
Periodontal Maintenance Therapy: Efficacy of Oral Irrigator in the Home Oral Hygiene Protocol Associated with Microbiological Analysis with Phase Contrast Microscope


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Inclusion Criteria
- age from 35 to 65;
- no systemic diseases;
- clinical attachment loss of less than 5 mm in at least two non-near teeth;
- no dental mobility;
- bleeding index under 30%;
- plaque index under 30%.
2.3. Phase Contrast Microscope: Qualitative Microbiological Analysis of Bacterial Plaque for Periodontal Diagnosis and Re-Evaluation
- -
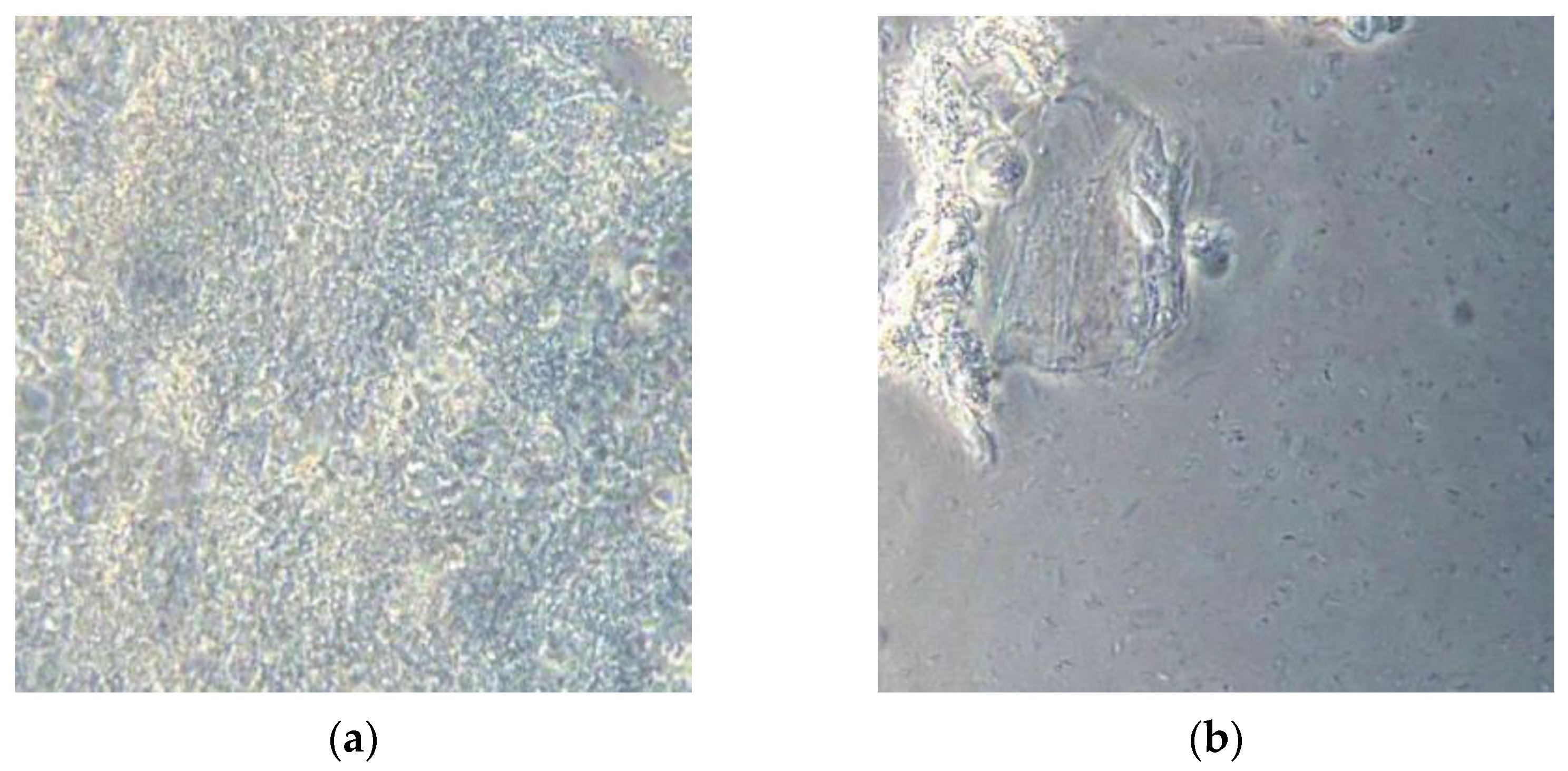
- Non-pathogenic bacterial flora: immobile, similar to the aerial view of the mainland (Figure 3a);
- -
- Pathogenic bacterial flora: in which are visualized “Streams” or “basins” with mobile bacteria, mostly composed of spirochetes (including Treponema Denticola) and Trichomonas Tenax that flow in motion, as if dragged by the current. The most consistent similarity is that of the aerial visualization of the Norwegian fjords (Figure 3b).
