
Augmenting Mental Health Support for Patients Accessing Different Degrees of Formal Psychiatric Care through a Supportive Text Messaging Program: Protocol for a Randomized Controlled Trial
 , , , , , , , , add
Show full author list
, , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
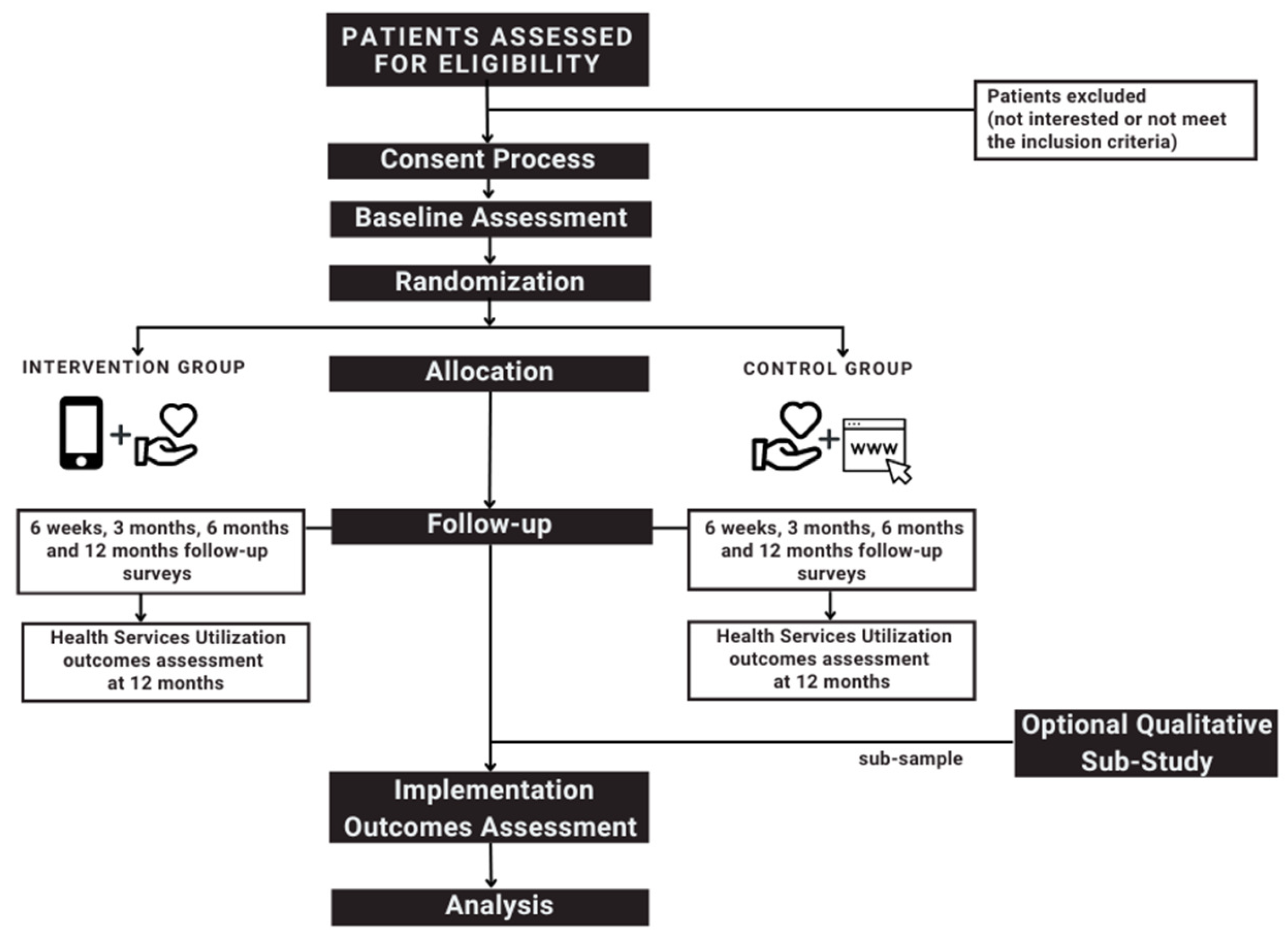
2.1. Study Design
2.2. Settings and Study Participants
2.3. Sample Size Considerations
2.4. Study Procedures
2.4.1. Consent Process
2.4.2. Baseline Assessment
2.4.3. Randomization and Allocation
2.4.4. Follow-Up Assessment
2.4.5. Optional Qualitative Sub-Study
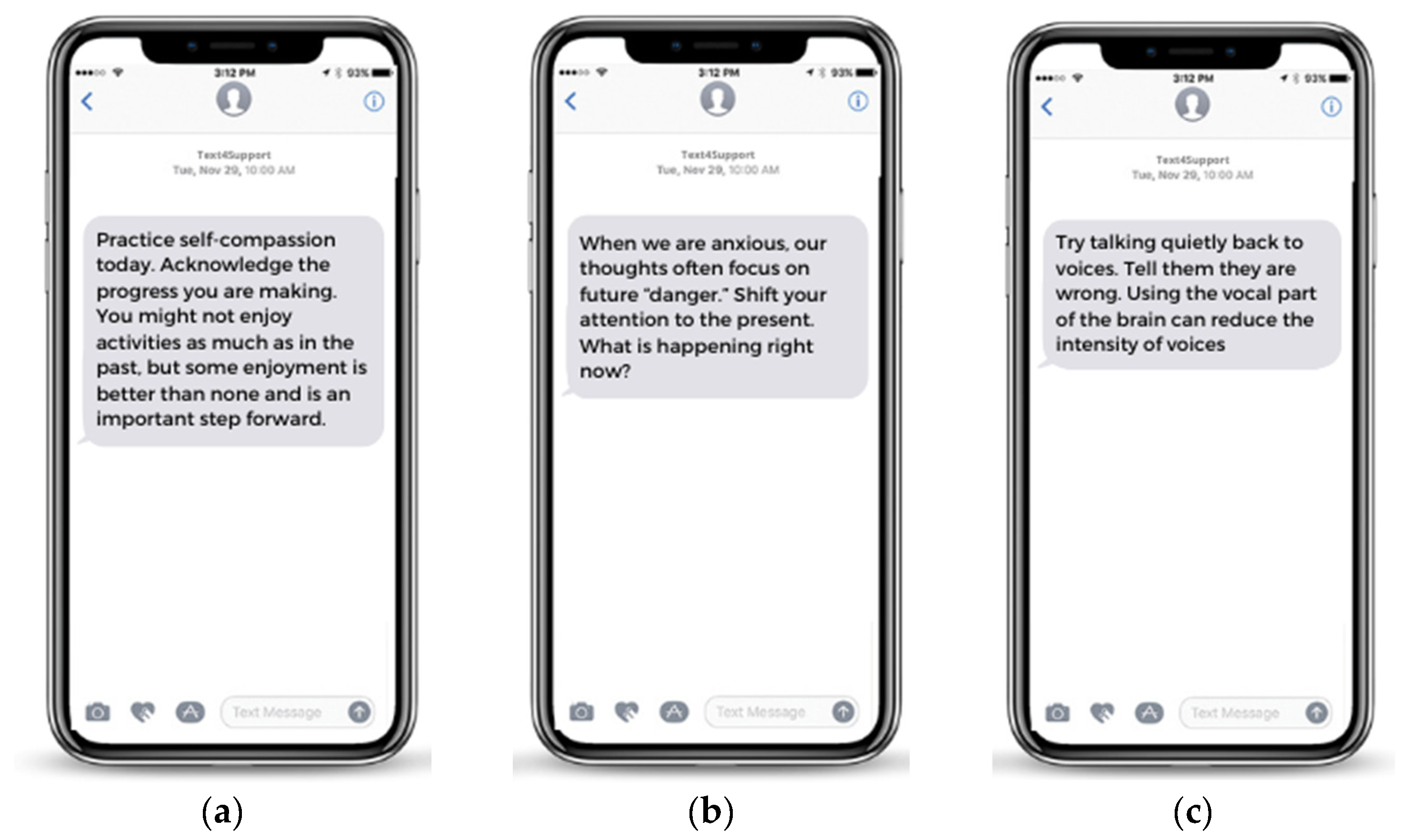
2.5. Proposed Interventions
2.6. Outcome Measures
- Clinical outcomes: The primary clinical outcome will be the differences in mean change in patient recovery and quality of life, assessed through the Recovery Assessment Scale (RAS) [37] and the World Health Organization Five Well-Being Index (WHO-5) [38]. Secondary clinical outcomes will include the differences between the intervention and control groups in prevalence changes for moderate-to-high depression (likely major depressive disorder), moderate-to-high anxiety (likely generalized anxiety disorder), and low resilience from the baseline to these time points, assessed through the Patient Health Questionnaire-9 (PHQ-9) [39], Generalized Anxiety Disorder-7 scale [40], and the Brief Resilience Scale (BRS) [41]. The mean score differences between groups from the baseline to determine time points will also be assessed using the Adverse Childhood questionnaire (ACE questionnaire) [42], and the Brief Substance Use Craving Scale (BSCS) [43], which will be used to assess childhood trauma and substance craving, as well as the clinician-rated Columbia-Suicide Severity Rating Scale (C-SSRS) [44], which will be used to assess suicide risk.
