
Blood-Transfusion Risk Factors after Intramedullary Nailing for Extracapsular Femoral Neck Fracture in Elderly Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample
2.3. Surgical Technique, Intervention, and Blood-Transfusion Criteria
2.4. Risk Factors and Outcome Measurements
2.5. Statistical Analysis
3. Results
3.1. Patients
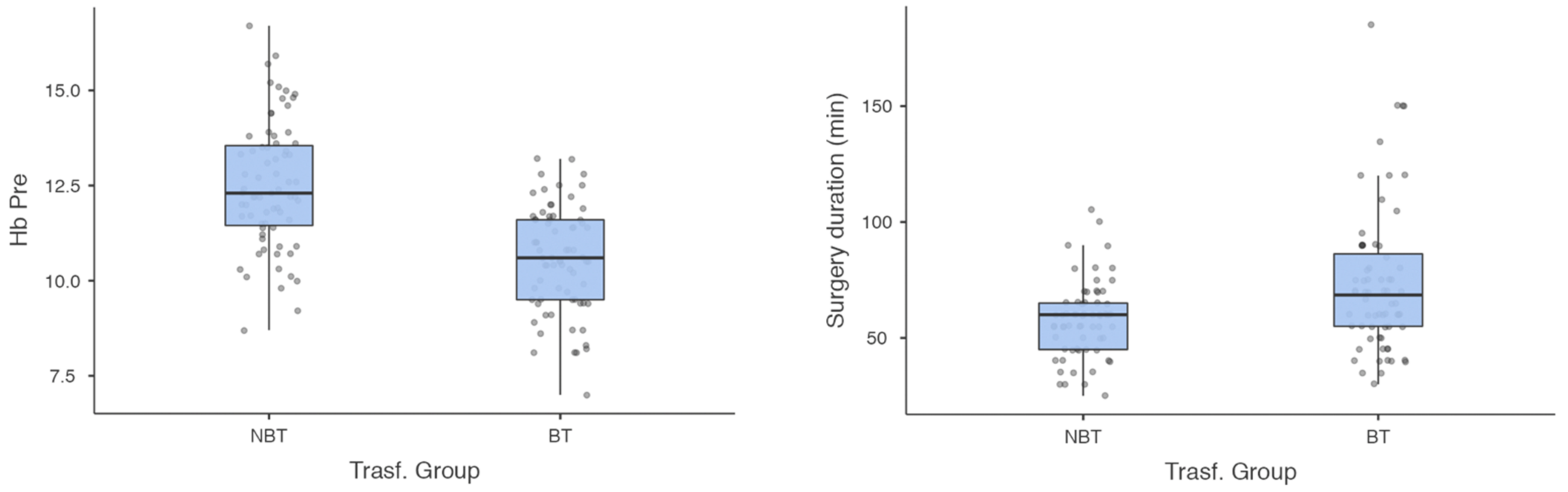
3.2. Group Comparisons
3.3. Relative-Risk Parameters
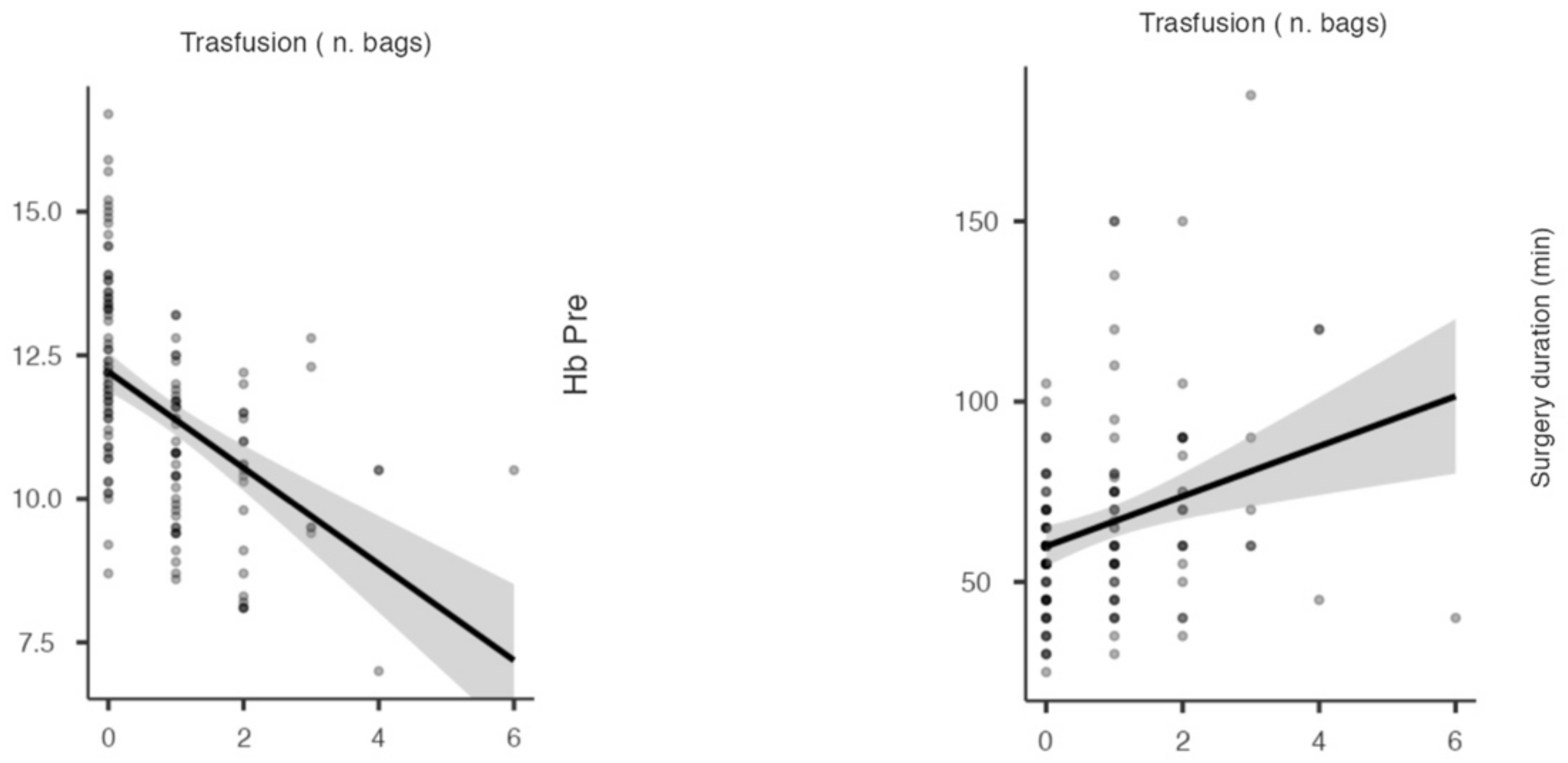
3.4. Cohort-Parameter Correlation
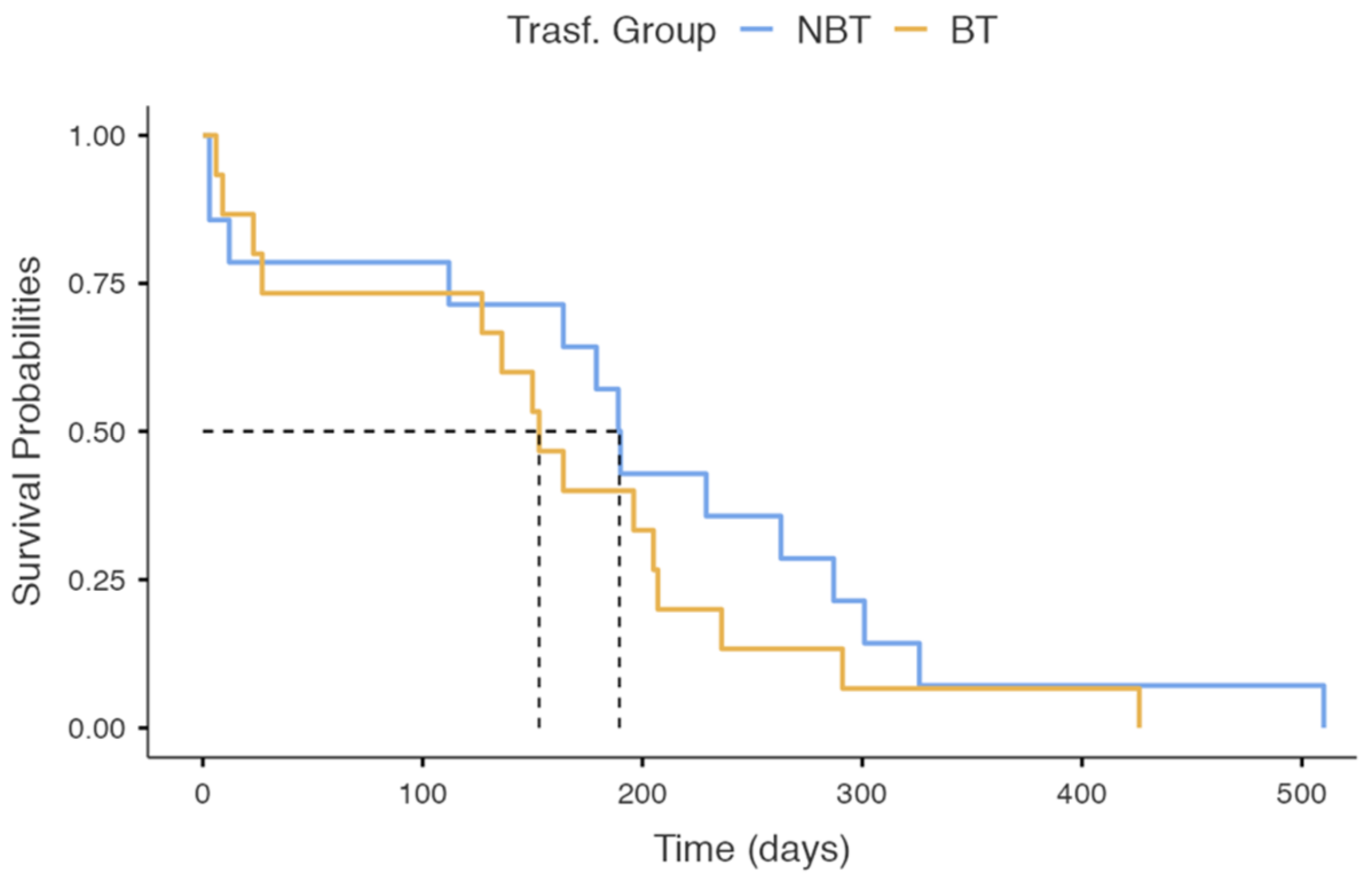
3.5. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bastard, C. Femoral neck fracture. Rev. Prat. 2019, 69, 1124–1128. [Google Scholar] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in Elderly People. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keene, G.S.; Parker, M.J.; Pryor, G.A. Mortality and Morbidity after Hip Fractures. BMJ 1993, 307, 1248–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sambrook, P.; Cooper, C. Osteoporosis. Lancet 2006, 367, 2010–2018. [Google Scholar] [CrossRef]
- Pillai, A.; Eranki, V.; Shenoy, R.; Hadidi, M. Age Related Incidence and Early Outcomes of Hip Fractures: A Prospective Cohort Study of 1177 Patients. J. Orthop. Surg. Res. 2011, 6, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamb, J.N.; Panteli, M.; Pneumaticos, S.G.; Giannoudis, P.V. Epidemiology of Pertrochanteric Fractures: Our Institutional Experience. Eur. J. Trauma Emerg. Surg. 2014, 40, 225–232. [Google Scholar] [CrossRef]
- Hoffmann, M.F.; Khoriaty, J.D.; Sietsema, D.L.; Jones, C.B. Outcome of Intramedullary Nailing Treatment for Intertrochanteric Femoral Fractures. J. Orthop. Surg. Res. 2019, 14, 360. [Google Scholar] [CrossRef]
- Roberts, K.C.; Brox, W.T.; Jevsevar, D.S.; Sevarino, K. Management of Hip Fractures in the Elderly. J. Am. Acad. Orthop. Surg. 2015, 23, 131–137. [Google Scholar] [CrossRef]
- Florschutz, A.V.; Langford, J.R.; Haidukewych, G.J.; Koval, K.J. Femoral Neck Fractures: Current Management. J. Orthop. Trauma 2015, 29, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Bennett-Guerrero, E.; Zhao, Y.; O’Brien, S.M.; Ferguson, T.B.; Peterson, E.D.; Gammie, J.S.; Song, H.K. Variation in Use of Blood Transfusion in Coronary Artery Bypass Graft Surgery. JAMA 2010, 304, 1568. [Google Scholar] [CrossRef] [Green Version]