- -
- Non-pathogenic bacterial flora (static flora, Gram-positive bacteria): usual periodontal maintenance therapy with appointments every 6 months;
- -
- Pathogenic bacterial flora (spirochete, moving flora): immediate treatment with supra-gingival and sub-gingival ultrasonic instrumentation, air flow with bicarbonate powder, and a single-stage session of photodynamic therapy without dye (OHLLT) in the entire mouth. This protocol has also been applied without signs of inflammation.
2.4. Laser-Assisted Non-Surgical Causal Therapy: OHLLT
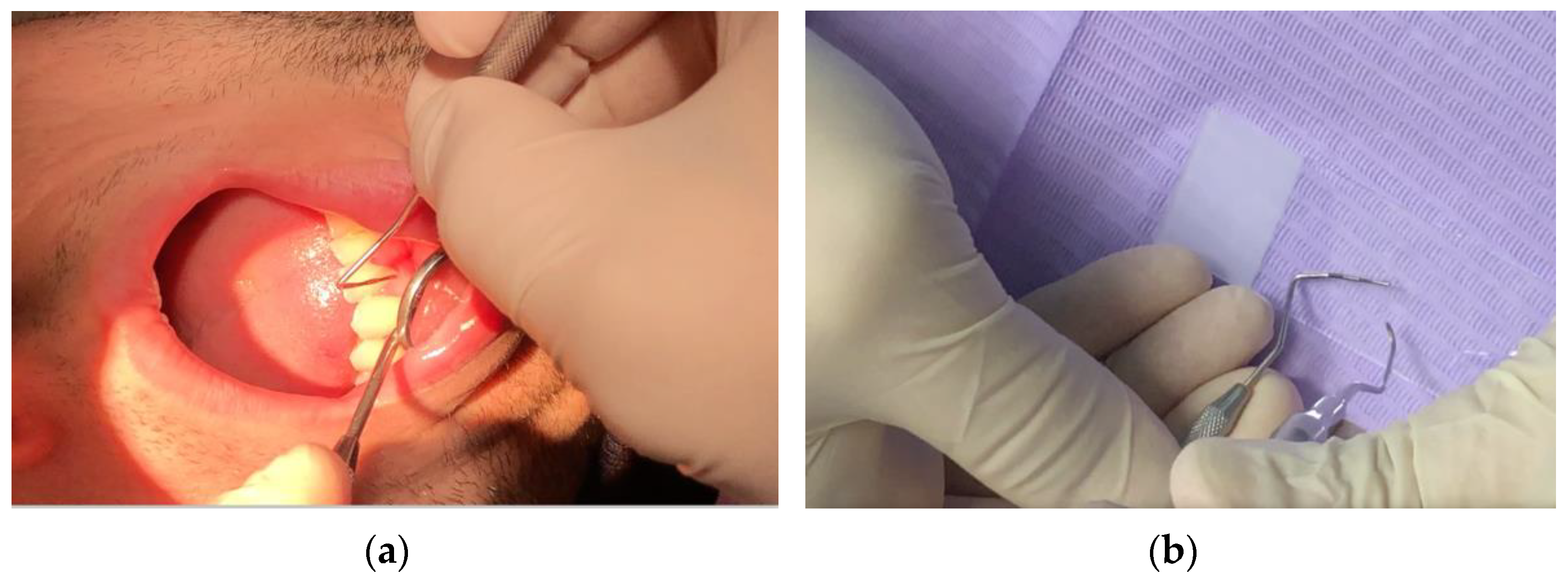