- Health service utilization outcomes: Health service utilization data will be extracted by the registration, reporting, and analytics, mental health and addiction team from the multiple health information systems utilized across NS Health and provided to the research team through reports. The differences in health service utilization data (mobile crisis visits, number of ED presentations, number of admissions in the last 12 months, length of stay, and the number of hospital readmissions) will be evaluated for participants in both groups. The differences between groups will be evaluated at 12 months.
- Patient experience and satisfaction outcomes: Patient satisfaction and patient experience with the e-mental health interventions (Text4Support and other e-mental health programs offered freely through NSH Authority) will be evaluated using both quantitative and qualitative data. Overall satisfaction will be assessed at each of the four time points (6 weeks and 3, 6, and 12 months) using a self-designed scale. Self-reported retention and withdrawal will both be assessed through the satisfaction survey, which addresses questions about the frequency of reading messages, the frequency of returning to messages stored in their phones, and actions taken by the participants after reading the text messages or freely available e-mental health resources (i.e., text “STOP”, clicking on links, searching for more information) up to 12 months after enrolment. Patient experience and satisfaction qualitative data will be collected through individual interviews and focus groups.
- Implementation Outcomes: Implementation outcomes are indicators of implementation efforts and are distinct from service or clinical outcomes [45]. For the intervention arm, we will include the reach of the interventions, acceptability, appropriateness, fidelity, and cost-effectiveness, evaluated at each of the four time points [28]. These implementation indicators will not be collected from the e-mental health or website visits in the control arm because they are not tied to the patient’s study ID and cannot be linked to the other measures.
2.7. Data Analysis
3. Expected Results
4. Risks and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Y.; Murray, A.M.; Toussaint, A.-K.; Chen, L.; Guo, W.-J.; He, N.; Luo, S.-X.; Yu, J.-Y.; Liu, Y.; Huang, M.-J.; et al. Why is the recognition rate of psychological distress under-estimated in general hospitals? A cross-sectional observational study in China. Medicine 2019, 98, e16274. [Google Scholar] [CrossRef]
- Faessler, L.; Kutz, A.; Haubitz, S.; Mueller, B.; Perrig-Chiello, P.; Schuetz, P. Psychological distress in medical patients 30 days fol-lowing an emergency department admission: Results from a prospective, observational study. BMC. Emerg. Med. 2016, 16, 33. [Google Scholar] [CrossRef]
- Phillips, M.S.; Steelesmith, D.L.; Campo, J.V.; Pradhan, T.; Fontanella, C.A. Factors Associated with Multiple Psychiatric Readmissions for Youth with Mood Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 619–631. [Google Scholar] [CrossRef]
- Kalb, L.G.; Stapp, E.K.; Ballard, E.D.; Holingue, C.; Keefer, A.; Riley, A. Trends in Psychiatric Emergency Department Visits Among Youth and Young Adults in the US. Pediatrics 2019, 143, e20182192. [Google Scholar] [CrossRef]
- Fleury, M.-J.; Ngui, A.N.; Bamvita, J.-M.; Grenier, G.; Caron, J. Predictors of Healthcare Service Utilization for Mental Health Reasons. Int. J. Environ. Res. Public Health 2014, 11, 10559–10586. [Google Scholar] [CrossRef]
- Urichuk, L.; Hrabok, M.; Hay, K.; Spurvey, P.; Sosdjan, D.; Knox, M.; Fu, A.; Surood, S.; Brown, R.; Coulombe, J.; et al. Enhancing peer support experience for patients discharged from acute psychiatric care: Protocol for a randomised controlled pilot trial. BMJ Open 2018, 8, e022433. [Google Scholar] [CrossRef]
- Willcox, J.C.; Dobson, R.; Whittaker, R. Old-Fashioned Technology in the Era of “Bling”: Is There a Future for Text Messaging in Health Care? J. Med. Internet Res. 2019, 21, e16630. [Google Scholar] [CrossRef]
- Fleming, C. The Chronicle Review. The Tyranny of Trendy Ideas. Available online: https://www.chronicle.com/interactives/20190701-trendyideas (accessed on 14 December 2019).
