
Simulating Knee-Stress Distribution Using a Computed Tomography-Based Finite Element Model: A Case Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Overview of the CT-FEM Software
2.3. Calibration of CT Image Acquisition Conditions and CT Values
2.4. Outline up to CT-FEM Analysis
2.5. Loading Method
2.6. Gait Analysis
2.7. The CT-FEM Model
2.7.1. Scope of Modeling
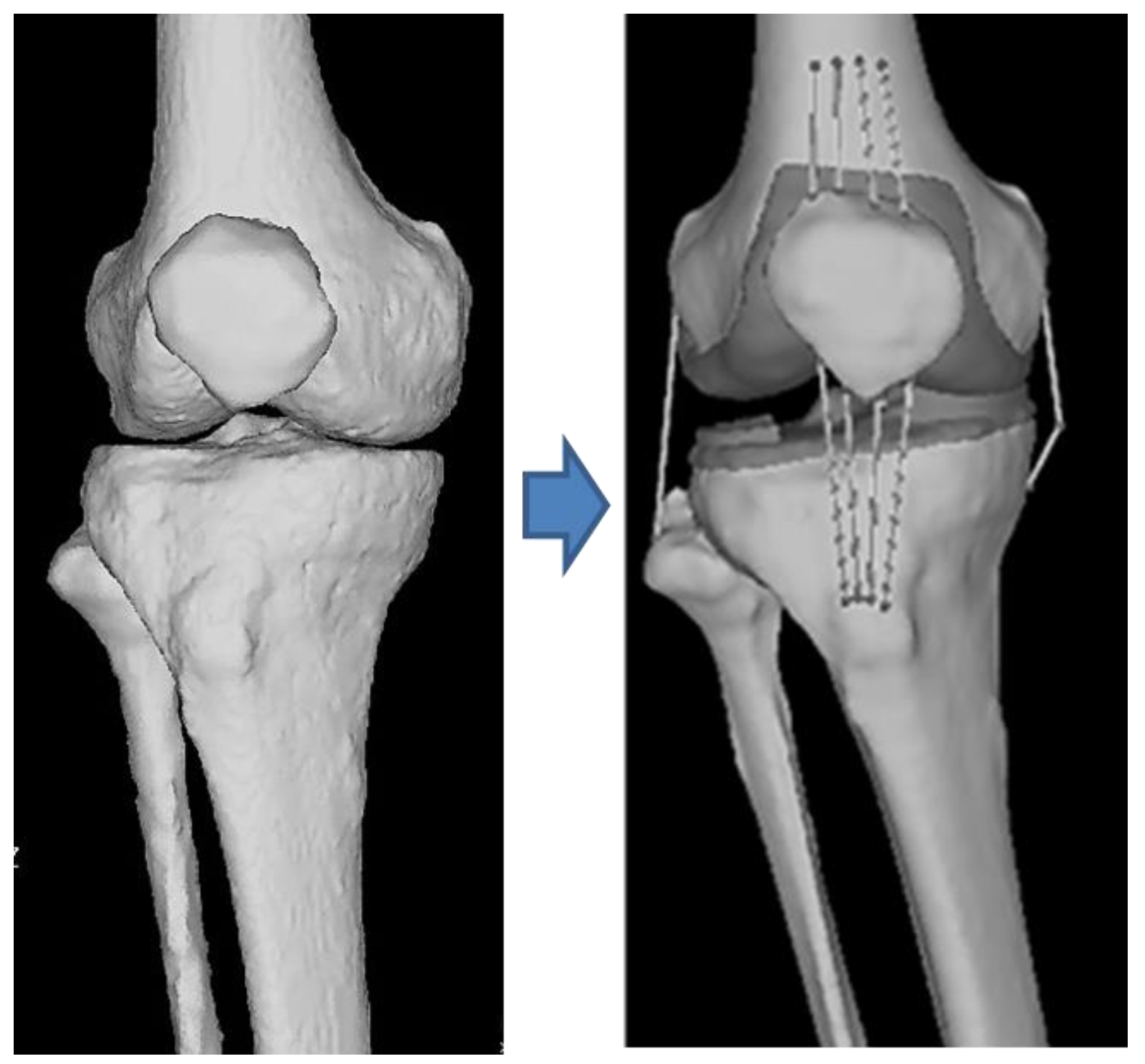
2.7.2. Construction of the CT-FEM Model
2.7.3. Determining Material Properties
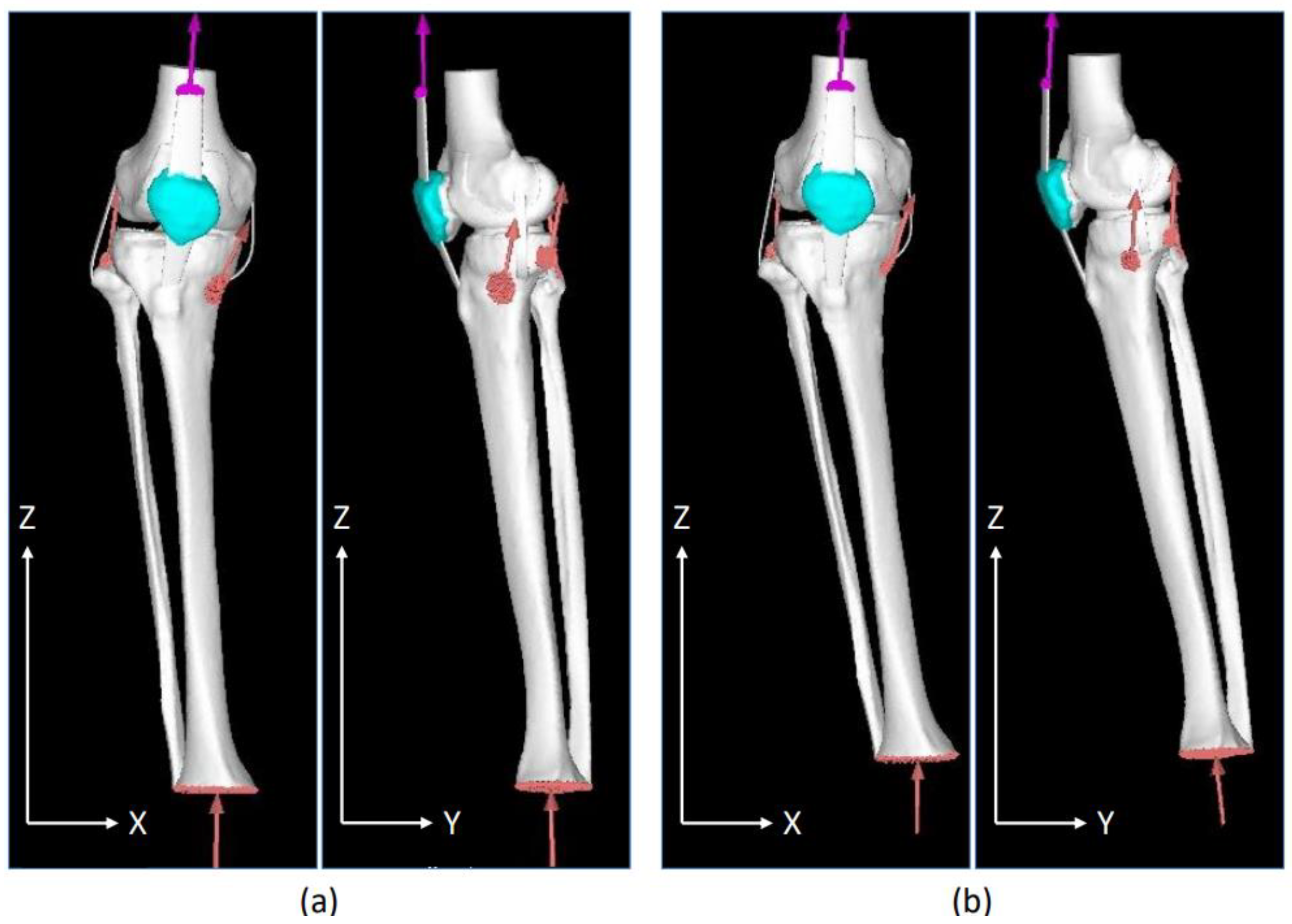
2.7.4. Loading and Restraint Conditions
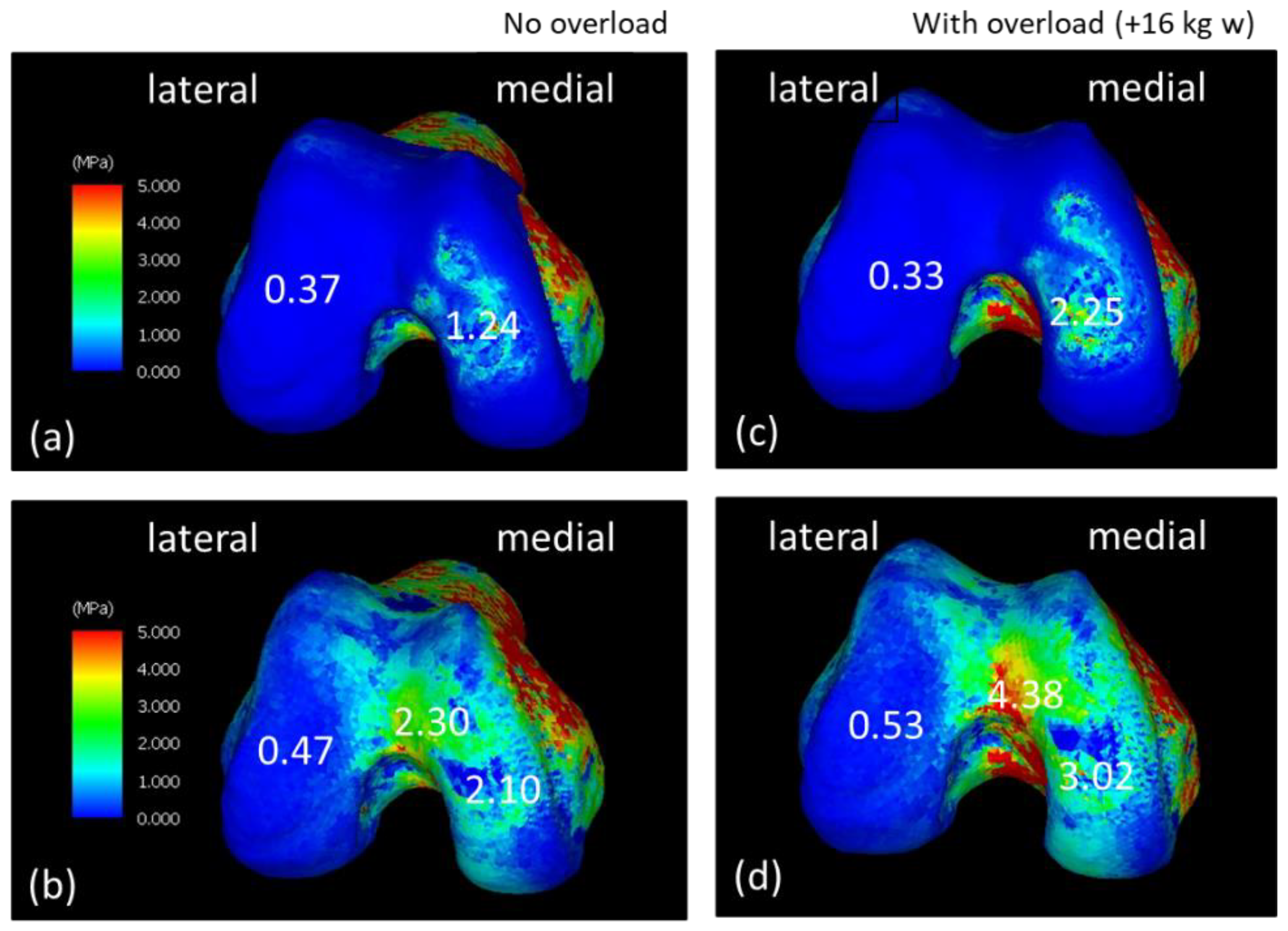
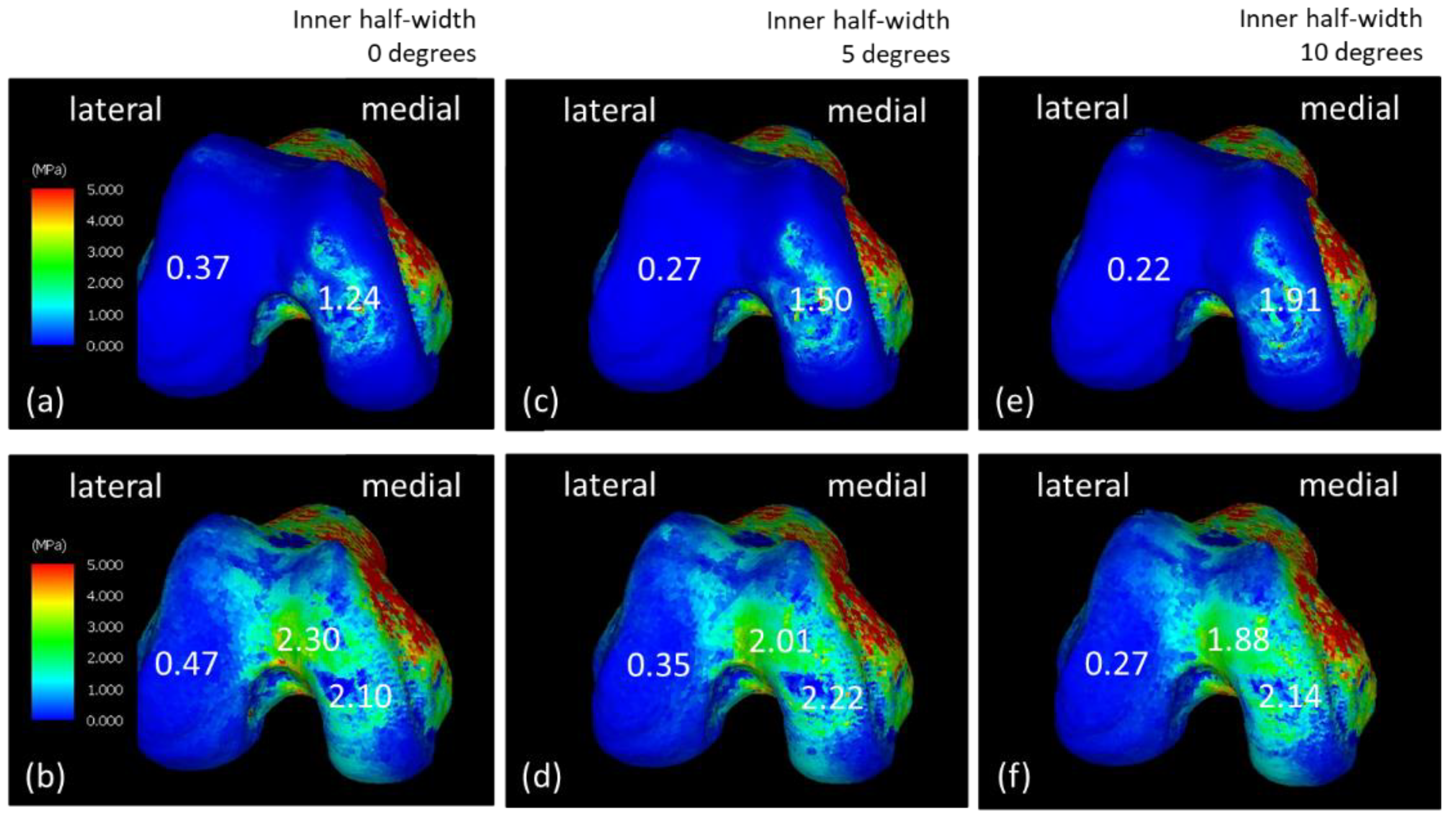
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ackroyd, R.T. Finite Element Methods for Particle Transport; Research Studies Press: Taunton, UK, 1997; pp. 8–12. [Google Scholar]
- Zlámal, M. On the finite element method. Numer. Math. 1968, 12, 394–409. [Google Scholar] [CrossRef]
- Nakanowatari, K.; Watanabe, K.; Mori, K.; Nakajima, S.; Sekine, N.; Mutsuzaki, H. Evaluation of vertebral bone strength with a finite element method using low dose computed tomography imaging. J. Orthop. Sci. 2022, 27, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Okubo, T.; Mori, K.; Wadano, Y.; Kawanami, K.; Tachibana, K.; Shimizu, Y.; Sekine, N. Prediction of compression fracture risk of lumber vertebra using a X-ray CT-based finite element method. Jpn. Acad. Health Sci. 2013, 16, 90–98. (In Japanese) [Google Scholar]