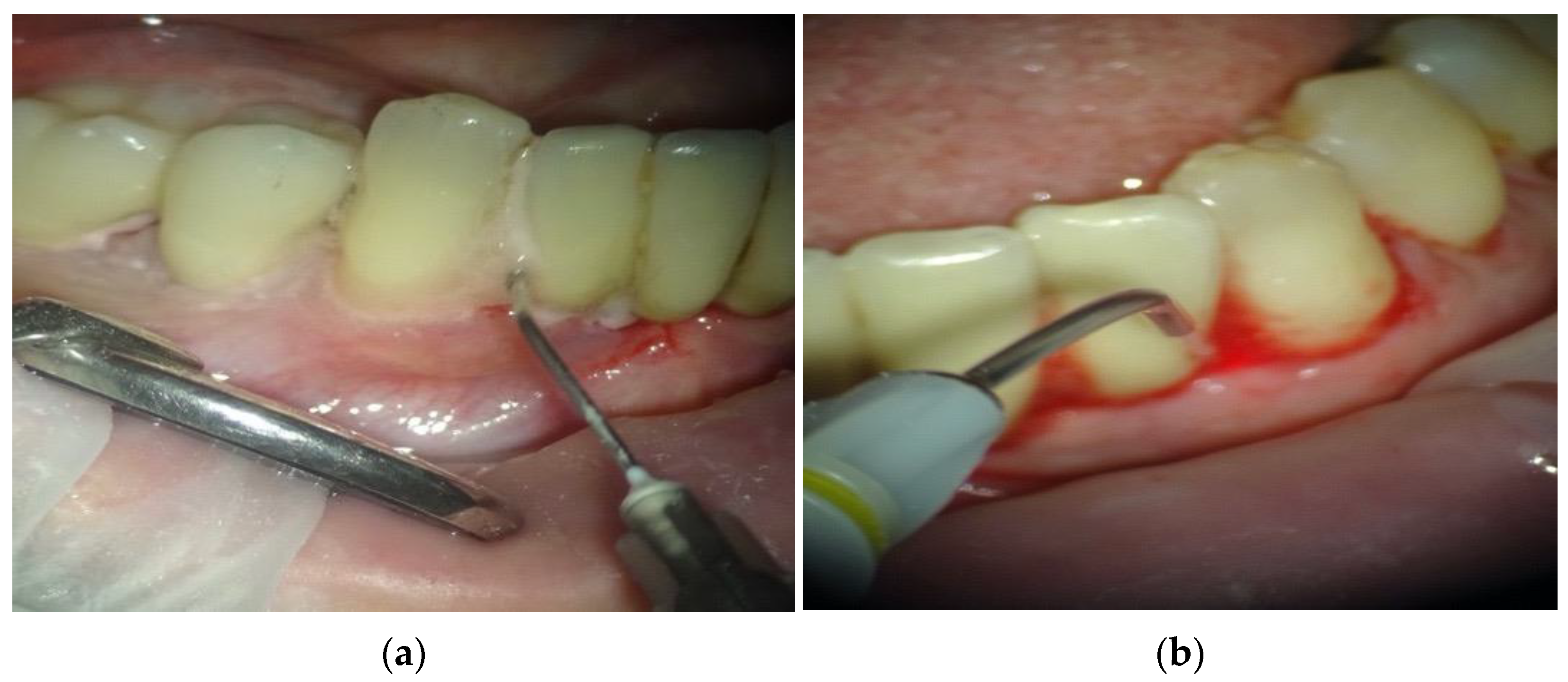
- Irrigation of periodontal pockets with Sioxyl solution (derivative of hydrogen peroxide);
- Aspiration of Sioxyl solution emerging from the gingival sulcus and leaving the remaining solution inside the pocket for 2 min;
- Introduction of the HF Diode Laser 980 nm, Fiber 400 microns (Wiser Doctor Smile, Lambda, Vicenza, Italy) within the pocket and reaching the bottom;
- Radiation of subgingival tissues with a movement back and forth using the dedicated program, 60 s for each side (2.5 W peak power, high frequency, 10 KHz, power average 0.5 W, Fluency 25,000/cm2).