- Hoffman, L.; Benedetto, E.; Huang, H.; Grossman, E.; Kaluma, D.; Mann, Z.; Torous, J. Augmenting mental health in primary care: A 1-year study of deploying smartphone apps in a multi-site primary care/behavioural health integration program. Front. Psychiatry 2019, 10, 94. [Google Scholar] [CrossRef]
- Czyz, E.K.; Arango, A.; Healy, N.; King, C.A.; Walton, M. Augmenting Safety Planning with Text Messaging Support for Adolescents at Elevated Suicide Risk: Development and Acceptability Study. JMIR Ment. Health 2020, 7, e17345. [Google Scholar] [CrossRef]
- Shalaby, R.; Adu, M.K.; El Gindi, H.M.; Agyapong, V.I.O. Text Messages in the Field of Mental Health: Rapid Review of the Reviews. Front. Psychiatry. 2022, 13, 921982. [Google Scholar] [CrossRef]
- Musiat, P.; Tarrier, N. Collateral outcomes in e-mental health: A systematic review of the evidence for added benefits of computerized cognitive behavior therapy interventions for mental health. Psychol. Med. 2014, 44, 3137–3150. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.O.; Mrklas, K.; Juhás, M.; Omeje, J.; Ohinmaa, A.; Dursun, S.M.; Greenshaw, A.J. Cross-sectional survey evaluating Text4Mood: Mobile health program to reduce psychological treatment gap in mental healthcare in Alberta through daily supportive text messages. BMC Psychiatry 2016, 16, 378. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Hrabok, M.; Vuong, W.; Gusnowski, A.; Shalaby, R.; Mrklas, K.; Li, D.; Urichuk, L.; Snaterse, M.; Surood, S.; et al. Closing the Psychological Treatment Gap During the COVID-19 Pandemic with a Supportive Text Messaging Program: Protocol for Implementation and Evaluation. JMIR Res. Protoc. 2020, 9, e19292. [Google Scholar] [CrossRef] [PubMed]
- Shalaby, R.; Spurvey, P.; Knox, M.; Rathwell, R.; Vuong, W.; Surood, S.; Urichuk, L.; Snaterse, M.; Greenshaw, A.J.; Li, X.-M.; et al. Clinical Outcomes in Routine Evaluation Measures for Patients Discharged from Acute Psychiatric Care: Four-Arm Peer and Text Messaging Support Controlled Observational Study. Int. J. Environ. Res. Public Health 2022, 19, 3798. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Juhás, M.; Ohinmaa, A.; Omeje, J.; Mrklas, K.; Suen, V.Y.M.; Dursun, S.M.; Greenshaw, A.J. Randomized controlled pilot trial of supportive text messages for patients with depression. BMC Psychiatry 2017, 17, 286. [Google Scholar] [CrossRef]
- Agyapong, V.; Shalaby, R.; Hrabok, M.; Vuong, W.; Noble, J.; Gusnowski, A.; Mrklas, K.; Li, D.; Snaterse, M.; Surood, S.; et al. Mental Health Outreach via Supportive Text Messages during the COVID-19 Pandemic: Improved Mental Health and Reduced Suicidal Ideation after Six Weeks in Subscribers of Text4Hope Compared to a Control Population. Int. J. Environ. Res. Public Health 2021, 18, 2157. [Google Scholar] [CrossRef] [PubMed]
- Shalaby, R.; Agyapong, B.; Vuong, W.; Hrabok, M.; Gusnowski, A.; Surood, S.; Greenshaw, A.J.; Agyapong, V.I.O. Naturalistic randomized controlled trial demonstrating effectiveness of Text4Hope in supporting male population mental health during the COVID-19 pandemic. Front. Public Health 2022, 10, 1002288. [Google Scholar] [CrossRef]
