1. Introduction
Cuff tear arthropathy (CTA) is one of the secondary forms of shoulder arthritis and the main indication for reverse shoulder arthroplasty (RSA). Despite the extensive knowledge of this kind of pathology and its prevalence according to age and sex, there is still little information about the natural progression and development of CTA. Furthermore, no studies exist on the differences in the morphologies of CTA between females and males as well as younger and older patients. Therefore, we analyzed the age- and gender-related morphological differences of CTA in order to gain deeper insight into CTA progression.
In the nineteenth century, the pathology was commonly known as chronic rheumatic arthritis, until in 1983, Neer et al. first introduced the term “arthropathy of the rotator cuff” [
1]. Several theories explained the development of CTA and its close relation to rotator cuff tear (RCT) [
2,
3,
4,
5,
6]. Rotator cuff deficiency results in the humeral head moving position into an anteroinferior subluxation and therefore leads to arthritic changes, as Walch et al. have shown [
7]. In 2020, Van Parys et al. found a difference of the coracoacromial complex between CTA, glenohumeral osteoarthritis and non-pathological shoulders [
8]. However, despite the well-known pathogenesis of CTA and the underlying mechanisms of a rotator cuff tear, the question of why patients develop different glenoid defects remains unclear. To date, there has been no scientific examination of the reasons for these differences. Thus, the purpose of this study was to investigate possible age- and gender-related irregularities of the bony structures and soft tissue of the glenohumeral joint, which would lead to an increased understanding of the background of CTA.
The purpose of this study was to radiologically investigate patients suffering from CTA in terms of morphology depending on age or gender.
2. Materials and Methods
This retrospective cohort study was conducted to investigate age- and gender-related differences in CTA morphology. Patients who received RTSA for CTA in the period between January 2009 and September 2019 with preoperative computed tomography and magnetic resonance imaging were included. The exclusion criteria were: (1) fractures affecting the glenohumeral joint; (2) pre-existing rheumatic disorders; and (3) revision surgery. A total of 309 patients, adding up to 342 shoulder treatments, from one single institution, were included after screening for eligibility. Approval from the Institutional Review Board was obtained prior to the investigation (1018/2020). Informed consent from all subjects involved in the study was provided.
Preoperative X-rays, computed tomography and magnetic resonance images of every patient were assessed using common classifications. These were from the works of: (1) Seebauer [
9] and (2) Hamada [
10] (classifications for rotator cuff tear arthropathy); (3) Favard [
11] and (4) Walch [
12] (classifications for glenoid configuration); and (5) Habermeyer [
13], (6) Goutallier [
14], (7) Thomazeau [
15] and (8) Patte [
16] (classifications for muscular conditions). Additionally, (9) the acromiohumeral index (AHI) [
17], (10) the acromiohumeral distance (AHD), (11) the critical shoulder angle (CSA) [
18] and (12) the version of the glenoid were measured to evaluate morphologic differences between both groups.
Patients were then assigned into groups according to gender, resulting in one female (n = 257) and one male group (n = 85). For the assessment of age-related differences, patients were divided into younger and older age groups. The divisor was set as the median age of the trial population at the time of surgery (74.5 years). The twelve different classifications and measurements were then compared to determine differences.
Data were analyzed using IBM SPSS Statistics (Windows, 64-bit, version 23.0; IBM Corp., Armonk, NY, USA). Metrical variables were tested using the Kolmogorov–Smirnov test to check for normal distribution. A two-way ANOVA and Mann–Whitney U test were then performed to analyze metrical dependent variables. To evaluate the nominal variables, a Chi-square test was performed. The statistical significance was set at p < 0.05. The effect size was calculated for significant differences (r < 0.3 = low effect size; 0.3 ≤ r ≤ 0.5 = medium effect size; r > 0.5 = large effect size).
3. Results
In total, 342 shoulders were examined in this study, of which 133 were left and 209 were right shoulders. There were 257 female and 85 male shoulders. The demographic data for each group are shown in
Table 1. A significant difference was found between both gender groups—female patients were significantly older than male patients (r = 0.18)—and between both age groups—the proportion of female patients was higher in the older age group (r = 0.12). While X-rays were available for 300 shoulders, MRI was performed preoperatively on 166 shoulders and a CT scan on 77 shoulders.