- -
- Non-pathogenic bacterial flora: Patients begin periodontal maintenance therapy with 6-month controls;
- -
- Pathogenic bacterial flora: It is recommended re-motivation to home oral hygiene, and a single-stage session of laser-assisted PDT without dye.
2.5. Modified Home Oral Hygiene Protocol: Sonic Toothbrush, Interdental Brushes, Oral Irrigator
2.6. Methods for a Study Aimed at Demonstrating the Efficacy of the Oral Irrigator in Modifying the Subgingival Bacterial Flora
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Manresa, C.; Sanz-Miralles, E.C.; Twigg, J.; Bravo, M. Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst. Rev. 2018, 1, CD009376. [Google Scholar] [CrossRef] [PubMed]
- Rhemrev, G.E.; Timmerman, M.F.; Veldkamp, I.; van Winkelhoff, A.J.; van der Velden, U. Immediate effect of instrumen-tation on the subgingival microflora in deep inflamed pockets under strict plaque control. J. Clin. Periodontol. 2006, 33, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.; Tonetti, M.S.; Cortellini, P.; Lang, N.P. Microbial colonization patterns predict the outcomes of surgi-cal treatment of intrabony defects. J. Clin. Periodontol. 2006, 33, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Gursoy, H.; Ozcakir-Tomruk, C.; Tanalp, J.; Yilmaz, S. Photodynamic therapy in dentistry: A literature review. Clin. Oral Investig. 2013, 17, 1113–1125. [Google Scholar] [CrossRef]
- Ando, Y.; Aoki, A.; Watanabe, H.; Ishikawa, I. Bactericidal Effect of Erbium YAG Laser on Periodontopathic Bacteria. Lasers Surg. Med. 1996, 19, 190–200. [Google Scholar] [CrossRef]
- Moritz, A.; Gutnetcht, N.; Schoop, U.; Gobarkhay, K.; Doerbudak, O.; Speer, W. Irradiation of infected root canals with a diode laser in vivo: Results of microbiological examinations lasers in surgery and medecine. Lasers Surg. Med. 1997, 21, 221–226. [Google Scholar] [CrossRef]
- Nammour, S.; El Mobadder, M.; Maalouf, E.; Namour, M.; Namour, A.; Rey, G.; Matamba, P.; Matys, J.; Zeinoun, T.; Grzech-Leśniak, K. Clinical Evaluation of Diode (980 nm) Laser-Assisted Nonsurgical Periodontal Pocket Therapy: A Randomized Comparative Clinical Trial and Bacteriological Study. Photobiomodul. Photomed. Laser Surg. 2021, 39, 10–22. [Google Scholar] [CrossRef] [PubMed]
- Azarpazhooh, A.; Shah, P.S.; Tenenbaum, H.C.; Berg, M.B.G. Photodynamic therapy for periodontitis: A systematic review and meta-analysis. J. Periodontol. 2010, 81, 4–14. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Baldoni, M.; Paiusco, A. Clinical, radiographic and microbiological evaluation of high level laser therapy, a new photodynamic therapy protocol, in peri-implantitis treatment; a pilot experience. Biomed. Res. Int. 2016, 2016, 6321906. [Google Scholar] [CrossRef] [Green Version]
- Rey, G. L’apport du laser dans le traitement des poches paradontales. Implantodontie 2000, 38, 37–44. [Google Scholar]