- Noble, J.M.; Vuong, W.; Surood, S.; Urichuk, L.; Greenshaw, A.J.; Agyapong, V.I. Text4Support Mobile-Based Programming for Individuals Accessing Addictions and Mental Health Services—Retroactive Program Analysis at Baseline, 12 Weeks, and 6 Months. Front. Psychiatry 2021, 12, 781. [Google Scholar] [CrossRef] [PubMed]
- Shalaby, R.; Vuong, W.; Eboreime, E.; Surood, S.; Greenshaw, A.J.; Agyapong, V.I.O. Patients’ Expectations and Experiences With a Mental Health–Focused Supportive Text Messaging Program: Mixed Methods Evaluation. JMIR Form. Res. 2022, 6, e33438. [Google Scholar] [CrossRef]
- Rathbone, A.L.; Prescott, J. The Use of Mobile Apps and SMS Messaging as Physical and Mental Health Interventions: Systematic Review. J. Med. Internet Res. 2017, 19, e295. [Google Scholar] [CrossRef] [Green Version]
- Carolan, S.; Harris, P.R.; Cavanagh, K. Improving Employee Well-Being and Effectiveness: Systematic Review and Meta-Analysis of Web-Based Psychological Interventions Delivered in the Workplace. J. Med. Internet Res. 2017, 19, e271. [Google Scholar] [CrossRef] [PubMed]
- D’Arcey, J.; Collaton, J.; Kozloff, N.; Voineskos, A.N.; Kidd, S.A.; Foussias, G. The Use of Text Messaging to Improve Clini-cal Engagement for Individuals with Psychosis: Systematic Review. JMIR Ment. Health 2020, 7, e16993. [Google Scholar] [CrossRef]
- Steinkamp, J.M.; Goldblatt, N.; Borodovsky, J.T.; Lavertu, A.; Kronish, I.M.; Marsch, L.A.; Schuman-Olivier, Z. Technological Interventions for Medication Adherence in Adult Mental Health and Substance Use Disorders: A Systematic Review. JMIR Ment. Health 2019, 6, e12493. [Google Scholar] [CrossRef] [PubMed]
- Berrouiguet, S.; Baca-García, E.; Brandt, S.A.; Walter, M.; Courtet, P. Fundamentals for Future Mobile-Health (mHealth): A Systematic Review of Mobile Phone and Web-Based Text Messaging in Mental Health. J. Med. Internet Res. 2016, 18, e5066. [Google Scholar] [CrossRef]
- Liverpool, S.; Mota, C.P.; Sales, C.M.D.; Čuš, A.; Carletto, S.; Hancheva, C.; Sousa, S.; Cerón, S.C.; Moreno-Peral, P.; Pietrabissa, G.; et al. Engaging Children and Young People in Digital Mental Health Interventions: Systematic Review of Modes of Delivery, Facilitators, and Barriers. J. Med. Internet Res. 2020, 22, e16317. [Google Scholar] [CrossRef] [PubMed]
- Clarke, V.; Braun, V. Teaching thematic analysis: Overcoming challenges and developing strategies for effective learning. Psychologist 2013, 1, 26–32. [Google Scholar]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- O’Keeffe, A.G.; Ambler, G.; Barber, J.A. Sample size calculations based on a difference in medians for positively skewed outcomes in health care studies. BMC Med. Res. Methodol. 2017, 17, 157. [Google Scholar] [CrossRef]
- Benchmark Six Sigma: Sample Size Calculator for 2 Sample T-Tests. Available online: https://www.benchmarksixsigma.com/calculators/sample-size-calculator-for-2-sample-t-test/ (accessed on 2 April 2022).