- Testa, G.; Vescio, A.; Zuccalà, D.; Petrantoni, V.; Amico, M.; Russo, G.I.; Sessa, G.; Pavone, V. Diagnosis, Treatment and Prevention of Sarcopenia in Hip Fractured Patients: Where We Are and Where We Are Going: A Systematic Review. JCM 2020, 9, 2997. [Google Scholar] [CrossRef]
- Avola, M.; Mangano, G.R.A.; Testa, G.; Mangano, S.; Vescio, A.; Pavone, V.; Vecchio, M. Rehabilitation Strategies for Patients with Femoral Neck Fractures in Sarcopenia: A Narrative Review. JCM 2020, 9, 3115. [Google Scholar] [CrossRef] [PubMed]
- Lakstein, D.; Hendel, D.; Haimovich, Y.; Feldbrin, Z. Changes in the Pattern of Fractures of the Hip in Patients 60 Years of Age and Older between 2001 and 2010: A Radiological Review. Bone Jt. J. 2013, 95-B, 1250–1254. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.-Q.; Wang, L.-H.; Zhu, Y.-Q.; Xu, G.-H.; Shan, J.-B.; Huang, W.-C.; Wei, L.-H.; Zhou, F.-L.; Li, Y. Risk Factors of Perioperative Blood Transfusion in Elderly Patients with Femoral Intertrochanteric Fracture. Medicine 2020, 99, e19726. [Google Scholar] [CrossRef] [PubMed]
- Luangwaranyoo, A.; Suksintharanon, M.; Tangadulrat, P.; Iamthanaporn, K.; Hongnaparak, T.; Yuenyongviwat, V. Factors for Blood Transfusions Following Hemi Hip Arthroplasty for Patients With Femoral Neck Fracture. Geriatr. Orthop. Surg. Rehabil. 2020, 11, 215145932097299. [Google Scholar] [CrossRef] [PubMed]
- Nagra, N.S.; van Popta, D.; Whiteside, S.; Holt, E.M. An Analysis of Postoperative Hemoglobin Levels in Patients with a Fractured Neck of Femur. Acta Orthop. Traumatol. Turc. 2016, 50, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.-Q.; Chen, L.-Y.; Jiang, B.-J.; Zhao, Y.-M. Development of a Nomogram for Predicting Blood Transfusion Risk After Hemiarthroplasty for Femoral Neck Fractures in Elderly Patients. Med. Sci. Monit. 2020, 26, e920255-1–e920255-7. [Google Scholar] [CrossRef] [PubMed]
