
The Streaming Web-Based Exercise at Home Study for Breast and Prostate Cancer Survivors: A Feasibility Study Protocol
 , ,
, ,
Abstract
:1. Introduction
2. Experimental Design
2.1. Study Design and Participants
2.2. Recruitment and Consent
2.3. Sample Size
2.4. Devices
2.4.1. Zoom
2.4.2. Fitbit
3. Procedures
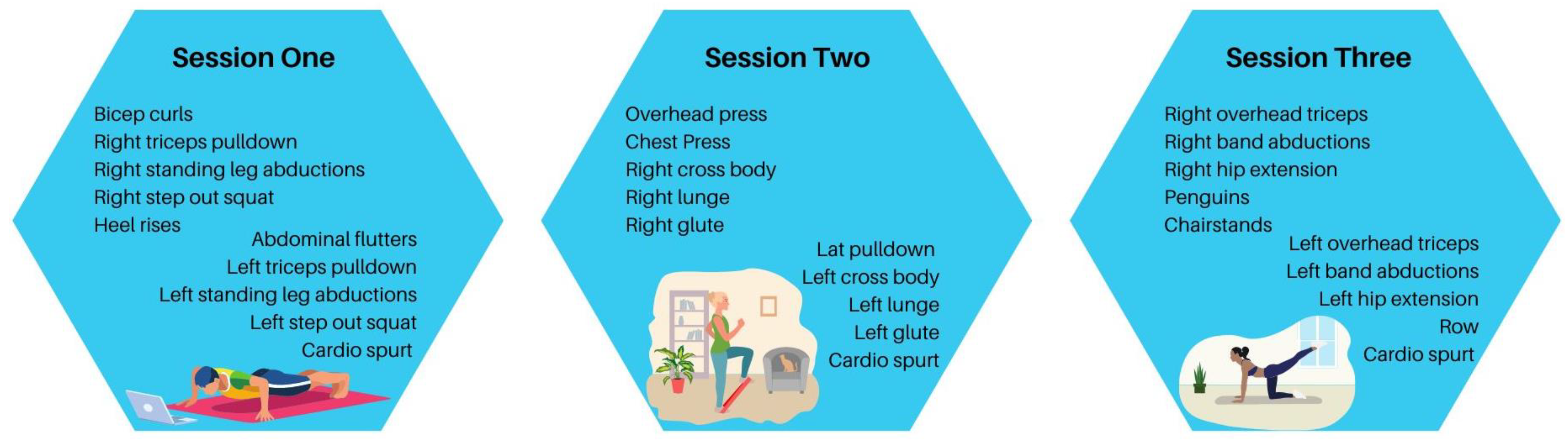
3.1. Intervention
3.2. Safety and Adverse Events
3.3. Withdrawal
3.4. Data Collection and Measures
3.5. Screening
3.6. Primary Outcomes
3.7. Secondary Outcomes
3.7.1. Fitness Outcomes
3.7.2. Patient-Reported Outcomes
3.8. Statistical Analysis
4. Expected Results
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Courneya, K.S.; Friedenreich, C.M. Physical Activity and Cancer Control. Semin. Oncol. Nurs. 2007, 23, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Speck, R.M.; Courneya, K.S.; Mâsse, L.C.; Duval, S.; Schmitz, K.H. An Update of Controlled Physical Activity Trials in Cancer Survivors: A systematic review and meta-analysis. J. Cancer Surviv. 2010, 4, 87–100. [Google Scholar] [CrossRef] [PubMed]
- McDonough, M.H.; Beselt, L.J.; Kronlund, L.J.; Albinati, N.K.; Daun, J.T.; Trudeau, M.S.; Wong, J.B.; Culos-Reed, S.N.; Bridel, W. Social Support and Physical Activity for Cancer Survivors: A Qualitative Review and Meta-study. J. Cancer Surviv. 2021, 15, 713–728. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, C.M.; Courneya, K.S.; Stein, K. Cancer Survivors’ Adherence to Lifestyle Behavior Recommendations and Associations with Health-related Quality of Life: Results from the American Cancer Society’s SCS-II. J. Clin. Oncol. 2008, 26, 2198–2204. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A.; et al. American College of Sports Medicine Roundtable on Exercise Quidelines for Cancer Survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Troeschel, A.N.; Leach, C.R.; Shuval, K.; Stein, K.D.; Patel, A.V. Physical Activity in Cancer Survivors During “Re-Entry” Following Cancer Treatment. Prev. Chronic Dis. 2018, 15, E65. [Google Scholar] [CrossRef]
- Nayak, P.; Holmes, H.M.; Nguyen, H.T.; Elting, L.S. Self-reported physical activity among middle-aged cancer survivors in the United States: Behavioral Risk Factor Surveillance System Survey, 2009. Prev. Chronic Dis. 2014, 11, E156. [Google Scholar] [CrossRef]
- Speed-Andrews, A.E.; Rhodes, R.E.; Blanchard, C.M.; Culos-Reed, S.N.; Friedenreich, C.M.; Belanger, L.J.; Courneya, K.S. Medical, Demographic and Social Cognitive Correlates of Physical Activity in a Population-Based Sample of Colorectal Cancer Survivors. Eur. J. Cancer Care 2012, 21, 187–196. [Google Scholar] [CrossRef]
- Forbes, C.C.; Blanchard, C.M.; Mummery, W.K.; Courneya, K.S. A Comparison of Physical Activity Correlates Across Breast, Prostate and Colorectal Cancer Survivors in Nova Scotia, Canada. Support. Care Cancer 2014, 22, 891–903. [Google Scholar] [CrossRef]