- Bessho, M.; Ohnishi, I.; Matsumoto, T.; Ohashi, S.; Matsuyama, J.; Tobita, K.; Kaneko, M.; Nakamura, K. Prediction of proximal femur strength using a CT-based nonlinear finite element method: Differences in predicted fracture load and site with changing load and boundary conditions. Bone 2009, 45, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, S.; Kullmer, G.; Richard, H.A. Designing the construction of an FE model exemplified by the knee joint. Biomed. Tech. 1997, 42, 347–351. (In German) [Google Scholar] [CrossRef] [PubMed]
- Chantarapanich, N.; Nanakorn, P.; Chernchujit, B.; Sitthiseripratip, K. A finite element study of stress distributions in normal and osteoarthritic knee joints. J. Med. Assoc. Thai. 2009, 92, S97–S103. [Google Scholar] [PubMed]
- Quintana, J.M.; Arostegui, I.; Escobar, A.; Azkarate, J.; Goenaga, J.I.; Lafuente, I. Prevalence of knee and hip osteoarthritis and the appropriateness of joint replacement in an older population. Arch. Intern. Med. 2008, 168, 1576–1584. [Google Scholar] [CrossRef]
- Michael, J.W.P.; Schlüter-Brust, K.U.; Eysel, P. The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Dtsch. Arztebl. Int. 2010, 107, 152–162. [Google Scholar] [CrossRef]
- Guilak, F. Biomechanical factors in osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2011, 25, 815–823. [Google Scholar] [CrossRef] [Green Version]
- Petrigna, L.; Roggio, F.; Trovato, B.; Zanghì, M.; Guglielmino, C.; Musumeci, G. How physical activity affects knee cartilage and a standard intervention procedure for an exercise program: A systematic review. Healthcare 2022, 10, 1821. [Google Scholar] [CrossRef]