- D’Amore, T.; Loewen, M.; Gorczyca, M.T.; Judd, K.; Ketz, J.P.; Soles, G.; Gorczyca, J.T. Rethinking Strategies for Blood Transfusion in Hip Fracture Patients. OTA Int. Open Access J. Orthop. Trauma 2020, 3, e083. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.-Y.; Cha, Y.-H.; Yoo, J.-I.; Oh, T.; Kim, J.-T.; Park, C.H.; Choy, W.-S.; Ha, Y.-C.; Koo, K.-H. Blood Transfusion for Elderly Patients with Hip Fracture: A Nationwide Cohort Study. J. Korean Med. Sci. 2020, 35, e313. [Google Scholar] [CrossRef] [PubMed]
- Goh, E.L.; Lerner, R.G.; Achten, J.; Parsons, N.; Griffin, X.L.; Costa, P.M.L. Complications Following Hip Fracture: Results from the World Hip Trauma Evaluation Cohort Study. Injury 2020, 51, 1331–1336. [Google Scholar] [CrossRef] [PubMed]
- Kamiloski, V. Analysis of the Hemoglobin Level Drop in Patients with Hip Fracture After Admission. ACC 2017, 56, 645–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, H.; Zhang, Y.; Wang, H.; Sun, T.; Sun, Q. Comparison of Perioperative Hidden Blood Loss for Intertrochanteric Fractures in the Elderly by Different Intramedullary Fixations: A Randomized Controlled Study Protocol. Medicine 2020, 99, e21666. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Wang, T.; Di, L.; Hu, W.; Wang, J. Comparison of Intramedullary and Extramedullary Fixation of Stable Intertrochanteric Fractures in the Elderly: A Prospective Randomised Controlled Trial Exploring Hidden Perioperative Blood Loss. BMC Musculoskelet. Disord. 2016, 17, 475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, X.; He, S.; Li, Z.; Li, Q. Quantification and Influencing Factors of Perioperative Hidden Blood Loss during Intramedullary Fixation for Intertrochanteric Fractures in the Elderly. Arch. Orthop. Trauma Surg. 2020, 140, 1339–1348. [Google Scholar] [CrossRef]
- Greenhalgh, M.S.; Gowers, B.T.V.; Iyengar, K.P.; Adam, R.F. Blood Transfusions and Hip Fracture Mortality—A Retrospective Cohort Study. J. Clin. Orthop. Trauma 2021, 21, 101506. [Google Scholar] [CrossRef]