- Nkire, N.; Mrklas, K.; Hrabok, M.; Gusnowski, A.; Vuong, W.; Surood, S.; Abba-Aji, A.; Urichuk, L.; Cao, B.; Greenshaw, A.J.; et al. COVID-19 Pandemic: Demographic Predictors of Self-Isolation or Self-Quarantine and Impact of Isolation and Quarantine on Perceived Stress, Anxiety, and Depression. Front. Psychiatry 2021, 12, 553468. [Google Scholar] [CrossRef] [PubMed]
- Morse, J.M. Determining sample size. Qual. Health Res. 2000, 10, 3–5. [Google Scholar] [CrossRef]
- Guest, G.; Namey, E.; Chen, M. A simple method to assess and report thematic saturation in qualitative research. PLoS ONE 2020, 15, e0232076. [Google Scholar] [CrossRef]
- ResilienceNHope: ResilienceNHope Programs. Available online: https://www.resiliencenhope.org/programs (accessed on 15 March 2022).
- Global Psychological e-Health Foundation. Available online: https://www.gpehealth.org/ (accessed on 2 April 2022).
- Nova Scotia Health: Mental Health and Addictions Tools. Available online: https://mha.nshealth.ca/en/tools (accessed on 25 March 2022).
- Giffort, D. The recovery assessment scale. In Can we Measure Recovery? A Compendium of Recovery and Recovery-Related Instruments; Ralph, R.O., Kidder, K., Phillips, D., Eds.; HSRI: Cambridge, MA, USA, 2000; Volume II. [Google Scholar]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.E.; Lee, B. The Psychometric Properties of the Patient Health Questionnaire-9 in a Sample of Korean University Students. Psychiatry Investig. 2019, 16, 904–910. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Somoza, E.; Dyrenforth, S.; Goldsmith, J.; Mezinskis, J.; Cohen, M. In search of a universal drug craving scale. Presented at the Annual Meeting of the American Psychiatric Association, Miami, FL, USA, 22 May 1995. [Google Scholar]
- Posner, K.; Brent, D.; Lucas, C.; Gould, M.; Stanley, B.; Brown, G.; Fisher, P.; Zelazny, J.; Burke, A.; Oquendo, M.J.; et al. Columbia-Suicide Severity Rating Scale (C-SSRS); Columbia University Medical Center: New York, NY, USA, 2008; Volume 10. [Google Scholar]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for Implementation Research: Conceptual Distinctions, Measurement Challenges, and Research Agenda. Adm. Ment. Health Adm. Policy Ment. Health Ment. Health Serv. Res. 2011, 38, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; for the CONSORT Group. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomized Trials. Ann. Intern. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Hemming, K.; Haines, T.P.; Chilton, P.J.; Girling, A.J.; Lilford, R.J. The stepped wedge cluster randomised trial: Rationale, design, analysis, and reporting. BMJ 2015, 350, h391. [Google Scholar] [CrossRef] [PubMed]
- QSR International Pty Ltd. NVivo Qualitative Data Analysis Software, Version 12; QSR International Pty Ltd.: Melbourne, Australia, 2018. [Google Scholar]
- Klasnja, P.; Pratt, W. Healthcare in the pocket: Mapping the space of mobile-phone health interventions. J. Biomed. Inform. 2011, 45, 184–198. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Outcome Measures | Instrument | Description | Data Collection Time Points | ||||
|---|---|---|---|---|---|---|---|
| Baseline | 6 w | 3 m | 6 m | 12 m | |||
| Clinical outcomes (measures of impact) | |||||||
| Patient’s recovery | Recovery Assessment Scale (RAS) [37] * | RAS is a 20-item measure developed based on a process model of recovery, which evaluates various aspects of recovery with a special focus on hope and self-determination. | X | X | X | X | X |
| Quality of Life | WHO-5 Well-Being Index [38] * | WHO-5-Well-Being Index is a short 5-item generic global rating scale measuring subjective well-being. The scale was derived from the WHO-10, which in turn was derived from a 28-item rating scale. The scale has adequate validity both as a screening tool for depression and as an outcome measure in clinical trials. | X | X | X | X | X |
| Likely depression | PHQ-9 [39] * | The PHQ-9 is a 9-item validated instrument used to diagnose and measure the severity of depression in general medical and mental health settings. The scale has good convergent validity and adequate internal consistency. | X | X | X | X | X |