Our analysis of the patients’ data is shown in
Table 2. When comparing female with male patients, fatty degeneration according to Goutallier showed significantly lower grading in the males and higher grading in the female population (
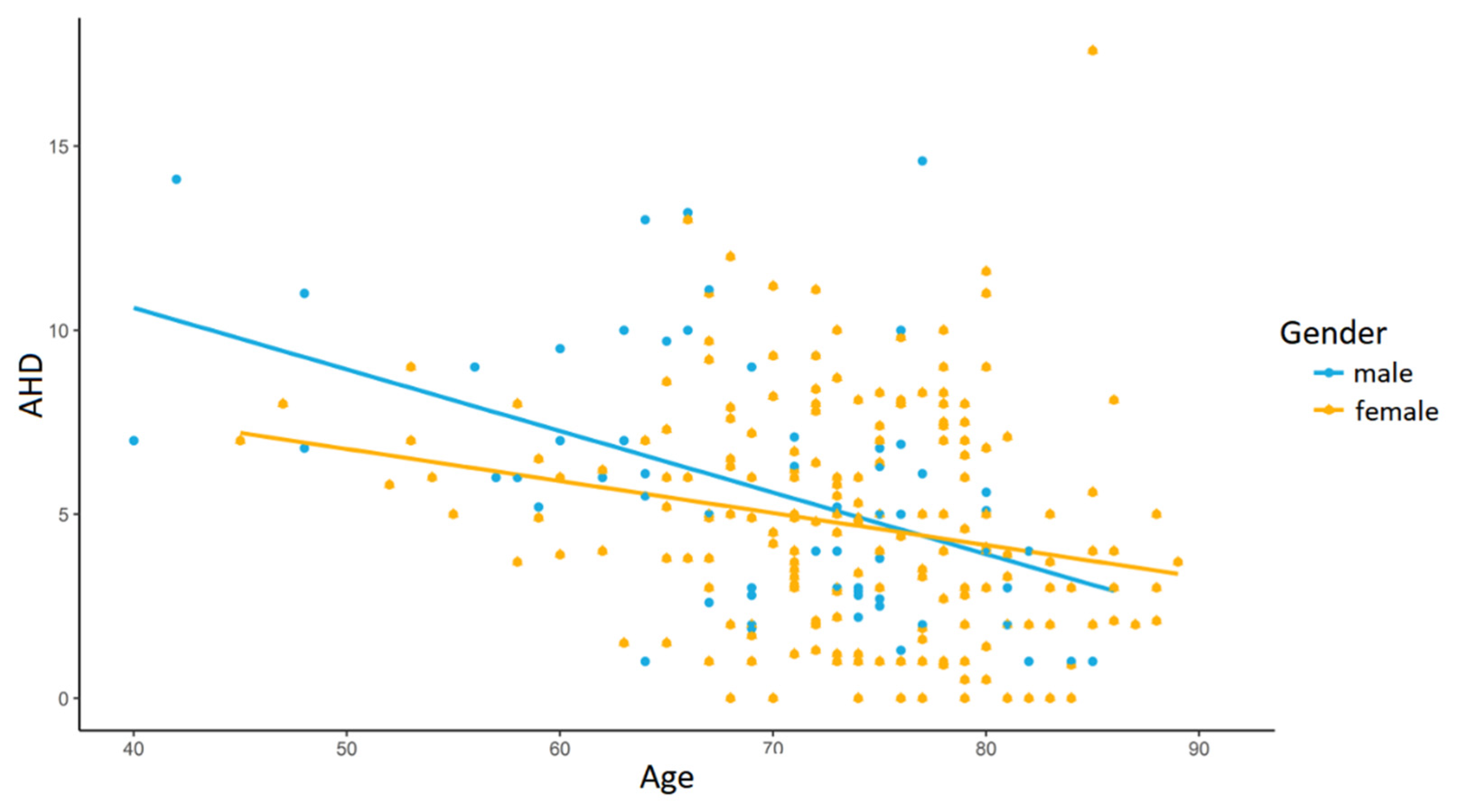
p = 0.006; r = 0.29). The other data did not show any significant difference; however, men tended to have greater AHD and the glenoid version, although both were not significant.