- Coups, E.J.; Ostroff, J.S. A Population-Based Estimate of the Prevalence of Behavioral Risk Factors Among Adult Cancer Survivors and Noncancer Controls. Prev. Med. 2005, 40, 702–711. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, K.M.; Rowland, J.H.; Jeffery, D.D.; McNeel, T. Health Behaviors of Cancer Survivors: Examining opportunities for cancer control intervention. J. Clin. Oncol. 2005, 23, 8884–8893. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute, Surveillance, Epidemiology, and End Results Program. Available online: https://seer.cancer.gov (accessed on 9 December 2022).
- Wong, J.N.; McAuley, E.; Trinh, L. Physical Activity Programming and Counseling Preferences Among Cancer Survivors: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 48. [Google Scholar] [CrossRef] [PubMed]
- Hefferon, K.; Murphy, H.; McLeod, J.; Mutrie, N.; Campbell, A. Understanding Barriers to Exercise Implementation 5-year Post-Breast Cancer Diagnosis: A large-scale qualitative study. Health Educ. Res. 2013, 28, 843–856. [Google Scholar] [CrossRef]
- Stout, N.L.; Baima, J.; Swisher, A.K.; Winters-Stone, K.M.; Welsh, J. A Systematic Review of Exercise Systematic Reviews in the Cancer Literature (2005–2017). PM&R 2017, 9, S347–S384. [Google Scholar] [CrossRef]
- Grazioli, E.; Cerulli, C.; Dimauro, I.; Moretti, E.; Murri, A.; Parisi, A. New Strategy of Home-Based Exercise during Pandemic COVID-19 in Breast Cancer Patients: A Case Study. Sustainability 2020, 12, 6940. [Google Scholar] [CrossRef]
- Natalucci, V.; Marini, C.F.; Flori, M.; Pietropaolo, F.; Lucertini, F.; Annibalini, G.; Vallorani, L.; Sisti, D.; Saltarelli, R.; Villarini, A.; et al. Effects of a Home-Based Lifestyle Intervention Program on Cardiometabolic Health in Breast Cancer Survivors during the COVID-19 Lockdown. J. Clin. Med. 2021, 10, 2678. [Google Scholar] [CrossRef]
- Kim, H.I.; Lim, H.; Moon, A. Sex Differences in Cancer: Epidemiology, Genetics and Therapy. Biomol. Ther. 2018, 26, 335–342. [Google Scholar] [CrossRef]
- Sitlinger, A.S.; Shelby, R.A.; Van Denburg, A.N.; White, H.; Edmond, S.N.; Marcom, P.K.; Bosworth, H.B.; Keefe, F.J.; Kimmick, G.G. Higher Symptom Burden is Associated with Lower Function in Women Taking Adjuvant Endocrine Therapy for Breast Cancer. J. Geriatr. Oncol. 2019, 10, 317–321. [Google Scholar] [CrossRef]
- Fleck, S.J. Detraining: Its Effects on Endurance and Strength. Strength Cond. J. 1994, 16, 22–28. [Google Scholar] [CrossRef]
- Chen, Y.-T.; Hsieh, Y.-Y.; Ho, J.-Y.; Lin, T.-Y.; Lin, J.-C. Two Weeks of Detraining Reduces Cardiopulmonary Function and Muscular Fitness in Endurance Athletes. Eur. J. Sport Sci. 2022, 22, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Bredin, S.S.D.; Jamnik, V.K.; Gledhill, N. Validation of the PAR-Q+ and ePARmed-X+. HFJC 2011, 4, 38–46. [Google Scholar] [CrossRef]