| Likely anxiety | GAD-7 [40] * | GAD-7 is a validated 7-item questionnaire used to assess the self-reported levels of anxiety in respondents in the two weeks prior to assessment. | X | X | X | X | X |
| Patient’s Resilience | BRS [41] * | The BRS assesses the perceived ability to bounce back or recover from stress. The possible score range on the BRS is from 1 (low resilience) to 5 (high resilience) | X | X | X | X | X |
| Patient’s trauma-related stress | ACE questionnaire [42] * | The ACE Questionnaire is a 10-item measure used to measure childhood trauma. The questionnaire assesses 10 types of childhood trauma measured in the ACE Study. | X | ||||
| Patient’s tendency and desire for each addictive substance | BSCS [43] * | BSCS is a self-reporting scale to assess the intensity, frequency, and length of time spent craving in the past 24 h, using a five-point Likert scale ranging from 0 to 4 with a mean score of 0 indicating no cravings in the past 24 h and a mean score of 4 indicating a high tendency for drug craving. | X | X | X | X | X |
| Patient’s suicidal risk | Columbia Rating Scale [44] ** | C-SSRS is a self-reporting suicidal ideation and behaviour rating scale to evaluate suicide risk. | X | X | X | X | X |
| Health Services Utilization Outcomes (measures of impact) | |||||||
| Crisis calls | Administrative data | The number and proportion of patients calling the Crisis helpline. | - | - | - | - | X |
| Hospital Admissions | Administrative data | The number and proportion of MHA admissions into medical units, specialty, forensic of withdrawal management units in the last 12 months | - | - | - | - | X |
| Length of Stay | Administrative data | Length of stay for each MHA-related hospital admission. | - | - | - | - | X |
| Hospital readmissions | Administrative data | The number and proportion of patients readmitted into MHA acute care units within 30-days after discharge. | - | - | - | - | X |
| Emergency Department (ED) presentations | Administrative data | The number and proportion of MHA-specific ED presentations. | |||||
| Implementation outcomes (measures of process) | |||||||
| Reach | Administrative data | The proportion of the target population who receive daily supportive text messages across Nova Scotia. | - | X | X | X | X |
| Acceptability | Self-designed instrument | Evaluates clients’ satisfaction and experiences with supportive text messaging programs. | - | X | X | X | X |
| Appropriateness | Sociocultural, gender and age sensitivity. | Qualitative in-depth interviews | - | X | X | X | X |
| Incremental cost-utility | Administrative data | The incremental cost-effectiveness ratio (ICER) is the ratio between the difference in costs and the difference in benefits of the intervention | - | X | X | X | X |
| Overall satisfaction, retention, withdrawal, and engagement rate | Self-designed Online survey | Evaluates clients’ satisfaction and experiences with supportive text messaging programs. | X | X | X | X | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dias, R.d.L.; Shalaby, R.; Agyapong, B.; Obuobi-Donkor, G.; Adu, M.K.; Eboreime, E.; Obeng Nkrumah, S.; Sridharan, S.; Simon, P.; Taylor, B.; et al. Augmenting Mental Health Support for Patients Accessing Different Degrees of Formal Psychiatric Care through a Supportive Text Messaging Program: Protocol for a Randomized Controlled Trial. Methods Protoc. 2023, 6, 19. https://doi.org/10.3390/mps6010019
Dias RdL, Shalaby R, Agyapong B, Obuobi-Donkor G, Adu MK, Eboreime E, Obeng Nkrumah S, Sridharan S, Simon P, Taylor B, et al. Augmenting Mental Health Support for Patients Accessing Different Degrees of Formal Psychiatric Care through a Supportive Text Messaging Program: Protocol for a Randomized Controlled Trial. Methods and Protocols. 2023; 6(1):19. https://doi.org/10.3390/mps6010019
Chicago/Turabian StyleDias, Raquel da Luz, Reham Shalaby, Belinda Agyapong, Gloria Obuobi-Donkor, Medard K. Adu, Ejemai Eboreime, Samuel Obeng Nkrumah, Sanjana Sridharan, Patryk Simon, Bryanne Taylor, and et al. 2023. "Augmenting Mental Health Support for Patients Accessing Different Degrees of Formal Psychiatric Care through a Supportive Text Messaging Program: Protocol for a Randomized Controlled Trial" Methods and Protocols 6, no. 1: 19. https://doi.org/10.3390/mps6010019