
| Space | Dimension | Space Characterization |
|---|---|---|
| General practice | 3 × 3 mod. | Generally, it is used for basic healthcare, in the minimal aggregation of the project it can be used also in gynecology |
| Special medicine | 3 × 6 mod. | Provides a private toilet and sterilization machine (as the equipment is not sent to auxiliary facilities to be sterilized). |
| Listening Centre | 3 × 3 mod. | A private room where the patient can talk with the therapist or the psychotherapist without feeling anxiety. |
| Administrative area | 3 × 3 mod. | This space is different from the triage area because it is dedicated to more personal issues such as economic aid or individual problems. |
| Storage and Pharmaceutical Bank | 3 × 3 mod. | It is not essential in clinics where there is not enough space available. It is possible to form crowds in the structure. |
| Restroom | 3 × 3 mod. | It is essential if the structure is not adjacent to a principal structure (e.g., a hospital) where toilets are available. |
| Staff area | 3 × 3/3 × 6 mod. | It depends on the size of the service, and on the number of personnel. |
| Space | Dimension | Space Characterization |
|---|---|---|
| Triage area | No dim. | It is used for the first diagnosis of users and guidance in the service. |
| Waiting area | No dim. | Nearby the practice. |
| Social area | No dim. | All around the building. |
| Title 1 | Title 3 |
|---|---|
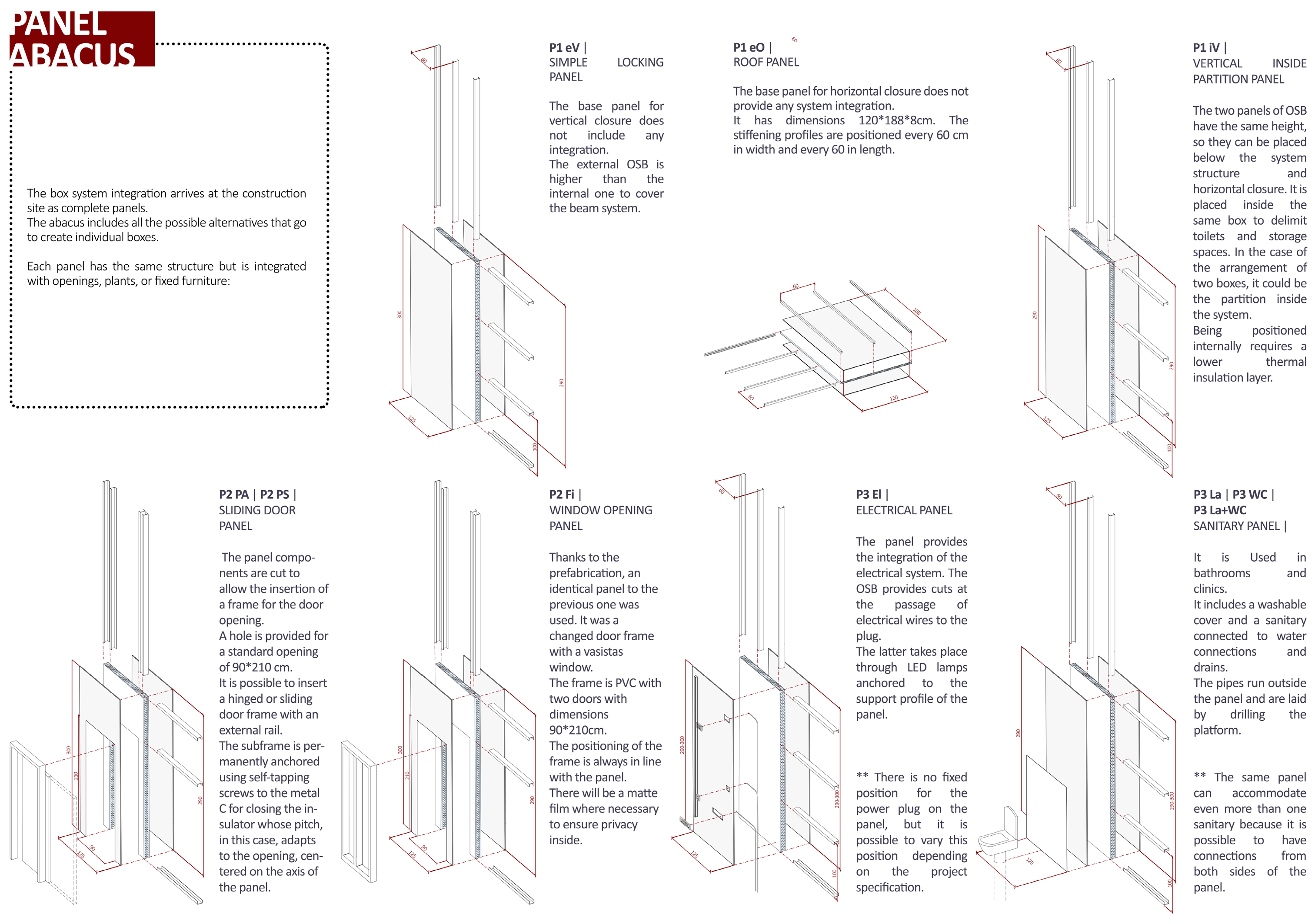
| External Vertical panel | 125 × 300 cm size, thickness 11.2 cm. Defines the spaces between inside and outside, does not require plant equipment. |
| Roof Panel | 120 × 188 cm side, thickness 8 cm. Designed with a different pitch to be anchored to the frame cover, the panel is necessary because the box is heated. Contained more metal C to prevent bending. |
| Inner Vertical panel | 125 × 290 cm size, thickness 9.9 cm This panel is similar to the external vertical panel except for the height, that is lower, being placed under the frame beams to allow the anchoring. Additionally, it is thinner, due to less insulation inside. |
| Sliding door panel | Panels are cut to insert a door-frame for the access to the box. Prefabrication system is optimized. Standard opening 90 × 210 cm. |
| Window opening panel | Similar to door panel. A window frame 90 × 210 cm instead of the door. A moveable vasistas window to optimize the space, to discourage intrusions and ensure privacy in the interior environment. |
| Wiring panel | The OSB panel is cut and shaped to allow wiring and the LED lighting, both inside the box and outside, in the platform). Cables are placed in the empty space under the platform structure. |
| Toilet panel | A floor tile covering characterizes this panel typology. Drain pipes are not inside the panel, but in an implemented cavity. It is possible to use washbasin and toilet on the same wall when there are in two adjacent boxes. |
| Average Number of Users per Year (2020–2021) | Main Provenience (More than 10%) | Type of Care | |
|---|---|---|---|
| City of Trento, several association | 1114 | - | General medicine 35% Gynecology 8% Certifications of violence 3% Visits to inadequate low-threshold aid facilities 41% Infirmary 7% Other 6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brunoro, S.; Mensi, L. A Modular Structure for Immediate and Transitory Interventions to Guarantee Access to Basic Healthcare in Italy. Sci 2023, 5, 17. https://doi.org/10.3390/sci5020017
Brunoro S, Mensi L. A Modular Structure for Immediate and Transitory Interventions to Guarantee Access to Basic Healthcare in Italy. Sci. 2023; 5(2):17. https://doi.org/10.3390/sci5020017
Chicago/Turabian StyleBrunoro, Silvia, and Lisa Mensi. 2023. "A Modular Structure for Immediate and Transitory Interventions to Guarantee Access to Basic Healthcare in Italy" Sci 5, no. 2: 17. https://doi.org/10.3390/sci5020017