- Bucknor, M.D.; Nardo, L.; Joseph, G.B.; Alizai, H.; Srikhum, W.; Nevitt, M.C.; Lynch, J.A.; McCulloch, C.E.; Link, T.M. Association of cartilage degeneration with four year weight gain--3T MRI data from the osteoarthritis initiative. Osteoarthr. Cartil. 2015, 23, 525–531. [Google Scholar] [CrossRef] [Green Version]
- Tamaki, M.; Koga, Y. Osteoarthritis of the knee joint: A field study. Nihon Seikei Geka. Gakkai Zasshi 1994, 68, 737–750. (In Japanese) [Google Scholar]
- Watanabe, K.; Mutsuzaki, H.; Fukaya, T.; Aoyama, T.; Nakajima, S.; Sekine, N.; Mori, K. Development of a knee joint CT-FEM model in load response of the stance phase during walking using muscle exertion, motion analysis, and ground reaction force data. Medicina 2020, 56, 56. [Google Scholar] [CrossRef] [Green Version]
- Fukaya, T.; Mutsuzaki, H.; Aoyama, T.; Watanabe, K.; Mori, K.A. A simulation case study of knee joint compressive stress during the stance phase in severe knee osteoarthritis using finite element method. Medicina 2021, 57, 550. [Google Scholar] [CrossRef]
- Davids, J.R.; Perry, J.; Slac, T. Gait analysis: Normal and pathological function. J. Pediatr. Orthop. 1992, 12, 815. [Google Scholar] [CrossRef]
- Imai, K.; Ohnishi, I.; Yamamoto, S.; Nakamura, K. In vivo assessment of lumbar vertebral strength in elderly women using computed tomography-based nonlinear finite element model. Spine 2008, 33, 27–32. [Google Scholar] [CrossRef]
- Silva, M.J.; Keaveny, T.M.; Hayes, W.C. Load sharing between the shell and centrum in the lumbar vertebral body. Spine 1997, 22, 140–150. [Google Scholar] [CrossRef]
- Keyak, J.H.; Rossi, S.A.; Jones, K.A.; Skinner, H.B. Prediction of femoral fracture load using automated finite element modeling. J. Biomech. 1998, 31, 125–133. [Google Scholar] [CrossRef]