- Arshi, A.; Lai, W.C.; Iglesias, B.C.; McPherson, E.J.; Zeegen, E.N.; Stavrakis, A.I.; Sassoon, A.A. Blood Transfusion Rates and Predictors Following Geriatric Hip Fracture Surgery. HIP Int. 2021, 31, 272–279. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Epidemiology 2007, 18, 800–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carson, J.L.; Guyatt, G.; Heddle, N.M.; Grossman, B.J.; Cohn, C.S.; Fung, M.K.; Gernsheimer, T.; Holcomb, J.B.; Kaplan, L.J.; Katz, L.M.; et al. Clinical Practice Guidelines From the AABB: Red Blood Cell Transfusion Thresholds and Storage. JAMA 2016, 316, 2025. [Google Scholar] [CrossRef]
- Yombi, J.C.; Putineanu, D.C.; Cornu, O.; Lavand’homme, P.; Cornette, P.; Castanares-Zapatero, D. Low Haemoglobin at Admission Is Associated with Mortality after Hip Fractures in Elderly Patients. Bone Jt. J. 2019, 101-B, 1122–1128. [Google Scholar] [CrossRef]
- Carson, J.L. Perioperative Blood Transfusion and Postoperative Mortality. JAMA 1998, 279, 199. [Google Scholar] [CrossRef] [Green Version]
- Johnston, P.; Wynn-Jones, H.; Chakravarty, D.; Boyle, A.; Parker, M.J. Is Perioperative Blood Transfusion a Risk Factor for Mortality or Infection After Hip Fracture? J. Orthop. Trauma 2006, 20, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Brunskill, S.J.; Millette, S.L.; Shokoohi, A.; Pulford, E.; Doree, C.; Murphy, M.F.; Stanworth, S. Red Blood Cell Transfusion for People Undergoing Hip Fracture Surgery. Cochrane Database Syst. Rev. 2015, 4, CD009699. [Google Scholar] [CrossRef] [PubMed]
- Gregersen, M.; Damsgaard, E.M.; Borris, L.C. Blood Transfusion and Risk of Infection in Frail Elderly after Hip Fracture Surgery: The TRIFE Randomized Controlled Trial. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 1031–1038. [Google Scholar] [CrossRef]
- Hart, A.; Khalil, J.A.; Carli, A.; Huk, O.; Zukor, D.; Antoniou, J. Blood Transfusion in Primary Total Hip and Knee Arthroplasty. Incidence, Risk Factors, and Thirty-Day Complication Rates. J. Bone Jt. Surg. 2014, 96, 1945–1951. [Google Scholar] [CrossRef] [PubMed]
- Tüzün, H.Y.; Bilekli, A.B.; Erşen, Ö. The Factors That Affect Blood Loss in Intertrochanteric Fractures Treated with Proximal Femoral Nail in the Elderly. Eur. J. Trauma Emerg. Surg. 2022, 48, 1879–1884. [Google Scholar] [CrossRef] [PubMed]
