The Mental Health State of Canadian Ophthalmologists during the COVID-19 Pandemic: A Survey-Based Study and Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Mental Health Questionnaires
2.3. Literature Review
2.4. Statistical Analysis
3. Results
3.1. Respondent Baseline Characteristics
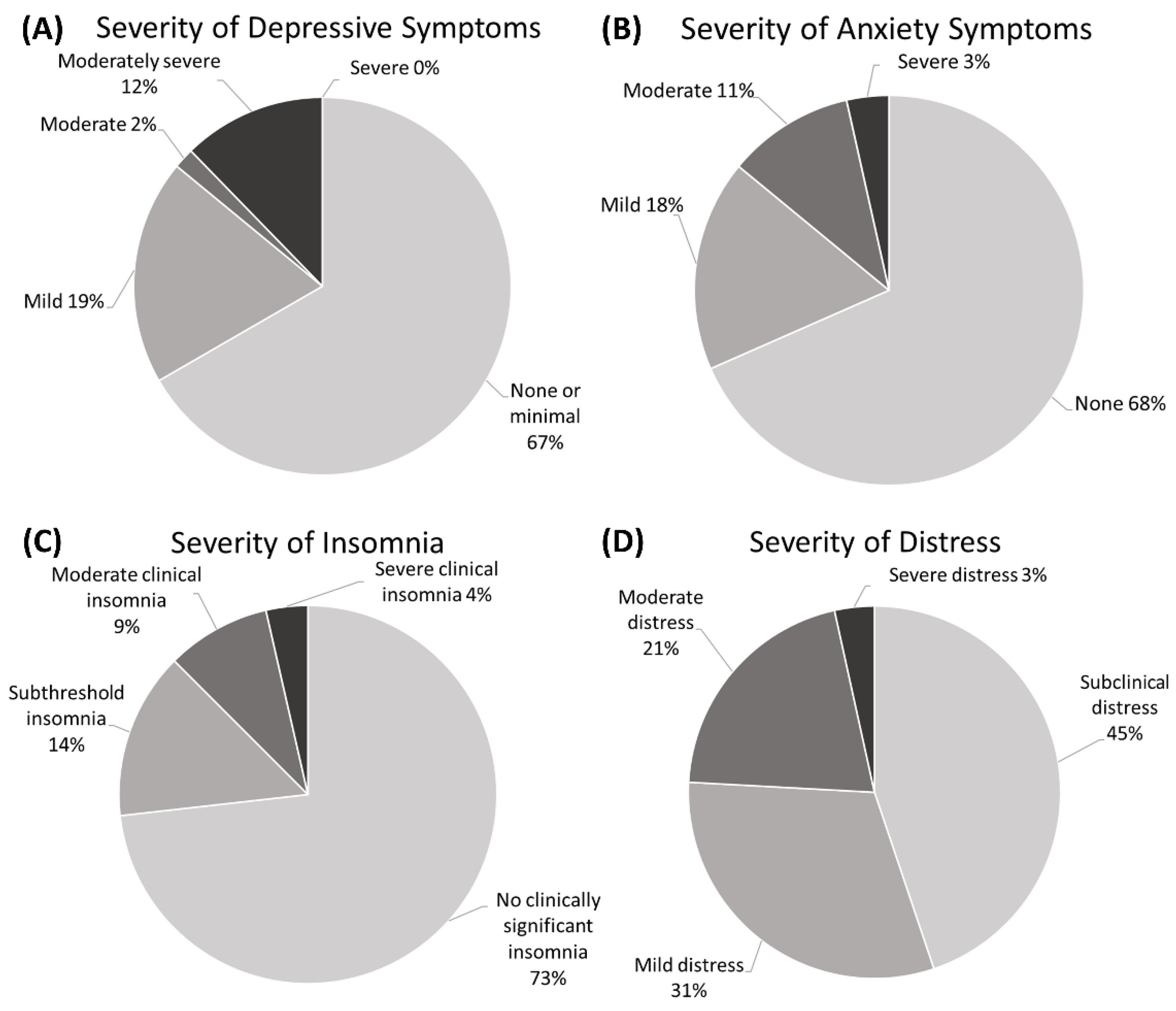
3.2. Mental Health Questionnaire Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Green, A. Li Wenliang. Lancet 2020, 395, 682. [Google Scholar] [CrossRef]
- Kuo, I.C.; O’Brien, T.P. COVID-19 and ophthalmology: An underappreciated occupational hazard. Infect. Control. Hosp. Epidemiol. 2020, 41, 1207–1208. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Li, Y.; Li, X.-Y.; Zhao, Y.-J.; Cheung, T.; Ungvari, G.S.; Li, M.; An, F.-R.; Xiang, Y.-T. Prevalence of Fatigue and Its Association With Quality of Life Among Frontline Clinicians in Ophthalmology and Otolaryngology Departments During the COVID-19 Pandemic. Front. Psychiatry 2021, 12, 678917. [Google Scholar] [CrossRef] [PubMed]
- Almater, A.I.; Tobaigy, M.F.; Younis, A.S.; Alaqeel, M.K.; Abouammoh, M.A. Effect of 2019 Coronavirus Pandemic on Ophthalmologists Practicing in Saudi Arabia: A Psychological Health Assessment. Middle E. Afr. J. Ophthalmol. 2020, 27, 79–85. [Google Scholar] [CrossRef]
- Khanna, R.C.; Honavar, S.G.; Metla, A.L.; Bhattacharya, A.; Maulik, P.K. Psychological impact of COVID-19 on ophthalmologists-in-training and practising ophthalmologists in India. Indian J. Ophthalmol. 2020, 68, 994–998. [Google Scholar] [CrossRef]
- Parija, S.; Parida, S.P.; Dash, N.; Mohapatra, K.; Kumar, P.S.S. A study on knowledge, attitudes, and mental health status of patients and health care workers of ophthalmology during COVID-19 post-lockdown phase at a tertiary hospital. Indian J. Ophthalmol. 2021, 69, 2542–2543. [Google Scholar] [CrossRef]
- Durmaz Engin, C.; Senel Kara, B.; Ozturk, T.; Dadas, O.F. The Impact of COVID-19 Pandemic on Practice Patterns and Psychological Status of Ophthalmologists in Turkey. Cureus 2021, 13, e16614. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, C.A.; Varela-Agra, M.; Pérez-Roldán, L.; Álvarez-Reguera, A.; Martínez-Reglero, C.; Campo-Gesto, A. Impact of COVID-19 on Eye Care in Spain during the First Phase of the Pandemic. J. Clin. Med. 2021, 10, 4087. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Brunet, A.; St-Hilaire, A.; Jehel, L.; King, S. Validation of a French Version of the Impact of Event Scale-Revised. Can. J. Psychiatry 2003, 48, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.S. The Impact of Event Scale: Revised. In Cross-Cultural Assessment of Psychological Trauma and PTSD; Wilson, J.P., Tang, C.S., Eds.; International and Cultural Psychology Series; Springer US: Boston, MA, USA, 2007; pp. 219–238. ISBN 978-0-387-70990-1. [Google Scholar]
- Kang, L.; Ma, S.; Chen, M.; Yang, J.; Wang, Y.; Li, R.; Yao, L.; Bai, H.; Cai, Z.; Xiang Yang, B.; et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav. Immun. 2020, 87, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the Impact of Event Scale—Revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef]
- Kawamura, N.; Kim, Y.; Asukai, N. Suppression of Cellular Immunity in Men With a Past History of Posttraumatic Stress Disorder. AJP 2001, 158, 484–486. [Google Scholar] [CrossRef]
- Grover, R.; Dua, P.; Juneja, S.; Chauhan, L.; Agarwal, P.; Khurana, A. “Depression, Anxiety and Stress” in a Cohort of Registered Practicing Ophthalmic Surgeons, Post Lockdown during COVID-19 Pandemic in India. Ophthalmic Epidemiol. 2021, 28, 322–329. [Google Scholar] [CrossRef]
- Erdem, B.; Gok, M.; Bostan, S. The evolution of the changes in the clinical course: A multicenter survey-related impression of the ophthalmologists at the peak of the COVID-19 pandemic in Turkey. Int. Ophthalmol. 2021, 41, 1261–1269. [Google Scholar] [CrossRef] [PubMed]
- Kavadarlı, I.; Mutlu, M. Effects of the COVID-19 Pandemic on Turkish Ophthalmologists. Turk. J. Ophthalmol. 2021, 51, 95–101. [Google Scholar] [CrossRef]
- Scott, D.A.R.; Hadden, P.W.; Wilson, G.A. Impact of the COVID-19 pandemic lockdown on public sector ophthalmic work by New Zealand’s ophthalmologists. N. Z. Med. J. 2021, 134, 120–127. [Google Scholar]
- Szigiato, A.-A.; Palakkamanil, M.; Aubin, M.-J.; Ziai, S. Canadian ophthalmology resident experience during the COVID-19 pandemic. Can. J. Ophthalmol. 2021, 56, e42–e44. [Google Scholar] [CrossRef]