- Keyak, J.H.; Sigurdsson, S.; Karlsdottir, G.; Oskarsdottir, D.; Sigmarsdottir, A.; Zhao, S.; Kornak, J.; Harris, T.B.; Sigurdsson, G.; Jonsson, B.Y.; et al. Male-female differences in the association between incident hip fracture and proximal femoral strength: A finite element analysis study. Bone 2011, 48, 1239–1245. [Google Scholar] [CrossRef] [Green Version]
- Matsuura, Y.; Giambini, H.; Ogawa, Y.; Fang, Z.; Thoreson, A.R.; Yaszemski, M.J.; Lu, L.; An, K.N. Specimen-specific nonlinear finite element modeling to predict vertebrae fracture loads after vertebroplasty. Spine 2014, 39, E1291–E1296. [Google Scholar] [CrossRef] [Green Version]
- Saxena, R.; Keller, T.S.; Sullivan, J.M.A. A three-dimensional finite element scheme to investigate the apparent mechanical properties of trabecular bone. Comput. Methods Biomech. Biomed. Eng. 1999, 2, 285–294. [Google Scholar] [CrossRef]
- Hayashi, S. Quantitative analysis of lateral force of floor reactions in normal and above-knee prosthetic gait. Nihon Seikei Geka. Gakkai Zasshi 1983, 57, 1911–1921. (In Japanese) [Google Scholar]
- Warnecke, D.; Meßemer, M.; de Roy, L.; Stein, S.; Gentilini, C.; Walker, R.; Skaer, N.; Ignatius, A.; Dürselen, L. Articular cartilage and meniscus reveal higher friction in swing phase than in stance phase under dynamic gait conditions. Sci. Rep. 2019, 9, 5785. [Google Scholar] [CrossRef] [Green Version]
- Kubıcek, M.; Florian, Z. Stress strain analysis of knee joint. J. Eng. Mech. 2009, 16, 315–322. [Google Scholar]