- Hou, G.; Zhou, F.; Tian, Y.; Ji, H.; Zhang, Z.; Guo, Y.; Lv, Y. Predicting the Need for Blood Transfusions in Elderly Patients with Pertrochanteric Femoral Fractures. Injury 2014, 45, 1932–1937. [Google Scholar] [CrossRef] [PubMed]
- Fazal, M.A.; Bagley, C.; Garg, P. Predictors for Perioperative Blood Transfusion in Elderly Patients with Extra Capsular Hip Fractures Treated with Cephalo-Medullary Nailing. Chin. J. Traumatol. 2018, 21, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Adunsky, A.; Lichtenstein, A.; Mizrahi, E.; Arad, M.; Heim, M. Blood Transfusion Requirements in Elderly Hip Fracture Patients. Arch. Gerontol. Geriatr. 2003, 36, 75–81. [Google Scholar] [CrossRef]
- Desai, S.; Wood, K.; Marsh, J.; Bryant, D.; Abdo, H.; Lawendy, A.-R.; Sanders, D. Factors Affecting Transfusion Requirement after Hip Fracture: Can We Reduce the Need for Blood? Can. J. Surg. 2014, 57, 342–348. [Google Scholar] [CrossRef] [Green Version]
- Walsh, M.; Preston, C.; Bong, M.; Patel, V.; Di Cesare, P.E. Relative Risk Factors for Requirement of Blood Transfusion after Total Hip Arthroplasty. J. Arthroplast. 2007, 22, 1162–1167. [Google Scholar] [CrossRef]
- Shelton, C.; White, S. Anaesthesia for Hip Fracture Repair. BJA Educ. 2020, 20, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.X.; Yang, L.; Ding, L.; Li, S.Y.; Qi, Y.N.; Li, Q. Perioperative Outcomes in Geriatric Patients Undergoing Hip Fracture Surgery with Different Anesthesia Techniques: A Systematic Review and Meta-Analysis. Medicine 2019, 98, e18220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basques, B.A.; Bohl, D.D.; Golinvaux, N.S.; Samuel, A.M.; Grauer, J.G. General versus Spinal Anaesthesia for Patients Aged 70 Years and Older with a Fracture of the Hip. Bone Jt. J. 2015, 97-B, 689–695. [Google Scholar] [CrossRef]
- Borghi, B.; Casati, A.; Iuorio, S.; Celleno, D.; Michael, M.; Serafini, P.; Pusceddu, A.; Fanelli, G. Frequency of Hypotension and Bradycardia during General Anesthesia, Epidural Anesthesia, or Integrated Epidural-General Anesthesia for Total Hip Replacement. J. Clin. Anesth. 