- Cardinal, B.J.; Esters, J.; Cardinal, M.K. Evaluation of the Revised Physical Activity Readiness Questionnaire in Older Adults. Med. Sci. Sports Exerc. 1996, 28, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Amireault, S.; Godin, G. The Godin-Shephard Leisure-Time Physical Activity Questionnaire: Validity evidence supporting its use for classifying healthy adults into active and insufficiently active categories. Percept. Mot. Skills 2015, 120, 604–622. [Google Scholar] [CrossRef]
- Amireault, S.; Godin, G.; Lacombe, J.; Sabiston, C.M. The use of the Godin-Shephard Leisure-Time Physical Activity Questionnaire in oncology research: A systematic review. BMC Med. Res. Methodol. 2015, 15, 60. [Google Scholar] [CrossRef]
- American College of Sports Medicine; Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Beam, W.C.; Adams, G.M. Exercise Physiology Laboratory Manual, 6th ed.; McGraw-Hill Education: New York, NY, USA, 2011. [Google Scholar]
- Heyward, V.H.; Gibson, A.L. Advanced Fitness Assessment and Exercise Prescription, 7th ed.; Human Kinetics: Champaign, IL, USA, 2014. [Google Scholar]
- Functional Assessment of Cancer Therapy—General. Available online: https://www.facit.org/measures/FACT-G (accessed on 9 December 2022).
- Brucker, P.S.; Yost, K.; Cashy, J.; Webster, K.; Cella, D. General Population and Cancer Patient Norms for the Functional Assessment of Cancer Therapy-General (FACT-G). Eval. Health Prof. 2005, 28, 192–211. [Google Scholar] [CrossRef]
- Cella, D.F.; Tulsky, D.S.; Gray, G.; Sarafian, B.; Linn, E.; Bonomi, A.; Silberman, M.; Yellen, S.B.; Winicour, P.; Brannon, J.; et al. The Functional Assessment of Cancer Therapy scale: Development and Validation of the General Measure. J. Clin Oncol. 1993, 11, 570–579. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on Reflexive Thematic Analysis. Qual. Res. Sport Exerc. 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. One Size Fits All? What Counts as Quality Practice in (reflexive) Thematic Analysis? Qual. Res. Psychol. 2021, 18, 328–352. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shirazipour, C.H.; Ruggieri-Bacani, R.M.; Lockshon, L.; Waring, C.; Jarman, A.; Cruz, N.; Bresee, C.; Fong, A.J.; Lin, P.-H.; Gresham, G.; et al. The Streaming Web-Based Exercise at Home Study for Breast and Prostate Cancer Survivors: A Feasibility Study Protocol. Methods Protoc. 2023, 6, 51. https://doi.org/10.3390/mps6030051
Shirazipour CH, Ruggieri-Bacani RM, Lockshon L, Waring C, Jarman A, Cruz N, Bresee C, Fong AJ, Lin P-H, Gresham G, et al. The Streaming Web-Based Exercise at Home Study for Breast and Prostate Cancer Survivors: A Feasibility Study Protocol. Methods and Protocols. 2023; 6(3):51. https://doi.org/10.3390/mps6030051
Chicago/Turabian StyleShirazipour, Celina H., Rachel M. Ruggieri-Bacani, Laura Lockshon, Christopher Waring, Aubrey Jarman, Novalyn Cruz, Catherine Bresee, Angela J. Fong, Pao-Hwa Lin, Gillian Gresham, and et al. 2023. "The Streaming Web-Based Exercise at Home Study for Breast and Prostate Cancer Survivors: A Feasibility Study Protocol" Methods and Protocols 6, no. 3: 51. https://doi.org/10.3390/mps6030051