
The Impact of Introducing Midwives and also Mentoring on the Quality of Sexual, Reproductive, Maternal, Newborn, and Adolescent Health Services in Low- and Middle-Income Countries: An Integrative Review Protocol


Abstract
:1. Introduction
1.1. Background
1.2. Objectives
1.3. Rationale
2. Methods
2.1. Study Design
2.2. Eligibility Criteria
- Population: Midwives, maternity staff (nurses, paramedics), health managers, patients receiving care
- Intervention: Midwifery-led interventions with mentorship on the quality of maternal and newborn healthcare
- Comparison: Effective vs. ineffective for health system strengthening and quality and availability of services
- Outcome: Operationalisation of evidence-based maternal health care within health systems, improved health outcomes including health and well-being of women and newborns, experiences of midwives, facility staff, and managers regarding deploying midwives, and improvements in care quality.

{kind=link}
| Key Concepts | Search Terms |
|---|---|
| Midwives/midwifery | Delivery, Obstetric; maternal health services; midwife * or midwiv *; maternal; skilled birth attendan * |
| Enabling environment | Enabling environment; supportive environment; mentoring; mentor; supervis * |
| Care quality/care improvement | Quality of health care; quality improvement; care quality; outcome; quality improvement; healthcare |
| Low- and middle-income countries (LMICs) | All countries will be included as per World Bank’s definition |
2.3. Exclusion Criteria
- (i)
- articles or reports published before 2010;
- (ii)
- national surveys published between 2010 and March 2023;
- (iii)
- studies that do not provide any impact or outcome;
- (iv)
- articles that are not available in full text; or
- (v)
- articles that are not accessible after contacting the corresponding author.
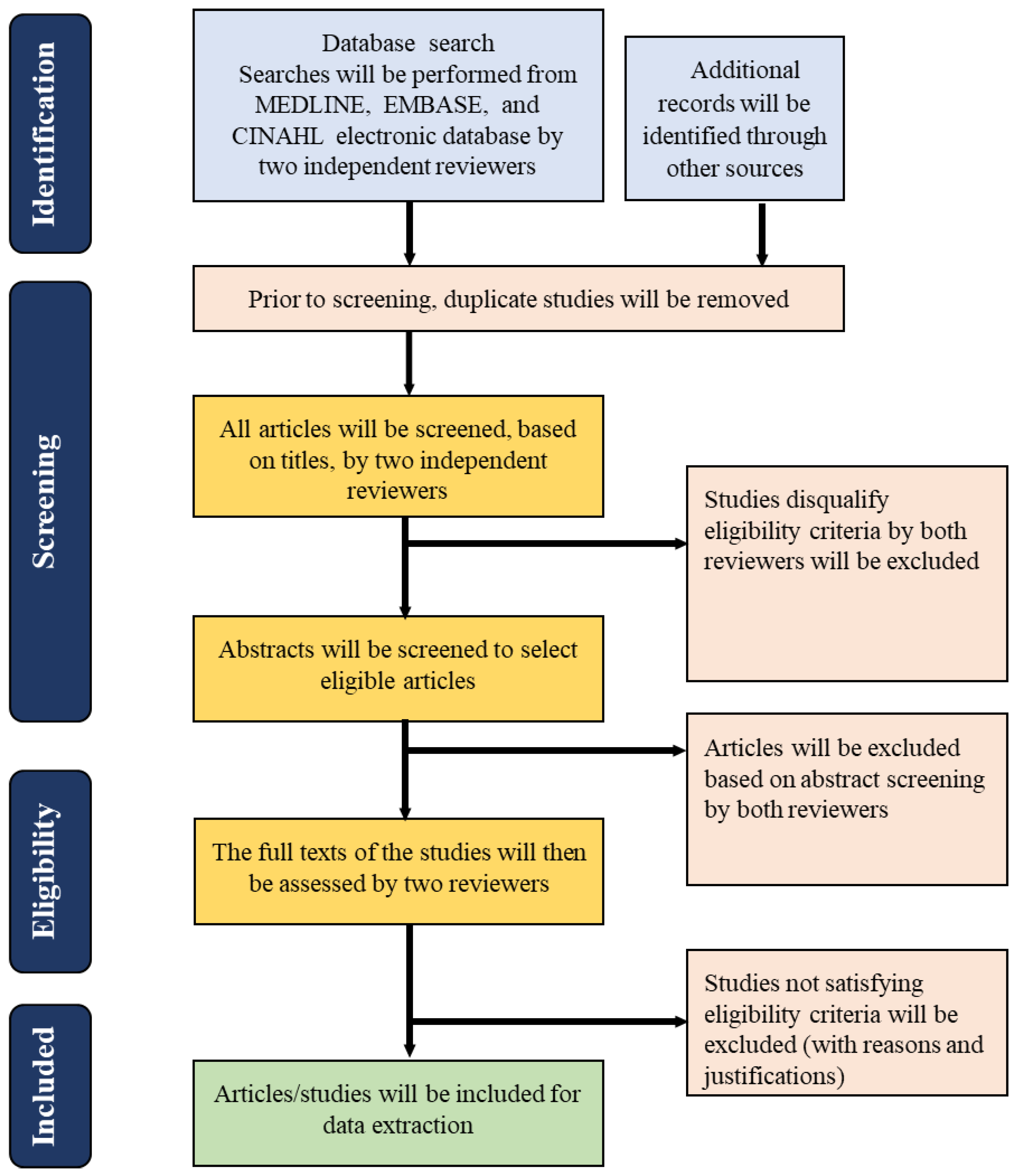
2.4. Study Selection/Type of Study to Be Included
2.5. Search Strategy
2.6. Information Sources
2.7. Data Extraction (Study Selection and Coding)
Operational Definition
2.8. Data Analysis and Presentation
2.9. Quality Assessment
3. Expected Results
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nove, A.; Friberg, I.K.; de Bernis, L.; McConville, F.; Moran, A.C.; Najjemba, M.; ten Hoope-Bender, P.; Tracy, S.; Homer, C.S. Potential impact of midwives in preventing and reducing maternal and neonatal mortality and stillbirths: A Lives Saved Tool modelling study. Lancet Glob. Health 2021, 9, e24–e32. [Google Scholar] [CrossRef]