2002, 14, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Sessler, D.I.; Warner, D.S.; Warner, M.A. Temperature Monitoring and Perioperative Thermoregulation. Anesthesiology 2008, 109, 318–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dillon, M.F.; Collins, D.; Rice, J.; Murphy, P.G.; Nicholson, P.; Mac Elwaine, J. Preoperative Characteristics Identify Patients with Hip Fractures at Risk of Transfusion. Clin. Orthop. Relat. Res. 2005, 439, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Hasan, O.; Barkat, R.; Rabbani, A.; Rabbani, U.; Mahmood, F.; Noordin, S. Charlson Comorbidity Index Predicts Postoperative Complications in Surgically Treated Hip Fracture Patients in a Tertiary Care Hospital: Retrospective Cohort of 1045 Patients. Int. J. Surg. 2020, 82, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Quach, L.H.; Jayamaha, S.; Whitehouse, S.L.; Crawford, R.; Pulle, C.R.; Bell, J.J. Comparison of the Charlson Comorbidity Index with the ASA Score for Predicting 12-Month Mortality in Acute Hip Fracture. Injury 2020, 51, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Haugan, K.; Klaksvik, J.; Foss, O.A. 30-Day Mortality in Patients after Hip Fracture Surgery: A Comparison of the Charlson Comorbidity Index Score and ASA Score Used in Two Prediction Models. Injury 2021, 52, 2379–2383. [Google Scholar] [CrossRef]
- Guo, J.; Zhang, Y.; Hou, Z. Intramedullary Fixation Does Not Cause a Large Amount of Hidden Blood Loss in Elderly Patients with Intertrochanteric Fractures. CIA 2021, 16, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.-H.; Chien, J.-T.; Hung, J.-P.; Hong, C.-K.; Tsai, T.-Y.; Yang, C.-C. Unstable Intertrochanteric Fractures Are Associated with a Greater Hemoglobin Drop during the Perioperative Period: A Retrospective Case Control Study. BMC Musculoskelet. Disord. 2020, 21, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, J.; Kuang, M.; Fan, Z.; Xing, F.; Zhao, Y.; Zhang, L.; Chen, H.; Han, C.; Ma, X. Comparison of Clinical Outcomes with InterTan vs Gamma Nail or PFNA in the Treatment of Intertrochanteric Fractures: A Meta-Analysis. Sci. Rep. 2017, 7, 15962. [Google Scholar] [CrossRef] [Green Version]