- Derrick, T.R.; Edwards, W.B.; Fellin, R.E.; Seay, J.F. An integrative modeling approach for the efficient estimation of cross sectional tibial stresses during locomotion. J. Biomech. 2016, 49, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Maly, M.R.; Acker, S.M.; Totterman, S.; Tamez-Peña, J.; Stratford, P.W.; Callaghan, J.P.; Adachi, J.D.; Beattie, K.A. Knee adduction moment relates to medial femoral and tibial cartilage morphology in clinical knee osteoarthritis. J. Biomech. 2015, 48, 3495–3501. [Google Scholar] [CrossRef]
- Lenhart, R.L.; Kaiser, J.; Smith, C.R.; Thelen, D.G. Prediction and validation of load-dependent behavior of the tibiofemoral and patellofemoral joints during movement. Ann. Biomed. Eng. 2015, 43, 2675–2685. [Google Scholar] [CrossRef] [Green Version]
- Venäläinen, M.S.; Mononen, M.E.; Salo, J.; Räsänen, L.P.; Jurvelin, J.S.; Töyräs, J.; Virén, T.; Korhonen, R.K. Quantitative evaluation of the mechanical risks caused by focal cartilage defects in the knee. Sci. Rep. 2016, 6, 37538. [Google Scholar] [CrossRef] [Green Version]
- Van Ginckel, A.; Bennell, K.L.; Campbell, P.K.; Wrigley, T.V.; Hunter, D.J.; Hinman, R.S. Location of knee pain in medial knee osteoarthritis: Patterns and associations with self-reported clinical symptoms. Osteoarthr. Cartil. 2016, 24, 1135–1142. [Google Scholar] [CrossRef] [Green Version]
- Palmer, J.S.; Jones, L.D.; Monk, A.P.; Nevitt, M.; Lynch, J.; Beard, D.J.; Javaid, M.K.; Price, A.J. Varus alignment of the proximal tibia is associated with structural progression in early to moderate varus osteoarthritis of the knee. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 3279–3286. [Google Scholar] [CrossRef] [Green Version]