- Caccianiga, G.; Baldoni, M.; Ghisalberti, C.A.; Paiusco, A. A Preliminary In Vitro Study on the Efficacy of High-Power Photodynamic Therapy (HLLT): Comparison between Pulsed Diode Lasers and Superpulsed Diode Lasers and Impact of Hydrogen Peroxide with Controlled Stabilization. Biomed. Res. Int. 2016, 2016, 1386158. [Google Scholar] [CrossRef]
- Caccianiga, G.; Cambini, A.; Donzelli, E.; Baldoni, M.; Rey, G.; Paiusco, A. Effects of laser biostimulation on the epithelial tissue for keratinized layer differentiation: An in vitro study. J. Biol. Regul. Homeost. Agents 2016, 30 (Suppl. 1), 99–105. [Google Scholar]
- Caccianiga, G.; Rey, G.; Baldoni, M.; Caccianiga, P.; Baldoni, A.; Ceraulo, S. Periodontal Decontamination Induced by Light and Not by Heat: Comparison between Oxygen High Level Laser Therapy (OHLLT) and LANAP. Appl. Sci. 2021, 11, 4629. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Caccianiga, P.; Leonida, A.; Baldoni, M.; Baldoni, A.; Ceraulo, S. Rough Dental Implant Surfaces and Peri-Implantitis: Role of Phase-Contrast Microscopy, Laser Protocols, and Modified Home Oral Hygiene in Maintenance. A 10-Year Retrospective Study. Appl. Sci. 2021, 11, 4985. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Caccianiga, P.; Leonida, A.; Baldoni, M.; Baldoni, A.; Ceraulo, S. Peri-Implantitis Management: Surgical versus Non-Surgical Approach Using Photodynamic Therapy Combined with Hydrogen Peroxide (OHLLT—Oxygen High Level Laser Therapy). A Retrospective Controlled Study. Appl. Sci. 2021, 11, 5073. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Caccianiga, P.; Leonida, A.; Baldoni, M.; Baldoni, A.; Ceraulo, S. Laser Management of Peri-Implantitis: A Comparison between Photodynamic Therapy Combined with Hydrogen Peroxide (OHLLT) and OHLLT + Er:YAG Laser. A Retrospective Controlled Study. Appl. Sci. 2021, 11, 6771. [Google Scholar] [CrossRef]
- Caccianiga, G.; Rey, G.; Baldoni, M.; Caccianiga, P.; Porcaro, G.; Baldoni, A.; Ceraulo, S. Laser Decontamination and LED Photobiomodulation Promote Bone Regeneration and Wound Healing by Secondary Intention, in Alveolar Ridge Preservation-Clinical and Radiographic Evaluation: A Pilot Experience. Photobiomodul. Photomed. Laser Surg. 2022, 40, 343–354. [Google Scholar] [CrossRef]
- Caccianiga, G.; Ferri, L.; Baldoni, M.; Bader, A.A.; Caccianiga, P. Magnetic Mallet and Laser for a Minimally Invasive Implantology: A Full Arch Case Report. Appl. Sci. 2022, 12, 9995. [Google Scholar] [CrossRef]
- Caccianiga, G.; Caccianiga, P.; Baldoni, M.; Lo Giudice, A.; Perillo, L.; Moretti, N.; Ceraulo, S. Pain Reduction during Rapid Palatal Expansion Due to LED Photobiomodulation Irradiation: A Randomized Clinical Trial. Life 2022, 12, 37. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Nucera, R.; Leonardi, R.; Paiusco, A.; Baldoni, M.; Caccianiga, G. A Comparative Assessment of the Efficiency of Orthodontic Treatment with and Without Photobiomodulation During Mandibular Decrowding in Young Subjects: A Single-Center, Single-Blind Randomized Controlled Trial. Photobiomodulation Photomed. Laser Surg. 2020, 38, 272–279. [Google Scholar] [CrossRef] [Green Version]