On the other hand, the analysis according to the age groups showed several significant differences. Firstly, a greater AHD was measured in younger patients’ shoulders (
p = 0.001; r = 0.11;
Figure 1). Secondly, CTA classified according to Seebauer [
9] showed a larger extent of progression among the older population, with more patients graded at 2A and 2B (
p = 0.006; r = 0.21). Thirdly, greater damage of the rotator cuff combined with more retraction and higher fatty infiltration in older compared to younger patients was detected—all four classifications of Habermeyer [
13] (
p < 0.001; r = 0.31), Goutallier [
14] (
p = 0.001; r = 0.33), Thomazeau [
15] (
p = 0.037; r = 0.21) and Patte [
16] (
p = 0.003; r = 0.29) showed significantly greater damage of the rotator cuff in older patients.
4. Discussion
In this study, we evaluated 309 patients (342 shoulders) with CTA according to popular classifications. The aim of this study was to investigate possible age- and gender-related irregularities of the bony structures or the soft tissue of the glenohumeral joint to better understand CTA.
As expected, our data confirmed the natural progression of cuff tear arthropathy over time. The examination considering age showed significant differences of AHD, the progression of the CTA, according to the classification of Seebauer, and greater damage of the rotator cuff combined with more retraction and higher fatty infiltration in older patients. The younger patients had a significantly greater AHD, lower stages in the Seebauer classification (more patients graded 2A and 2B) and less soft tissue damage than the older population according to Habermeyer, Goutallier, Thomazeau and Patte. These results support the widely known principle of the natural degeneration of the cuff tear in older people and its progression over time.
Furthermore, we found some interesting differences between the female and male populations. The examined female shoulders showed significantly more fatty degeneration of the rotator cuff muscles than the male ones according to Goutallier’s classification (
p = 0.006). We conducted a power calculation according to Hoenig and Heisey [
19], which showed a power of >80%.
We suggest that this is related to a higher mean age of the female patients and hence greater progression of fatty degeneration. A study conducted in 2010 by Oh et al. concluded that “older age is correlated with higher fatty degeneration grade”, supporting this theory [
20]. As described, the patient population was significantly different regarding age at surgery; male patients were on average 70.11 years old, whereas the female patients were on average 74.37 years old. No other gender-related differences were found, except for fatty degeneration, and female and male patients showed the same progression of CTA when we saw them for the first time. However, despite the younger mean age, the AHD tends to be lower in male patients. Gelvosa et al. suggested gender-related differences with regard to AHD, but stated that rather female patients had a lower acromiohumeral distance [
21].
Our trial included 257 female and 85 male shoulders. This appears to be consistent with the existing literature, which states that the prevalence of CTA is higher among women than men [
22,
23]. We can only assume that this result is of multifactorial genesis and highly dependent on local conditions, including retirement age, life expectancy and the distribution of the population, since the prevalence of RCT shows the opposite trend, with men making up the majority of the patient population [
24,
25].
The data suggest that female and male patients both suffer from progressing CTA to the same extent, but female patients receive surgery at an overall higher age due to their superior health conditions compared to male patients in the same age groups. However, this is not statistically significant; hence, this only represents the personal opinion of the authors.
Our study had several strengths. With 342 shoulders, a large number of patients were evaluated in this study. Furthermore, data over a period of ten years were analyzed. Internationally respected and commonly used classification methods were used to make a good comparison between our results and the results of existing and future studies.
Nevertheless, our study did have some limitations too. The trial was conducted retrospectively, and only radiographic data were analyzed. Neither pre- nor postoperative clinical scores were included. Due to its retrospective study design, many patients only had either X-rays and MRI or X-rays and a CT scan. Finally, our study lacked a control group.