- Mishra, D.; Nair, A.G.; Gandhi, R.A.; Gogate, P.J.; Mathur, S.; Bhushan, P.; Srivastav, T.; Singh, H.; Sinha, B.P.; Singh, M.K. The impact of COVID-19 related lockdown on ophthalmology training programs in India—Outcomes of a survey. Indian J. Ophthalmol. 2020, 68, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Alahmadi, A.S.; Alhatlan, H.M.; Bin Helayel, H.; Khandekar, R.; Al Habash, A.; Al-Shahwan, S. Residents’ Perceived Impact of COVID-19 on Saudi Ophthalmology Training Programs-A Survey. Clin. Ophthalmol. 2020, 14, 3755–3761. [Google Scholar] [CrossRef]
- El-Saied, H.M.A.; Salah Eddin Abdelhakim, M.A. Impact of COVID-19 Pandemic on Young Ophthalmologists in Cairo University Hospitals. Semin. Ophthalmol. 2020, 35, 296–306. [Google Scholar] [CrossRef] [PubMed]
- Gustavsson, K.; Goetz-Kundera, Z.; Flaga-Łuczkiewicz, M.; Wichniak, A. Which Aspects of Work Safety Satisfaction Are Important to Mental Health of Healthcare Workers during COVID-19 Pandemic in Poland? Int. J. Environ. Res. Public Health 2023, 20, 2870. [Google Scholar] [CrossRef]
- Viviers, S.; Lachance, L.; Maranda, M.-F.; Ménard, C. Burnout, psychological distress, and overwork: The case of Quebec’s ophthalmologists. Can. J. Ophthalmol. 2008, 43, 535–546. [Google Scholar] [CrossRef]
- Dub, N.; Konopińska, J.; Obuchowska, I.; Lisowski, Ł.; Dmuchowska, D.A.; Rękas, M. The Impact of the COVID-19 Pandemic on Ophthalmology Residents: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 11567. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Greenberg, N.; Weston, D.; Hall, C.; Caulfield, T.; Williamson, V.; Fong, K. Mental health of staff working in intensive care during COVID-19. Occup. Med. 2021, 71, kqaa220. [Google Scholar] [CrossRef]
- Luo, D.; Liu, Q.; Chen, Q.; Huang, R.; Chen, P.; Yang, B.X.; Liu, Z. Mental Health Status of the General Public, Frontline, and Non-frontline Healthcare Providers in the Early Stage of COVID-19. Front. Psychiatry 2021, 12, 288. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, A.; Paleri, V.; Bennett, R.; Paleri, V. Impact of COVID-19 on the mental health of surgeons and coping strategies. Head Neck 2020, 42, 1638–1644. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study Authors | Country | # Ophthalmologists | Anxiety/Stress | Depression | Fatigue/Insomnia |
|---|---|---|---|---|---|
| [3] | China | 2155 (+1757 otolaryngologists) | NA | PHQ-9 ≥ 5 in 33.2% overall | Clinically relevant fatigue (≥4/10) in 52.4% |
| [4] | Saudi Arabia | 107 (66 residents) | GAD-7 ≥ 5 in 46.7%; GAD-7 ≥ 7 in 38.3%; PSS-10 ≥ 14 (moderate to high stress) in 71.9% | PHQ-9 ≥ 5 in 50.6%; PHQ-9 ≥ 10 in 29.0% | ISI ≥ 8 in 44.9%; ISI ≥ 15 in 15% |