- Thamyongkit, S.; MacKenzie, J.S.; Sirisreetreerux, N.; Shafiq, B.; Hasenboehler, E.A. Outcomes after Unstable Pertrochanteric Femur Fracture: Intermediate versus Long Cephalomedullary Nails. Eur. J. Trauma Emerg. Surg. 2020, 46, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-H.; Kim, N.Y. Can Early Surgery Reduce the Need to Packed Red Blood Cell Transfusion in Elderly Patients with Intertrochanteric Femur Fractures? Injury 2021, 52, 3047–3050. [Google Scholar] [CrossRef] [PubMed]
- Mattisson, L.; Lapidus, L.J.; Enocson, A. What Is the Influence of a Delay to Surgery >24 Hours on the Rate of Red Blood Cell Transfusion in Elderly Patients With Intertrochanteric or Subtrochanteric Hip Fractures Treated With Cephalomedullary Nails? J. Orthop. Trauma 2018, 32, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Shokoohi, A.; Stanworth, S.; Mistry, D.; Lamb, S.; Staves, J.; Murphy, M.F. The Risks of Red Cell Transfusion for Hip Fracture Surgery in the Elderly: The Risks of Red Cell Transfusion for Hip. Vox Sang. 2012, 103, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Scharman, C.D.; Burger, D.; Shatzel, J.J.; Kim, E.; DeLoughery, T.G. Treatment of Individuals Who Cannot Receive Blood Products for Religious or Other Reasons. Am. J. Hematol. 2017, 92, 1370–1381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuenca, J.; García-Erce, J.A.; Martínez, A.A.; Solano, V.M.; Molina, J.; Muñoz, M. Role of Parenteral Iron in the Management of Anaemia in the Elderly Patient Undergoing Displaced Subcapital Hip Fracture Repair: Preliminary Data. Arch. Orthop. Trauma Surg. 2005, 125, 342–347. [Google Scholar] [CrossRef]
- Rowlands, M.; Forward, D.P.; Sahota, O.; Moppett, I.K. The Effect of Intravenous Iron on Postoperative Transfusion Requirements in Hip Fracture Patients: Study Protocol for a Randomized Controlled Trial. Trials 2013, 14, 288. [Google Scholar] [CrossRef] [Green Version]
- Xing, F.; Chen, W.; Long, C.; Huang, F.; Wang, G.; Xiang, Z. Postoperative Outcomes of Tranexamic Acid Use in Geriatric Trauma Patients Treated with Proximal Femoral Intramedullary Nails: A Systematic Review and Meta-Analysis. Orthop. Traumatol. Surg. Res. 2020, 106, 117–126. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients (M:F) | Age (Range) | BMI | Hb | INR | Hospital Stay | Time To Surgery | Surgery Duration | Anesthesia (GA/CSEA) | ASA | CCI | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group NBT | 71 (24:47) | 80.2 ± 10.7 (65–94) | 26.5 ± 5.9 (15.4–44.4) | 12.5 ± 1.67 (8.7–16.7) | 1.1 ± 0.12 (0.9–1.4) | 10.8 ± 4 (5–24) | 2.4 ± 1.6 (0–8) | 57.8 ± 16.2 (25–105) | 9/62 | 2.8 ± 0.6 (1–5) | 5.21 ± 2.1 (1–10) |
| Group BT | 72 (17:55) | 82.9 ± 7.6 (65–99) | 26.1 ± 5.1 (12.9–39.1) | 10.6 ± 1.4 (7.0–13.2) | 1.1 ± 0.16 (0.9–1.6) | 11.4 ± 5.3 (5–39) | 2.3 ± 2 (0–9) | 73.3 ± 31.2 (30–185) | 11/61 | 2.8 ± 0.5 (2–4) | 5.78 ± 2.4 (2–12) |
| NBT vs. BT | 0.17 | 0.07 | 0.65 | <0.001 | 0.88 | 0.44 | 0.64 | <0.001 | 0.65 | 0.81 | 0.19 |
| RR (95% C.I.) | 1.43 (0.8, 2.4) | 1.52 (0.9, 2.5) | 1.0 (0.77, 1.4) | 1.03 (0.9, 1.7) | 0.91 (0.49, 1.4) | 1.16 (0.45, 2.8) | 0.74 (0.5, 1.1) | 1.37 (0.80, 2.3) | 1.05 (0.9, 1.2) | 0.96 (0.55, 1.6) | 0.82 (0.62, 1.1) |
| PCC (p) | 0.07 (0.64) | 0.08 (0.33) | −0.033 (0.70) | −0.49 (<0.001) | −0.02 (0.89) | 0.16 (0.06) | −0.07 (0.41) | 0.28 (0.001) | 0.11 (0.17) | 0.02 (0.74) | 0.16 (0.10) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Testa, G.; Montemagno, M.; Vescio, A.; Micali, G.; Perrotta, R.; Lacarrubba, F.; Avitabile, T.; Basile, G.; Pavone, V. Blood-Transfusion Risk Factors after Intramedullary Nailing for Extracapsular Femoral Neck Fracture in Elderly Patients. J. Funct. Morphol. Kinesiol. 2023, 8, 27. https://doi.org/10.3390/jfmk8010027
Testa G, Montemagno M, Vescio A, Micali G, Perrotta R, Lacarrubba F, Avitabile T, Basile G, Pavone V. Blood-Transfusion Risk Factors after Intramedullary Nailing for Extracapsular Femoral Neck Fracture in Elderly Patients. Journal of Functional Morphology and Kinesiology. 2023; 8(1):27. https://doi.org/10.3390/jfmk8010027
Chicago/Turabian StyleTesta, Gianluca, Marco Montemagno, Andrea Vescio, Giuseppe Micali, Rosario Perrotta, Francesco Lacarrubba, Teresio Avitabile, Guido Basile, and Vito Pavone. 2023. "Blood-Transfusion Risk Factors after Intramedullary Nailing for Extracapsular Femoral Neck Fracture in Elderly Patients" Journal of Functional Morphology and Kinesiology 8, no. 1: 27. https://doi.org/10.3390/jfmk8010027