- Thomas, T.N.; Gausman, J.; Lattof, S.R.; Wegner, M.N.; Kearns, A.D.; Langer, A. Improved maternal health since the ICPD: 20 years of progress. Contraception 2014, 90, S32–S38. [Google Scholar] [CrossRef] [PubMed]
- Renfrew, M.J.; McFadden, A.; Bastos, M.H.; Campbell, J.; Channon, A.A.; Cheung, N.F.; Silva, D.R.A.D.; Downe, S.; Kennedy, H.P.; Malata, A.; et al. Midwifery and quality care: Findings from a new evidence-informed framework for maternal and newborn care. Lancet 2014, 384, 1129–1145. [Google Scholar] [CrossRef] [PubMed]
- Homer, C.S.; Friberg, I.K.; Dias, M.A.B.; Hoope-Bender, P.T.; Sandall, J.; Speciale, A.M.; A Bartlett, L. The projected effect of scaling up midwifery. Lancet 2014, 384, 1146–1157. [Google Scholar] [CrossRef] [PubMed]
- Michel-Schuldt, M.; McFadden, A.; Renfrew, M.; Homer, C. The provision of midwife-led care in low-and middle-income countries: An integrative review. Midwifery 2020, 84, 102659. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J.R.; Sabin, L.L.; Onyango, M.A.; Sarker, M.; Declercq, E. Midwifery centers as enabled environments for midwifery: A quasi experimental design assessing women’s birth experiences in three models of care in Bangladesh, before and during covid. PLoS ONE 2022, 17, e0278336. [Google Scholar] [CrossRef]
- Sen, G.; Govender, V. Sexual and reproductive health and rights in changing health systems. Glob. Public Health 2015, 10, 228–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, R.; Williams, A.; Jess, N.; Read, J.M.; Limmer, M. The impact of professional midwives and mentoring on the quality and availability of maternity care in government sub-district hospitals in Bangladesh: A mixed-methods observational study. BMC Pregnancy Childbirth 2022, 22, 827. [Google Scholar] [CrossRef] [PubMed]
- McHugh, S.; Droog, E.; Foley, C.; Boyce, M.; Healy, O.; Browne, J. Understanding the impetus for major systems change: A multiple case study of decisions and non-decisions to reconfigure emergency and urgent care services. Health Policy 2019, 123, 728–736. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Low Quality Healthcare Is Increasing the Burden of Illness and Health Costs Globally 2018. Available online: https://www.who.int/news/item/05-07-2018-low-quality-healthcare-is-increasing-the-burden-of-illness-and-health-costs-globally. (accessed on 31 January 2023).