| [5] | India | 2355 (475 in training) | NA | Mean PHQ-9 3.98 ± 4.65; PHQ-9 ≥ 5 in 32.6%; PHQ-9 ≥ 10 in 11.2% | NA |
| [6] | India | 40 HCW and 200 patients in ophthalmology | NA | Mean PHQ-9 9.50 ± 4.77 in HCW vs. 5.98 ± 3.49 in patients (p = 0.001); PHQ-9 ≥ 5 in 80% and PHQ-9 ≥ 10 in 52.5% of HCW | NA |
| [19] | India | 144 | DASS-A ≥ 8 in 51.4%; DASS-S ≥ 15 in 13.9% | DASS-D ≥ 10 in 52.7% | NA |
| [20] | Turkey | 121 | At least mild anxiety in 36.4% using Beck anxiety scale | NA | NA |
| [21] | Turkey | 161 (71.3% consultants) | Anxiety mentioned by 91.3%, mostly from transmission risk to family members (83.1%) | NA | NA |
| [7] | Turkey | 360 | DASS-A ≥ 8 in 56.9%; DASS-S ≥ 15 in 43% | DASS-D ≥ 10 in 65% | ISI ≥ 8 in 46.9% |
| [8] | Spain | 328 (108 trainees) | Increased anxiety levels in 58.8%; start of anxiolytic or sleep-inducing treatment in 12.5% | NA | Worsened sleep quality in 53.7% |
| [22] | New Zealand | 57 | No reported significant impact on mental health from the COVID-19 lockdown overall: about 30% reported negative impact, while about 37% reported a positive impact | ||
| [23] | Canada | 102 residents | Higher anxiety in 56.9% | NA | NA |
| [24] | India | 716 trainees | Increased stress levels in 54.8% during the lockdown | 46.5% were unhappy during the lockdown | NA |
| [25] | Saudi Arabia | 108 residents | NA | PHQ-9 ≥ 5 in 92.6%; PHQ-9 ≥ 10 in 49.1% | NA |
| [26] | Egypt | 79 young ophthalmologists and residents | 7.6% extremely anxious regarding psychological concerns about the pandemic | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hébert, M.; Bouhout, S.; Freeman, E.E.; Aubin, M.-J. The Mental Health State of Canadian Ophthalmologists during the COVID-19 Pandemic: A Survey-Based Study and Review. Vision 2023, 7, 23. https://doi.org/10.3390/vision7010023
Hébert M, Bouhout S, Freeman EE, Aubin M-J. The Mental Health State of Canadian Ophthalmologists during the COVID-19 Pandemic: A Survey-Based Study and Review. Vision. 2023; 7(1):23. https://doi.org/10.3390/vision7010023
Chicago/Turabian StyleHébert, Mélanie, Soumaya Bouhout, Ellen E. Freeman, and Marie-Josée Aubin. 2023. "The Mental Health State of Canadian Ophthalmologists during the COVID-19 Pandemic: A Survey-Based Study and Review" Vision 7, no. 1: 23. https://doi.org/10.3390/vision7010023