- Caccianiga, G.; Lo Giudice, A.; Paiusco, A.; Portelli, M.; Militi, A.; Baldoni, M.; Nucera, R. Maxillary Orthodontic Expansion Assisted by Unilateral Alveolar Corticotomy and Low-Level Laser Therapy: A Novel Approach for Correction of a Posterior Unilateral Cross-Bite in Adults. J. Lasers Med. Sci. 2019, 10, 225–229. [Google Scholar] [CrossRef]
- Odorici, A.; Colombari, B.; Bellini, P.; Meto, A.; Venturelli, I.; Blasi, E. Novel Options to Counteract Oral Biofilm Formation: In Vitro Evidence. Int. J. Environ. Res. Public Health 2022, 19, 8056. [Google Scholar] [CrossRef]
- Meto, A.; Colombari, B.; Castagnoli, A.; Sarti, M.; Denti, L.; Blasi, E. Efficacy of a Copper-Calcium-Hydroxide Solution in Reducing Microbial Plaque on Orthodontic Clear Aligners: A Case Report. Eur. J. Dent. 2019, 13, 478–484. [Google Scholar] [CrossRef] [Green Version]
- Callens, A. Darkfield or phase contrast microscopy. Usefulness in periodontology. Ned. Tijdschr. Tandheelkd. 1992, 99, 381–384. [Google Scholar]
- Rose, G.G. Phase-Contrast Microscopy in living cells. Microsc. Soc. 1964, 83, 97–114. [Google Scholar] [CrossRef]
- Leggott, P.J.; Anderson, A.W.; Punwani, I.; Sabet, T.; Murphy, R.; Crawford, J. Phase contrast microscopy of microbial aggregates in the gingival sulcus of Macaca mulatta. Subgingival plaque bacteria in macaca mulatta. J. Clin. Periodontol. 1983, 10, 412–421. [Google Scholar] [CrossRef]
- Quirynen, M.; Mongardini, C.; de Soete, M.; Pauwels, M.; Coucke, W.; van Eldere, J.; van Steenberghe, D. The role of chlorhexi-dine in the one-stage full-mouth disinfection treatment of patients with advanced adult periodontitis. Long-term clinical and microbiological observations. J. Clin. Periodontol. 2000, 27, 578–589. [Google Scholar] [CrossRef]
- Bollen, C.M.; Vandekerckhove, B.N.; Papaioannou, W.; Van Eldere, J.; Quirynen, M. Full-versus partial-mouth disinfection in the treatment of periodontal infections. A pilot study: Long-term microbiological observations. J. Clin. Periodontol. 1996, 23, 960–970. [Google Scholar] [CrossRef]
- Yeom, H.R.; Park, Y.J.; Lee, S.J.; Rhyu, I.C.; Chung, C.P.; Nisengard, R.J. Clinical and microbiological effects of minocycline-loaded microcapsules in adult periodontitis. J. Periodontol. 1997, 68, 1102–1109. [Google Scholar] [CrossRef]
- Quirynen, M.; Bollen, C.M.; Papaioannou, W.; Van Eldere, J.; van Steenberghe, D. The influence of titanium abutment surface roughness on plaque accumulation and gingivitis: Short-term observations. Int. J. Oral Maxillofac. Implant. 1996, 11, 169–178. [Google Scholar]
- Acharya, S.; Goyal, A.; Utreja, A.K.; Mohanty, U. Effect of three different motivational techniques on oral hygiene and gingi-val health of patients undergoing multibracketed orthodontics. Angle Orthod. 2011, 81, 884–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallie, A. Home use of interdental cleaning devices and toothbrushing and their role in disease prevention. Evid. Based Dent. 2019, 20, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Goyal, C.R.; Lyle, D.M.; Qaqish, J.G.; Schuller, R. The addition of a water flosser to power tooth brushing: Effect on bleeding, gingivitis, and plaque. J. Clin. Dent. 2012, 23, 57–63. [Google Scholar]