- Filby, A.; McConville, F.; Portela, A. What Prevents Quality Midwifery Care? A Systematic Mapping of Barriers in Low and Middle Income Countries from the Provider Perspective. PLoS ONE 2016, 11, e0153391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eby, L.T.; Allen, T.D.; Evans, S.C.; Ng, T.; DuBois, D. Does mentoring matter? A multidisciplinary meta-analysis comparing mentored and non-mentored individuals. J. Vocat. Behav. 2008, 72, 254–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ragins, B.R.; Cotton, J.L.; Miller, J.S. Marginal mentoring: The effects of type of mentor, quality of relationship, and program design on work and career attitudes. Acad. Manag. J. 2000, 43, 1177–1194. [Google Scholar] [CrossRef]
- Fagenson-Eland, E.A.; Marks, M.A.; Amendola, K.L. Perceptions of mentoring relationships. J. Vocat. Behav. 1997, 51, 29–42. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategic Directions for Nursing and Midwifery 2021–2025. 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/344562/9789240033863-eng.pdf (accessed on 30 January 2023).
- Feyissa, G.T.; Balabanova, D.; Woldie, M. How Effective are Mentoring Programs for Improving Health Worker Competence and Institutional Performance in Africa? A Systematic Review of Quantitative Evidence. J. Multidiscip. Healthc. 2019, 12, 989–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, D. Student midwives and accountability: Are mentors good role models? Br. J. Midwifery 2008, 16, 100–104. [Google Scholar] [CrossRef]
- Catton, H.N. Developing a Mentorship Program in Laos. Front. Public Health 2017, 5, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, R. The Sacred Hour: Uninterrupted Skin-to-Skin Contact Immediately after Birth. Newborn Infant Nurs. Rev. 2013, 13, 67–72. [Google Scholar] [CrossRef]
- Saxton, A.; Fahy, K.; Rolfe, M.; Skinner, V.; Hastie, C. Does skin-to-skin contact and breast feeding at birth affect the rate of primary postpartum haemorrhage: Results of a cohort study. Midwifery 2015, 31, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.; Williams, A.; Hoque, D.M.E.; Jess, N.; Shahjahan, F.; Hossain, A.; Bogren, M. Implementing midwifery services in public tertiary medical college hospitals in Bangladesh: A longitudinal study. Women Birth 2022, 36, 299–304. [Google Scholar] [CrossRef]
- ten Hoope-Bender, P.; de Bernis, L.; Campbell, J.; Downe, S.; Fauveau, V.; Fogstad, H.; Homer, C.S.; Kennedy, H.P.; Matthews, Z.; McFadden, A.; et al. Improvement of maternal and newborn health through midwifery. Lancet 2014, 384, 1226–1235. [Google Scholar] [CrossRef] [PubMed]
- Lavender, D.T. Improving quality of care during labour and childbirth and in the immediate postnatal period. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 36, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.; Soto, E.J.; Bhandari, G.; Kermode, M. Provider perspectives on the enabling environment required for skilled birth attendance: A qualitative study in western Nepal. Trop. Med. Int. Health 2014, 19, 1457–1465. [Google Scholar] [CrossRef]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. Medical Education: Entrusting Faith in Bedside Teaching. Res. Dev. Med. Educ. 2014, 3, 1–2. [Google Scholar]
- Anatole, M.; Magge, H.; Redditt, V.; Karamaga, A.; Niyonzima, S.; Drobac, P.; Mukherjee, J.S.; Ntaganira, J.; Nyirazinyoye, L.; Hirschhorn, L. Nurse mentorship to improve the quality of health care delivery in rural Rwanda. Nurs. Outlook 2013, 61, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Wallen, G.R.; Mitchell, S.A.; Melnyk, B.; Fineout-Overholt, E.; Miller-Davis, C.; Yates, J.; Hastings, C. Implementing evidence-based practice: Effectiveness of a structured multifaceted mentorship programme. J. Adv. Nurs. 2010, 66, 2761–2771. [Google Scholar] [CrossRef]