5. Conclusions
Summarizing the findings, female patients account for the majority of RSA cases due to CTA. Female patients undergo the surgery at a higher age. CTA seems to be progressive, which is underlined by our findings that there were significantly higher gradings in six out of 12 classifications in the older population.
Author Contributions
Conceptualization, M.S.G., J.H., P.S. and R.O.; methodology, M.S.G., P.B. and R.O.; formal analysis, M.S.G. and P.B.; investigation, P.B.; data curation, M.S.G. and P.B.; writing—original draft preparation, M.S.G. and M.B.; writing—review and editing, M.S.G., P.B., J.H., P.S. and R.O.; supervision, J.H. and R.O.; project administration, M.S.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Upper Austria (protocol code 1018/2020, 17 April 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data and materials this study is based on are available from the corresponding author, R.O.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Brorson, S. Cuff tear arthropathy in the nineteenth century: “Chronic rheumatic arthritis” with “partial luxation upwards” of the humeral head. Int. Orthop. 2019, 43, 2415–2423. [Google Scholar] [CrossRef] [PubMed]
- Neer, C.S.; Craig, E.V.; Fukuda, H. Cuff-tear arthropathy. J. Bone Jt. Surg. Am. 1983, 65, 1232–1244. [Google Scholar] [CrossRef] [Green Version]
- Mccarty, D.J.; Halverson, P.B.; Carrera, G.F.; Brewer, B.J.; Kozin, F. “Milwaukee shoulder”—Association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. Arthritis Rheum. 1981, 24, 464–473. [Google Scholar] [CrossRef]
- Collins, D.N.; Harryman, D.T.I. Arthroplasty for arthritis and rotator cuff deficiency. Orthop. Clin. N. Am. 1997, 28, 225–239. [Google Scholar] [CrossRef] [PubMed]
- Silldorff, M.D.; Choo, A.D.; Choi, A.J.; Lin, E.; Carr, J.A.; Lieber, R.L.; Lane, J.G.; Ward, S.R. Effect of Supraspinatus Tendon Injury on Supraspinatus and Infraspinatus Muscle Passive Tension and Associated Biochemistry. J. Bone Jt. Surg. 2014, 96, e175. [Google Scholar] [CrossRef] [Green Version]
- Gibbons, M.C.; Sato, E.J.; Bachasson, D.; Cheng, T.; Azimi, H.; Schenk, S.; Engler, A.J.; Singh, A.; Ward, S.R. Muscle architectural changes after massive human rotator cuff tear. J. Orthop. Res. 2016, 34, 2089–2095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walch, G.; Collotte, P.; Raiss, P.; Athwal, G.S.; Gauci, M.O. The Characteristics of the Favard E4 Glenoid Morphology in Cuff Tear Arthropathy: A CT Study. J. Clin. Med. 2020, 9, 3704. [Google Scholar] [CrossRef]
- Van Parys, M.; Alkiar, O.; Naidoo, N.; Van Tongel, A.; De Wilde, L. Three-dimensional evaluation of scapular morphology in primary glenohumeral arthritis, rotator cuff arthropathy, and asymptomatic shoulders. J. Shoulder Elb. Surg. 2021, 30, 1803–1810. [Google Scholar] [CrossRef] [PubMed]
- Visotsky, J.L.; Basamania, C.; Seebauer, L.; Rockwood, C.A.; Jensen, K.L. Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J. Bone Jt. Surg. Am. 2004, 86-A (Suppl. 2), 35–40. [Google Scholar] [CrossRef]
- Brolin, T.J.; Updegrove, G.F.; Horneff, J.G. Classifications in Brief: Hamada Classification of Massive Rotator Cuff Tears. Clin. Orthop. Relat. Res. 2017, 475, 2819–2823. [Google Scholar] [CrossRef] [PubMed]