- Askari, A.; Gholami, T.; Naghizadeh, M.M.; Farjam, M.; Kouhpayeh, S.A.; Shahabfard, Z. Hyaluronic acid compared with corticosteroid injections for the treatment of osteoarthritis of the knee: A randomized control trail. Springerplus 2016, 5, 442. [Google Scholar] [CrossRef] [Green Version]
- Cho, B.W.; Hong, H.T.; Koh, Y.G.; Choi, J.; Park, K.K.; Kang, K.T. Analysis of gender differences in the rotational alignment of the distal femur in kinematically aligned and mechanically aligned total knee arthroplasty. J. Clin. Med. 2021, 10, 3691. [Google Scholar] [CrossRef]
- Blagojevic, M.; Jinks, C.; Jeffery, A.; Jordan, K.P. Risk factors for onset of osteoarthritis of the knee in older adults: A systematic review and meta-analysis. Osteoarthritis. Osteoarthr. Cartil. 2010, 18, 24–33. [Google Scholar] [CrossRef] [Green Version]
- Simic, M.; Harmer, A.R.; Agaliotis, M.; Nairn, L.; Bridgett, L.; March, L.; Votrubec, M.; Edmonds, J.; Woodward, M.; Day, R.; et al. Clinical risk factors associated with radiographic osteoarthritis progression among people with knee pain: A longitudinal study. Arthritis Res. Ther. 2021, 23, 160. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Angle between the tibia and floor | |||
| No overload (NO) | Varus angle 6.18° | Flexion angle 10.42° | Internal rotation 41.26° |
| With overload (WO) | Varus angle 5.86° | Flexion angle −0.27° | Internal rotation 44.84° |
| Angle between the femur and tibia | |||
| No overload (NO) | Varus angle 4.61° | Flexion angle 2.30° | Internal rotation 0° |
| With overload (WO) | Varus angle 6.80° | Flexion angle 7.90° | Internal rotation 0° |