- Da Silva, R.N.; Brandão, M.A.G.; Ferreira, M.D.A. Integrative review as a method to generate or to test nursing theory. Nurs. Sci. Q. 2020, 33, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Eldawlatly, A.; Alshehri, H.; Alqahtani, A.; Ahmad, A.; Al-Dammas, F.; Marzouk, A. Appearance of Population, Intervention, Comparison, and Outcome as research question in the title of articles of three different anesthesia journals: A pilot study. Saudi J. Anaesth. 2018, 12, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.M.d.C.; Pimenta, C.A.d.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Lat.-Am. Enfermagem. 2007, 15, 508–511. [Google Scholar] [CrossRef] [Green Version]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid.-Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Everybody’s Business—Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action; Report No.: 9789241596077; World Health Organization: Geneva, Switzerland, 2007.
- Gough, D. Weight of Evidence: A framework for the appraisal of the quality and relevance of evidence. Res. Pap. Educ. 2007, 22, 213–228. [Google Scholar] [CrossRef]
- Wirth, M. Professionals with delivery skills: Backbone of the health system and key to reaching the maternal health Millennium Development Goal. Croat. Med. J. 2008, 49, 318–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, R.; Zaman, S.B. Improving the Quality of Maternity Care through the Introduction of Professional Midwives and Mentoring in Selected Sub-District Hospitals in Bangladesh: A Mixed Method Study Protocol. Methods Protoc. 2022, 5, 84. [Google Scholar] [CrossRef] [PubMed]

| Sl. | First Author, Country, Year | Title | Study Aim | Study Methods & Participants | Themes | ICM-Standard Midwives | Maternity Staff | Mentoring | Key Findings |
|---|---|---|---|---|---|---|---|---|---|
| 1 | |||||||||
| 2 | |||||||||
| 3 | |||||||||
| 4 |
| Dimension | Description of Review |
|---|---|
| A generic non-review-specific judgment of the coherence and relevance on its own terms, using the generally accepted criteria for this type of evidence. |
| A review-specific judgment about the fitness for purpose of the evidence for answering the question. |
| A review-specific judgment about the relevance of the focus of the evidence for the question. This could include issues of propriety in how the research was conducted, which could impact its inclusion and interpretation. |
| The three above judgments are then combined to give an overall assessment. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anderson, R.; Zaman, S.B.; Limmer, M. The Impact of Introducing Midwives and also Mentoring on the Quality of Sexual, Reproductive, Maternal, Newborn, and Adolescent Health Services in Low- and Middle-Income Countries: An Integrative Review Protocol. Methods Protoc. 2023, 6, 48. https://doi.org/10.3390/mps6030048
Anderson R, Zaman SB, Limmer M. The Impact of Introducing Midwives and also Mentoring on the Quality of Sexual, Reproductive, Maternal, Newborn, and Adolescent Health Services in Low- and Middle-Income Countries: An Integrative Review Protocol. Methods and Protocols. 2023; 6(3):48. https://doi.org/10.3390/mps6030048
Chicago/Turabian StyleAnderson, Rondi, Sojib Bin Zaman, and Mark Limmer. 2023. "The Impact of Introducing Midwives and also Mentoring on the Quality of Sexual, Reproductive, Maternal, Newborn, and Adolescent Health Services in Low- and Middle-Income Countries: An Integrative Review Protocol" Methods and Protocols 6, no. 3: 48. https://doi.org/10.3390/mps6030048