- Tawakoli, P.N.; Sauer, B.; Becker, K.; Buchalla, W.; Attin, T. Interproximal biofilm removal by intervallic use of a sonic tooth brush compared to an oral irrigation system. BMC Oral Health 2015, 15, 91. [Google Scholar] [CrossRef] [Green Version]
- Eakle, W.S.; Ford, C.; Boyd, R.L. Depth of penetration in periodontal pockets with oral irrigation. J. Clin. Periodontol. 1986, 13, 39–44. [Google Scholar] [CrossRef]
- Cutler, C.W.; Stanford, T.W.; Abraham, C.; Cederberg, R.A.; Boardman, T.J.; Ross, C. Clinical benefits of oral irrigation for per-iodontitis are related to reduction of pro-inflammatory cytokine levels and plaque. J. Clin. Periodontol. 2000, 27, 134–143. [Google Scholar] [CrossRef]
- Costa, F.O.; Costa, A.A.; Cota, L.O.M. The use of interdental brushes or oral irrigators as adjuvants to conventional oral hygiene associated with recurrence of periodontitis in periodontal maintenance therapy: A 6-year prospective study. J. Periodontol. 2020, 91, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Quirynen, M.; Teughels, W.; van Steenberghe, D. Impact of antiseptics on one-stage, full-mouth disinfection. J. Clin. Periodontol. 2006, 33, 49–52. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compatible Flora | T0 | T1 |
|---|---|---|
| Group A | 30 | 30 |
| Group B | 30 | 3 |
| Plaque Index < 30% | T0 | T1 |
|---|---|---|
| Group A | 30 | 30 |
| Group B | 30 | 23 |
| Group A (n = 30) | Group B (n = 30) | p Value | |
|---|---|---|---|
| Mean ± Sd | Mean ± Sd | ||
| BoP | 0.14 ± 0.09 | 0.11 ± 0.10 | <0.018 |
| P.I. | 0.23 ± 0.12 | 0.21 ± 0.11 | 0.006 |
| P.D. | 2.24 ± 0.23 | 2.25 ± 0.21 | 0.267 |
| Group A (n = 30) | Group B (n = 30) | p Value | |
|---|---|---|---|
| Mean ± Sd | Mean ± Sd | ||
| BoP | 0.12 ± 0.05 | 1.12 ± 0.21 | <0.0005 * |
| P.I. | 0.12 ± 0.15 | 0.93 ± 0.21 | <0.001 * |
| P.D. | 2.16 ± 0.18 | 2.41 ± 0.24 | 0.135 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caccianiga, P.; Bader, A.A.; Erba, P.; Caccianiga, G. Periodontal Maintenance Therapy: Efficacy of Oral Irrigator in the Home Oral Hygiene Protocol Associated with Microbiological Analysis with Phase Contrast Microscope. Inventions 2022, 7, 104. https://doi.org/10.3390/inventions7040104
Caccianiga P, Bader AA, Erba P, Caccianiga G. Periodontal Maintenance Therapy: Efficacy of Oral Irrigator in the Home Oral Hygiene Protocol Associated with Microbiological Analysis with Phase Contrast Microscope. Inventions. 2022; 7(4):104. https://doi.org/10.3390/inventions7040104
Chicago/Turabian StyleCaccianiga, Paolo, Ayt Alla Bader, Paola Erba, and Gianluigi Caccianiga. 2022. "Periodontal Maintenance Therapy: Efficacy of Oral Irrigator in the Home Oral Hygiene Protocol Associated with Microbiological Analysis with Phase Contrast Microscope" Inventions 7, no. 4: 104. https://doi.org/10.3390/inventions7040104