- Lévigne, C.; Boileau, P.; Favard, L.; Garaud, P.; Molé, D.; Sirveaux, F.; Walch, G. Scapular notching in reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2008, 17, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Bercik, M.J.; Kruse, K.; Yalizis, M.; Gauci, M.O.; Chaoui, J.; Walch, G. A modification to the Walch classification of the glenoid in primary glenohumeral osteoarthritis using three-dimensional imaging. J. Shoulder Elb. Surg. 2016, 25, 1601–1606. [Google Scholar] [CrossRef]
- Habermeyer, P.; Magosch, P.; Lichtenberg, S. Classifications and Scores of the Shoulder; Springer: Berlin/Heidelberg, Germany, 2006; ISBN 978-3-540-24350-2. [Google Scholar]
- Goutallier, D.; Postel, J.-M.; Bernageau, J.; Lavau, L.; Voisin, M.-C. Fatty Muscle Degeneration in Cuff Ruptures. Pre- and Postoperative Evaluation by CT Scan. Clin. Orthop. Relat. Res. 1994, 304, 78–83. [Google Scholar] [CrossRef]
- Thomazeau, H.; Rolland, Y.; Lucas, C.; Duval, J.; Langlais, F. Atrophy of the supraspinatus belly Assessment by MRI in 55 patients with rotator cuff pathology. Acta Orthop. Scand. 1996, 67, 264–268. [Google Scholar] [CrossRef]
- Patte, D. Classification of rotator cuff lesions. Clin. Orthop. Relat. Res. 1990, 254, 81–86. [Google Scholar] [CrossRef]
- Nyffeler, R.W.; Werner, C.M.L.; Sukthankar, A.; Schmid, M.R.; Gerber, C. Association of a large lateral extension of the acromion with rotator cuff tears. J. Bone Jt. Surg. Ser. A 2006, 88, 800–805. [Google Scholar] [CrossRef]
- Moor, B.K.; Bouaicha, S.; Rothenfluh, D.A.; Sukthankar, A.; Gerber, C. Is there an association between the individual anatomy of the scapula and the development of rotator cuff tears or osteoarthritis of the glenohumeral joint? A radiological study of the critical shoulder angle. Bone Jt. J. 2013, 95 B, 935–941. [Google Scholar] [CrossRef]
- Hoenig, J.M.; Heisey, D.M. The abuse of power: The pervasive fallacy of power calculations for data analysis. Am. Stat. 2001, 55, 19–24. [Google Scholar] [CrossRef]
- Han, O.J.; Hoon, K.S.; Kang, J.Y.; Hee, O.C.; Gong, H.S. Effect of Age on Functional and Structural Outcome after Rotator Cuff Repair. Am. J. Sports Med. 2010, 38, 672–678. [Google Scholar] [CrossRef]
- Gelvosa, M.N.; Azarcon, A. Gender and laterality differences on measurements of acromiohumeral distance (AHD) at rest and at shoulder abduction using musculoskeletal ultrasound in asymptomatic Filipino adults. Ann. Phys. Rehabil. Med. 2018, 61, e435–e436. [Google Scholar] [CrossRef]
- Feeley, B.T.; Gallo, R.A.; Craig, E.V. Cuff tear arthropathy: Current trends in diagnosis and surgical management. J. Shoulder Elb. Surg. 2009, 18, 484–494. [Google Scholar] [CrossRef] [PubMed]
- Petrillo, S.; Longo, U.G.; Papalia, R.; Denaro, V. Reverse shoulder arthroplasty for massive irreparable rotator cuff tears and cuff tear arthropathy: A systematic review. Musculoskelet. Surg. 2017, 101, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Minagawa, H.; Yamamoto, N.; Abe, H.; Fukuda, M.; Seki, N.; Kikuchi, K.; Kijima, H.; Itoi, E. Prevalence of symptomatic and asymptomatic rotator cuff tears in the general population: From mass-screening in one village. J. Orthop. 2013, 10, 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, A.; Takagishi, K.; Osawa, T.; Yanagawa, T.; Nakajima, D.; Shitara, H.; Kobayashi, T. Prevalence and risk factors of a rotator cuff tear in the general population. J. Shoulder Elbow Surg. 2010, 19, 116–120. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 

{kind=link}