| Anatomical Element | Poisson’s Ratio | Young’s Modulus (MPa) |
|---|---|---|
| Femur, tibia, fibula, patella | 0.4 | Keyak’s conversion formula |
| Cartilage | 0.4 | 20 (100 only on the fibula) |
| Meniscal | 0.4 | 20 |
| Ligament | 0.4 | 0.1 |
| Muscle Traction (N) | ||
|---|---|---|
| No Overload (NO) | With Overload (WO) | |
| Quadriceps | 392.49 | 608.51 |
| Biceps femoris | 405.24 | 620.51 |
| Semimembranosus | 166.13 | 245.96 |
| Semitendinosus + gracilis | 96.48 | 133.30 |
| Floor reaction force (N) | ||
| No overload (NO) | With overload (WO) | |
| Inward direction | 47.67 | 43.30 |
| Forward direction | 43.97 | 67.52 |
| Upward direction | 753.44 | 987.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, K.; Mutsuzaki, H.; Fukaya, T.; Aoyama, T.; Nakajima, S.; Sekine, N.; Mori, K. Simulating Knee-Stress Distribution Using a Computed Tomography-Based Finite Element Model: A Case Study. J. Funct. Morphol. Kinesiol. 2023, 8, 15. https://doi.org/10.3390/jfmk8010015
Watanabe K, Mutsuzaki H, Fukaya T, Aoyama T, Nakajima S, Sekine N, Mori K. Simulating Knee-Stress Distribution Using a Computed Tomography-Based Finite Element Model: A Case Study. Journal of Functional Morphology and Kinesiology. 2023; 8(1):15. https://doi.org/10.3390/jfmk8010015
Chicago/Turabian StyleWatanabe, Kunihiro, Hirotaka Mutsuzaki, Takashi Fukaya, Toshiyuki Aoyama, Syuichi Nakajima, Norio Sekine, and Koichi Mori. 2023. "Simulating Knee-Stress Distribution Using a Computed Tomography-Based Finite Element Model: A Case Study" Journal of Functional Morphology and Kinesiology 8, no. 1: 15. https://doi.org/10.3390/jfmk8010015